
Abstract
This study aimed to investigate the effect of age in patients with chronic rhinosinusitis with nasal polyp (CRSwNP). 269 patients were divided into eosinophilic and non-eosinophilic groups based on tissue eosinophilia, defined by eosinophils accounting for more than 20% of the total inflammatory cells. Patients were then further divided into younger and older groups based on the age of 35 years. Clinical characteristics including blood eosinophil, Lund Mackay score, and modified Lund-Kennedy (mLK) scores were compared. Levels of 14 cytokines from nasal tissues of an additional 78 patients were analyzed. Tissue eosinophilia was significantly associated with age and the proportion of non-eosinophilic CRSwNP was significantly higher in younger patients as compared to older patients (79.2% vs 56.6%). There was no difference in clinical characteristics and cytokine levels between the younger and older patients with eosinophilic CRSwNP. In contrast, in patients with non-eosinophilic CRSwNP, younger patients had significantly lower preoperative blood eosinophils and higher mLK scores at three and six months, postoperatively, compared to older patients. Alpha-1 antitrypsin and IL-5 levels were significantly lower in younger patients than in older patients in non-eosinophilic CRSwNP. This study suggests a potential association between age, non-type 2 inflammation and treatment outcome in CRSwNP.
Similar content being viewed by others


Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a common inflammatory upper airway disorder that affects approximately 1–4% of the population worldwide1,2. A significant proportion of patients require surgical treatment, such as functional endoscopic sinus surgery, which is the current standard. However, CRSwNP is a heterogeneous disorder that is composed of many disease subtypes. Patients with tissue eosinophilia and high IL-5 levels have a higher prevalence of comorbid asthma and difficult-to-treat cases1,3,4,5. For difficult-to-treat cases, additional surgical procedures, or medical treatment, such as biologics, may be required6,7,8. Therefore, it is important to identify patients who may require additional therapy in conjunction with standard care. The Japanese Epidemiology Survey of Refractory Eosinophilic Chronic Rhinosinusitis Study (JESREC) demonstrated that tissue eosinophilia is an important marker for polyp recurrence9. This study proposes a novel scoring system using routinely available clinical markers. A high JESREC score indicates the presence of eosinophilic CRS, and patients are expected to have higher recurrence rates after standard surgical treatment.
Non-eosinophilic polyps are diagnosed in a significant proportion of Asian populations. Studies have demonstrated refractory cases among patients with non-eosinophilic polyps that may not be reliably predicted by the JESREC scoring system4,10. Very little is known about the risk factors associated with disease refractoriness in non-eosinophilic polyps.
We previously employed unsupervised cluster analysis to categorize heterogeneous CRSwNP subtypes using routinely available clinical markers. Our previous studies have shown that treatment outcomes can vary with the age of patients with non-eosinophilic polyps11. Patients aged less than 35 years tended to have worse outcomes, as manifested by higher revision surgery rate. Therefore, age may be an important clinical factor associated with treatment outcomes in CRSwNP. The goal of this study was to evaluate the association between age and the clinical and immunological parameters of CRSwNP.
Materials and methods
Study population
This study retrospectively analyzed the medical records of patients with CRSwNP who underwent bilateral functional endoscopic sinus surgery (FESS) at Seoul National University Bundang Hospital (Bundang, South Korea) between June 2017 and January 2020; a period that had not been previously analyzed. Patients of all ages with refractory primary bilateral CRSwNP were analyzed. Diagnosis of CRSwNP was made based on the criteria described by the European position paper on rhinosinusitis with nasal polyps12. Patients who had undergone FESS before June 2017 or who had been treated with preoperative systemic corticosteroids within the four‐week surgery period were excluded. Patients with unilateral disease, fungal disease, antrochoanal polyps, cystic fibrosis, primary ciliary dyskinesia, or other tumorous conditions, such as sinonasal inverted papilloma, were excluded. Only patients of Asian ethnicity were included in the study.
Two independent cohorts of patients were analyzed. The first cohort (cohort 1) comprised 269 patients with primary bilateral CRSwNP who underwent FESS during the study period and had been followed up for at least three months after the surgery. The second cohort (cohort 2) comprised 65 primary bilateral CRSwNP patients and 13 controls, both of which underwent immunological analysis for tissue cytokine levels and evaluation of clinical characteristics. The controls were patients who underwent endoscopic skull base surgery without any evidence of sinonasal disease. All subjects who underwent tissue analysis provided written informed consent for participation in the study. This study was approved by the Institutional Review Board of the Seoul National University Bundang Hospital (B-2009–636-302). All methods were performed in accordance with the relevant guidelines and regulations.
Analysis of the perioperative clinical parameters
For all patients, Lund-Mackay (LM) scoring was performed using a CT scan13. This grades each sinus separately on the 0 to 2 scale depending on whether the sinuses are clear, partially, or completely opacified. The sum of the LM scores for the right and left nasal cavities were then, calculated. The presence of asthma was assessed by the institution's allergist after thorough review of previous medical history and lung function tests: spirometry, methacholine challenge test, or bronchodilator response test. A complete blood cell count with differential was performed within four weeks prior to surgery to check the peripheral blood eosinophil count. Nasal polyp tissues were obtained during FESS for histopathological analysis. Postoperative specimens were reviewed by pathologists at our institution. Pathological findings were reported as “eosinophilic” or “non‐eosinophilic.” Tissue eosinophilia was considered when eosinophils accounted for more than 20% of the total inflammatory cells at 400X magnification14. Nasal polyps were defined as eosinophilic or non-eosinophilic according to tissue eosinophilia status. Smoking status was also collected during the study period and was reported as never smoker or current/ex-smoker.
Patient classification
Patients were classified according to their tissue eosinophilia status. They were further divided as younger or older by the age above or below 35 years; NE-Y (non-eosinophilic CRSwNP with younger age), NE-O (non-eosinophilic CRSwNP with older age), E-Y (eosinophilic CRSwNP with younger age) and E-O (eosinophilic CRSwNP with older age). The cutoff value of 35 years was based on a previously described decision tree, which was constructed after cluster analysis using a patient's clinical features, including age, peripheral blood eosinophil, tissue eosinophilia, Lund‐Mackay computed tomography (CT) scores, ratio of the CT scores for the ethmoid sinus and maxillary sinus, and comorbid asthma11.
Cytokine measurement from tissue homogenates
Tissues were harvested from nasal polyps in CRSwNP patients during FESS and the ethmoid sinus mucosa in the controls without any evidence of sinonasal disease during the endoscopic endonasal approach for pituitary adenoma or skull base tumors. Tissue samples were snap-frozen in liquid nitrogen and stored at − 80 °C, thawed at room temperature, and homogenized with a mechanical homogenizer. After homogenization, the suspensions were centrifuged at 4000 rpm for 20 min at 4 °C, and the supernatants were separated and stored at 80° C for further analysis. The samples were thawed and vortexed at room temperature to ensure adequate mixing. Protein concentrations of tissue extracts were determined using Pierce 660 nm Protein Assay Kits (Thermo Fisher Scientific Inc., Rochester, NY, USA). Tissue homogenates were then assayed using the multiple cytokine analysis kits: macrophage inflammatory protein (MIP)-1β/CCL4, interferon (IFN)-γ, interleukin (IL)-1β/IL-1F2, IL-5, IL-6, IL-8/CXCL8, IL-12 (p70), IL-33, tumor necrosis factor (TNF)-α (Luminex Human Magnetic Assay (10-Plex) (LXSAHM-10; R&D Systems, Minneapolis, MN, USA), myeloperoxidase (MPO) (Luminex Human Magnetic Assay (LXSAHM-01); R&D Systems), TGFβ1 (TGFBMAG-64K-01; Millipore, Billerica, MA, USA), α1 antitrypsin (A1AT) (HNDG2MAG-36K-01; Millipore), human neutrophil elastase (HNE) (HSP3MAG-63K-01; Millipore), and IL-22 (HTH17MAG-14K-01; Millipore). Data were collected using a Luminex 100 reader (Luminex, Austin, TX, USA). Data analysis was performed using MasterPlex QT version 2.0 software (MiraiBio, Alameda, CA, USA). All assays were performed in duplicate, according to the manufacturer’s protocol. All protein levels in the tissue homogenates were normalized to total protein concentration. The sensitivity for each cytokine were as follows :macrophage : MIP-1β/CCL4 (5.8 pg/ml), IFN-γ (0.4 pg/ml), IL-1β/IL-1F2 (0.8 pg/ml), IL-5 (0.5 pg/ml), IL-6 (1.7 pg/ml), IL-8/CXCL8 (1.8 pg/ml), IL-12 (p70) (20.2 pg/ml), IL-33 (1.8 pg/ml), TNF-α (1.2 pg/ml), MPO (26.2 pg/ml), TGFβ1 (11.4 pg/ml), α1 anti-trypsin (0.085 ng/ml), human neutrophil elastase (HNE) (6.2 pg/ml) and IL-22 (0.032 pg/ml). Values less than the detection limit were considered as half of the lower limit5.
Evaluation of treatment outcomes
After standard FESS, oral antibiotics were routinely prescribed for five-seven days, and intranasal corticosteroid spray was used afterward. Patients were encouraged to perform saline nasal irrigation for three months. Endoscopic findings were evaluated three months, six months, and one year postoperatively using a modified Lund-Kenney (mLK) score15 from the physician’s report. The mLK scores assesses edema, discharge on the 0 to 2 scale for each parameter, for a total possible score of 6. The scores on both sides were then summed. Short courses of antibiotics or systemic corticosteroids were prescribed when necessary. In such cases, endoscopic examinations were re-evaluated after two weeks and were used for analysis.
Statistical analysis
Differences between groups were analyzed using the Kruskal–Wallis tests with Dunn multiple comparisons tests or Mann–Whitney U-test, after confirmation of a non-parametric distribution, by the Shapiro tests for continuous variables. To reduce the false discovery rate, the method of Benjamini and Yekutieli was used16 Chi-square or Fisher’s exact test tests were performed for categorical variables. Results are presented as mean ± standard deviation (SD) or median with interquartile range (IQR). Spearman correlation coefficients were determined to assess the relationship between cytokine levels and age. Cytokine data that significantly correlated with age were displayed using locally weighted scatterplot smoothing regression curve by R 3.4.2 software (R Foundation for Statistical Computing; http://www.r-project.com). Statistical analyses were performed using IBM SPSS Statistics version 22.0 software (; IBM Corp., Armonk, NY, USA) and R 3.4.2 software. Statistical significance was set at p < 0.05.
Results
General characteristics
Cohort 1 included 106 patients with eosinophilic CRSwNP and 163 patients with non-eosinophilic CRSwNP. Among patients with eosinophilic CRSwNP, 10 (9.4%) were younger (E-Y) and 96 (90.6%) were older (E-O). Of the non-eosinophilic CRSwNP patients, 38 (23.3%) were of younger age (NE-Y) and 125 (76.7%) were of older age (NE-O). There was a strong association between age group and tissue eosinophilia status (p = 0.004). The prevalence of non-eosinophilic CRSwNP was significantly higher in younger patients than in older patients (79.2% vs. 56.6%) (Fig. 1).

Distribution of eosinophilic and non-eosinophilic chronic rhinosinusitis with nasal polyp (CRSwNP) among younger (< 35 years) and older age groups (≥ 35 years).
The clinical characteristics of cohort 1 are summarized in Table 1. Comorbid asthma (20.8% vs 11.7%, p = 0.042) and blood eosinophils (8.0 ± 4.1% vs 4.9 ± 4.7%, p < 0.001) were significantly higher in patients with eosinophilic CRSwNP compared to that of non-eosinophilic CRSwNP. There was no significant difference in clinical characteristics between E-Y and E-O. However, patients with NE-O had a significantly higher level of blood eosinophils compared to that with NE-Y (5.3 ± 5.0% vs 3.5 ± 3.2%, p = 0.016). Other clinical characteristics were not significantly different between NE-Y and NE-O.
Treatment outcomes
When it comes to treatment outcome, post-operative mLK scores three months were significantly lower in patients with eosinophilic CRSwNP compared to those with non-eosinophilic CRSwNP (1.1 ± 1.2 vs 1.9 ± 2.0, p = 0.008). However, six months and twelve months post-operative mLK scores were not significantly different.
In eosinophilic CRSwNP, there was no significant difference in outcomes between E-Y and E-O. However, in non-eosinophilic CRSwNP, compared to NE-O, NE-Y had higher mLK scores measured at three months (1.5 ± 1.7 vs. 2.9 ± 2.5, respectively, p < 0.001) and six months (1.5 ± 1.8 vs. 2.5 ± 1.9, respectively, p = 0.045) postoperatively. NE-Y had a significantly higher mLK score 3 months postoperatively compared to E-O (p < 0.001). (Table 1).
Immunological characteristics
Cohort 2 comprised 39 patients with eosinophilic CRSwNP, 26 patients with non-eosinophilic CRSwNP and 13 controls. Clinical characteristics of cohort 2 are described in S1 Table. Age, male to female ratio, and LM scores were not significantly different between patients with eosinophilic and non-eosinophilic CRSwNP. Comorbid asthma (p = 0.042) and blood eosinophils (p < 0.001) were significantly higher in patients with eosinophilic CRSwNP compared to those with non-eosinophilic CRSwNP or controls.
A heatmap of protein concentrations among patient groups is shown in Fig. 2. Grossly looking, control tissue, eosinophilic polyp, and non-eosinophilic polyp are clearly separated. Cytokine levels of TGF-ß, IL-1ß, IL-33, IL-5, IL-6, IL-8, and TNF-α were significantly different among groups. Post hoc comparison revealed a significant difference in the levels of IL-1ß and IL-5, IL-6, IL-8, and TNF-α between eosinophilic and non-eosinophilic polyp (S2 Table).

Heatmap of protein concentrations among patient classes. The color bar presents Z-scores of tissue concentration for each measured cytokine.
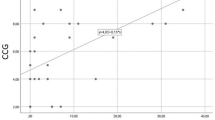
Among patients with eosinophilic CRSwNP,6 patients (15.4%) were younger (E-Y) and 33 patients (84.6%) were older (E-O), while in patients with non-eosinophilic CRSwNP, 10 (38.5%) were younger (NE-Y) and 16 (61.5%) were older (NE-O). Cytokine measurements were not statistically different between E-Y and E-O (S3 Table). In cases of non-eosinophilic polyps, A1AT and IL-5 levels were significantly lower in NE-Y than in NE-O (Fig. 3). The cytokine measurements of non-eosinophilic polyps are summarized in Table 2. Of the 14 cytokines, IL-5 showed a positive correlation with age (Spearman's rho = 0.523, p = 0.006, Fig. 4) in non-eosinophilic polyps. However, there was no significant relationship between cytokine levels and age in the eosinophilic polyp group (S4 Table).

Inflammatory mediators in NE-O and NE-Y. Data were evaluated by Kruskal–Wallis test and Dunn multiple comparison test. Bars indicate p < 0.05 after post hoc Dunn’s test. NE-Y: Non-eosinophilic polyp with age under 35 years, NE-O: Non-eosinophilic polyp with age over 35 years, A1AT: Alpha 1 antitrypsin.

Correlation bewteen tissue IL-5 level and age in patients with non-eosinophilic chronic rhinosinusitis with nasal polyp.
There were no significant differences in clinical characteristics and treatment outcomes between NE-Y and NE-O nor E-Y and E-O in cohort 2 (data not shown).
Discussion
In current study, patients were first categorized according to tissue eosinophilia, defined as eosinophils accounting for more than 20% of total inflammatory cells when viewed at high magnification. Although this method is only semiquantitative and may depend on the pathologist’s subjective judgment, it is intuitive and swift. In this study, we analyzed our results from an immunological perspective with a panel of multiple cytokines. Eosinophilic polyps had elevated levels of IL-5 (type 2 inflammation), whereas non-eosinophilic polyps had elevated levels of IL-1b, IL-6, IL-8, and TNF-α (non-type 2 inflammation). Therefore, defining tissue eosinophilia based on histological analysis seems to incorporate immunological characteristics as well.
Although immunologically distinct, tissue eosinophilia status alone does not seem to incorporate prognosis, since treatment outcomes of patients with eosinophilic CRSwNP were similar to those with non-eosinophilic CRSwNP14. Therefore, for Koreans population, the dichotomous classification into eosinophilic and non-eosinophilic subtypes is not enough and subclassification beyond tissue eosinophilia is necessary. Our previous study demonstrated that several phenotypes of CRSwNP can be classified using routinely available clinical markers. According to our previous study, among patients with non-eosinophilic polyps, patients less than 35 years of age had worse outcomes compared to patients older than 35 years of age. Therefore, the goal of this study was to validate whether age can be used as a factor that could clinically and immunologically differentiate patients with CRSwNP.
First, age seems to be associated with the tissue eosinophilia status. In patients less than 35 years of age, almost 80% were non-eosinophilic CRSwNP suggesting that CRSwNP in younger age is more associated with non-type 2 inflammation. In addition, within patients with non-eosinophilic CRSwNP, younger patient (NE-Y) seems to be clinically and immunological distinct compared to older patients (NE-O).
Compared to NE-O, NE-Y was characterized by lower levels of IL-5 and A1AT. This suggests an age-dependent association for IL-5 and A1AT levels. Although measured from healthy adults, serum concentrations of A1AT is known to increase with age17. Type 2 mediators, including IL-5 and chemokine (CC motif) ligand 24 (CCL-24), have also been shown to increase with age in patients with non-eosinophilic CRSwNP18. An unpublished study from Korea demonstrated the duration of the disease in non-eosinophilic CRSwNP is correlated with the tissue level of IL-519 suggesting that prolonged disease duration in NE-O may explain higher level of IL-5. However, this must be further validated as we have not measured disease duration in the current study.
From clinical perspective, blood eosinophils were significantly lower in NE-Y than in NE-O which can be partially explained by the higher level of IL-5 in NE-O patients. In addition, mLK scores measured at three months and six months postoperatively were significantly higher in NE-Y patients than in NE-O patients. As mLK score reflects disease outcome after the surgery15, NE-Y patients had worse postoperative short-term outcomes compared to NE-O patients, which is in accordance with the results of our previous study11. Therefore, decreased levels of IL-5 and A1AT in the tissue samples and worsening short-term outcomes result in NE-Y being a distinguishing phenotype in CRSwNP.
In the current study, patients were treated with short courses of systemic corticosteroid therapy when necessary. As blood or tissue eosinophil is known to be associated with corticosteroid response20,21,22, better endoscopic scores in NE-O patients than in NE-Y patients may have been derived from higher blood eosinophil in NE-O patients. Similarly, this may also explain a significantly lower endoscopic scores in patients with eosinophilic CRSwNP than in patients with non-eosinophilic CRSwNP at post operative 3 months. Poor treatment outcomes may also be explained by the low levels of IL-5 and A1AT in NE-Y. In non-eosinophilic CRSwNP, one of the possible factors responsible for disease refractoriness is tissue neutrophilia4. IL-5, which is a typical type 2 inflammatory cytokine, is known to suppress neutrophil activity23. Α1ΑΤ exerts its anti-inflammatory action by inhibiting inflammatory HNE, a serine protease stored in the azurophilic granules of neutrophils and released during neutrophil degranulation24. Low Α1ΑΤ is known to be associated with disease refractoriness and tissue neutrophilia in nasal polyps10. Therefore, characteristics of NE-Y may be associated with increased neutrophilic inflammation. However, this needs to be further evaluated since there was no significant difference in expression level neutrophilic markers, such as MPO, HNE, and IL-8 between NE-Y and NE-O.
There was a significant increase in proportion of eosinophilic CRSwNP in older patients compared to younger patients (20.8% to 43.4%). This may also mean that type 2 inflammation is more associated with older age that there is a higher proportion of eosinophilic CRSwNP compared to younger patients. Age association to eosinophilic CRSwNP can be partially explained by physiological and functional changes in the nasal mucosa, epithelial barrier dysfunction, or interaction with microbiome manifested as IgE responses to Staphylococcal enterotoxin B which is also known to be associated with adult onset asthma25,26,27.
However, there were no significant clinical or immunological differences between young and old-aged eosinophilic polyps. Our study showed somewhat contradictory results from other studies. Other studies had shown that elderly patients with CRS showed significantly higher CT scores, which were associated with nasal polyps28,29. From immunological perspective, age affected tissue cytokine profile differently in eosinophilic polyps. Among eosinophilic polyps, levels of IL-17 and chemokine C-X-C motif ligand (CXCL1), both of which are type 3 cytokines related to neutrophilic inflammation, positively correlated with age30. The discrepancy between current study and others may be due to arbitrarily determined age cutoff values among patients with eosinophilic polyps and the limited number of patients, especially those with younger age.
Our study has several limitations. This is not a longitudinal study and demonstrates only a cross-sectional association of age and disease endotype. Therefore, our study does not suggest that disease endotype may change over time as demonstrated in other study31. Postoperative endoscopy scores were the only outcome measured in our study. Since the endoscopy scores tend to reach a nadir around three to six months postoperatively and rise afterward32, a longer follow-up duration is necessary to observe differences between the patient groups. Also, as this is a single center study, there may be a risk of selection bias. Therefore, a larger cohort, perhaps a multicenter study, with long-term follow-up is warranted.
In summary, age is associated the tissue eosinophilia status in CRSwNP. Especially, for younger patients, there was a significantly higher proportion of non-eosniphilic CRSwNP. Age appears to have a significant effect in patients with non-eosinophilic CRSwNP. Younger patients had worse treatment outcomes and were characterized by low IL-5 and A1AT compared to older patients with non-eosinophilic CRSwNP. Therefore, age may be an important parameter for phenotyping CRSwNP.
Data availability
The data cannot be publicized for legal reasons in Korea.
Change history
17 February 2023
A Correction to this paper has been published: https://doi.org/10.1038/s41598-023-30110-3
References
Ahn, J., Kim, J., Lee, C. H. & Rhee, C. Prevalence and risk factors of chronic rhinosinusitus, allergic rhinitis, and nasal septal deviation: Results of the Korean national health and nutrition survey 2008–2012. JAMA Otolaryngol. Head Neck Surg. 142, 162–167 (2016).
Larsen, K. & Tos, M. The estimated incidence of symptomatic nasal polyps. Acta Otolaryngol. 122, 179–182 (2002).
Calus, L. et al. Twelve-year follow-up study after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Clin. Transl. Allergy 9, 30 (2019).
Liao, B. et al. Multidimensional endotypes of chronic rhinosinusitis and their association with treatment outcomes. Allergy 73, 1459–1469 (2018).
Tomassen, P. et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 137, 1449–1456 (2016).
Alsharif, S. et al. Endoscopic sinus surgery for type-2 CRS wNP: An endotype-based retrospective study. Laryngoscope 129, 1286–1292 (2019).
Bachert, C. et al. Biologics for chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 145, 725–739 (2020).
Morrissey, D. K., Bassiouni, A., Psaltis, A. J., Naidoo, Y. & Wormald, P. J. Outcomes of modified endoscopic Lothrop in aspirin-exacerbated respiratory disease with nasal polyposis. Int. Forum Allergy Rhinol. 6, 820–825 (2016).
Tokunaga, T. et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC Study. Allergy 70, 995–1003 (2015).
Kim, D. K. et al. Elastase-positive neutrophils are associated with refractoriness of chronic rhinosinusitis with nasal polyps in an Asian population. Allergy Asthma Immunol. Res. 12, 42–55 (2020).
Kim, J. W. et al. Unsupervised cluster analysis of chronic rhinosinusitis with nasal polyp using routinely available clinical markers and its implication in treatment outcomes. Int. Forum Allergy Rhinol. 9, 79–86 (2019).
Fokkens, W. J. et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 58, 1–464. https://doi.org/10.4193/Rhin20.600 (2020).
Lund, V. J. & Kennedy, D. W. Staging for rhinosinusitis. Otolaryngol. Head Neck Surg. 117, S35–S40 (1997).
Kim, S. Y., Park, J. H., Rhee, C. S., Chung, J. H. & Kim, J. W. Does eosinophilic inflammation affect the outcome of endoscopic sinus surgery in chronic rhinosinusitis in Koreans?. Am. J. Rhinol. Allergy 27, e166–e169 (2013).
Psaltis, A. J., Li, G., Vaezeafshar, R., Cho, K. S. & Hwang, P. H. Modification of the Lund-Kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope 124, 2216–2223 (2014).
Yoav, B. & Daniel, Y. The control of the false discovery rate in multiple testing under dependency. Ann. Stat. 29, 1165–1188. https://doi.org/10.1214/aos/1013699998 (2001).
Paczek, L., Michalska, W. & Bartlomiejczyk, I. Trypsin, elastase, plasmin and MMP-9 activity in the serum during the human ageing process. Age Ageing 37, 318–323. https://doi.org/10.1093/ageing/afn039 (2008).
Ryu, G. et al. Age-associated changes in chronic rhinosinusitis endotypes. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 50, 585–596. https://doi.org/10.1111/cea.13586 (2020).
Kim, D. K. & Kim, D. W. Does inflammatory endotype change in patients with chronic rhinosinusitis?. Allergy Asthma Immunol. Res. 11, 153–155. https://doi.org/10.4168/aair.2019.11.2.153 (2019).
Snidvongs, K. et al. Corticosteroid nasal irrigations after endoscopic sinus surgery in the management of chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2, 415–421. https://doi.org/10.1002/alr.21047 (2012).
Wu, D., Yan, B., Wang, Y., Zhang, L. & Wang, C. Charcot-Leyden crystal concentration in nasal secretions predicts clinical response to glucocorticoids in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 144, 345-348.e348. https://doi.org/10.1016/j.jaci.2019.03.029 (2019).
Hong, H. et al. Sinus computed tomography predicts clinical response to corticosteroids in chronic rhinosinusitis with nasal polyps. Clin. Transl. Allergy 8, 24. https://doi.org/10.1186/s13601-018-0211-1 (2018).
Gorski, S. A. et al. Expression of IL-5 receptor alpha by murine and human lung neutrophils. PLoS ONE 14, e0221113. https://doi.org/10.1371/journal.pone.0221113 (2019).
Janciauskiene, S. et al. The multifaceted effects of alpha1-antitrypsin on neutrophil functions. Front. Pharmacol. 9, 341. https://doi.org/10.3389/fphar.2018.00341 (2018).
Cho, S. H. et al. Age-related increased prevalence of asthma and nasal polyps in chronic rhinosinusitis and its association with altered IL-6 trans-signaling. Am. J. Respir. Cell Mol. Biol. 53, 601–606. https://doi.org/10.1165/rcmb.2015-0207RC (2015).
Song, W. J., Lee, J. H., Won, H. K. & Bachert, C. Chronic rhinosinusitis with nasal polyps in older adults: Clinical presentation, pathophysiology, and comorbidity. Curr. Allergy Asthma Rep. 19, 46. https://doi.org/10.1007/s11882-019-0880-4 (2019).
Song, W. J. et al. Staphylococcal enterotoxin IgE sensitization in late-onset severe eosinophilic asthma in the elderly. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 46, 411–421. https://doi.org/10.1111/cea.12652 (2016).
Cho, S. H. et al. Age-related differences in the pathogenesis of chronic rhinosinusitis. J. Allergy Clin. Immunol. 129, 858-860.e852. https://doi.org/10.1016/j.jaci.2011.12.002 (2012).
Tan, B. K. et al. Incidence and associated premorbid diagnoses of patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 131, 1350–1360. https://doi.org/10.1016/j.jaci.2013.02.002 (2013).
Ryu, G. et al. Immunological characteristics in refractory chronic rhinosinusitis with nasal polyps undergoing revision surgeries. Allergy Asthma Immunol. Res. 11, 664–676. https://doi.org/10.4168/aair.2019.11.5.664 (2019).
Al-Samri, M. T. et al. Variability of sputum inflammatory cells in asthmatic patients receiving corticosteroid therapy: A prospective study using multiple samples. J. Allergy Clin. Immunol. 125, 1161-1163.e1164. https://doi.org/10.1016/j.jaci.2010.02.005 (2010).
Shikani, A. H., Chahine, K. A. & Alqudah, M. A. The rhinotopic protocol for chronic refractory rhinosinusitis: how we do it. Clin. Otolaryngol. 35, 329–332. https://doi.org/10.1111/j.1749-4486.2010.02157.x (2010).
Acknowledgements
This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. NRF-2019R1C1C1009886).
Funding
This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. NRF-2019R1C1C1009886).
Author information
Authors and Affiliations
Contributions
J.-W.K. and S.-W.C. designed the clinical study and drafted main manuscript. S.K.Y., H.W., C.P. and S.A.K. assisted data collection and analyzed data. H.K., T.-B.W., C.-S.R. gave critical revision for important intellectual content. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the spelling of the author Jeong-Whun Kim which was incorrectly given as Jeong-Whum Kim.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, JW., Won, TB., Woo, H. et al. Age related non-type 2 inflammation and its association with treatment outcome in patients with chronic rhinosinusitis with nasal polyp in Korea. Sci Rep 12, 1671 (2022). https://doi.org/10.1038/s41598-022-05614-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-022-05614-z
