
Abstract
The use of dipeptidyl peptidase-4 (DPP-4) inhibitors may be associated with pancreatic cancer and acute pancreatitis. Recent meta-analyses have reported conflicting findings. Therefore, we performed a meta-analysis to assess the risk of both pancreatic cancer and acute pancreatitis associated with the use of DPP-4 inhibitors. We also used trial sequential analysis to evaluate whether the number of patients included was enough to reach conclusions. We included randomised controlled trials lasting 24 weeks or more that compared DPP-4 inhibitors with placebo or other antihyperglycaemic agents. A total of 59,404 patients were included. There was no relationship between the use of DPP-4 inhibitors and pancreatic cancer (Peto odds ratio 0.65; 95% CI 0.35–1.21), and the optimal sample size was reached to determine a number needed to harm (NNH) of 1000 patients. DPP-4 inhibitors were associated with increased risk for acute pancreatitis (Peto odds ratio 1.72; 95% CI 1.18–2.53), with an NNH of 1066 patients, but the optimal sample size for this outcome was not reached. In conclusion, there is no association between DPP-4 inhibitors and pancreatic cancer, and a small risk for acute pancreatitis was observed with DPP-4 inhibitor use, although the latter finding is not definitive.
Similar content being viewed by others

Introduction
Dipeptidyl peptidase-4 (DPP-4) inhibitors, or gliptins, are incretin-mimetic oral antihyperglycaemic agents whose clinical use has steadily increased over the past ten years1. These medications are not associated with severe hypoglycaemia and have a neutral effect on weight. However, there are concerns that the use of DPP-4 inhibitors may be associated with increased risk for pancreatic cancer and acute pancreatitis2,3.
An early study analysed the FDA reports of pancreatic cancer and concluded that there was a 2.7-fold increase in the risk for pancreatic cancer with DPP-4 inhibitor use2. Another study suggested that DPP-4 inhibitor use was associated with the occurrence of α-cell hyperplasia, that is, increased proliferation and dysplasia, with potential evolution into neuroendocrine tumours4. Later, a pooled analysis of clinical trials with sitagliptin suggested no association between use of this medication and pancreatic cancer5. The lack of association between DPP-4 inhibitor use and pancreatic cancer was evaluated in a pooled analysis including only two large randomised trials, and no association was found6. Recently, three meta-analyses assessed the risk for acute pancreatitis among patients taking gliptins. Li et al. analysed the results of 60 randomised and non-randomised trials and found no increased risk of pancreatitis in patients treated with gliptins compared with controls7. Despite this reassuring finding, the inclusion of observational studies might have influenced the results owing to selection bias. Conversely, two other meta-analyses found contradictory results when analysing the results of three large studies assessing the cardiovascular risk of sitagliptin, saxagliptin and alogliptin1,3. In these studies, the use of DPP-4 inhibitors increased the risk of pancreatitis. Importantly, the potential cases of acute pancreatitis were adjudicated in these three trials.
Considering the potential association between DPP-4 inhibitor use and both pancreatic cancer and acute pancreatitis, we performed a meta-analysis including all randomised trials with DPP-4 inhibitor use lasting at least 24 weeks, in order to analyse whether there is an increased risk of pancreatic cancer and/or acute pancreatitis. We also applied trial sequential analysis (TSA) to assess whether the number of patients randomised in these trials was sufficient to reach definitive conclusions.
Methods
Protocol and registration
This systematic review and meta-analysis follows the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) protocol8 and was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the number CRD42016953346.
Patient Involvement
No patients were directly involved in the study.
Information source and search strategy
We performed a systematic literature search for all randomised clinical trials (RCTs) that compared DPP-4 inhibitor use with either placebo or other antihyperglycaemic medications. We searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL) and ClinicalTrials.gov from database inception to May 2016. We also searched abstracts from the most recent meetings of the American Diabetes Association and the European Association for the Study of Diabetes. The search strategy used the Medical Subject Headings (MeSH) terms “sitagliptin” OR “saxagliptin” OR “linagliptin” OR “alogliptin” OR “vildagliptin” AND “diabetes mellitus, type 2” AND a validated filter to identify RCTs9. All eligible trials were considered for review, regardless of language. A manual search of the reference lists of key articles was also performed.
Eligibility criteria
The inclusion criteria were: (1) RCTs, (2) DPP-4 inhibitor use versus any standard of comparison, (3) treatment for at least 24 weeks, (4) definition of events of acute pancreatitis and/or pancreatic cancer, (5) inclusion of patients ≥18 y old, and (6) diagnosis of type 2 diabetes according to the American Diabetes Association criteria10.
Study selection and data collection
Two independent investigators (L.C.P. and S.S.B.) selected studies on the basis of titles and abstracts. Studies satisfying the inclusion criteria and those with abstracts that lacked crucial information to decide upon their exclusion were retrieved for full-text evaluation. Both investigators also analysed the selected trials and extracted data; disagreements were resolved by a third reviewer (D.V.R.). The following information was extracted: first author’s name, year of publication, sample size and dropouts, age distribution, gender distribution, trial duration, treatment in use prior to randomisation, acute pancreatitis and pancreatic cancer events.
Risk of bias in individual studies and the quality of meta-analysis
The quality of studies was assessed according to the Cochrane Collaboration tool for risk of bias, including the following six domains: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other biases such as adjudication of events11,12. In adjudicated trails, the diagnosis was confirmed by the following criteria: symptoms of abdominal pain or vomiting and evidence of pancreatic inflammation (e.g., elevated pancreatic enzymes, amylase or lipase >3× the normal upper limit; in patients with chronic pancreatitis, enzyme elevations >2× the normal upper limit) or evidence of acute pancreatitis documented by abdominal computerised tomography, magnetic resonance imaging or ultrasound showing focal, diffuse and inhomogeneous gland enlargement. The quality of each outcome (pancreatic cancer and acute pancreatitis) was evaluated by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach13. Each meta-analysis was rated as high, moderate, low or very low quality.
Synthesis of results
We compared the events of interest between patients randomised to the use of DPP-4 inhibitors and patients randomised to the control treatment (placebo or other antihyperglycaemic medications). The outcomes of interest were pancreatic cancer and acute pancreatitis.
Data were summarised with direct meta-analysis to compare DPP-4 inhibitors with placebo and other antihyperglycaemic agents. We used the Peto odds ratio and the Mantel-Haenszel test for analysis. We used the Peto odds ratio in the primary analyses as it is more conservative (can identify smaller associations) and is superior when dealing with rare events. Heterogeneity was assessed by Cochran’s Q test (a p-value of 0.1 was considered statistically significant) and the I2 test (values greater than 50% were considered to indicate elevated statistical heterogeneity). For studies with no events in either arm, continuity correction was performed to include these data in TSA analyses. To assess whether the length of the trials was related to the outcome, we performed meta-regression, using study duration as a covariate.
Furthermore, to address whether current information is sufficient for firm conclusions, we performed TSA of the identified studies. This analysis is analogous to sample size estimation or interim analysis of a single study14,15 and is associated with a cumulative meta-analysis represented by the Z-curve. Therefore, we calculated the sample size required to detect or reject a minimal relevant difference between DPP-4 inhibitors and the control1,4. We defined this minimal relevant difference as an absolute difference of 0.1% in the incidence of both outcomes (pancreatic cancer and acute pancreatitis) between groups on the basis of previous trial results1. We conducted the TSA with an overall 5% risk of type I error and 20% risk of type II error (power of 80%).
We evaluated publication bias with visual inspection of funnel plots and with Begg’s and Egger’s tests. If small-study bias was identified, we applied the trim-and-fill method to explore the effect of missing studies on the outcomes.
The analyses were performed using the programs RevMan version 5.3 (Cochrane Collaboration, Copenhagen, Denmark) and STATA 12.0 (Stata Inc., College Station, Texas, USA). The TSA was performed with TSA software (Centre for Clinical Intervention Research Department, Copenhagen, Denmark).
Results
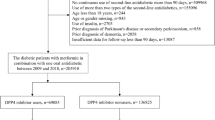
Our search retrieved 763 articles. After we scanned through the titles and abstracts and removed all duplicates, 186 articles remained for full-text evaluation. Ultimately, 38 trials were included in the analysis (Fig. 1 – Study Flowchart).

Study flowchart.
The selected studies were published between 2009 and 2015. The mean trial duration was 63.5 weeks (range, 24–260). The analysis included 59,404 patients; 39,970 (62.1%) were men, and the mean age was 57.39 ± 5.12 years. The main characteristics of the included trials are presented in Table 1. Results regarding the individual quality of the included trials are presented in Supplemental Material.
The analysis of the funnel plots and Begg’s and Egger’s tests suggested no publication bias for either outcome (pancreatic cancer or acute pancreatitis).
DPP-4 inhibitors and pancreatic cancer
There were 16 events of pancreatic cancer in the DPP-4 inhibitor group and 24 events in the control group. DPP-4 inhibitors were not associated with increased risk for pancreatic cancer in the direct meta-analysis (Peto odds ratio 0.65; 95% CI 0.35–1.21) (Fig. 2A – Forest plot for association between DPP-4 inhibitors and pancreatic cancer). Similar results were observed with the Mantel-Haenszel test (0.65; 95% CI 0.35–1.19). When we performed TSA, DPP-4 inhibitors were still not associated with pancreatic cancer (Peto odds ratio 0.66; 95% CI 0.36–1.19), and the number of randomised patients for this outcome surpassed the futility boundary (Fig. 2B – TSA for pancreatic cancer). Meta-regression did not show an interference of study duration with the outcome (p = 0.867; 8 studies included) (Supplemental Material).

(A) Forest plot for association between DPP-4 inhibitors and pancreatic cancer; (B) TSA for pancreatic cancer.
DPP-4 inhibitors and acute pancreatitis
There were 64 events of acute pancreatitis in the DPP-4 inhibitor group and 39 events in the control group. DPP-4 inhibitors were associated with an increased risk of acute pancreatitis in direct meta-analysis (Peto odds ratio 1.72; 95% CI 1.18–2.53; Supplemental Material) and with an absolute risk difference of 0.1% (representing a number needed to harm (NNH) of 1066). Mantel-Haenszel analysis showed comparable results (1.52; 95% CI 1.05–2.18). As we aimed to be conservative, TSA was performed to assess whether there was enough information to reach a definite conclusion regarding the association between DPP-4 inhibitors and acute pancreatitis. For this outcome, the number of patients evaluated (n = 59,404) did not reach the optimal sample size (n = 140,665), and the boundaries of benefit, harm and futility were not crossed (Peto odds ratio 1.34; 95% CI 1.00–1.79). In meta-regression, no interference of study duration with acute pancreatitis was seen (p = 0.252; 25 studies included).
Discussion
The results of the present review indicate that the use of DPP-4 inhibitors is not associated with increased risk for pancreatic cancer. Furthermore, the TSA meta-analysis confirmed that the number of patients available was enough to reach this conclusion. There seemed to be an association between the use of DPP-4 inhibitors and acute pancreatitis, although the number of randomised patients was not sufficient for a firm conclusion and the estimated risk of acute pancreatitis is small (one patient in 1066 patients treated with DPP-4 inhibitors).
Concern regarding the association between DPP-4 inhibitor use and pancreatic cancer was raised after a review of cases reported by the FDA2. Other studies have suggested an association between DPP-4 inhibitor use and pancreatic cancer4,5, but there is still an ongoing debate on this topic. Additionally, several observational studies have explored the association between DPP-4 inhibitors and pancreatitis16,17. However, owing to study design characteristics, the results may be affected by selection and confounding biases. As there are a great number of randomised trials evaluating these medications, a systematic review and meta-analysis of these studies is recommended to properly address this clinical question.
Before this review, three other meta-analyses evaluated the association between clinical use of DPP-4 inhibitors and acute pancreatitis. The first one7 did not find an association between use of DPP-4 inhibitors and acute pancreatitis; however, this review included not only randomised trials but also prospective and retrospective observational cohort studies. Most importantly, the events were not adjudicated. The other two1,3 found an increased risk of acute pancreatitis in patients treated with DPP-4 inhibitors; however, they included only three large cardiovascular randomised trials, namely, EXAMINE, SAVOR-TIMI 53 and TECOS18,19,20. In these trials, a specialised committee adjudicated the diagnosis of acute pancreatitis. None of these reviews performed TSA to evaluate whether the results were definitive, and, more importantly, none of them evaluated the risk of pancreatic cancer associated with use of DPP-4 inhibitors.
Our study adds new information regarding this point. It included all randomised trials with DPP-4 inhibitor use that lasted for at least 24 weeks and, through TSA meta-analysis, evaluated whether the number of cases was sufficient to support the conclusions. There was a small risk of acute pancreatitis, such that it would be necessary to treat 1066 patients to have one case of acute pancreatitis, but the number of patients included in the meta-analysis was not sufficient to support this conclusion. Notably, owing to the large number of diabetic patients using DPP-4 inhibitors worldwide, a great number of cases of acute pancreatitis might be prevented by taking into account pre-existing risk factors for acute pancreatitis, such as gallstones and hypertriglyceridaemia, when considering whether to prescribe this type of medication.
On the other hand, GLP-1 agonist use is not associated with an elevated risk of acute pancreatitis, as recently revealed by a meta-analysis from Storgaard et al.21. Receptors for GLP-1 are largely found in the pancreatic ducts and the pancreatic islets. Acinar and duct cells respond to GLP-1 therapy with proliferation22,23. A previous study in rats exposed to sitagliptin reported haemorrhagic pancreatitis in one rat and acinar-to-ductal metaplasia in others24. Therefore, the association between incretins and acute pancreatitis is biologically plausible. However, it remains unclear why DPP-4 inhibitors are associated with pancreatitis and GLP-1 agonists are not21.
Regarding pancreatic cancer, no association between use of gliptins and pancreatic cancer was observed, and TSA meta-analysis showed that there were enough patients randomised for this observation.
The main limitation of our meta-analysis was the duration of the trials (mean of 63.5, minimum and maximum of 24 and 260 weeks), which may be insufficient to evaluate the development of pancreatic cancer. We tried to overcome this limitation by including study duration as a covariate in the meta-regression, and this variable did not have an influence on the outcome. However, we must consider that this analysis might have low power owing to the number of included trials. Another limitation is the criteria used for diagnosis of acute pancreatitis in trials. In adjudicated trails, the diagnosis was confirmed by an adjudication committee and the criteria used were clearly described. However, in non-adjudicated trials, the criteria used are less straightforward. Nonetheless, restricting the analysis to adjudicated studies did not change the results. Furthermore, owing to the design of the present study, we were not able to explore whether there is a specific subgroup of diabetic patients with increased susceptibility to acute pancreatitis. The included trials did not describe the risk factors for this complication, such as hypertriglyceridaemia, alcohol consumption, and previous history of cholelithiasis. The only factor classically associated with acute pancreatitis that was mentioned was smoking status, which was similar in the intervention and control groups.
Finally, there is enough information to suggest a lack of association between the use of DPP-4 inhibitors and pancreatic cancer, but not acute pancreatitis. The latter seems to be a continued concern, and additional study data are needed. Despite this uncertainty, the apparent risk is small.
References
Tkáč, I. & Raz, I. Combined Analysis of Three Large Interventional Trials With Gliptins Indicates Increased Incidence of Acute Pancreatitis in Patients With Type 2 Diabetes. Diabetes Care, https://doi.org/10.2337/dc15-1707 (2016).
Elashoff, M., Matveyenko, A. V., Gier, B., Elashoff, R. & Butler, P. C. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 141, 150–156, https://doi.org/10.1053/j.gastro.2011.02.018 (2011).
Roshanov, P. S. & Dennis, B. B. Incretin-based therapies are associated with acute pancreatitis: Meta-analysis of large randomized controlled trials. Diabetes Res Clin Pract 110, e13–17, https://doi.org/10.1016/j.diabres.2015.10.014 (2015).
Butler, A. E. et al. Marked expansion of exocrine and endocrine pancreas with incretin therapy in humans with increased exocrine pancreas dysplasia and the potential for glucagon-producing neuroendocrine tumors. Diabetes 62, 2595–2604, https://doi.org/10.2337/db12-1686 (2013).
Engel, S. S., Round, E., Golm, G. T., Kaufman, K. D. & Goldstein, B. J. Safety and tolerability of sitagliptin in type 2 diabetes: pooled analysis of 25 clinical studies. Diabetes Ther 4, 119–145, https://doi.org/10.1007/s13300-013-0024-0 (2013).
Buse, J. B. et al. Pancreatic Safety of Sitagliptin in the TECOS Study. Diabetes Care 40, 164–170, https://doi.org/10.2337/dc15-2780 (2017).
Li, L. et al. Incretin treatment and risk of pancreatitis in patients with type 2 diabetes mellitus: systematic review and meta-analysis of randomised and non-randomised studies. BMJ 348, g2366 (2014).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G. & Group, P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
Robinson, K. A. & Dickersin, K. Development of a highly sensitive search strategy for the retrieval of reports of controlled trials using PubMed. Int J Epidemiol 31, 150–153 (2002).
Standards of Medical Care in Diabetes. Summary of Revisions. Diabetes Care 39(Suppl 1), S4–5, https://doi.org/10.2337/dc16-S003 (2016).
Higgins, J. P. T. & Green, S. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration (2011).
Higgins, J. P. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928 (2011).
Guyatt, G. H. et al. Incorporating considerations of resources use into grading recommendations. Bmj 336, 1170–1173, https://doi.org/10.1136/bmj.39504.506319.80 (2008).
Wetterslev, J., Thorlund, K., Brok, J. & Gluud, C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol 61, 64–75, https://doi.org/10.1016/j.jclinepi.2007.03.013 (2008).
Thorlund, K. et al. User manual for Trial Sequential Analysis (TSA). Copenhagen Trial Unit, Centre for Clinical Intervention Research, Copenhagen, Denmark, 1–115 (2011).
Garg, R., Chen, W. & Pendergrass, M. Acute pancreatitis in type 2 diabetes treated with exenatide or sitagliptin: a retrospective observational pharmacy claims analysis. Diabetes Care 33, 2349–2354, https://doi.org/10.2337/dc10-0482 (2010).
Sudhakaran, C., Kishore, U., Anjana, R. M., Unnikrishnan, R. & Mohan, V. Effectiveness of sitagliptin in asian Indian patients with type 2 diabetes-an Indian tertiary diabetes care center experience. Diabetes Technol Ther 13, 27–32, https://doi.org/10.1089/dia.2010.0120 (2011).
White, W. B. et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 369, 1327–1335, https://doi.org/10.1056/NEJMoa1305889 (2013).
Scirica, B. M. et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 369, 1317–1326, https://doi.org/10.1056/NEJMoa1307684 (2013).
Green, J. B. et al. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 373, 232–242, https://doi.org/10.1056/NEJMoa1501352 (2015).
Storgaard, H., Cold, F., Gluud, L. L., Vilsbøll, T. & Knop, F. K. Glucagon-like peptide-1 receptor agonists and risk of acute pancreatitis in patients with type 2 diabetes. Diabetes Obes Metab 19, 906–908, https://doi.org/10.1111/dom.12885 (2017).
Butler, P. C., Elashoff, M., Elashoff, R. & Gale, E. A. A critical analysis of the clinical use of incretin-based therapies: Are the GLP-1 therapies safe? Diabetes Care 36, 2118–2125, https://doi.org/10.2337/dc12-2713 (2013).
Perfetti, R., Zhou, J., Doyle, M. E. & Egan, J. M. Glucagon-like peptide-1 induces cell proliferation and pancreatic-duodenum homeobox-1 expression and increases endocrine cell mass in the pancreas of old, glucose-intolerant rats. Endocrinology 141, 4600–4605, https://doi.org/10.1210/endo.141.12.7806 (2000).
Matveyenko, A. V. et al. Beneficial endocrine but adverse exocrine effects of sitagliptin in the human islet amyloid polypeptide transgenic rat model of type 2 diabetes: interactions with metformin. Diabetes 58, 1604–1615, https://doi.org/10.2337/db09-0058 (2009).
Acknowledgements
This work was funded by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) n° 307015/2010-6 and FIPE – Fundo de Incentivo à Pesquisa do Hospital de Clínicas de Porto Alegre.
Author information
Authors and Affiliations
Contributions
L.C.P. retrieved the full texts, extracted the data, performed statistical analysis, wrote the first draft of the manuscript and revised the final version; D.V.R. retrieved the full texts, extracted the data, and revised the final version of the manuscript; S.S.B. retrieved the full texts, extracted the data and revised the final version of the manuscript; C.B.L. revised the final version of the manuscript; J.L.G. conceived of the idea for the study and revised the final version of the manuscript. L.C.P. is the guarantor for the contents of the article, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing Interests
J.L.G. reports grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) during the conduct of the study; the sponsor had no interference on data extraction, analyses or manuscript writing. L.C.P., D.V.R., S.S.B. and C.B.L. have declared that no competing interests exist.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pinto, L.C., Rados, D.V., Barkan, S.S. et al. Dipeptidyl peptidase-4 inhibitors, pancreatic cancer and acute pancreatitis: A meta-analysis with trial sequential analysis. Sci Rep 8, 782 (2018). https://doi.org/10.1038/s41598-017-19055-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-017-19055-6
This article is cited by
-
Insulin resistance and cancer: molecular links and clinical perspectives
Molecular and Cellular Biochemistry (2025)
-
Insights on metabolic connections and interplay between cancer and diabetes: role of multi-target drugs
Discover Medicine (2025)
-
Therapie des Typ-2-Diabetes
Die Diabetologie (2024)
-
Therapie des Typ-2-Diabetes
Die Diabetologie (2023)
-
The Current Place of DPP4 Inhibitors in the Evolving Landscape of Type 2 Diabetes Management: Is It Time to Bid Adieu?
American Journal of Cardiovascular Drugs (2023)

Natalia
24 weeks is too short time for observation, even 24 months would be too short considering that DM2 patients get the medication for decades