
Abstract
Kawasaki disease (KD) is one of the most common vasculitides of early childhood. There are no previous studies on KD in Cyprus. The aim of this study was to evaluate the epidemiology of KD in Cyprus, risk factors for resistance to treatment and the development of cardiac complications. This is a retrospective multicenter study of pediatric patients with KD hospitalized between January 2000 and-December 2019. The data were collected from medical records. A total of 136 patients with KD were included in the study. 83% of patients were < 5 years of age and 10% were < 6 months. Thirty patients (22%) developed coronary artery lesions. Serum sodium ≤ 133 mmol/L, albumin ≤ 3.2 g/dl, ALT ≥ 80 U/L and neutrophils percentage ≥ 80% at diagnosis, were identified as risk factors for resistance to IVIG. Clinical and epidemiological characteristics of KD in Cyprus population were similar to those reported in the literature. Although the majority of cases received appropriate treatment in time, cardiac complications still occurred.
Similar content being viewed by others
Introduction
Kawasaki disease (KD) is one of the most common vasculitides of early childhood and the leading cause of acquired heart disease in children in developed countries1. The majority of patients are younger than 5 years old. KD is very rarely encountered in adults. The disease was initially described by Tomisaku Kawasaki, a Japanese pediatrician, in 19672. Japanese children have been affected more frequently having the highest incidence of the disease which seems to increase over time. Children populations in Korea and Taiwan are following, whereas the incidence in European countries and in the United States of America is much lower3,4. In other countries, the disease incidence remains higher in children with Japanese origin in comparison to the rest of the children population which shows that genetic factors may play an important role in the incidence of disease4. More than fifty years have passed since the disease was first described, yet the disease etiology remains unknown. There are many theories about the pathogenesis of KD, including an unknown infectious triggering factor4.
As a result of the unknown etiology of the disease, diagnosis depends on clinical criteria, which include fever, changes of lips and oral cavity, bilateral conjunctival injection, cervical lymphadenopathy, changes in the extremities and rash. The diagnosis becomes doubtful and challenging in atypical- incomplete cases where not all of the clinical criteria are met. In such cases the use of laboratory tests can be helpful in supporting the diagnosis5.
KD is an acute disease characterized by fever and inflammation of small and medium size arteries. Without treatment, it is a self-limited condition with an average duration of 12 days. However, about 15–25% of those who remain untreated may develop coronary artery lesions. Up to 50% of them may develop transient coronary dilation and approximately 25% may develop more persistent coronary artery abnormalities (CAA’s) such as aneurysms6,7. Other cardiac complications may be pericardial effusion, myocarditis and valvular regurgitation5. Moreover, in patients who receive timely treatment with intravenous immunoglobin (IVIG), only 4% develop cardiac artery abnormalities.
According to American Heart Association (AHA) guidelines, the most appropriate treatment is a single dose of IVIG (2 g/kg), concurrently with acetylsalicylic acid. A percentage of cases, despite this first-line treatment, are unresponsive. An IVIG non-responsive patient is defined as the patient whose fever persists for more than 36 h after the end of IVIG infusion5.
Research on factors associated with non-responsiveness to the administration of initial treatment with IVIG carried out in Japan, showed that non-responsiveness was associated with several parameters such as the young age of patient, the number of days of illness before administration of treatment and laboratory findings recorded before treatment with IVIG, such as high level of C Reactive Protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), percentage of neutrophils in full blood count (FBC), low platelet (Plt) count and serum sodium (Na) before treatment.
CAA’s is the most severe complication of KD. Factors associated with CAA’s in some studies, are the young age and the male gender, the delay of treatment beyond 10 days and non-responsiveness to the initial dose of IVIG. Studies reveal also laboratory parameters associated with the development of CAA’s such as high level of CRP8.
The aim of this retrospective study is to evaluate the burden, epidemiology and clinical characteristics of Kawasaki disease in the Cyprus population between 2000 and 2019. Further to this, risk factors for resistance to treatment and the development of cardiac complications were explored.
Methods
Data sources and collection
Medical records of patients less than 15 years of age, with complete or incomplete KD, hospitalized in Archbishop Makarios Hospital (AMH) and Limassol General Hospital between January 2000 and December 2019 were retrospectively reviewed. As Archbishop Makarios Hospital (our hospital), served as the referral center for Pediatric Cardiology services in all Cyprus, patients from other hospitals in Cyprus, were also referred to our hospital for cardiology assessment. In addition, all severe cases of KD from all Cyprus were referred to AMH for management as it also acts as the tertiary Pediatric referral center in Cyprus. All cases were categorized into complete and incomplete form, according to the American Heart Association Recommendations 20041. The first day of fever was defined as the onset of disease. Initial treatment of KD was the administration of high dose IVIG (2 g/kg) together with high dose aspirin (80-100 mg/kg/d) and when the patient became afebrile for at least two to three days the dose of aspirin was reduced to 3-5 mg/kg/day. Because this study includes cases in a time frame of 20 years, treatment regimen in some cases varied. While the total dose remained the same, in the first years of the study the IVIG was administered over 2- 5 days instead of one day. Patients who remained febrile 36 h after administration of initial IVIG, were defined as IVIG non-responders. Treatment was considered as delayed when the first dose of IVIG was given after the 10th day of illness.
A database was created to include all information regarding cases. This database included demographic, clinical and laboratory as well as outcome data of the patients. Data included age, sex, season of admission, nationality, days of fever before treatment, total days of illness. It contained laboratory values before IVIG treatment (Albumin, Gamma -Glutamyl Transferase (γGT), Hemoglobin (Hb), White Blood Cell count (WBC), Percentage of Neutrophils in FBC, CRP, Erythrocyte Sedimentation Rate (ESR), Na, ALT, AST and the highest number of platelets during the course of illness.
A case of complete KD was defined as the presence of fever longer than 4 days and the presence of 4 out of the 5 clinical features that is changes of lips and oral cavity, bilateral conjunctival injection, cervical lymphadenopathy, changes in the extremities and rash. Based on the AHA guidelines a case of incomplete KD was defined as the child with fever > = 5 days and two or three of the other clinical criteria or infants with fever for at least 7 days duration without other explanation5.
Our group of pediatric cardiologists classified the coronary artery abnormalities according to the AHA guidelines 2004 and updated in 20175 into 4 categories, depending on coronary artery Z-score which was based on assessment of populations of healthy afebrile children:
-
Dilation is defined when Z-score is between 2 and 2,5, or if initially < 2 and then decrease in Z score during follow-up for at least one year.
-
Small aneurysm: ≥ 2,5 to < 5
-
Medium aneurysm: ≥ 5 to < 10, and absolute dimension < 8 mm
-
Large or giant aneurysm: ≥ 10, or absolute dimension ≥ 8 mm
Children with KD were evaluated by Pediatric Cardiology before the initiation of treatment and prior to discharge, during the acute phase. A follow-up echo was performed between 4 to 8 weeks after diagnosis. Time of further reassessments was dependent on echocardiographic findings. In the cases that the z score of inner diameters of coronary arteries decreased by more than 1 during follow-up, then the patient was diagnosed retrospectively as a case of dilation even if the initial measurement was within normal limits.
Ethics approval
Ethical approval was waived by the National Bioethics Committee as it was retrospective, completely anonymized and did not include any personal data.
Statistical analysis
Data were analyzed using the R statistical software version 3.5.19. Package ggplot2 was used for all plots10. Differences in clinical findings between complete and incomplete cases of Kawasaki disease were assessed using a chi-squared test. Blood test results between the two groups were also compared. In order to test whether there was a difference, Student T-test and U-Mann–Whitney were applied in parametric and nonparametric distributions respectively. Normality was tested by means of Shapiro–Wilk test. A p-value less 0.05 was considered statistically significant.
Logistic regression modeling was used to investigate factors associated with (a) resistance to intravenous immunoglobulin and (b) development of coronary artery abnormalities. Univariable analysis of all the factors against each outcome variable using Fisher’s exact test was used to select variables to be considered in the multivariable analysis. Variables with a p-value of less than 0.2 were considered for inclusion in each model. All variable combinations were considered using R package MuMIn11. Multivariable logistic regression models were fit using Firth’s bias reduction method from R package logistf12. Model selection was based on Second-order Akaike Information Criterion (AICc). Models with an AICc within 2 units of the lowest AICc were averaged to give the final model.
Results
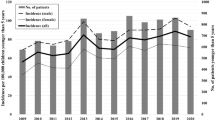
A total of 136 patients with KD were included in the study. Male to female ratio was 1.25:1 and mean age of patients at diagnosis was 2.97 years (ranged from 0.23 to 14.67 years) and the median age 2.29 years. Eighty-three per cent of the patients were under 5 years of age. Only 32 patients (23%) were less than 12 months of age, while 14 children (10%) were younger than 6 months (Fig. 1).

Age distribution of patients with KD.
The majority of the cases were diagnosed during winter and spring months (65%) (p = 0.0006) (Supplementary Fig. S1). The patients were mainly Greek Cypriots (88%).
Overall, 88 cases were classified as complete (69%) and 40 (31%) as incomplete Kawasaki disease. The duration of fever before administration of IVIG treatment was on average 7.2 days with a median of 6. In 17 cases diagnosis was delayed and treatment was started 10 days or more after onset of symptoms, with the longest interval between symptom onset and treatment being 22 days. A small percentage (11%) of children with KD were started on treatment less than 5 days after onset of the disease.
Clinical characteristics
All patients presented with persistent fever for at least 5 days. Overall, changes of lips and/or oral cavity (erythema and cracking of lips, strawberry tongue, erythema of oral and pharyngeal mucosa) were the most common manifestations, seen in 113/127 patients (89%), followed by skin rash in 109/131 cases (83%). This included maculopapular, morbilliform, erythematous or urticarial rash. Bilateral bulbar conjunctival injection without exudates was seen in 103/128 patients (80%). Changes of extremities were detected in 89/126 cases (71%) in this study. Specifically, in early stages of the disease palmar or/and soles edema or/and erythema were noticed, while desquamation of digits developed in the second week of illness. Cervical lymphadenopathy was the least common clinical finding (71/124 cases -57%).
Other clinical findings which do not belong to the main criteria for diagnosis were also observed, particularly gastrointestinal (GI), musculoskeletal and central nervous system symptoms. A total of 60 out of 109 patients (55%) complained about GI symptoms. Diarrhea/abdominal pain/vomiting were the most common features in these patients. Five patients had hepatomegaly, one of them with jaundice (high level of direct bilirubin, acholic stools), and one with ascites. Musculoskeletal symptoms were present in 20/107 (19%). Arthralgia and less commonly arthritis occurred in 10 and 7 patients respectively, in various large joints. Two of these had difficulty standing up. In addition, central nervous system features developed in 15/113 patients (13.3%), extreme irritability being the most frequent symptom, followed by lethargy. Three cases, in which lumbar puncture was done, were diagnosed with aseptic meningitis. Unilateral facial nerve paresis was detected in one patient.
In Table 1 the clinical manifestations in complete vs incomplete cases of KD are compared. There were statistically significant differences in all principal criteria of KD. Changes of lips and/or oral cavity remained the most frequent clinical finding in both complete and incomplete cases.
Laboratory findings
Regarding the laboratory findings, children with complete KD had significantly lower levels of platelets before treatment in comparison to incomplete KD patients (median value 383 vs 453, p = 0.04) and also higher hemoglobin levels (median value 10.5 g/l vs 9.8 g/l, p = 0.038). In complete KD patients, liver enzymes values were higher in comparison to incomplete KD (median ALT 62 vs 22, p = 0.001, median AST 40 vs 29 (p = 0.026) (Table 2).
Cardiological complications
A total of 56 (41.1%) patients developed some form of cardiological complication in the acute phase. As shown in Table 3, coronary artery abnormalities were the most frequent cardiological complication (22.1%). The majority of them (23/30 patients) developed transient dilations. In one of these cases the patient developed concurrently myocarditis with ventricular dysfunction. Small aneurysms were detected in four cases and medium diameter aneurysms in two patients. In two cases, the initial echo revealed a small aneurysm, and on subsequent echocardiographic investigation it further expanded, becoming in one case a giant aneurysm. Pericardial effusion was the second most common complication (18%) in acute phase.
Table 3 shows the frequency of CAAs in different phases of the disease. It is evident that most of these abnormalities were detected in the acute pre-treatment phase (18.4%) while these abnormalities were becoming less frequent in the post-treatment and the convalescent phase. In 18 patients dilations were evident from the initial pre-treatment phase and they gradually resolved whereas in 5 other patients these abnormalities were not evident in the pre-treatment phase and they developed later in the post-treatment phase.
Treatment and response
A large proportion of all the patients (108/129 -84%) responded well to the initial treatment with IVIG. Fourteen out of the 21 non-responders became afebrile after the administration of a second dose of IVIG. Five of the remaining seven patients who did not respond to two doses of IVIG responded to a third dose, while two patients required intravenous pulse of methyl prednisolone. One of these two patients additionally required treatment with infliximab, cyclosporin and tocilizumab. The median interval between onset of fever and administration of IVIG was 6 days in complete cases and 6.5 days in incomplete cases (p-value = 0.339).
Risk factors for resistance to intravenous immunoglobulin
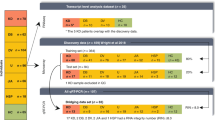
A total of 21 patients (16%) were non-responders to the initial administration of IVIG. A univariable analysis (Supplementary Table S1) was carried out in order to identify clinical and laboratory factors for resistance to IVIG. Non- responders had more commonly lower level of serum albumin and sodium, and higher level of ALT. In our population the age of patients and the day of administration of IVIG were not found to be risk factors for non-responsiveness. Multivariable regression analysis (Fig. 2) suggested that four variables were risk factors for IVIG resistance: Sodium ≤ 133 mmol/L, Albumin ≤ 3.2 g/dl, ALT ≥ 80 U/L and percentage of neutrophils ≥ 80%.

Multivariable logistic regression analysis of factors associated with IVIG non-response.
KD and coronary abnormalities
Overall, 30 patients (22%) developed coronary artery abnormalities. Univariable logistic regression analysis (Table 4) indicated that when compared with children less than 6 months old (reference category), children between 1 and 5 years had lower odds of developing CAAs. Odds of developing CAAs in age groups 6–12 months and 60 months or older, were lower than the reference category, but these differences were not statistically significant. No significant associations between gender, delayed treatment, the total duration of fever and blood parameters such as Hb, Na, Plts and CAAs were observed in our study population (Supplementary Table S2).
Discussion
This is the first study on KD carried out in Cyprus using National multicenter data. The epidemiology of the disease in our country, has similar characteristics with the previous studies in other countries especially those sharing the same climatic conditions such as Spain and Greece13,14. There is a slight preponderance of males (male/female ratio 1.25:1), which is similar to Japan and Taiwan and also in concurrence with reports from West Asian countries, such as studies from Kuwait and Western Saudi Arabia. Exception was one study from Jordan, where it was found that the male to female ratio was much higher (3.9:1)15,16,17,18,19. Children younger than 5 years old are the most frequently affected (83% of cases) with median age of cases 2.23 years, similar to other European countries and countries in West Asia. These findings were different than Japan where the incidence rate was highest among children aged 6–11 months15,16,17,18,19. The onset of KD was more frequent in winter and spring (65%), which is consistent with findings in European reports and in neighboring countries13,20. However, in reports from some East Asian countries, such as China and Taiwan, the highest incidence rates were reported during summer. Interestingly, in Japanese and Korean population in addition to the summer peak, a second peak was noted during winter15,19,20,21.
The majority of children with KD in Cyprus presented with changes of the lips/oral cavity (89%), which is in accordance with reports from other countries13,14. Followed by the skin rash, which considerably varied in nature. More precisely, maculopapular was the most common form, while in two cases a petechial rash was present. Petechial rash is not described as a frequent finding in other studies. Whilst bilateral bulbar conjunctival injection without exudates was the first or second most frequently seen manifestation in some studies13, in our study it was the third most frequent manifestation noted (80.4%). Unilateral cervical lymphadenopathy was the least common finding (57%), which was in accordance with other studies5.
Diagnosis of complete and incomplete KD depends on clinical and/or laboratory criteria. The rate for incomplete cases in our population was 31%, which is consistent with the rate found in a study in the Spanish population but differs from the rate in a study from Japan where the rate of incomplete disease was only 10%13,23. However, the percentage of patients with incomplete KD from studies in other Asian countries, such as Shanghai and South Korea were slightly higher than our findings20,21. In general, the rate of incomplete KD is underestimated and is higher in infants than in older age groups23,25. As expected, all clinical criteria were detected at a significantly lower rate in incomplete vs complete cases. However, similar to complete cases, changes of lips and oral cavity was the most frequent clinical finding in incomplete cases. This was similar to the findings in the Spanish population13. Hemoglobin levels on admission were found to be significantly lower in incomplete vs complete cases and AST and ALT were found to be significantly higher. Platelets before administration of IVIG were found higher in incomplete vs complete cases.
The rate of responsiveness to the first dose of IVIG administered is high (84%) similar to other countries in Europe5,14,25. Japanese and S. Korean population had similar rate of responsiveness, whereas studies from East China and Shanghai showed an even higher rate of responsiveness, more than 90,26. Data on the same characteristic from West Asian countries are scarce. In one study from Jordan the rate of responsiveness was similar to our results16. Multivariable regression analysis indicated that four laboratory parameters on admission i.e. sodium ≤ 133 mmol/L, albumin ≤ 3.2 g/dl, ALT ≥ 80 U/L and the percentage of neutrophils ≥ 80% were positively associated with non-responsiveness to IVIG. There is great variation in risk factors for IVIG non-responsiveness identified in different studies. A large study in the Spanish population also revealed hypoalbuminemia and hyponatremia as risk factors for non-responsiveness. In addition to these it also revealed anemia and high procalcitonin values as risk factors13. In a study in San Diego USA, multivariable analysis revealed early administration of IVIG (before day 5), higher concentrations of γGT, higher % bands and lower hemoglobin, as risk factors associated with resistance to IVIG28.
In our population, the rate of developing CAAs was similar to results from other European countries, such as Greece and North Italy15,27. Our findings are also in accordance to results of studies from Korea and Shanghai, whereas in the Japanese population the development of CAAs was less common20,21,23. Risk factors for the development of CAAs were evaluated in our study and only young age less than 12 months was identified as a risk factor. Young age < 12 months was also identified in other studies29. However, some other studies have also identified other factors as risk factors for the development of CAAs such as gender, delayed treatment, the total duration of fever and blood parameters30.
Our study has several strengths and limitations. The retrospective nature of study means it was not possible to collect additional data relevant to Kawasaki disease and that some recorded data may have been missed. However, the records kept were very detailed, in nearly all cases, and contained most data required for the study. The study covers a 19-year period, providing one of the longest Kawasaki datasets described. The study includes children with KD who have been diagnosed since 2000, therefore the treatment regimen maybe variable in some cases, according to the existing guidelines at the time. However, the total amount of immunoglobulin administered was the same in all cases.
Conclusions
This retrospective study was the first report on KD in Cyprus. Overall, the epidemiology of the disease, seems to be in accordance with other studies in Europe. Blood parameters such as low level of serum albumin, sodium, high level of ALT and high percentage of neutrophils in the FBC, were found as risk factors for non-responsiveness. Age was the only risk factor identified for the development of CAAs in our study.
Data availability
Most important elaborated data generated and analyzed during the study are included in this published article. Raw data will be available on request to the corresponding author.
Abbreviations
- KD:
-
Kawasaki disease
- CAAs:
-
Coronary artery abnormalities
- CRP:
-
C reactive protein
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- FBC:
-
Full blood count
- Plt:
-
Platelet count
- Na:
-
Serum sodium
- AMH:
-
Archbishop Makarios Hospital
- γGT:
-
Gamma -Glutamyl transferase
- Hb:
-
Hemoglobin
- WBC:
-
White blood cell count
- ESR:
-
Erythrocyte sedimentation rate
- AHA:
-
American Heart Association
- AICc:
-
Akaike information criterion
- GI:
-
Gastrointestinal
- CNS:
-
Central nervous system
- IVIG:
-
Intravenous immunoglobulin
References
Newburger, J. W. et al. Diagnosis, treatment, and long-term management of kawasaki disease: A statement for health professionals from the committee on rheumatic fever, endocarditis, and kawasaki disease, council on cardiovascular disease in the young, American Heart Association. Circulation 110, 2747–2771. https://doi.org/10.1161/01.CIR.0000145143.19711.78 (2004).
Kawasaki T. [Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children]. Arerugi 16(3), 178–222 (1967).
Sharma, D. & Singh, S. Kawasaki disease—a common childhood vasculitis. Indian J. Rheumatol. 10, S78–S83 (2015).
Rife, E. & Gedalia, A. Kawasaki disease: an update. Curr Rheumatol Rep. 22, 1–10 (2020).
McCrindle, B. W. et al. Diagnosis, treatment, and long-term management of kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 135(17), e927–e999 (2017).
Kato, H., Koike, S., Yamamoto, M., Ito, Y. & Yano, E. Coronary aneurysms in infants and young children with acute febrile mucocutaneous lymph node syndrome. J. Pediatr. 86(6), 892–898 (1975).
Yanagisawa, M., Kobayashi, N. & Matsuya, S. Myocardial infarction due to coronary thromboarteritis, following acute febrile mucocutaneous lymph node syndrome (MLNS) in an infant. Pediatrics 54(3), 277–280 (1974).
Yan, F., Pan, B., Sun, H., Tian, J. & Li, M. Risk factors of coronary artery abnormality in children with kawasaki disease: A systematic review and meta-analysis. Front. Pediatr. 7, 374 (2019).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/ (2019).
Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Springer, 2016).
Bartoń, K. MuMIn: Multi-Model Inference. R package version 1.43.6. https://CRAN.R-project.org/package=MuMIn(2019).
Heinze, G. & Ploner, M. logistf: Firth's Bias-Reduced Logistic Regression. R package version 1.23. https://CRAN.R-project.org/package=logistf to address issues of data separation (2018).
Fernandez-Cooke, E. et al. Epidemiological and clinical features of Kawasaki disease in Spain over 5 years and risk factors for aneurysm development. (2011–2016): KAWA-RACE study group. PLoS ONE 14(5), e0215665 (2019).
Alexopoulos, A. et al. Kawasaki disease in Greek children: A retrospective study. J. Eur. Acad. Dermatol. Venereol. 27(5), 580–588 (2013).
Uehara, R. & Belay, E. D. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J. Epidemiol. 22(2), 79–85 (2012).
Al-Ammouri, I., Al-Wahsh, S. & Khuri-Bulos, N. Kawasaki disease in Jordan: Demographics, presentation, and outcome. Cardiol. Young 22(4), 390–395 (2012).
Abushaban, L., Salama, A., Uthaman, B., Kumar, A. & Selvan, J. Do we have a less severe form of Kawasaki disease or is it the gammaglobulin effect?. Int. J. Cardiol. 69(1), 71–76 (1999).
Al-Harbi, K. M. Kawasaki disease in Western Saudi Arabia. Saudi Med. J. 31(11), 1217–1220 (2010).
Nakamura, Y. et al. Epidemiologic features of Kawasaki disease in Japan: Results of the 2007–2008: Nationwide survey. J. Epidemiol. 20(4), 302–307 (2010).
Xie, L. P. et al. Epidemiologic features of Kawasaki disease in Shanghai from 2013 through 2017. J. Epidemiol. 30(10), 429–435 (2020).
Beom, K. G. et al. Epidemiology of Kawasaki disease in South Korea: A nationwide survey 2015–2017. Pediatr. Infect. Dis. J. 39(11), 1012–1016 (2020).
Bar-Meir, M., Haklai, Z. & Dor, M. Kawasaki disease in Israel. Pediatr. Infect. Dis. J. 30(7), 589–592 (2011).
Yeom, J. S. et al. Kawasaki disease in infants. Korean J. Pediatr. 56(9), 377–382 (2013).
Fukushige, J., Takahashi, N., Ueda, Y. & Ueda, K. Incidence and clinical features of incomplete Kawasaki disease. Acta Paediatr. 83(10), 1057–1060 (1994).
Burns, J. C. & Glodé, M. P. Kawasaki syndrome. Lancet 364(9433), 533–544 (2004).
Tang, Y., Gao, X., Shen, J., Sun, L. & Yan, W. Epidemiological and clinical characteristics of Kawasaki disease and factors associated with coronary artery abnormalities in East China: Nine years experience. J. Trop. Pediatr. 62(2), 86–93 (2016).
Falcini, F. et al. Kawasaki disease in Northern Italy: A multicenter data collection of 250 patients. Clin. Exp. Rheumatol. 20, 421–426 (2002).
Tremoulet, A. H. et al. Resistance to intravenous immunoglobulin in children with Kawasaki disease. J. Pediatr. 153(1), 117–121 (2008).
Salgado, A. P. et al. High risk of coronary artery aneurysms in infants younger than 6 months of age with Kawasaki Disease. J. Pediatr. 185, 112-116.e1 (2017).
Brian, W. M. et al. Coronary artery involvement in children with Kawasaki disease: Risk factors from analysis of serial normalized measurements. Circulation 116(2), 174–179 (2007).
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
M.G.K. and A.J. designed the study and wrote the study protocol. M.G.K., E.G., A.A., M.K., A.E. and M.A. collected data. M.G.K., A.A. and S.M. analyzed the data and prepared the first draft of the manuscript. S.M. advised for the statistical analysis and critically reviewed the data interpretation. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koliou, M.G., Aristidou, A., Mazeri, S. et al. Epidemiology and risk factors for resistance to treatment of Kawasaki disease in Cyprus. Sci Rep 13, 352 (2023). https://doi.org/10.1038/s41598-023-27694-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-023-27694-1
