
Abstract
Ambient pollutants, particularly fine particulate matter (PM2.5) and ozone (O3), pose significant risks to both public health and economic development. In recent years, PM2.5 concentration in China has decreased significantly, whereas that of O3 has increased rapidly, leading to considerable health risks. In this study, a generalized additive model was employed to establish the relationship of PM2.5 and O3 exposure with non-accidental mortality across 17 districts and counties in Jilin Province, China, over 2015–2016. The health burden and economic losses attributable to PM2.5 and O3 were assessed using high-resolution satellite and population data. According to the results, per 10 µg/m3 increase in PM2.5 and O3 concentrations related to an overall relative risk (95% confidence interval) of 1.004 (1.001–1.007) and 1.009 (1.005–1.012), respectively. In general, the spatial distribution of mortality and economic losses was uneven. Throughout the study period, a total of 23,051.274 mortalities and 27,825.015 million Chinese Yuan (CNY) in economic losses were attributed to O3 exposure, which considerably surpassing the 5,450.716 mortalities and 6,553,780 million CNY in economic losses attributed to PM2.5 exposure. The O3-related health risks and economic losses increased by 3.75% and 9.3% from 2015 to 2016, while those linked to PM2.5 decreased by 23.33% and 18.7%. Sensitivity analysis results indicated that changes in pollutant concentrations were the major factors affecting mortality rather than baseline mortality and population.
Similar content being viewed by others

Introduction
Air pollution, recognized as the largest environmental threat, has led to a massive toll on human health worldwide1. Due to the rapid progress of urbanization, industrialization, and energy consumption, China has become one of the countries with the most severe air pollution levels2. PM2.5 and O3, two of the six criteria air pollutants prescribed by the U.S. Environmental Protection Agency, have received considerable attention for their health threats3,4. Upon inhalation, PM2.5 and O3 interact with respiratory tissues, damage lung function, and elicit inflammatory responses, finally leading to various adverse health effects3,5,6.
Epidemiological studies have evaluated the health risks related to PM2.5 and O3 exposure in the United States7,8, European9,10 and Asian countries11,12, such as China. Chen et al. estimated that a 10 μg/m3 increment in PM2.5 concentration was connected to a 0.13% increase in all-cause mortality in 30 Chinese counties13. Moreover, Lu et al. demonstrated that a 10 μg/m3 increase in PM2.5 concentration led to 0.40% increased non-accidental mortality in several Chinese cities14. Similarly, Shi et al. determined that a 10 μg/m3 increase in O3 concentration contributed to 0.37% increased non-accidental mortality in 128 counties between 2013 and 201815. Vicedo-Cabrera et al. investigated the county-specific effects of O3 on mortality and found that a 10 µg/m3 rise in O3 concentration had a relative risk (RR) (95% confidential interval CI) of 1.001 (1.000–1.003)16. In order to tackle air quality issues and safeguard public health, the Chinese government initiated the “Air Pollution Prevention and Control Action Plan” (APPCAP) in 2013. By modifying the energy structure and reducing pollutant emissions, this initiative has succeeded in reducing PM2.5 levels in numerous regions. However, PM2.5 concentrations in China still exceed the World Health Organization’s (WHO’s) Air Quality Guideline (AQG) recommendations. Moreover, O3 pollution has gotten worse contemporaneously17. Therefore, air pollution remains a persistent threat to China's public health and economy18,19.
Focusing on the United States, Deryugina et al. valued improvements in mortality from reductions in PM2.5 concentrations over 1999–2013 at US$24 billion annually20. Berman et al. noted that 1,410–2,480 premature deaths could be avoided when the O3 reached the standard of 75 ppb21. Fann and Risley evaluated that monitored reductions in PM2.5 and O3 concentrations prevented 22,000–60,000 and 880–4100 premature deaths over 2,000–2007, respectively22. Trejo-Gonzalez et al. observed that reducing PM2.5 levels to 10 µg/m3 prevented 14,666 deaths, leading to savings of US$24.1 billion in Mexico23. Lelieveld et al. demonstrated that air pollution caused 790,000 premature deaths per year in Europe24. Ballester et al. suggested that controlling PM2.5 pollution can prevent thousands of deaths annually, engendering potential benefits25. Health-related economic losses have also been assessed in several Chinese cities and regions. For instance, Yao et al. reported that PM2.5 and O3 exposure carries a substantial health burden and causes substantial economic losses nationwide26. Maji et al. estimated that in 2016, the national O3-attributable mortality was approximately 74,200, resulting in US$7.6 billion in economic losses27. Fan et al. estimated that in the Beijing–Tianjin–Hebei Region (BTH), health hazard–related economic losses due to PM2.5 exposure were 122.40 billion CNY, accounting for 1.62% of the region’s GDP (Gross Domestic Product)2. Fu et al. reported that in 2015, 2016, and 2017, PM2.5 affected 7.41%, 7.05%, and 6.94% of the population in the Central Plains Urban Agglomeration (CPUA), respectively, leading to economic losses of 97.398, 93.516, and 94.485 billion CNY, respectively28. Similar studies have been conducted in cities such as Beijing29, Shanghai30, Guangzhou31, Tianjin32, and Wuhan33. However, most of these studies have focused on the national level or key regions such as BTH, Pearl River Delta (PRD), Yangtze River Delta (YRD), and other major cities, only a few studies have examined the health burden and economic losses at the provincial level.
Therefore, the present study focused on Jilin Province, an underdeveloped area in need of both economic development and environmental protection. We estimated the association of regional PM2.5 and O3 exposure with mortality in Jilin Province and assessed the resultant health risks and economic losses caused by pollutants. The findings enable to facilitate accurate evaluations of local health risks and losses attributable to pollutants and provide the impetus and scientific basis for enhancing pollution prevention efforts in China.
Data and methods
Study area
Jilin Province is located in the geographic center of Northeast Asia and the central part of Northeast China. It spans 121°38′–131°19′E and 40°50′-46°19′N, encompassing an area of approximately 187,400 km2. Jilin is a crucial industrial hub in China and had 27.33 million residents at the end of 2016. This province has a temperate continental monsoon climate, with four distinct seasons. The winter is long and cold, with an average temperature below − 11 °C. The summer is short and warm, with an average temperature exceeding 23 °C. The average annual precipitation ranges from 400 to 600 mm. Jilin’s complex geographical conditions result from its proximity to the sea in the east and the Mongolian plateau in the west.
Data acquisition
Data for generalized additive model fitting
From January 1, 2015, to December 31, 2016, we obtained daily mortality, ambient air pollutant concentration, and meteorological factor data for 17 districts and counties within Jilin Province. The distribution of the study area and monitoring stations is illustrated in Fig. 1.

Geographical location of Jilin Province, and distribution of study areas, air quality monitoring stations, and meteorological stations (The map was generated by ArcGIS 10.7 https://www.esri.com/en-us/arcgis/products/arcgis-desktop/resources).
Mortality data were gathered from the Jilin Provincial Center for Disease Control and Prevention (CDC). These data were reported by district authorities after qualified medical practitioners diagnosed the cause of death and issued death certificates. These data were recorded along with date of death, individual’s age, sex, residence address, and cause of death (classified by the International Classification of Diseases, Tenth Revision [ICD-10]). Data on non-accidental mortality were extracted using the ICD-10 codes A00–R99, and there were no missing data for the study period.
Data on PM2.5 and O3 concentrations were collected from the China Urban Air Quality Real-time Release Platform (https://air.cnemc.cn:18007). The study area has 21 air quality monitoring stations that are operated throughout the year, with few missing data (< 2.6%). Missing values were filled by linear interpolation of observations from the preceding and subsequent days. These stations were located far from local pollution sources, and adhered to the China Ambient Air Quality Standard, making them representative of urban air pollution levels. For PM2.5, we adopted the daily mean concentration, whereas for O3, we adopted the daily maximum 8-h moving-average (MDA8) concentration.
Daily meteorological data were obtained from the China Meteorological Data Network (https://data.cma.cn), including average temperature, air pressure, relative humidity (Rh), precipitation, wind speed, and sunshine duration. These data are sourced from national-level surface meteorological stations, which are managed and quality-controlled by the China Meteorological Administration.
As monitoring stations were unevenly distributed over the study area, for districts and counties with multiple monitoring stations, we used the average value of all station observations in the region. For the areas without monitoring stations, the inverse distance weighting (IDW) method was applied to interpolate the observations from stations in other districts or counties in the city (Supplementary Appendix 1).
ChinaHighAirPollutants dataset
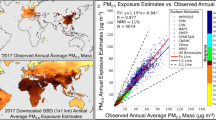
Data on average annual PM2.5 and O3 concentrations were obtained from the ChinaHighAirPollutants (CHAP) dataset. These data were utilized to calculate the spatial distribution and total health and economic losses associated with pollutants in Jilin Province. The CHAP dataset comprises a series of full-coverage, long-term, high-resolution, and high-quality datasets of ground-level air pollutants in China, all of which are derived from big data sets (from, for example, ground-based observations, satellite remote sensing products, model simulations, and atmospheric reanalysis) by using artificial intelligence and with data that reflect the spatiotemporal heterogeneity of air pollution34,35. Here, the spatial resolution of the PM2.5 dataset was 1 × 1 km2, with a root-mean-square error (RMSE) of 10.76 μg/m3 and a crossvalidation coefficient of determination (CV-R2) of 0.92 on a daily basis. Moreover, the spatial resolution of the O3 dataset was 10 × 10 km2, with an RMSE of 17.10 μg/m3 and a CV-R2 of 0.87.
Population and socioeconomic data
Highly accurate population data in 2015, precise to 1 × 1 km2, were provided by the Resource and Environment Science and Data Center (https://www.resdc.cn). These data incorporated various population-relevant characteristics, including land-use type, night light brightness, and settlement density, enabling accurate representation of China’s population distribution. The population distribution in 2016 was calculated using the annual population growth rate of Jilin Province since 2015. Socioeconomic data such as baseline mortality and disposable income in Jilin Province were obtained from the China Statistics Yearbook in 2015 and 2016.
Statistical methods
Exposure–response relationship of mortality with PM 2.5 and O 3
Based on the collected data, we used a generalized additive model to estimate the exposure–response relationship of mortality with PM2.5 and O3 in 17 districts and counties with different lags. The core model was created as follows:
where \({\text{E(Y}}_{{\text{i}}} {) }\) refers to the expected non-accidental mortality on day i; \(\upalpha\) is the intercept;\({\text{X}}_{{\text{i}}}\) indicates PM2.5 and O3 concentrations;\({ }\upbeta\) is the exposure–response coefficient; s(time, df) and s(\({\text{Z}}_{{\text{i}}}\), df) refer to the spline function of calendar time and meteorological factors, respectively. df is the degrees of freedom; and DOW and Holiday denote the influence of the week and Chinese public holidays, respectively. The spline function with 3 df was used to eliminate the potential impacts of meteorological factors, and 10 df per year was used to eliminate long-term trends. The results are finally presented as RR with 95% CI per 10 μg/m3 increase in PM2.5 and O3.
We combined the exposure–response coefficient for each district and county through meta-analysis to derive an overall estimate for Jilin Province. A random-effects model (REM) was used to combine the effect estimates when I2 > 25%; otherwise, the fixed-effects model was selected. The Mgcv package in R (version 4.1.2) was used to construct the models, and Stata (version 15.0) was used for the meta-analysis.
Estimates of additional mortality attributable to PM 2.5 and O 3
Using geographic information system (GIS) technology, high-resolution pollutant and population data were interpolated into grid with a spatial resolution of 10 km. These interpolated layers were overlaid spatially to calculate the additional mortality in each grid based on the combined exposure–response coefficient. The following equation was used36,37:
where \(\Delta {\text{Mortality}}_{{\text{i}}}\) is the additional mortality caused by PM2.5 and O3 in grid i, \({\text{Y}}_{{0}}\) is baseline mortality, \(\upbeta\) is the combined exposure–response coefficient, \({\text{C}}_{{\text{i}}}\) is the average annual pollutant concentration at grid i,\({\text{ C}}_{{0}}\) is the threshold concentration below which no health risk is assumed, and \({\text{ POP}}_{{\text{i}}}\) is the exposed population. Because it has been reported that there appeared to be no concentration (or threshold) beneath which adverse events were not observed38. 0 μg/m3 was chosen as the threshold for pollutant concentrations here.
After calculating the mortality in each grid separately, we performed spatial interpolation to obtain the distribution of the average annual additional mortality across Jilin Province and calculated the total death count using the spatial analyst tool in ArcMap (version 10.3).
Estimation of economic losses
Economic losses associated with additional mortality were quantified using the value of a statistical life (VSL). VSL is calculated through survey studies, reflecting the value people attach to a slight reduction in mortality risk 39. Given that VSL is affected by individual income levels, it varies across provinces and years. In this study, we applied a base VSL estimate of 1.68 million CNY derived from Xie’s study in Beijing40. The estimated unit economic losses in Jilin Province was converted using the following Eq. 19,36:
where \({\text{VSL}}_{{2015/2016}}\) is the unit loss per case in Jilin Province in 2015 and 2016; \({\text{VSL}}_{{{\text{base}}}}\) is 1.68 million CNY; \({\text{Income}}_{{{\text{Jilin}}, 2015/2016}}\) and \({\text{Income}}_{{{\text{base}}, 2010}}\) is the per capita disposable income of Jilin and Beijing at the given time, respectively; and e is the income elastic coefficient, set at 0.8 according to the Organisation for Economic Co-operation and Development (OECD) recommendations41.
Based on the calculated unit loss, the economic losses in each grid were estimated by the following equation:
The spatial distribution and total economic losses were also obtained using ArcMap (version 10.3).
Sensitivity analysis
Because additional mortality is influenced not only by changes in pollutant concentrations but also by social factors such as baseline mortality and population, we quantified the effect of each variable on health and calculated its relative contribution through sensitivity analysis—where only one variable was allowed to change at a time from 2015 to 2016, whereas the other variables were kept constant42.
Results
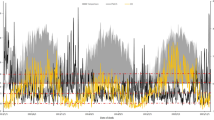
During 2015–2016, 83,868 non-accidental deaths (48,961 male and 34,907 female deaths) were reported across 17 districts in Jilin Province. The daily characteristics of the mortality, air pollutants, and meteorological factors were summarized in Table 1. The average daily mortality ranged from 3.3 to 14.6, with the lowest value observed in Xi’an and the highest value in Dehui. Daily PM2.5 concentration ranged from 41.2 to 58.6 μg/m3, exceeding the WHO's recommended limit of 15 μg/m3. The MDA8 of O3 ranged from 84.5 (in Chaoyang) to 110.3 μg/m3 (in Shuangyang). Meteorological conditions, including average daily mean temperature (ranged from 6.1 °C to 7.6 °C) and relative humidity (ranged from 61.7% to 68.3%), were fairly consistent across the study area, reflecting the temperate monsoon climate in Northeast China. Furthermore, the concentrations of PM2.5 and O3 showed distinct seasonal patterns, with PM2.5 peaking in autumn and winter and O3 peaking in summer (Fig. 2).

Time series of PM2.5 (a) and O3 (b) in 17 districts of Jilin Province over 2015–2016.
Figure 3 illustrates the estimated effects of PM2.5 and O3 on non-accidental mortality at different lag days. The RRs of mortality associated with per 10 μg/m3 increase in PM2.5 and O3 varied by districts. The maximum RR (95% CI) for PM2.5 during the single-day lag ranged from 0.986 (0.979–0.993) to 1.015 (1.007–1.023). The strongest and smallest effect was estimated in Yitong and Nong’an respectively. Significant PM2.5-mortality associations were only found in Changyi, Erdao, Jiutai, Luyuan, and Yitong. For O3, the maximum RR (95% CI) ranged from 0.990 (0.980–1.000) to 1.019 (1.004–1.035), with Dongliao having the highest impact and Kuancheng the lowest. Significant O3-mortality associations were observed in Chaoyang, Dehui, Dongliao, Jiutai, Longtan, Luyuan, Tiedong, and Yongji.

RRs (95% CIs) of mortality associated with 10 μg/m3 increases in PM2.5 (a) and O3 (b) concentrations at different lag days in 17 districts of Jilin and the combined estimates obtained from meta-analysis.
Given the heterogeneity among districts, REM was used to combine the effect estimates for both PM2.5 and O3. The results demonstrated that the overall effect of the two pollutants was significant, with O3 having a more substantial impact than PM2.5. On average, every 10 µg/m3 increase in PM2.5 and O3 concentrations corresponded to overall RRs (95% CI) of 1.004 (1.001–1.007) and 1.009 (1.005–1.012), respectively.
The average annual additional mortality and economic losses associated with PM2.5 and O3 exposure in Jilin Province varied across regions due to uneven spatial distribution of pollutants and population. As shown in Fig. 4, areas heavily affected by PM2.5 and O3 were concentrated in the central regions of Jilin, with high-value areas clustered in urban centers and sparsely distributed in suburban areas. Changchun, the provincial capital, has high levels of pollutants and high population density, leading to severe health and economic losses. Other cities, such as Songyuan, Jilin, Yanji, Siping, Liaoyuan, and Tonghua, also experienced significant economic losses. Province-wide, the average annual additional mortality and economic losses attributable to O3 exposure were approximately four times higher than those attributable to PM2.5 exposure.

Spatial distribution of the average annual non-accidental mortality (left) and economic loss (right) associated with PM2.5 and O3 exposure in Jilin Province over 2015–2016 (unit for mortality: person; unit for economic loss: million CNY) (The map was generated by ArcGIS 10.7 https://www.esri.com/en-us/arcgis/products/arcgis-desktop/resources).
Figure 5 presents the total additional mortality and economic losses in Jilin Province over 2015–2016. In 2015, PM2.5 exposure led to a total of 3,077.971 (95% CI 795.073–5,481.245) additional deaths and economic losses of 3,614.971 (95% CI 933.786–6,437.533) million CNY, which decreased to 2,372.745 (95% CI 611.900–4,232.761) additional deaths and 2,938.809 (95% CI 757.881–5,242.568) million CNY in economic losses in 2016. Conversely, O3 exposure caused 11,318.892 (95% CI 6,608.547–15,395.248) additional deaths and economic losses of 13,293.649 (95% CI 7761.511–18,081.189) million CNY in 2015, which increased to 11,732.382 (95% CI 6856.330–15,944.577) additional deaths and 14,531.366 (95% CI 8492.039–19,748.460) million CNY in economic losses in 2016.

Total non-accidental mortality (a) and economic loss (b) associated with PM2.5 and O3 exposure in Jilin Province in 2015 and 2016.
The sensitivity analysis revealed that the changes in additional mortality between 2015 and 2016 were influenced by pollutant concentrations, baseline mortality, and population. The number of deaths attributable to PM2.5 exposure decreased by 23.33% in 2016 compared to 2015. This decrease was primarily driven by a reduction in PM2.5 concentrations (21.39%), with smaller contributions from changes in baseline mortality (1.21%) and population (0.73%). In contrast, the number of deaths attributable to O3 exposure increased by 3.75% in 2016 compared to 2015. This increase was primarily due to a rise in O3 concentration (5.69%), partially offset by changes in baseline mortality (1.21%) and population (0.73%) (Table 2).
Discussion
In this study, we assessed the health burden and economic losses associated with PM2.5 and O3 exposure in Jilin Province over 2015–2016. The results indicated that despite the implementation of China’s pollution prevention and control policies has facilitated air pollutant hazard mitigation, PM2.5 and O3 still pose a significant health risk and constitute a source of economic losses in Jilin Province.
PM2.5 and O3 stimulate oxidative stress, promote airway hyperresponsiveness, induce airway inflammation, and affect vascular endothelial function and thus influence heart rate and vascular tone regulation43,44. Numerous studies have well revealed the exposure–response relationship of non-accidental mortality with PM2.5 and O3. Cai et al. observed that for every 10 μg/m3 increase in PM2.5 concentration, the strongest excess risk (ER; 95% CI) for non-accidental mortality was 0.67% (0.01%–1.33%) in Shenzhen45. Xu et al. reported 0.17% (95% CI 0.05%–0.29%) increased non-accidental mortality in Beijing46, and Fang et al. observed 0.26%–0.35% increased mortality in Shanghai47. Li et al. found that a 10 μg/m3 increase in O3 concentration is correlated with a 0.56% (95% CI 0.36%–0.76%) higher risk of non-accidental death in Guangzhou42. Kan et al. reported a 0.31% (95% CI 0.04%–0.58%) increase in mortality in Shanghai48, whereas Lei et al. reported 0.05% (95% CI 0.42%–0.53%) increased mortality in Hefei49. In the present study, the maximum RR (95% CI) during the single-day lag ranged from 0.986 (0.979–0.993) to 1.015 (1.007–1.023) for PM2.5 and from 0.990 (0.980–1.000) to 1.019 (1.004–1.035) for O3. The effect estimates vary between counties and regions because of differences in pollution conditions, population characteristics, and lifestyles50. After the effect values were combined in a meta-analysis, both pollutants were found to be significantly associated with non-accidental mortality, with an overall RR (95% CI) of 1.004 (1.001–1.007) and 1.009 (1.005–1.012), respectively.
Our study revealed an uneven spatial distribution of additional mortality and economic losses associated with PM2.5 and O3 in Jilin Province. The results demonstrated a higher health burden in the central region and a lower health burden in the western region. The central region, characterized by large cities, had higher pollutant concentrations and population density, so people are more likely to be subjected to a higher level of pollutants51. In contrast, the western region, closer to the coastline, experienced improved pollution diffusion and better air quality52. As the capital city of Jilin Province, Changchun bore the most severe health burden and economic losses. Another study in Gansu Province also reported that economic costs in the capital city are higher than those in other cities53. Provincial capitals are typically demonstrating a rapid increase in population, urbanization, industrialization, and energy consumption. Thus, high emission, a developed economy, and high population density result in large health burden and economic losses.
In 2015, PM2.5 exposure resulted in 3,077.971 additional deaths and 3,614.971 million CNY in economic losses, accounting for 0.26% of the province’s GDP. However, in 2016, these figures decreased to 2,372.745 deaths and 2,938.809 million CNY in economic losses, respectively, accounting for 0.20% of GDP. At the national level, Sun et al. reported that in China, PM2.5 affected an average of 15.03 million people per year and caused economic losses of 1.71% of China's GDP, about US$86,886.94 million54. Diao et al. found that in China’s 338 cities, the overall economic losses caused by exposure to PM2.5 in 2015 was 1.846 trillion CNY, which was 2.73% of their total annual GDP51. Chen et al. calculated in 2014, when the PM2.5 reached the national air quality standards in China, an estimated 0.35 million deaths were avoided, along with an economic gain of 430 billion CNY37. Fan et al. estimated that in 2016, the average economic cost caused by PM2.5 was 122.40 billion CNY in the BTH, accounting for 1.62% of the region’s GDP2. Wang et al. explored that in the YRD, the short-term mortality and economic losses due to PM2.5 were estimated to be 13,162 and 22.1 billion CNY in 2010, respectively55. Similar results have also been drawn from studies in the PRD and the Fenwei Plain (FWP)56,57. At the provincial and city levels, Gao et al. found that PM2.5 exposure contributed 17.6% to premature mortality in Hebei Province19. Liao et al. evaluated the health burden and economic losses in the cities of Gansu Province and reported that from 2015 to 2017, PM2.5 caused 1,644,870, 1,551,447, and 1,531,372 deaths, respectively, with an economic loss of 42,699, 43,982 and 44,261 million CNY, respectively53. Cui et al. demonstrated that decreasing PM2.5 concentrations to 15 μg/m3 may reduce mortality and morbidity by 70% and 95%, respectively, in Jinan, saving US$1,289.5 million58. Similar studies have been conducted in Guangzhou31, Shanghai30, Lanzhou59, and Taiyuan60. Although these studies are not directly comparable for the differences in study areas, study design and period, health endpoints, and population lifestyle, their results are valid. In addition, over 2015–2016, the losses caused by PM2.5 exposure exhibited a downward trend, as noted previously. Ding et al. estimated the change in PM2.5-related mortality from 2013 to 2017 and indicated that the estimated mortality in China decreased significantly from 1.389 (95% CI 1.005–1.631) million CNY to 1.102 (95% CI 0.755–1.337) million CNY61. Fu et al. observed that the health damage caused by PM2.5 exposure decreased in the CPUA between 2015 and 201728. Cui et al. discovered significant decreases in ambient PM2.5 concentrations in Jinan from 2013 to 2017, which prevented 2,317 premature deaths and saved US$317.7 million58. In Beijing and Wuhan, the worsening trend of air quality began to reverse as well33. These results jointly indicate that the implementation of APPCAP in China has yielded substantial environmental, health, and economic benefits.
Along with the decrease in PM2.5 concentrations, however, O3 concentrations have been gradually increasing in recent years, leading to higher additional mortality and economic losses. Gao et al. found that over 2015–2017, in Handan, Hebei Province, the average annual O3 concentration increased by 35.1%, whereas PM2.5 concentration decreased by 6.6%3. Zhang et al. reported that in 331 cities in China, the rate of the population exposed to O3 increased from 13.35% in 2015 to 14.15% in 2020, whereas that of the population exposed to PM2.5 declined over 2015–202062. Guan et al. revealed that in BTH and FWP cities, the PM2.5-related health impact decreased by 17.14% but the O3-related health impact increased by > 90% between 2015 and 20204. Wang et al. revealed that in 74 Chinese cities, the number of additional deaths correlated with short-term and long-term PM2.5 exposure decreased by approximately 72.49% and 10%, respectively, while O3-related deaths increased by 76.16% and 130.57%, respectively, during 2013–201863. Our study in Jilin Province also demonstrated that O3 exposure contributed to an increase in mortality and economic losses. In 2015, O3 exposure contributed to 11,318.892 (95% CI 6,608.547–15,395.248) additional deaths and 13,293.649 (95% CI 7,761.511–18,081.189) million CNY in economic losses, accounting for 0.95% of the province’s GDP. In 2016, these figures rose to 11,732.382 (95% CI 6,856.330–15,944.577) and 14,531.366 (95% CI 8,492.039–19,748.460), respectively, accounting for 0.98% of the province’s GDP. The increasing trends for O3 in China after air pollution control may be because the decreases in PM2.5 further affected O3 concentration through changes in aerosol chemistry and photolysis rates64,65. In the future, comprehensive air pollution control strategies should be implemented on the basis of existing policies.
Additional mortality is simultaneously affected by pollutant concentrations, baseline mortality, and population. For mortality attributable to PM2.5 exposure, these factors collectively contributed to a decrease in mortality, with PM2.5 concentration changes being the key driver. For mortality attributable to O3 exposure, changes in O3 concentration resulted in increased mortality, although changes in baseline mortality and population partially offset this increase. In the literature, Li et al. assessed premature mortality in China with respect to independent variations in PM2.5, baseline mortality, and population42. The authors noted that PM2.5 change had a greater effect on mortality than other factors did and that it was the primary determinant of changes in mortality. Yin et al. reported that between 1990 and 2017, a decline in air pollution exposure partially offset population growth and aging in China66. Zhang et al. quantified the contribution of different factors to the health burden and noted that the reduction in pollutant concentration is the dominant factor in mitigating adverse health effects67. Consequently, from a risk perspective, reducing pollutant concentrations is likely the most effective strategy for reducing health risks associated with ambient pollutants.
Our study has some limitations. The first major limitation is related to safety thresholds for air pollutants. At present, no consistent indications for setting a specific threshold have been reported. In the present study, we used 0 μg/m3 as the threshold for both PM2.5 and O3 concentrations, which may yield a relatively higher estimation than studies set thresholds according to China’s national standards and WHO standards63,68. Moreover, we estimated the spatial distribution of health burden and economic losses with a 10-km resolution using GIS. In this process, PM2.5 and population data with a 1-km resolution were converted to an identical resolution, which may potentially obscure or overestimate the benefit estimates69. Finally, when calculating health burden and economic losses, we assumed a static population in the study region even though actual exposure is typically dynamic, which may result in underestimated results70. In addition, other factors such as age structures, income conditions, and medical conditions in different regions were not considered during the current evaluation, affecting the current assessment accuracy. Despite these limitations, the overall trend identified in this study remained unaffected, and these findings can still aid in assessments of the actual situation in Jilin Province.
Conclusion
According to our findings, although the air quality has improved in recent years, Jilin Province continues to face significant health and economic challenges associated with PM2.5 and O3 exposure. During the study period, the additional mortality and economic losses related to PM2.5 exposure were significantly lower than those related to O3 exposure. Specifically, from 2015 to 2016, the health impact and economic losses attributable to PM2.5 exposure decreased by 23.33% and 18.7%, respectively, whereas those linked to O3 exposure increased by 3.75% and 9.3%, respectively. Pollutant concentration is the dominant factor affecting mortality. Therefore, more aggressive air pollution control strategies should continue to be implemented in the future to reduce ambient PM2.5 concentrations and mitigate O3 pollution.
Data availability
The datasets are not publicly available due to data privacy but are available from the corresponding author on reasonable request.
References
WHO. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide (2021).
Xue, W., et al. Can clean heating effectively alleviate air pollution: An empirical study based on the plan for cleaner winter heating in northern China. Appl. Energy 351, 121923 (2023).
Gao, A. et al. Health and economic losses attributable to PM2.5 and ozone exposure in Handan, China. Air Qual. Atmos. Health 14, 605–615 (2021).
Guan, Y. et al. Long-term health impacts attributable to PM2.5 and ozone pollution in China’s most polluted region during 2015–2020. J. Clean Prod. 321, 128970 (2021).
Li, Y. et al. Premature mortality attributable to PM2.5 pollution in China during 2008–2016: Underlying causes and responses to emission reductions. Chemosphere 263, 127925 (2021).
Zhang, Y. et al. Short-term effects of ambient PM1 and PM2.5 air pollution on hospital admission for respiratory diseases: Case-crossover evidence from Shenzhen, China. Int. J. Hyg. Environ. Health 224, 13418 (2020).
Zigler, C. M. et al. Impact of national ambient air quality standards nonattainment designations on particulate pollution and health. Epidemiology 29, 165–174 (2018).
Peng, R. et al. Acute effects of ambient ozone on mortality in Europe and North America: results from the APHENA study. Air Qual. Atmos. Health 6, 445–453 (2013).
Pattenden, S. et al. Ozone, heat and mortality: Acute effects in 15 British conurbations. Occup. Environ. Med. 67, 699–707 (2010).
Samoli, E. et al. Associations between fine and coarse particles and mortality in Mediterranean cities: Results from the MED-PARTICLES project. Environ. Health Perspect 121, 932–938 (2013).
Lee, H. et al. Short-term exposure to fine and coarse particles and mortality: A multicity time-series study in East Asia. Environ. Pollut. 207, 43–51 (2015).
Chen, R. et al. Ozone and daily mortality rate in 21 cities of East Asia: How does season modify the association?. Am. J. Epidemiol. 180, 729–736 (2014).
Chen, C. et al. Short-term exposures to PM2.5 and cause-specific mortality of cardiovascular health in China. Environ. Res. 161, 188–194 (2018).
Lu, F. et al. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 136, 196–204 (2015).
Shi, W. et al. Modification effects of temperature on the ozone-mortality relationship: A nationwide multicounty study in China. Environ. Sci. Technol. 54, 2859–2868 (2020).
Vicedo-Cabrera, A. M. et al. Short term association between ozone and mortality: Global two stage time series study in 406 locations in 20 countries. BMJ. 368, m108 (2020).
Guan, Y. et al. Assessing the health impacts attributable to PM2.5 and ozone pollution in 338 Chinese cities from 2015 to 2020. Environ. Pollut. 287, 117623 (2021).
Fang, Z. et al. Air pollution’s impact on the economic, social, medical, and industrial injury environments in China. Healthcare 9, 261 (2021).
Gao, A. et al. Coordinated health effects attributable to particulate matter and other pollutants exposures in the North China Plain. Environ. Res. 208, 112671 (2022).
Deryugina, T. et al. The mortality and medical costs of air pollution: Evidence from changes in wind direction. Am. Econ. Rev. 109, 4178–4219 (2019).
Berman, J. D. et al. Health benefits from large-scale ozone reduction in the United States. Environ. Health Perspect. 120, 1404–1410 (2012).
Fann, N. et al. The public health context for PM2.5 and ozone air quality trends. Air Qual. Atmos. Health 6, 1–11 (2013).
Trejo-González, A. G. et al. Quantifying health impacts and economic costs of PM2.5 exposure in Mexican cities of the National Urban System. Int. J. Public Health 64, 561–572 (2019).
Lelieveld, J. et al. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart J. 40, 1590–1596 (2019).
Ballester, F. et al. Health impact assessment on the benefits of reducing PM2.5 using mortality data from 28 European Cities. Epidemiology 17, 566–567 (2006).
Yao, M. et al. Estimating health burden and economic loss attributable to short-term exposure to multiple air pollutants in China. Environ. Res. 183, 109184 (2020).
Maji, K. J. et al. Ozone pollution in Chinese cities: Assessment of seasonal variation, health effects and economic burden. Environ. Pollut. 247, 792–801 (2019).
Fu, X. et al. The economic loss of health effect damages from PM2.5 pollution in the Central Plains Urban Agglomeration. Environ. Sci. Pollut. Res. Int. 27, 25434–25449 (2020).
Jiang, Y. et al. Burden of cardiovascular diseases associated with fine particulate matter in Beijing, China: An economic modelling study. BMJ Glob. Health. 5, e003160 (2020).
Voorhees, A. S. et al. Public health benefits of reducing air pollution in Shanghai: A proof-of-concept methodology with application to BenMAP. Sci. Total Environ. 485–486, 396–405 (2014).
Lin, H. et al. Quantifying short-term and long-term health benefits of attaining ambient fine particulate pollution standards in Guangzhou, China. Atmos. Environ. 137, 38–44 (2016).
Zhang, J. et al. Health benefits on cardiocerebrovascular disease of reducing exposure to ambient fine particulate matter in Tianjin, China. Environ. Sci. Pollut. Res. Int. 27, 13261–13275 (2020).
Qu, Z. et al. PM2.5-related health economic benefits evaluation based on air improvement action plan in Wuhan City, Middle China. Int. J. Environ. Res. Public Health 17, 620 (2020).
Wei, J. et al. Reconstructing 1-km-resolution high-quality PM2.5 data records from 2000 to 2018 in China: spatiotemporal variations and policy implications. Remote Sens. Environ. 252, 112136 (2021).
Wei, J. et al. Full-coverage mapping and spatiotemporal variations of ground-level ozone (O3) pollution from 2013 to 2020 across China. Remote Sens. Environ. 270, 112775 (2022).
Luo, G. et al. Quantifying public health benefits of PM2.5 reduction and spatial distribution analysis in China. Sci. Total Environ. 719, 137445 (2020).
Chen, L. et al. Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on BenMAP. Environ. Pollut. 221, 311–317 (2017).
WHO. Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Global update 2005: Summary of Risk Assessment. 2006.
Yin, H. et al. External costs of PM2.5 pollution in Beijing, China: Uncertainty analysis of multiple health impacts and costs. Environ. Pollut. 226, 356–369 (2017).
Xie. The Value of Health: Environmental Valuation and Control Strategy Study of Urban Air Pollution (Peking University, Beijing, 2011) (Chinese).
OECD. Mortality Risk Valuation in Environment, Health and Transport Policies. (OECD Publishing, Paris, 2012).
Li, M. et al. Association between ambient ozone pollution and mortality from a spectrum of causes in Guangzhou, China. Sci. Total Environ. 754, 142110 (2021).
Bao, W. et al. Effects of ozone repeated short exposures on the airway/lung inflammation, airway hyperresponsiveness and mucus production in a mouse model of ovalbumin-induced asthma. Biomed. Pharmacother 101, 293–303 (2018).
Shang, J. et al. Acute changes in a respiratory inflammation marker in guards following Beijing air pollution controls. Sci. Total Environ. 624, 1539–1549 (2018).
Cai, J. et al. Association between PM2.5 exposure and all-cause, non-accidental, accidental, different respiratory diseases, sex and age mortality in Shenzhen, China. Int. J. Environ. Res. Public Health 16, 401 (2019).
Xu, M. et al. Modifiers of the effect of short-term variation in PM2.5 on mortality in Beijing. China. Environ. Res. 183, 109066 (2020).
Fang, X. et al. Relationship between fine particulate matter, weather condition and daily non-accidental mortality in Shanghai, China: A Bayesian approach. PLoS One 12, e0187933 (2017).
Kan, H. et al. Part 1. A time-series study of ambient air pollution and daily mortality in Shanghai, China. Res. Rep. Health Eff. Inst. 154, 17–78 (2010).
Lei, R. et al. Short-term effect of PM2.5/O3 on non-accidental and respiratory deaths in highly polluted area of China. Atmos. Pollut. Res. 10, 1412–1419 (2019).
Fold, N. R. et al. An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. Int. J. Environ. Res. Public Health 17, 7298 (2020).
Lu, X. et al. Analysis of the adverse health effects of PM2.5 from 2001 to 2017 in China and the role of urbanization in aggravating the health burden. Sci. Total Environ. 652, 683–695 (2019).
Diao, B. et al. Impact of Urbanization on PM2.5-Related Health and Economic Loss in China 338 Cities. Int. J. Environ. Res. Public Health 17, 990 (2020).
Liao, Q. et al. Health and economic loss assessment of PM2.5 pollution during 2015–2017 in Gansu Province, China. Int. J. Environ. Res. Public Health 17, 3253 (2020).
Sun, X. et al. Spatial-temporal evolution of health impact and economic loss upon exposure to PM2.5 in China. Int. J. Environ. Res. Public Health 19, 1922 (2022).
Wang, J. et al. Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta, China. Atmos. Environ. 123, 440–448 (2015).
Wu, D. et al. A study of control policy in the Pearl River Delta region by using the particulate matter source apportionment method. Atmos. Environ. 76, 147–161 (2013).
Dong, Z. et al. The economic loss of public health from PM2.5 pollution in the Fenwei Plain. Environ. Sci. Pollut. Res. Int. 28, 2415–2425 (2021).
Cui, L. et al. Analyses of air pollution control measures and co-benefits in the heavily air-polluted Jinan city of China, 2013–2017. Sci. Rep. 10, 5423 (2020).
Sun, Z. et al. Assessment of population exposure to PM10 for respiratory disease in Lanzhou (China) and its health-related economic costs based on GIS. BMC Public Health 13, 891 (2013).
Zhang, D. et al. The assessment of health damage caused by air pollution and its implication for policy making in Taiyuan, Shanxi, China. Energy Policy 38, 491–502 (2010).
Ding, D. et al. Estimated Contributions of Emissions Controls, Meteorological Factors, Population Growth, and Changes in Baseline Mortality to Reductions in Ambient PM2.5 and PM2.5-Related Mortality in China, 2013–2017. Environ. Health Perspect. 127, 67009 (2019).
Zhang, X. et al. A Health Impact and Economic Loss Assessment of O3 and PM2.5 Exposure in China From 2015 to 2020. Geohealth. 6, e2021GH000531 (2022).
Wang, F. et al. Policy-driven changes in the health risk of PM2.5 and O3 exposure in China during 2013–2018. Sci. Total Environ. 757, 143775 (2021).
Wei, J. et al. Separating daily 1 km PM2.5 inorganic chemical composition in China since 2000 via deep learning integrating ground, satellite, and model data. Environ. Sci. Technol. https://doi.org/10.1021/acs.est.3c00272 (2023).
Lou, S. et al. Impacts of aerosols on surface-layer ozone concentrations in China through heterogeneous reactions and changes in photolysis rates. Atmos. Environ. 85, 123–138 (2014).
Yin, P. et al. The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990–2017: an analysis for the Global Burden of Disease Study 2017. Lancet Planet Health 4, e386–e398 (2020).
Zhang, M. et al. Health Impact Attributable to the Control of PM2.5 Pollution in China During 2013–2017. Huan Jing Ke Xue 42, 513–522 (2021).
Sun, Z. et al. The health impacts of aerosol-planetary boundary layer interactions on respiratory and circulatory mortality. Atmos. Environ. 276, 119050 (2022).
Chen, L. et al. Estimating short-term mortality and economic benefit attributable to PM10 exposure in China based on BenMAP. Environ. Sci. Pollut. Res. Int. 25, 28367–28377 (2018).
Beckx, C. et al. A dynamic activity-based population modelling approach to evaluate exposure to air pollution: Methods and application to a Dutch urban area. Environ. Impact Assess. Rev. 29, 179–185 (2009).
Acknowledgements
This research is supported by National Natural Science Foundation of China (Grant Nos. 41975141) and the Fundamental Research Funds for the Central Universities (No. lzujbky-2022-it21). Part of the work is funded by a Scholarship awarded to Yuxia Ma (File No. 20206185010) supported by the China Scholarship Council.
Author information
Authors and Affiliations
Contributions
Conception and design: Y.M. Statistical analysis: Y.M., Y.Z. Drafting of the article: Y.M., Y.Z., W.W. Analysis and interpretation of the data: P.Q., H.L. Data acquisition and curation: Y.M., H.J., J.W. Funding acquisition: Y.M., Y.Z.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, Y., Zhang, Y., Wang, W. et al. Estimation of health risk and economic loss attributable to PM2.5 and O3 pollution in Jilin Province, China. Sci Rep 13, 17717 (2023). https://doi.org/10.1038/s41598-023-45062-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-023-45062-x
This article is cited by
-
Short-term exposure to ambient air pollution and onset of severe mental disorders: a case-crossover study in Northwestern China
BMC Public Health (2025)
-
Assessment of health economic losses caused by PM2.5 and ozone pollution in Beijing and Tianjin
Scientific Reports (2025)
-
Association between exposure to air pollutants and cardiovascular mortality in Iran: a case-crossover study
Scientific Reports (2025)
-
The spatiotemporal evolution and contributing factors of PM2.5 and O3 concentrations in Shandong Province from 2014–2023
Environmental Monitoring and Assessment (2025)
-
Assessing Spatiotemporal Characteristics, Health Impacts and Related Economic Losses of PM2.5, PM10 and O3 in Beijing-Tianjin-Hebei Region from 2015 to 2020
Environment, Development and Sustainability (2025)
