
Abstract
In our study, we aimed to evaluate the effect of high-dose intravenous anakinra treatment on the development of thrombotic events in severe and critical COVID-19 patients. This retrospective observational study was conducted at a tertiary referral center in Aksaray, Turkey. The study population consisted of two groups as follows; the patients receiving high-dose intravenous anakinra (anakinra group) added to background therapy and the patients treated with standard of care (SoC) as a historical control group. Age, gender, mcHIS scores, and comorbidities such as diabetes mellitus, hypertension, and coronary heart disease of the patients were determined as the variables to be matched. We included 114 patients in SoC and 139 patients in the Anakinra group in the study. Development of any thromboembolic event (5% vs 12.3%, p = 0.038; OR 4.3) and PTE (2.9% vs 9.6%, p = 0.023; OR 5.1) were lower in the Anakinra group than SoC. No patient experienced cerebrovascular accident and/or clinically evident deep venous thrombosis both in two arms. After 1:1 PS matching, 88 patients in SoC and 88 patients in the Anakinra group were matched and included in the analysis. In survival analysis, the development of any thromboembolic event, pulmonary thromboembolism, and acute coronary syndrome (ACS) were higher in SoC compared to Anakinra. Survival rate was also lower in patients with SoC arm than Anakinra in patients who had any thromboembolic event as well as ACS. In our study, the development of thrombosis was associated with hyperinflammation in patients with severe and critical COVID-19. Intravenous high-dose anakinra treatment decreases both venous and arterial events in patients with severe and critical COVID-19.
Similar content being viewed by others


Introduction
Coronavirus-19 (COVID-19) is an emerging infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and affects many organs mainly upper and lower respiratory tracts. Disease severity of COVID-19 ranges from asymptomatic and/or mild symptoms to potential life-threatening disease including acute respiratory distress syndrome (ARDS), multi-organ failure, and even death. Several risk factors such as male gender, advanced age, some comorbidities including diabetes mellitus (DM), hypertension (HT) and coronary heart disease (CHD), and immunosuppressive treatment were described for the development of poor prognosis as well as severe course in COVID-191.
Hyperinflammation (cytokine storm) is one of the main features of severe disease in COVID-19 and is also closely associated with poor outcomes including ARDS, the need for oxygen therapy, and higher mortality2. Several immunomodulatory treatments such as corticosteroids, baricitinib, anakinra, and tocilizumab were found to be effective in COVID-19 patients with signs of hyperinflammation3,4,5,6.
In addition to cytokine storm, some patients suffer from thrombotic events including acute coronary syndrome (ACS), cerebrovascular accident (CVA), and venous thromboembolism (VTE) such as deep vein thrombosis (DVT) and pulmonary thromboembolism (PTE) during the course of COVID-197. Thereby, prophylactic use of anticoagulant and/or antiaggregant therapies were applied especially in hospitalized COVID-19 patients in daily practice8. However, some studies have shown reduced mortality and also the development of thromboembolic events with prophylactic use of anticoagulant therapy9,10,11, there are conflicting results with the benefit of anticoagulant therapy in terms of development of mortality and/or thrombosis12. Moreover, it is not known whether immunomodulatory therapy reduces thromboembolic events in patients with severe COVID-19.
In our study, we aimed to evaluate the effect of high-dose intravenous anakinra treatment on the development of thrombotic events in severe and critical COVID-19 patients.
Materials and methods
Patients and data
This retrospective observational study, which includes a secondary analysis of our previous study13, was conducted at a tertiary referral center in Aksaray, Turkey. The patients who had available data about thrombotic events both in two arms (anakinra and control group) from our previous study were re-evaluated and included for PS matching in this study. The patients with no data about thrombotic events and/or missing data were excluded. Diagnosis of COVID-19 was performed by typical computer tomography (CT) findings in addition to clinical signs and symptoms. All patients had positive polymerase chain reaction (PCR) and delta variant (B.1.617.2) proven by variant analysis.
The study population consisted of two groups as follows; the patients receiving high-dose intravenous anakinra (anakinra group) added to background therapy between 01.09.2021 and 01.02.2022 and the patients treated with standard of care (SoC) as historical control group who were hospitalized between 01.07.2021 and 01.09.2021. COVID-19 disease severity was evaluated according to the National Institute of Health (NIH) severity scale and only severe (NIH score 3; patients with SpO2 < 94% on room air at sea level, PaO2/FiO2 < 300 mm Hg, a respiratory rate > 30 breaths/min, or lung infiltrates > 50%) and critically ill (NIH score 4; patients have acute respiratory distress syndrome, septic shock that may represent virus-induced distributive shock, cardiac dysfunction, an exaggerated inflammatory response, and exacerbation of underlying comorbidities, as well as requirement of high flow nasal oxygen therapy [HFNO] or invasive mechanical ventilation [IMV]) patients in the ward were included into the study14.
The study has been performed in accordance with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. An informed written consent was obtained for the study. Institutional Review Board approval was also obtained from the Aksaray University Ethics Committee (date/number: 24.02.2022, 2022/04-09).
Laboratory evaluation
Laboratory values such as hemogram, liver enzymes, troponin levels, C-reactive protein (CRP) (mg/dL), ferritin (pg/mL), d-dimer (pg/mL), lactate dehydrogenase (LDH) (U/L), procalcitonin (pg/dL) at the admission and consecutive days (procalcitonin was every other day but others were once in a day); the peak levels of CRP, ferritin, d-dimer and LDH levels were recorded. The inflammatory state of the patients was evaluated and derived based on the COVID hyperinflammatory syndrome score (cHIS) and it was calculated according to the combination of neutrophil and lymphocyte counts at the admission and the peak levels of CRP, ferritin, d-dimer, and LDH during to the follow-up15. The item of fever was removed in both arms due to its lower frequency (< %10) and inconsistent relevance in the diagnosis of COVID-19-associated hyperinflammation. Therefore, the maximum score of the new version of the cHIS score was 5 points (modified cHIS [mcHIS] score) was calculated in both groups13.
Treatment protocol and outcome
All patients received background corticosteroid therapy with intravenous 80 mg/day methylprednisolone or dexamethasone 6 mg/day (or its equivalent)16 and enoxaparin 0.4 mg/day at the admission and continued consecutive days (SoC). Anakinra was added to the background treatment in the early phase of the disease in patients who did not respond to initial treatment for at least two days or concomitantly with steroids in patients with higher risk and/or critical illness at admission. The average starting dose of anakinra was 400 mg/day intravenously and increased gradually to a maximum of 1600 mg/day if necessary (10 mg/kg/day). Anakinra dose adjustment was performed by the same experienced physician in COVID-19 (MB) according to daily clinical (respiratory symptoms, degree of oxygen supply, presence of fever) and laboratory findings. Anakinra and steroid treatment were administered until the hyperinflammatory response of the patients disappeared or the discharge or development of death.
Diagnosis of PTE was confirmed by thorax CT-angiography in patients with prominent d-dimer increase despite a decrease in acute phase reactants (APR) such as CRP and ferritin and/or increase in need of oxygen therapy and respiratory distress despite the decrease in levels of APRs. Diagnosis of acute coronary syndrome (ACS) was made according to the definition of the European Society of Cardiology guideline17. Severe infection was defined as the development of opportunistic infection, need for intravenous antibiotics, sepsis, or requirement of intensive care unit (ICU) admission or development of death due to secondary infection.
Statistical analysis
In our study, the 22.0 version (IBM, Armonk, NY, USA) of the SPSS (Statistical Package for the Social Sciences) program was used for statistical analysis of data. In descriptive statistics, discrete and continuous numerical variables were expressed as mean, ± standard deviation, or median (minimum–maximum), interquartile range (IQR). Categorical variables were expressed as number of cases (%). Cross-table statistics were used to compare categorical variables (Chi-Square, Fisher’s exact test). Normally distributed parametric data were compared with Student's t-test and non-parametric data that did not meet normal distribution were compared with Mann–Whitney U and Kruskal–Wallis tests. Correlation analysis was performed by Pearson or Spearman method according to normality distribution. Kaplan–Meier and log-rank methods were used for survival analysis. Multivariate analysis was performed by using logistic regression. Sensitivity and specificity calculations were performed by Receiver operating characteristic (ROC) analysis. p < 0.05 value was considered statistically significant.
Propensity score matching
The first step in Propensity Score Matching (PSM) is to identify the covariates from which to calculate propensity scores (PS). Age, gender, mcHIS scores, and comorbidities such as DM, HT, and CHD of the patients were determined as the variables to be matched. The PS matching was done as 1:1 with the nearest neighbor method. The caliper value was 0.2. When matching, we performed this analysis by assigning values according to the averages of the parameters with missing data. PSM was performed with the SPSS package program 28.0.1 using the R package program and an auxiliary plugin (PS matching 3.0 SPE). Dot-plot of standardized mean differences for all covariates before and after PS matching was shown in Supplementary Fig. 1. Jitter plots for trend scores and line plots of standardized differences were described in supplemental Figs. 2 and 3, respectively.
Ethics approval
The study has been performed in accordance with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. An informed written consent was obtained for the study. Institutional Review Board approval was also obtained from the Aksaray University Ethics Committee (date/number: 24.02.2022, 2022/04-09).
Results
Analysis before PS matching
We included 114 patients in SoC and 139 patients in the Anakinra group in the study. The baseline clinical and laboratory features of the patients are described in Table 1.
Development of any thromboembolic event (5% vs 12.3%, p = 0.038; OR 4.3) and PTE (2.9% vs 9.6%, p = 0.023; OR 5.1) were lower in the Anakinra group than SoC. No patient experienced CVA and/or clinically evident DVT both in two arms. Although severe infection, pneumothorax, and ACS were not different between the two arms (p = 0.1, p = 0.1, and p = 0.2, respectively); ICU admission (39.6% vs 22%, p = 0.003; OR 9) and mortality (36.7% vs 27%, p = 0.026; OR) were higher in Anakinra group compared to SoC before PS matching analysis (Table 1).
Patients experienced any thromboembolic event had longer duration of hospitalization (p = 0.03), higher vaccination counts (p = 0.028), more frequent CHD (p = 0.001; OR 11.8), critical disease (p = 0.001; OR 10.6), higher mcHIS scores (p < 0.001), lower NLR (p = 0.002) and higher baseline d-dimer levels (p = 0.04), higher peak levels of CRP (p = 0.012), ferritin (p < 0.001), d-dimer (p = 0.002), and LDH (p < 0.001). Development of thrombosis was also higher in patients who had mortality (62% vs 28%, p = 0.001; OR 10.4) in univariate analysis (Table 2). Patients developed PTE had longer duration of hospitalization (p = 0.03), higher vaccination counts (p = 0.03), critical disease (p = 0.005; OR 7.8), higher mcHIS scores (p < 0.001), and higher baseline d-dimer levels (p = 0.04), higher peak levels of CRP (p = 0.012), ferritin (p < 0.001), d-dimer (p = 0.002), and LDH (p < 0.001). Development of PTE was also higher in patients who had a severe infection (p = 0.028; OR 4.8), pneumothorax (p = 0.046; OR 4), ACS (p < 0.001; OR 12.6), and SoC (p = 0.023; OR 5.1) in univariate analysis (Table 3). In multivariate analysis, peak d-dimer levels (p < 0.001, OR 1.1, 95% Confidence interval [CI] 1.05–1.16), critical illness (p = 0.044, OR 9.5, 95% CI 1.06–85.5), and SoC (compared to Anakinra) (p = 0.002, OR 11.2, 95% CI 2.47–51.1) were associated with development of any thromboembolic event (supplementary table).
Analysis after PS matching
After 1:1 PS matching, 88 patients in SoC and 88 patients in the Anakinra group were matched and included in the analysis. The baseline clinical and laboratory features of the patients are described in Table 1. Severe infection (28.4% vs 16%, p = 0.05; OR 3.9), development of any thromboembolic event (15.9% vs 3.4%, p = 0.005; OR 7.9), PTE (12.5% vs 3.4%, p = 0.026; OR 5), ACS (6.8% vs 0, p = 0.013; OR 6.2) were higher in SoC arm compared to Anakinra.
Patients who experienced any thromboembolic event had more frequent CHD (p = 0.04; OR 4.1), critical illness (p < 0.001; OR 12.5), lower hemoglobin and baseline ferritin levels (p = 0.03 and p = 0.04, respectively), higher mcHIS scores (p = 0.001), higher peak levels of CRP (p < 0.001), d-dimer (p < 0.001), LDH (p = 0.038). Furthermore, severe infection (41% vs 20.3%, p = 0.05; OR 3.9) and mortality (64.7% vs 27.7%, p = 0.002; OR 9.8) were higher in patients who had any thromboembolic event than those had not (Table 2). Similarly, PTE was higher in patients who had a critical illness (p = 0.002; OR 9.5), lower hemoglobin and ferritin levels (p = 0.02 and p = 0.04, respectively), higher mcHIS scores (p = 0.002), peak levels of CRP (p < 0.001), d-dimer (p < 0.001), pneumothorax (p = 0.03; OR 4.8), ACS (p < 0.001; OR 15), and mortality (p = 0.03; OR 4.7) (Table 3). PTE development was associated with peak levels of d-dimer levels (p = 0.02, OR 1.08, 95% CI 1.01–1.15) in multivariate analysis.
Development of ACS was higher in patients who had a history of CHD and malignancy (p = 0.007; OR 7.3 and p = 0.02; OR 5.5, respectively), critical illness (p = 0.02; OR 5.4), higher mcHIS scores (p = 0.02), peak levels of CRP (p = 0.043), d-dimer (p = 0.03), LDH (p = 0.004) (Table 4). ACS was also higher in SoC (P = 0.016; OR 6.2) and patients had mortality (p < 0.001; OR 13.7) in univariate analysis. Development of ACS was associated with the history of CHD (p = 0.038, OR 6.9, 95% CI 1.1–42.3) and PTE (p = 0.008, OR 11.5, 95% CI 1.9–69.5) in multivariate analysis.
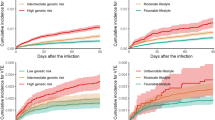
In survival analysis, development of any thromboembolic event, PTE, and ACS were higher in SoC compared to Anakinra [Log-Rank; p = 0.003 (Fig. 1), p = 0.003 (Fig. 2), and p = 0.007 (Fig. 3), respectively]. Survival rate was also lower in patients with the SoC arm than Anakinra in patients who had any thromboembolic event as well as ACS [Log-Rank; p = 0.03 (Fig. 4) and p < 0.001 (Fig. 5), respectively]. The survival rate of patients with and without PTE did not differ in patients with COVID-19 (Supplementary Fig. 4).

Development of any thromboembolic event in patients with COVID-19 according to the treatment groups (Kaplan–Meier survival analysis). Log-Rank; p = 0.003.

Development of pulmonary thromboembolism in patients with COVID-19 according to the treatment groups (Kaplan–Meier survival analysis). Log-Rank; p = 0.003.

Development of acute coronary syndrome in patients with COVID-19 according to the treatment groups (Kaplan–Meier survival analysis). Log-Rank; p = 0.007.

The survival rate of patients with COVID-19 according to the presence of any thromboembolic event (Kaplan–Meier survival analysis). Log-Rank; p = 0.03.

The survival rate of patients with COVID-19 (in the whole study group) according to the presence of acute coronary syndrome (Kaplan–Meier survival analysis). Log-Rank; p < 0.001.
ROC analysis revealed a cut-off value of d-dimer for the development of any thromboembolic event 16.75 (Area under curve [AUC] 0.804, p < 0.001 [95% CI 0.710–0.898]), for the development of PTE 14.97 (AUC 0.867, p < 0.001 [95% CI 0.774–0.960]), for the development of ACS 5.83 (AUC 0.736, p < 0.016 [95% CI 0.585–0.887]) (Supplementary Figs. 5, 6, and 7, respectively). Cut-off value of mcHIS score for the development of any thromboembolic event 3.5 (AUC 0.726, p = 0.001 [95% CI 0.632–0.821]), for the development of PTE 3.5 (AUC 0.740, p = 0.002 [95% CI 0.624–0.855]), for the development of ACS 3.5 (AUC 0.750, p = 0.01 [95% CI 0.630–0.870]) (Supplementary Fig. 8, 9, and 10, respectively). A cut-off value of peak levels of CRP for the development of any thromboembolic event 171.2 mg/L (AUC 0.780, p < 0.001 [95% CI 0.684–0.875]), for the development of PTE 201 mg/L (AUC 0.800, p < 0.001 [95% CI 0.694–0.905]), for the development of ACS 145.3 mg/L (AUC 0.743, p = 0.043 [95% CI 0.629–0.857]) (Supplementary Figs. 11, 12, and 13, respectively). Other results of ROC analysis are shown in Table 5 and Supplementary Figs. 14 and 15.
Discussion
It is well known that higher mortality rates and poor outcomes are mainly associated with the development of cytokine storms in patients with COVID-1918. Cytokine storm is a hyperinflammatory state that is seen in several conditions such as hematological malignancies, infectious diseases, and rheumatological conditions including adult-onset still disease (AOSD), and systemic lupus erythematosus19. Development of cytokine storm depends on the excessive production of several cytokines including interleukin-1 (IL-1), IL-6, tumor necrosis factor-alpha (TNF-α), and type 1 interferon (IFN) triggered by SARS-CoV-2 in COVID-1920. Recent studies revealed the importance of pulmonary macrophages’ activation secondary to SARS-CoV-2 (23), which results in inflammasome activation in COVID-1921,22. Inflammasomes are essential in the host defense against microorganisms including viruses that are present in various innate immune cells such as neutrophils, macrophages, and dendritic cells. Activation of inflammasomes leads to the cleavage of pro-IL-1β to produce active IL-1β23.
Anakinra is an IL-1 receptor antagonist which is widely used in several rheumatological diseases such as FMF, AOSD, and gout24,25,26 and also several hyperinflammatory conditions such as cancer-related hemophagocytic syndrome, chimeric antigen receptor-modified (CAR) T cell-associated cytokine storm, and macrophage activation syndrome27,28,29. Safety and efficacy of Anakinra was also established in COVID-19-associated cytokine storm3. Intravenous and high-dose anakinra is an emerging therapeutic option both in rheumatology practice, hyperinflammatory conditions, and COVID-1930,32,32. Although a study revealed a lack of efficacy with intravenous anakinra in patients with Multisystem Inflammatory Syndrome in Children (MIS-C), the anakinra dose was lower (4 mg/kg) in this study compared to our study33. Additionally, MIS-C has different pathogenetic mechanisms from COVID-19-associated cytokine storm which adaptive immune system activation is more prominent in the former one. Furthermore, the concomitant use of intravenous immunoglobulin as a background therapy may have influenced the outcome of the former study. Intravenous administration of anakinra ensures higher and faster maximum plasma concentration compared to the subcutaneous form34. Daily dose adjustment of anakinra may allow early intervention of the cytokine storm according to daily clinical status, as well as withdrawing the drug in case of infection or other complications. Additionally, intravenous high-dose anakinra treatment reduced mortality in our previous study13. Although the mortality rate was higher in the anakinra group compared to SoC before PS matching, it was thought to be related to a higher proportion of the patients with severe/critical disease in the anakinra group than in SoC. After adjusting confounder factors such as age, gender, disease severity, laboratory parameters (CRP, ferritin, d-dimer, LDH, NLR), and comorbidities with PS matching, the mortality rate tended to be lower in the anakinra group compared to the SoC. PS matching aims to ensure homogeneity and comparability between groups which includes potential bias due to the nature of a retrospective study.
Thromboembolic events are common in COVID-19 which is a remarkable finding from the beginning of the pandemic7. In the Middeldorp et al. study overall VTE frequency was 20% which was higher in patients in the ICU (47%) than ward (3.3%). In the former study, ICU admission, increased d-dimer, and NLR levels were associated with the development of VTE which were similar to our results. Furthermore, a study also revealed an association between the development of thrombosis and a prior history of CHD, critical disease, and increased d-dimer levels which were consistent with our results35. Moreover, the fact that higher values of peak levels of CRP, d-dimer, LDH, and ferritin than those baseline levels emphasize the crucial role of hyperinflammation in the development of thrombotic events in our study. COVID-19 patients have higher levels of d-dimer due to inflammation without an evident thrombosis, so reference values are not adequate and do not help in the diagnosis of thrombotic events in patients with COVID-197. Therefore establishing a cut-off of d-dimer for indicating thrombosis was important in patients with COVID-19 independent of the effect of COVID-19 itself.
In our study, the lower frequency of PTE in the anakinra group was a remarkable finding even though the anakinra group had more severe disease before PS matching. This finding persists after the PS matching procedure. As already known, endothelial dysfunction, thrombophilia, and stasis are the main contributors to the development of venous thrombosis according to Virchow’s triad. In COVID-19, endothelial dysfunction appears to be a more prominent factor in the development of thrombosis36. In our study, none of the patients with PTE had clinically evident DVT which suggests COVID-19-related pulmonary thrombosis is an in-situ thrombosis rather than embolism which was claimed by Gabrielli et. al. study37. In our study, all patients received background anticoagulant prophylaxis in two arms but could not prevent thrombotic events. This situation is recently defined as ‘inflammothrombosis’ which is similar to Behçet’s disease (BD) associated with venous thrombosis36,38. While DVT and PT (in situ thrombosis, not embolism) may develop in BD separately, DVT is not expected to cause embolism due to its inflammatory nature (firmly attached to the vascular wall). Therefore, the definition of pulmonary thrombosis may be more accurate than pulmonary embolism in patients with COVID-19 similar to BD. Furthermore, while anticoagulant therapy does not prevent vascular thrombosis in BD patients, anti-inflammatory treatment improves vascular outcomes such as recanalization and prevention of relapses39. However, it should be kept in mind that limited data is showing the efficacy of anti-inflammatory therapy as an anticoagulant effect in patients with COVID-19.
Inflammation is an important contributor to the development of cardiovascular events including ACS. During the pandemic arterial thrombotic events such as CVA and MI were increased in patients with COVID-1940,41. The NLRP3 (NOD [nucleotide oligomerization domain]-, LRR [leucine-rich repeat]-, and PYD [pyrin domain]-containing protein 3) [NLRP3] inflammasome, an innate immune signaling complex, is the key mediator of IL-1 family cytokine production. Recent evidence has shown that NLRP3 inflammasome activation has a crucial role in leading to higher IL-1 production for the development of ACS42. Furthermore, colchicine, an inflammasome inhibitor was found to be effective in the prevention of MI in patients with a history of ACS43. Similarly, canakinumab is an IL-1β monoclonal antibody that decreases composite cardiovascular events including MI, stroke, coronary revascularization, and cardiovascular death in the CANTOS study44. In our study, the decreased incidence of ACS with Anakinra was consistent with previous studies. Additionally, higher mcHIS scores in patients who had ACS compared with had not emphasized the crucial role of hyperinflammation in the development of arterial events similar to venous events.
This study has some strengths and limitations. The retrospective design of the study was the main limitation although the controlled design of the study adjusting potential confounders by PS matching was important to prevent bias. We could not perform Doppler USG screening in patients who had PTE since it did not cause a change in treatment and critical situation of the patients. Diagnosis of ACS could not be confirmed with cardiac catheterization due to the clinical status of extremely ill patients. Having missing data is also a limitation of the study. On the other hand, the fact that the study is conducted in a single center enables homogeneity in terms of patient population and treatment decisions that are made by a single physician.
Conclusions
Thromboembolic events were seen despite the anticoagulant prophylaxis in our study. The development of thrombosis was associated with hyperinflammation in patients with severe and critical COVID-19. Intravenous high-dose anakinra treatment decreases both venous and arterial events in patients with severe and critical COVID-19.
Data availability
The dataset of the study is available from the corresponding author upon reasonable request.
References
Verity, R. et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 20, 669–677 (2020).
Tufan, A., Avanoğlu Güler, A. & Matucci-Cerinic, M. COVID-19, immune system response, hyperinflammation and repurposing antirheumatic drugs. Turk. J. Med. Sci. 50, 620–632 (2020).
Kyriazopoulou, E. et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: A double-blind, randomized controlled phase 3 trial. Nat. Med. 27, 1752–1760 (2021).
Marconi, V. C. et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir. Med. 9, 1407–1418 (2021).
Horby, P. et al. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 384, 693–704 (2021).
Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet. 397, 1637–1645 (2021).
Asakura, H. & Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 113, 45–57 (2021).
Middeldorp, S. et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost 18, 1995–2002 (2020).
Tang, N. et al. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 18, 1094–1099 (2020).
Albani, F. et al. Thromboprophylaxis with enoxaparin is associated with a lower death rate in patients hospitalized with SARS-CoV-2 infection. A cohort study. EClinicalMedicine 27, 100562 (2020).
Lachant, D. J. et al. Chronic therapeutic anticoagulation is associated with decreased thrombotic complications in SARS-CoV-2 infection. J. Thromb. Haemost. 18, 2640–2645 (2020).
Sadeghipour, P. et al. Effect of intermediate-dose vs standard-dose prophylactic anticoagulation on thrombotic events, extracorporeal membrane oxygenation treatment, or mortality among patients with COVID-19 admitted to the intensive care unit: The INSPIRATION randomized clinical trial. JAMA 325, 1620–1630 (2021).
Bektaş, M. et al. High-dose intravenous anakinra treatment is safe and effective in severe and critical COVID-19 patients: A propensity score-matched study in a single center. Inflammopharmacology 31, 787–797 (2023).
COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. https://www.covid19treatmentguidelines.nih.gov/.
Webb, B. J. et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: A cohort study. Lancet Rheumatol. 2, e754–e763 (2020).
Salton, F. et al. Prolonged higher dose methylprednisolone versus conventional dexamethasone in COVID-19 pneumonia: A randomised controlled trial (MEDEAS). Eur. Respir. J. 61, 220514 (2023).
Collet, J. P. et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 42, 1289–1367 (2021).
Gustine, J. N. & Jones, D. Immunopathology of hyperinflammation in COVID-19. Am. J. Pathol. 191, 4–17 (2021).
Jarczak, D. & Nierhaus, A. Cytokine storm-definition, causes, and implications. Int. J. Mol. Sci. 23, 11740 (2022).
Chen, G. et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 130, 2620–2629 (2020).
Junqueira, C. et al. FcγR-mediated SARS-CoV-2 infection of monocytes activates inflammation. Nature 606, 576–584 (2022).
Sefik, E. et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature 606, 585–593 (2022).
Vora, S. M., Lieberman, J. & Wu, H. Inflammasome activation at the crux of severe COVID-19. Nat. Rev. Immunol. 21, 694–703 (2021).
Marko, L. et al. Anakinra for colchicine refractory familial Mediterranean fever: A cohort of 44 patients. Rheumatology (Oxford) 60, 2878–2883 (2021).
Giacomelli, R. et al. The treatment of adult-onset Still’s disease with anakinra, a recombinant human IL-1 receptor antagonist: A systematic review of literature. Clin. Exp. Rheumatol. 39, 187–195 (2021).
Saag, K. G. et al. A randomized, phase II study evaluating the efficacy and safety of anakinra in the treatment of gout flares. Arthritis Rheumatol. 73, 1533–1542 (2021).
Bami, S. et al. The use of anakinra in the treatment of secondary hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 67, e28581 (2020).
Strati, P. et al. Clinical efficacy of anakinra to mitigate CAR T-cell therapy-associated toxicity in large B-cell lymphoma. Blood Adv. 4, 3123–3127 (2020).
Grom, A. A., Horne, A. & De Benedetti, F. Macrophage activation syndrome in the era of biologic therapy. Nat. Rev. Rheumatol. 12, 259–268 (2016).
Chang, J. C. et al. Variation in early anakinra use and short-term outcomes in multisystem inflammatory syndrome in children. Arthritis Rheumatol. 75, 1466–1476 (2023).
Nigrovic, P. A. et al. Anakinra as first-line disease-modifying therapy in systemic juvenile idiopathic arthritis: Report of forty-six patients from an international multicenter series. Arthritis Rheum. 63, 545–555 (2011).
Mehta, P., Cron, R. Q., Hartwell, J., Manson, J. J. & Tattersall, R. S. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatol. 2, e358–e367 (2020).
Phadke, O., Rouster-Stevens, K., Giannopoulos, H., Chandrakasan, S. & Prahalad, S. Intravenous administration of anakinra in children with macrophage activation syndrome. Pediatr. Rheumatol. Online J. 19, 98 (2021).
Saunders, B. N., Kuijpers, M. V., Sloan, J. J. & Gertner, E. Continuous IV infusion of anakinra. Front. Pharmacol. 14, 1162742 (2023).
Bilaloglu, S. et al. Thrombosis in hospitalized patients with COVID-19 in a New York city health system. JAMA 324, 799–801 (2020).
Ahmed, S. Zimba, O. & Gasparyan, A. Y. Thrombosis in Coronavirus disease 2019 (COVID-19) through the prism of Virchow's triad. Clin. Rheumatol. 39, 2529–2543 (2020).
Gabrielli, M., Lamendola, P., Esperide, A., Valletta, F. & Franceschi, F. COVID-19 and thrombotic complications: Pulmonary thrombosis rather than embolism?. Thromb. Res. 193, 98 (2020).
de Maistre, E., Savard, P. & Guinot, P. G. COVID-19 and the concept of thrombo-inflammation: Review of the relationship between immune response, endothelium and coagulation. J. Clin. Med. 12, 7245 (2023).
Bettiol, A. et al. Vascular Behçet syndrome: From pathogenesis to treatment. Nat. Rev. Rheumatol. 19, 111–126 (2023).
Stein, L. K., Mayman, N. A., Dhamoon, M. S. & Fifi, J. T. The emerging association between COVID-19 and acute stroke. Trends Neurosci. 44, 527–537 (2021).
Knight, R. et al. Association of COVID-19 with major arterial and venous thrombotic diseases: A population-wide cohort study of 48 million adults in England and Wales. Circulation 146, 892–906 (2022).
Afrasyab, A. et al. Correlation of NLRP3 with severity and prognosis of coronary atherosclerosis in acute coronary syndrome patients. Heart Vessels 31, 1218–1229 (2016).
Tardif, J. C. et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N. Engl. J. Med. 381, 2497–2505 (2019).
Everett, B. M. et al. Inhibition of interleukin-1β and reduction in atherothrombotic cardiovascular events in the CANTOS trial. J. Am. Coll. Cardiol. 76, 1660–1670 (2020).
Acknowledgements
Many thanks to Prof. Ahmet Gül for shedding light on our way.
Funding
No specific funding was received from any bodies in the public, commercial, or not-for-profit sectors to carry out the work described in this article.
Author information
Authors and Affiliations
Contributions
M.B. and R.Ç. designed and planned the study, R.Ç., S.Y., M.A., M.H.U., and M.İ.K. collected the data, S.Y. and M.B. carried out the data evaluation and basic analyses, all authors contributed to the follow-up of the patients and interpretation of results. R.Ç. and M.B. wrote the first draft, and all authors provided critical feedback for the last version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Çakmak, R., Yüce, S., Ay, M. et al. Intravenous high-dose anakinra drops venous thrombosis and acute coronary syndrome in severe and critical COVID-19 patients: a propensity score matched study. Sci Rep 14, 12369 (2024). https://doi.org/10.1038/s41598-024-62079-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-62079-y
Keywords
This article is cited by
-
Viral sepsis: diagnosis, clinical features, pathogenesis, and clinical considerations
Military Medical Research (2024)
