
Abstract
Hematopoietic stem cell transplantation (HSCT) is a potentially curative therapy for several malignant and non-malignant hematologic conditions. However, patients undergoing HSCT are at increased risk of developing serious cardiovascular events. Whether cardiovascular risks differ by the type of transplantation strategy used, allogeneic versus autologous HSCT, is unknown. Leveraging the National Inpatient Sample (2016–2019), we assessed the incidence of early cardiovascular events by HSCT mode (allogeneic vs autologous). The primary outcome was the incidence of atrial fibrillation (AF). The secondary outcome was the occurrence of any major adverse cardiac events (MACE), defined as acute heart failure, myocardial infarction (MI), symptomatic atrial or ventricular arrhythmia or heart block, and cardiovascular death. Outcomes were compared between those undergoing allogeneic versus autologous HSCT. Multivariable regression, adjusting for cardiovascular and cancer-related factors, was used to define the association between pre-HSCT factors and MACE. We further assessed the effect of acute cardiovascular events on in-patient mortality by calculating adjusted odds ratio (aOR) with corresponding 95% confidence intervals (CI) and p-values. Overall, 64,705 weighted hospitalizations for HSCT were identified, of which 22,655 (35.0%) were allogeneic HSCT and 42,050 (65.0%) were autologous HSCT. The prevalence of AF was 9.1%, and 12.1% for any arrhythmia. In multivariable regression, allogeneic HSCT was associated with higher adjusted odds of peri-HSCT acute heart failure (aOR 2.64; 1.86–3.76; p < 0.0001), QT prolongation (aOR 1.40; 1.04–1.88; p = 0.025), MI (aOR 2.87; 1.16–7.11; p = 0.023), any major cardiovascular complication (aOR 1.16; 1.03–1.32; p = 0.016), and inpatient mortality (aOR 4.87; 3.60–6.58; p < 0.0001). Following cerebrovascular events, AF was the strongest predictor of mortality. Allogeneic HSCT was associated with higher odds of in-hospital cardiovascular complications among patients undergoing HSCT.
Similar content being viewed by others

Introduction
Nearly 100,000 people are diagnosed with aggressive leukemias and lymphomas every year in the United States1. Hematopoietic stem cell transplantation (HSCT) has emerged as a potentially curative therapy for patients with these aggressive hematologic malignancies2,3. HSCT dramatically improves the survival for malignancies and it is associated with up to > 90% 5-year survival in certain conditions4. However, HSCT is also associated with an increased risk of cardiovascular complications, including atrial fibrillation (AF), heart failure (HF), and other serious cardiovascular events5,6,7. Although there is considerable variation in published literature about the true incidence of these major cardiovascular complications, the comparative effect of different types of HSCT treatments and the risk of developing these cardiovascular complications is unclear.
Among other cardiovascular complications, HSCT appears to be associated with an increase in the risk of developing symptomatic AF5. AF and HF are the most common adverse cardiovascular events following HSCT and have been associated with adverse outcomes and increased risk of long-term mortality in these patients5,8,9. Our objective was to assess the incidence and predictors of developing adverse cardiovascular outcomes stratified by the allogenic vs autologous HSCT using a large nationally representative database.
Methods
Data source
From the National Inpatient Sample (NIS), we identified all patients treated with HSCT from 2016 to 2019 for any malignant condition. Hospital admissions before 2016 were excluded as the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) coding system came into effect in 2015. NIS is part of a family of databases developed under the Healthcare Cost and Utilization Project (HCUP) through a Federal-State-Industry Partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ) and is the largest publicly available inpatient healthcare database. NIS contains data on approximately 7 million unweighted and 35 million weighted hospitalizations each year which can be used to compute national estimates of healthcare utilization, costs, and outcomes10. Due to the de-identified nature of NIS, the need for informed consent and Institutional Review Board (IRB) approval was waived. The NIS adheres to the 2013 Declaration of Helsinki for the conduct of human research.
Study population
Patients undergoing HSCT were identified using International Classification of Diseases, 10th Revision, Procedure Coding System (ICD-10-PCS) codes “30243C0”, “30243G0”, “30243X0”, “30243Y0”, “30233C0”, “30233G0”, “30233X0” and “30233Y0” for autologous HSCT and “30243G2”, “30243G3”, “30243G4”, “30243U-”, “30243X2”, “30243X3”, “30243X4”, “30243Y2”, “30243Y3”, “30243Y4”, “30233G2”, “30233G3”, “30233G4”, “30233U”, “30233X2”, “30233X3”, “30233X4”, “30233Y2”, “30233Y3” and “30233Y4” for allogeneic HSCT. Patients aged < 18 years were excluded from this analysis.
Clinical and demographic characteristics and inpatient cardiovascular outcomes (AF, atrial flutter [AFL], supraventricular tachycardia [SVT], QT prolongation, ventricular tachycardia [VT], ventricular fibrillation [VF], first-degree atrioventricular [AV] block, second-degree AV block, third-degree AV block, sick sinus syndrome [SSS], cardiac arrest, acute heart failure [HF] exacerbation, cardiogenic shock, stroke, transient ischemic attack [TIA], type 2 myocardial infarction [MI], non-ST elevation MI [NSTEMI], ST-elevation MI [STEMI]), pericarditis and pericardial effusion were compared between patients undergoing allogeneic and autologous HSCT. The primary outcome was the incidence of atrial fibrillation (AF). The secondary outcome was the occurrence of any major adverse cardiac events (MACE), defined as acute heart failure, myocardial infarction (MI), symptomatic atrial or ventricular arrhythmia or heart block, and cardiovascular death. Data supporting the findings of this study are available from authors upon reasonable request.
Statistical analyses
Descriptive statistics are presented as frequencies and percentages with corresponding 95% confidence interval (CI) for categorical variables and as mean with corresponding 95% CI for continuous variables. Baseline characteristics and unadjusted outcomes were compared using the Pearson χ2 test and univariable logistic regression for categorical variables and univariable linear regression for continuous variables. For assessment of the independent association of type of HSCT with outcomes, a multivariable logistic regression model was utilized to calculate the adjusted odds ratio (aOR) with corresponding 95% CI and p-value. The multivariable regression model adjusted for demographics including age, sex, race/ethnicity, insurance status, median household income quartile, and underlying comorbidities, including hypertension, complicated and uncomplicated diabetes mellitus (DM), coronary artery disease (CAD), dyslipidemia, peripheral arterial disease (PAD), chronic HF, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), cerebrovascular disease, obesity, cirrhosis, anemia, thyroid dysfunction, tobacco use, alcohol use, substance use, hematologic malignancies (including Hodgkin’s lymphoma, non-Hodgkin’s lymphoma, multiple myeloma, acute and chronic myeloid leukemia, acute and chronic lymphoid leukemia, monocytic leukemia), and metastatic solid tumor disease. A p-value of < 0.05 was considered statistically significant. All statistical analyses were performed using the software Stata/BE version 17.0 (StataCorp).
Ethical approval
This material is the authors’ original work and has not been previously published elsewhere. The paper is not currently being considered for publication elsewhere. The paper reflects the authors’ own research and analysis in a truthful and complete manner. All authors have been personally and actively involved in substantial work leading to the paper and will take responsibility for its content. The NIS adheres to the 2013 Declaration of Helsinki for the conduct of human research. Due to the de-identified nature of the NIS database, the need for Institutional Review Board (IRB) approval was waived.
Informed consent
Due to the de-identified nature of the NIS database, the need for informed consent was waived.
Results
Overall, 64,705 weighted hospitalizations of patients undergoing HSCT were identified. Among these, 22,655 (35.0%) underwent allogeneic HSCT, and 42,050 (65.0%) underwent autologous HSCT. The mean age was 55.6 years, 41.3% were females, 67.9% were White, 12.5% were Black, 10.5% Hispanic, 3.2% Asian, and 0.3% were Native American.
Patients undergoing allogeneic compared to autologous HSCT were younger (average age 52.3 years vs 57.3 years, p < 0.001), and more likely to be female 43.8% vs 40.0%, p < 0.001), White (70.4% vs 66.6%, p < 0.001), Hispanic (11.5% vs 10.0%, p < 0.001) or Asian (4.2% vs 2.6%, p < 0.001), but less likely to be Black (7.8% vs 15.1%, p < 0.001). Allogeneic HSCT patients had a higher burden of comorbidities including cerebrovascular disease (1.8% vs 1.0%, p < 0.001), cirrhosis (0.5% vs 0.2%, p = 0.02), and coagulopathy (16.5% vs 14.2%, p = 0.003) but lower DM (13.9% vs 15.8%, p = 0.003), dyslipidemia (19.9% vs 23.4%; p < 0.001), CKD (4.9% vs 12.2%, p < 0.001), tobacco use (4.7% vs 6.4%, p < 0.001) and substance abuse (5.9% vs 7.6%, p < 0.001) compared to those undergoing autologous HSCT. Information on other clinical and demographic characteristics is available in Table 1. Information on indications for HSCT based on HSCT type is available in Data Supplement.
Comparison of in-hospital cardiovascular outcomes
The incidence of in-hospital cardiovascular events was 13.0%, with the most common being arrhythmias (12.1%), followed by acute HF exacerbation (1.2%). Allogeneic HSCT recipients had a higher incidence of inpatient mortality (4.6% vs 1.0%, p < 0.001), acute HF exacerbation (1.9% vs 0.9%, p < 0.001), cardiogenic shock (0.4% vs 0.2%, p = 0.033), type 2 MI (0.6% vs 0.2%, p < 0.001), pericardial effusions (2.2% vs 0.5%, p < 0.001), and pericarditis (0.3% vs 0.1%, p = 0.006) compared to autologous HSCT recipients on a crude analysis. The distribution of other relevant outcomes is shown in Table 2.
To assess the independent association of HSCT strategy with adverse outcomes, we used multivariable regression models, adjusted for potential confounders such as age, sex, race, insurance status, income quartile, CAD, PAD, chronic HF, cerebrovascular disease, CKD, anemia, coagulopathy, cirrhosis, thyroid dysfunction, and type of hematologic malignancy. On the adjusted analysis, allogeneic HSCT was found to be associated with higher odds of inpatient mortality (aOR 4.87; 95% CI 3.60–6.58; p < 0.0001), acute HF exacerbation (aOR 2.64; 95% CI 1.86–3.76; p < 0.0001), type 2 MI (aOR 2.87; 95% CI 1.16–7.11; p = 0.023), pericardial effusion (aOR 3.40; 95% CI 2.26–5.13; p < 0.001), pericarditis (aOR 3.38; 95% CI 1.34–8.51; p = 0.01) and any major adverse cardiovascular complication (aOR 1.16; 95% CI 1.03–1.32; p = 0.016). Figure 1 shows a comparison of cardiovascular outcomes between the allogeneic and autologous HSCT recipients.

Forest plot showing a comparison of cardiovascular outcomes including pericarditis, pericardial effusion, cardiac arrest, acute HF exacerbation, cardiogenic shock, type 2 myocardial infarction (MI), Non-ST-elevation MI, ST-elevation MI, any arrhythmia, major adverse cardiovascular complication and inpatient mortality between allogenic HSCT and autologous HSCT recipients after adjusting for demographic data including age, sex, race, insurance status, and median household income, comorbidities listed in Table 1 and underlying cancer type.
Comparative effect on AF and other serious arrhythmia risk
The overall burden of arrhythmias in patients undergoing HSCT patients was 12.1% and the most prevalent arrhythmia was AF (9.1%) followed by SVT (2.1%) and AFL (1.8%). Patients undergoing allogeneic HSCT had higher rates of QT prolongation (2.3% vs 1.6%, p = 0.013), but lower AF (8.4% vs 9.5%, p = 0.036) and AFL (1.4% vs 2.0%; p = 0.02) compared to those undergoing autologous HSCT on a crude analysis (Table 2). Results demonstrating a comparison of arrhythmia outcomes are shown in Fig. 2. In multivariable analysis, allogeneic HSCT was associated with higher odds of QT prolongation (aOR 1.40; 95% CI 1.04–1.88; p = 0.025); this association was independent of age, sex, race, insurance status, income quartile, and important comorbidities such as underlying CAD, chronic HF, hypertension, anemia, and coagulopathy on a multivariable logistic regression analysis. There was no difference in AF, AFL, SVT, VT, VF, first-degree AV block, second-degree AV block, third-degree AV block, SSS or cumulative arrhythmia prevalence. There was a trend towards higher odds of second-degree AV block (aOR 3.09; 95% CI 0.86–11.12; p = 0.084) with allogeneic HSCT.

Forest plot showing a comparison of all arrhythmias including atrial fibrillation, atrial flutter, supraventricular tachycardia, QT prolongation, ventricular tachycardia, ventricular fibrillation, 1st-degree AV block, 2nd-degree AV block, 3rd-degree AV block and sick sinus syndrome between allogenic HSCT and autologous HSCT recipients after adjusting for demographic data including age, sex, race, insurance status, and median household income, and underlying comorbidities listed in Table 1.
Comparative effect of cardiovascular events on inpatient mortality
The overall mortality rate among all HSCT recipients was 2.3%. Furthermore, the cardiovascular predictors of inpatient mortality among all HSCT recipients included AF (aOR 2.94; 95% CI 2.14–4.05; p < 0.001), CAD (aOR 2.11; 95% CI 1.44–3.08; p < 0.001), chronic HF (aOR 2.63; 95% CI 1.71–4.05; p < 0.001), dyslipidemia (aOR 0.55; 95% CI 0.37–0.81; p = 0.002), cerebrovascular disease (aOR 10.79; 95% CI 6.91–16.85; p < 0.001), anemia (aOR 2.19; 95% CI 1.39–3.43; p = 0.001) and coagulopathy (aOR 2.32; 95% CI 1.72–3.14) (Fig. 3). Cardiovascular predictors of mortality stratified based on HSCT type are available in Data Supplement.

Forest plot showing significant cardiovascular predictors of inpatient mortality in all HSCT recipients.
Discussion
In this large and nationally representative sample of HSCT recipients, we have shown that:
-
(1)
The overall arrhythmia burden in these patients is high (12.1%), with the most prevalent arrhythmia being AF (9.1%) followed by SVT (2.1%) and AFL (1.8%).
-
(2)
Allogeneic HSCT saw higher odds of QT prolongation. This association remained, even after accounting for age, gender, race, socioeconomic factors, and important comorbidities such as hypertension, DM, chronic HF, CAD, PAD, CKD, and obesity.
-
(3)
Allogeneic HSCT was associated with a greater than twofold relative increase in inpatient mortality, acute HF exacerbation, MI, pericarditis, and pericardial effusion, and an increase in the composite risk of any major cardiovascular complication.
-
(4)
Cardiovascular predictors of inpatient mortality among HSCT recipients included AF, CAD, chronic HF, dyslipidemia, cerebrovascular disease, anemia, and coagulopathy.
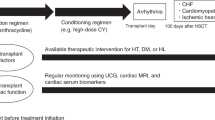
The Central Illustration (Fig. 4) shows an overview of the study design and results. The observation of increased cardiovascular event risk with HSCT, particularly allogeneic transplantation, adds to a growing body of literature. In smaller retrospective investigations, the increased burden of arrhythmia, particularly AF, has approached 20% in long-term follow-up11. Although a higher crude prevalence of AF and AFL was seen in the autologous HSCT group, upon adjustment for confounders, autologous HSCT was not found to be independently associated with higher odds of AF or AFL compared to the allogeneic HSCT group. Regarding arrhythmias, QT prolongation was the primary difference seen between the two populations, upon adjustment for confounders. The association of allogeneic HSCT with a higher prevalence of QT prolongation in comparison to autologous HCT could potentially be explained by differences in chemotherapeutic agents used for the underlying disease (e.g. cardiotoxic anthracyclines for AML), the potential need for prolonged antifungal and antibacterial prophylaxis, additional supportive measures including anti-emetics or a combination of these variables12,13,14,15. Allogeneic HSCT frequently requires immunomodulatory regimens to achieve myeloablation and minimize the risk of immunologic complications16. Notably, patients undergoing allogeneic HSCT were more likely to receive cytotoxic therapies which may contribute to cardiotoxicity17. Further, the engraftment of stem cells themselves may enhance the innate immune response, allowing a fertile state for enhanced arrhythmogenesis and atherosclerosis development, a condition more prominent than seen with autologous HSCT18. Although there has been a trend toward the avoidance of potentially cytotoxic agents in recent years, the presence of factors such as immunomodulation, immune activation following HSCT, and graft-versus-host effects may potentially enhance cardiovascular risk, even within months of HSCT19. Additionally, drugs such as cyclophosphamide used for graft-versus-host disease prophylaxis, have been associated with an increased risk for early (within 180 days post-transplantation) cardiovascular complications such as heart failure, pericarditis, acute coronary syndrome, and arrhythmia20,21. Allogeneic HSCT was also associated with higher odds of inpatient mortality and cardiovascular complications such as acute HF exacerbation and type 2 MI which could be attributed to the above-mentioned factors. Notably, these observations are compounded by the disparately increased longer-term risk of cardiovascular disease seen even within years of allogeneic transplant. However, additional prospective studies are needed to identify the drivers of cardiovascular disease among patients receiving HSCT.

Central Illustration depicting study design; AF atrial fibrillation, AFL atrial flutter, AV Block atrioventricular block, CAD coronary artery disease, CVD cerebrovascular disease, HF heart failure, HSCT hematopoietic stem cell transplantation, MI myocardial infarction, SSS sick sinus syndrome, SVT supraventricular tachycardia, VF ventricular fibrillation, VT ventricular tachycardia.
Among those undergoing allogeneic HSCT, underlying incident AF, chronic HF, CAD, CKD, cerebrovascular disease, anemia, and coagulopathy were predictors of inpatient mortality. Interestingly, dyslipidemia was noted to be associated with lower odds of inpatient mortality in the overall cohort and those undergoing allogeneic HSCT. Dyslipidemia can frequently be seen following allogeneic HSCT as a disorder of lipoprotein metabolism and is a major risk factor for CAD22,23. Recent evidence suggests that lipid-lowering therapy may have some role in modulating graft vs host disease and in improving cancer-associated survival in certain kinds of cancers24. Since the NIS does not provide data on in-hospital or outpatient pharmacologic therapies for patients, we are unable to determine whether subjects in our analysis were on lipid-lowering therapy. We suspect that a high proportion of subjects with dyslipidemia in our cohort may represent “treated dyslipidemia” and the unexpected finding of lower odds of inpatient mortality may potentially be from dyslipidemia treatment and its resultant effect on reduction in adverse cardiovascular events such as MI.
The observations are largely consistent with more isolated prior studies, which saw a higher incidence of adverse cardiovascular complications including heart failure, MI, stroke, and cardiovascular death in the long-term setting with either allogeneic or autologous HSCT alone9. The current study aligns with this, and shows higher risk of adverse cardiovascular events with contemporary allogeneic HSCT compared to autologous transplant. These findings are clinically significant as the use of allogeneic cell transplants continues to be expanded to wider populations. Allogeneic HSCT, as the only potentially curative treatment, is associated with lower relapse rates and better efficacy in specific populations such as those with acute myeloid leukemia, acute lymphoblastic leukemia, high-risk myelodysplastic syndrome, and multiple myeloma, however, the safety profile, particularly in the peri-HSCT setting, remains a concern as evidenced by our study25,26,27,28. Recognition of factors associated with adverse cardiovascular events is essential and aggressive control of cardiovascular risk factors in the peri-HSCT setting may help improve short and long-term non-relapse survival in these patients29. The development of predictive models such as the recently proposed CARE-BMT risk stratification score could aid in identifying (pre-transplant) high-risk patients who would benefit from timely referral to cardiovascular specialists for assessment and optimization of cardiovascular reserve prior to HSCT30,31. Strategies including the development and utilization of pre-HSCT risk stratification scores, identification of high-risk patients, the adoption of statin therapy to prevent treatment-induced CAD and cardiomyopathy, using cardiac biomarkers (troponin, natriuretic peptides) for early detection of cardiotoxicities, serial imaging to identify patients at risk of CAD or assessment of early left ventricular dysfunction, and the development of targeted novel strategies specific to HSCT-associated AF, such as immune-cell pathway targeted inhibition, may help further improve survival in these patients32,33,34,35,36. Additionally, there is growing data linking inflammatory pathway activation with cardiovascular outcomes, and monitoring immune activation markers (IL-1, IL-6, etc.) may have some role in long-term prognostication37. Prospective studies focused on identifying high-risk patients and specific management strategies to reduce cardiovascular risk are needed.
Limitations
The results of this study should be interpreted within the context of the following limitations. First, NIS is derived from administrative billing data that relies on ICD codes which may be subject to error. However, it is worth noting that AHRQ utilizes robust quality control measures which ensure data integrity10. Second, we are unable to address the incidence of cardiovascular complications in a time-dependent fashion and are unable to distinguish the history of arrhythmias from new-onset arrhythmias because of the lack of distinct ICD-10 distinguishing between the incident and old arrhythmias. It is important to note that this study also focused on early (peri-HSCT) events, and could not assess incidence of cardiovascular complications in a time-dependent manner. Thus, the true long-term incidence or ramifications of AF development following HSCT could not be defined (and is likely higher). Third, we focused on in-patient data, as NIS censors data upon discharge from the facility, therefore long-term or post-discharge follow-up outcomes and subsequent AF cannot be ascertained from the database. Fourth, NIS also censors medication administration data, thus precluding the analysis of chemotherapeutic agents used (for conditioning before HSCT). Additionally, NIS does not inform upon parameters such as hospital volume or center-specific monitoring policies and clinical practices which could impact the frequency of reporting cardiac events. Given the study's retrospective nature, causation cannot be concluded, and our results merely suggest an association.
Conclusion
In this large and nationally representative cohort of hospitalized patients undergoing HSCT, the overall prevalence of arrhythmias was high. Allogeneic HSCT was associated with worse cardiovascular outcomes and inpatient mortality, particularly among those with cardiovascular complications. These findings highlight the need for further prospective studies examining specific management strategies of cardiovascular comorbidities in the peri-HSCT setting to improve short and long-term clinical outcomes. Additional studies are needed to define the long-term incidence, mechanisms, and preventative strategies for HSCT-associated AF and other cardiovascular events.
Data availability
The datasets generated during and/or analysed during the current study are available in the [National Inpatient Sample (NIS)] repository, [https://hcup-us.ahrq.gov/nisoverview.jsp].
References
Siegel, R. L., Miller, K. D., Wagle, N. S. & Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 73, 17–48 (2023).
DeZern, A. E. et al. Haploidentical bone marrow transplantation in patients with relapsed or refractory severe aplastic anaemia in the USA (BMT CTN 1502): A multicentre, single-arm, phase 2 trial. Lancet Haematol. 9, e660–e669 (2022).
Bhatia, S. et al. Trends in late mortality and life expectancy after allogeneic blood or marrow transplantation over 4 decades: A blood or marrow transplant survivor study report. JAMA Oncol. 7, 1626–1634 (2021).
Martin, P. J. et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J. Clin. Oncol. 28, 1011–1016 (2010).
Chang, E. K. et al. Atrial fibrillation in patients undergoing allogeneic hematopoietic cell transplantation. J. Clin. Oncol. 39, 902–910 (2021).
Yeh, J. et al. Cardiac toxicity after matched allogeneic hematopoietic cell transplant in the posttransplant cyclophosphamide era. Blood Adv. 5, 5599–5607 (2021).
Armenian, S. H. & Chow, E. J. Cardiovascular disease in survivors of hematopoietic cell transplantation. Cancer 120, 469–479 (2014).
Krishan, S. et al. Association of atrial fibrillation and outcomes in patients undergoing bone marrow transplantation. Europace https://doi.org/10.1093/europace/euad129 (2023).
Vasbinder, A. et al. cardiovascular events after hematopoietic stem cell transplant. JACC: CardioOncol. 5, 821–832 (2023).
For Healthcare Research A, Quality. Overview of the national inpatient sample (NIS) (2020).
Tonorezos, E. S. et al. Arrhythmias in the setting of hematopoietic cell transplants. Bone Marrow Transplant. 50, 1212–1216 (2015).
Barreto, J. N. et al. QT prolongation in patients with acute leukemia or high-risk myelodysplastic syndrome prescribed antifungal prophylaxis during chemotherapy-induced neutropenia. Leuk Lymph. 60, 3512–3520 (2019).
Zeuli, J. D., Wilson, J. W. & Estes, L. L. Effect of combined fluoroquinolone and azole use on QT prolongation in hematology patients. Antimicrob. Agents Chemother. 57, 1121–1127 (2013).
Nousiainen, T., Vanninen, E., Rantala, A., Jantunen, E. & Hartikainen, J. QT dispersion and late potentials during doxorubicin therapy for non-Hodgkin’s lymphoma. J. Intern. Med. 245, 359–364 (1999).
Li, D. et al. Drug-induced QT prolongation and torsade de pointes: A real-world pharmacovigilance study using the FDA adverse event reporting system database. Front. Pharmacol. 14, 1259611 (2023).
Fasslrinner, F. et al. Long-term efficacy of reduced-intensity versus myeloablative conditioning before allogeneic haemopoietic cell transplantation in patients with acute myeloid leukaemia in first complete remission: Retrospective follow-up of an open-label, randomised phase 3 trial. Lancet Haematol. 5, e161–e169 (2018).
Saini, N. et al. Impact of TKIs post–allogeneic hematopoietic cell transplantation in philadelphia chromosome–positive ALL. Blood. 136, 1786–1789 (2020).
Tichelli, A. et al. Premature cardiovascular disease after allogeneic hematopoietic stem-cell transplantation. Blood 110, 3463–3471 (2007).
Gyurkocza, B. & Sandmaier, B. M. Conditioning regimens for hematopoietic cell transplantation: One size does not fit all. Blood 124, 344–353 (2014).
Pérez-Valencia, A. I. et al. Incidence, risk factors, and impact of early cardiac toxicity after allogeneic hematopoietic cell transplant. Blood Adv. 7, 2018–2031 (2023).
Duléry, R. et al. Early cardiac toxicity associated with post-transplant cyclophosphamide in allogeneic stem cell transplantation. JACC CardioOncol. 3, 250–259 (2021).
Griffith, M. L., Savani, B. N. & Boord, J. B. Dyslipidemia after allogeneic hematopoietic stem cell transplantation: Evaluation and management. Blood 116, 1197–1204 (2010).
Lacoste, L. et al. Hyperlipidemia and coronary disease. Correction of the increased thrombogenic potential with cholesterol reduction. Circulation 92, 3172–3177 (1995).
Longo, J., van Leeuwen, J. E., Elbaz, M., Branchard, E. & Penn, L. Z. Statins as anticancer agents in the era of precision medicine. Clin. Cancer Res. 26, 5791–5800 (2020).
Mizutani, M. et al. Comparable outcomes between autologous and allogeneic transplant for adult acute myeloid leukemia in first CR. Bone Marrow Transplant. 51, 645–653 (2016).
Goldstone, A. H. et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993). Blood 111, 1827–1833 (2008).
de Witte, T. et al. Value of allogeneic versus autologous stem cell transplantation and chemotherapy in patients with myelodysplastic syndromes and secondary acute myeloid leukemia. Final results of a prospective randomized European Intergroup Trial. Haematologica 95, 1754–1761 (2010).
Björkstrand, B. B. et al. Allogeneic bone marrow transplantation versus autologous stem cell transplantation in multiple myeloma: A retrospective case-matched study from the European group for blood and marrow transplantation. Blood 88, 4711–4718 (1996).
Majhail, N. S., Challa, T. R., Mulrooney, D. A., Baker, K. S. & Burns, L. J. Hypertension and diabetes mellitus in adult and pediatric survivors of allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 15, 1100–1107 (2009).
Vasbinder, A. et al. Cardiovascular risk stratification of patients undergoing hematopoietic stem cell transplantation: The CARE-BMT risk score. J. Am. Heart Assoc. 13, e033599 (2024).
Hayek, S. S. et al. Cardiovascular management of patients undergoing hematopoietic stem cell transplantation: From pretransplantation to survivorship—a scientific statement from the American heart association. Circulation https://doi.org/10.1161/CIR.0000000000001220 (2024).
Abdel-Qadir, H. et al. Statin exposure and risk of heart failure after anthracycline- or trastuzumab-based chemotherapy for early breast cancer: A propensity score-matched cohort study. J. Am. Heart Assoc. 10, e018393 (2021).
Hemu, M., Zimmerman, A., Kalra, D. & Okwuosa, T. Pretransplant cardiac evaluation using novel technology. J. Clin. Med. Res. 8, 690 (2019).
Proietti, M. et al. Relation of outcomes to ABC (atrial fibrillation better care) pathway adherent care in European patients with atrial fibrillation: An analysis from the ESC-EHRA EORP atrial fibrillation general long-term (AFGen LT) registry. Europace 23, 174–183 (2021).
Armenian, S. H. et al. National institutes of health hematopoietic cell transplantation late effects initiative: The cardiovascular disease and associated risk factors working group report. Biol. Blood Marrow Transplant. 23, 201–210 (2017).
Roziakova, L. et al. Serial measurements of cardiac biomarkers in patients after allogeneic hematopoietic stem cell transplantation. J. Exp. Clin. Cancer Res. 31, 13 (2012).
Ananthan, K. & Lyon, A. R. The role of biomarkers in cardio-oncology. J. Cardiovasc. Transl. Res. 13, 431–450 (2020).
Acknowledgements
The manuscript’s content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
This work was supported in part by an NIH P50-CA140158 grant. Dr. Addison is supported by NIH grant numbers K23-HL155890, R01HL170038, R01HL168045, and an American Heart Association‐Robert Wood Johnson Foundation Faculty Development Program grant. Dr. Quiroga is supported by a Robert A. Winn Diversity in Clinical Trials Career Development Award, funded by the Bristol Myers Squibb Foundation (non-profit), and an American Society of Clinical Oncology Young Investigator Award. Mr. Kola-Kehinde is supported by Ohio State University Comprehensive Cancer Center’s Pelotonia grant funds. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Author information
Authors and Affiliations
Contributions
All of the authors had full access to all of the data in the study, reviewed drafts of the manuscript, and approved the final version. Concept and design: S.K., D.A. Acquisition, analysis, or interpretation of data: S.K., Z.A., D.A. Drafting of the manuscript: S.K., Z.A., D.A. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: S.K. Administrative, technical, or material support: D.A. Supervision: D.A.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Krishan, S., Asad, Z.U.A., Quiroga, D. et al. Comparison of atrial fibrillation prevalence and in-hospital cardiovascular outcomes between patients undergoing allogeneic versus autologous hematopoietic stem cell transplantation: insights from the national inpatient sample. Sci Rep 14, 16829 (2024). https://doi.org/10.1038/s41598-024-65294-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-65294-9
