
Abstract
Hypophosphatemia (serum phosphate < 2.5 mg/dL) is a major concern when initiating nutritional support. We evaluated which factors contribute to hypophosphatemia development in critically ill patients, as well as the association between hypophosphatemia and mortality. A retrospective cohort study of patients who were ventilated for at least 2 days in a 16-bed mixed ICU. Data collected includes demographics, Acute Physiology & Chronic Health Evaluation 2 (APACHE2) admission score, Sequential Organ Failure Assessment score at 24 h (SOFA24), hourly energy delivery, plasma phosphate levels during the first 2 weeks of admission, ICU length of stay (LOS), length of ventilation (LOV), and mortality (ICU and 90 days). For the hypophosphatemia development model, we considered mortality as a competing risk. For mortality analysis, we used the Cox proportional hazards model considering hypophosphatemia development as a time-varying covariate. 462 patients were used in the analysis. 59.52% of the patients developed hypophosphatemia. Several factors were associated with a decreased risk of hypophosphatemia: age, BMI, pre-admission diabetes diagnosis, APACHE2, SOFA24, first kidney SOFA score, hospital admission time before ICU admission, and admission after liver transplantation. Admission due to trauma was associated with an increased risk of hypophosphatemia. Survival analysis with hypophosphatemia as a time-varying covariate showed a protective effect of hypophosphatemia from mortality (HR 0.447, 95% CI 0.281, 0.712). Age, APACHE2, and SOFA24 score were found to be significantly associated with ICU mortality. Fasting duration in the ICU before nutritional support initiation was not found to be significantly associated with hypophosphatemia. We examined several fasting intervals (12 h, 24 h, 36 h, 48 h, 60 h, 72 h). In each fast interval, we compared the prevalence of hypophosphatemia among patients who fasted the specified length of time, with those who did not fast for the same length of time. In each fasting interval, hypophosphatemia prevalence was lower in the fasting group compared to the non-fasting group. However, this difference was insignificant. BMI, APACHE2, and hospital LOS before ICU admission were inversely associated with hypophosphatemia development. Fasting for up to 72 h in the ICU before starting nutritional support did not affect hypophosphatemia occurrence. Hypophosphatemia was associated with lower mortality.
Similar content being viewed by others

Introduction
Refeeding syndrome (RFS) is a major concern in critically ill patients, due to its potential adverse cardiovascular and neurologic effects1. It is described as a range of metabolic and electrolyte derangements, usually due to reinitiating nutritional support after a period of fasting2. Patients are considered to be at risk for RFS after 5–10 days of undernourishment3. As RFS is not universally defined, its incidence cannot be clearly determined. Prospective work in an Italian medical ward found an incidence of 18%4, standing in line with a recent meta-analysis that reported a wide range of 0–62%5.
Hypophosphatemia (whether mild (2 ≤ Pi < 2.5 mg/dL), moderate (1 ≤ Pi < 2 mg/dL), or severe (Pi < 1 mg/dL)6,7 is considered the hallmark of refeeding syndrome2. Although hypophosphatemia has several other etiologies not related to RFS, most RFS definitions include hypophosphatemia8. Hypophosphatemia is found in 15–35% of critically ill patients6,9. While there is an ongoing debate regarding the effect of hypophosphatemia on mortality4,10,11,12,13, its effect on prolonging ventilation and LOS is well described4,7,9,12.
The duration of fasting and its effect on RFS and hypophosphatemia has not been extensively studied. The American Society for Parenteral and Enteral Nutrition (ASPEN) consensus defines RFS: “…after initiation of calorie provision to an individual who has been exposed to a substantial period of undernourishment”—but doesn’t state what is considered a substantial period2. Prolonged fasting (at least 72 h) causes physiological and pathophysiological changes, mainly basal metabolic rate decrease, increased fat utilization as an energy source, and vitamin and electrolyte depletion. The reinstitution of energy delivery from carbohydrates causes increases in adenosine triphosphate (ATP) production, which causes hypophosphatemia2,14,15. However, most clinical sources do not clearly define the fasting period prior to RFS4,5,7,16. Only scarce reports mention fast duration before energy delivery. In these studies, out of 123 patients who fasted between 3-65d, only 36 developed hypophosphatemia attributed to RFS17,18,19.
Critically ill patients are considered to be at risk for RFS2,3. Controversy exists regarding the initiation of energy delivery to critically ill patients. Some protocols favor restrictive energy delivery16, while others recommend higher and faster energy delivery2. A recent meta-analysis did not find a difference in outcome between both strategies20. We have recently demonstrated a correlation between lower daily energy deficit (i.e. higher daily energy delivery) and prolonged ventilation, with a trend toward decreased mortality in patients with hypophosphatemia21.
This study aimed to evaluate the factors contributing to the development of hypophosphatemia, including fast duration before nutritional support initiation, in critically ill ventilated patients, and to examine the association between hypophosphatemia and mortality in this population.
Methods
This study was approved by the Ethics Committee of Rabin Medical Centre (Approval no. RMC 0392-14). Since data were evaluated retrospectively, anonymously, and solely obtained for the study purposes, a requirement of informed consent was waived by Rabin Medical Centre ethics committee. All study methods were performed in accordance with Helsinki Declaration.
We conducted a retrospective analysis of data from the electronic medical charts of all ventilated patients who were admitted to a 16-bed general mixed medical-surgical adult ICU from Jan 1st 2017, till Oct 31st 2018. For patients who were admitted more than once in the ICU during the study period, only the first admission was used. Unventilated patients were considered ineligible for this study, as their oral calorie intake might not be recorded in their medical records. We excluded patients who were ventilated for less than 48 h (as they could start oral nutrition, which is not reported in the medical chart); who were not delivered energy at all during their admission (as energy delivery cannot be assessed in this population); and those who had hypophosphatemia within 12 h of admission (as it is likely that it appeared secondary to the critical illness per se).
Data obtained included sex, age at admission, body mass index (BMI), hospitalization dates, length of stay in ICU (LOS), readmissions number, the acute physiology and chronic health evaluation 2 (APACHE2) score, the sequential organ failure assessment score at 24 h from admission (SOFA24), ICU admission category (medical, surgical, trauma, obstetrics, transplantation (liver transplantations), length of ventilation (LOV), all phosphate levels in the first 2 weeks of admission (hourly time indexed from admission time), total hourly energy provided from enteral & parenteral nutrition (not including “hidden calories” from drugs or solutions) during the first 2 weeks of admission, ICU outcome (discharge to a hospital ward or a rehabilitation center, or ICU mortality), and mortality for up to 90 days after admission. Continuous variables are presented by median and interquartile range, and categorial variables by numbers and percentage. APACHE2 & SOFA24 score were considered as continuous variables.
APACHE2 (Acute Physiology and Chronic Health Evaluation 2) admission score is a commonly used and well-validated score for hospital mortality of critically ill patients, based on the patient’s age, baseline comorbidities, and 12 routine measurements taken during the first ICU admission day22,23.
SOFA (Sequential Organ Failure Assessment) score is a well-validated score for organ failure and mortality of critically ill patients. It is calculated based on six parameters, each representing a physiologic system. It can be calculated daily during ICU admission24.
Fast duration was defined as the duration of consecutive hourly 0 kcal delivery to a patient. We describe fast duration in groups of 12-h intervals up to 72 h of fasting, comparing patients who fasted the specific defined fast interval (12/24/36/48/60/72 h) with those who did not fast that whole interval. We focused on fasting during the first 3 days of admission, as our nutritional ward protocol is based on a locally developed protocol which principals are to initiate nutrition at a slow energy delivery rate, and progress to energy delivery target within 2 days (according to patient status)—inline with current restrictive energy delivery guidelines16.
In cases when a patient received energy delivery, and then started fasting again the longest fast duration was counted, had it occurred before hypophosphatemia developed. Hypophosphatemia occurrence (after the defined fast duration in the fasting groups) was described in fasting and non-fasting patients within each defined fasting interval; patients who had hypophosphatemia before or during the fasting period were excluded.
Hypophosphatemia was defined as a phosphate level lower than 2.5 mg/dL6,7. The primary endpoint was defined as hypophosphatemia development. Secondary endpoints were ICU mortality and 90 days mortality. For hypophosphatemia development we used Fine and Gray’s competing risk analysis25 considering mortality without hypophosphatemia as a competing risk. We analyzed which baseline variables contributed to developing hypophosphatemia. Intermediate variables (such as fast duration, ventilation length, and energy delivered to the patient) were not analyzed because these variables might be influenced by medical decisions taken with consideration of phosphate levels.
For mortality analysis we considered hypophosphatemia development (a variable that is not a baseline characteristic, but one that changes through the admission) as a time varying covariate26. The Cox proportional Hazards model was used for this analysis.
Statistical analysis was performed using SAS vs 9.4 (SAS Institute).
Ethical approval and consent to participate
This study was approved by the ethics committee of Rabin Medical Centre (RMC 0392–14).
Results
During the study period, there were 1335 admissions to the ICU. In 542 of them, the patient was ventilated for more than 48 h. There were 23 readmissions of 23 patients; 24 patients were not delivered energy at all; 33 had hypophosphatemia within 12 h of admission. Therefore, 462 patients were included in the final analysis (see Fig. 1 for study flowchart).

Flowchart of patients inclusion.
Baseline characteristics
Table 1 describes the baseline characteristics of the patients. Table 2 describes the hazard ratio of all characteristics for hypophosphatemia development in univariate analysis, considering mortality as a competing risk. All baseline characteristics but sex and surgical admission reason (compared to medical), were found significant for hypophosphatemia development). Except for trauma admission reason, all factors were associated with decreased risk for hypophosphatemia development.
Supplemental table S1 describes baseline characteristics by hypophosphatemia development during the first 14 days of admission. As mortality without hypophosphatemia is a competing risk, there are three options for hypophosphatemia development: mortality without hypophosphatemia, survival to ICU discharge without hypophosphatemia, or hypophosphatemia development. Patients who developed hypophosphatemia were younger, had lower BMI, lower prevalence of diabetes, lower APACHE2 score, lower SOFA24 score, and lower renal component on SOFA24 score; they tended to suffer more from trauma. Their first phosphate level was lower. Average time to hypophosphatemia development was 2.79 ± 2.19d.
Hypophosphatemia description
A total of 2805 phosphate measurements were used for the analysis, with a mean of 6.07 measurements per patient, i.e. a measurement every 1.4 days on average.
275 patients (59.53%) developed hypophosphatemia. Of those, 50 patients (18.18%) developed hypophosphatemia during the first day of their ICU stay; 77 (28%) during the 2nd day; 62 (22.55%) during the 3rd day; and 53 (12.36%) afterward. Most of the patients who developed moderate and severe hypophosphatemia did so during the first 48 h of their stay. See supplement table S2 for hypophosphatemia (according to severity) occurrence by days from ICU admission.
The average time for phosphate level to increase above the threshold of mild, moderate and severe hypophosphatemia (after hypophosphatemia was developed) was 53.83 ± 39.60 h, 39.63 ± 29.16 h, and 18.25 ± 10.97 h, respectively. See supplement table S3 for hypophosphatemia durations.
Multivariate analysis for hypophosphatemia development
For multivariate analysis, we included all baseline characteristics except the Kidney SOFA24 component and the first phosphate level. The former as it is part of the SOFA24 score, which was included in the analysis, and the latter is due to a missing phosphate level within 6 h from admission in 130 patients.
The model demonstrated that among the examined covariates, admission reason (with medical admission reason as reference), BMI, APACHE2 score, hospital admission time before ICU admission, and transplantation admission reason significantly decrease the risk for hypophosphatemia development (Table 3). Substituting SOFA24 score with kidney SOFA24 score slightly changes the results. Kidney SOFA24 score was found to be protective from hypophosphatemia development, while APACHE2 score became not significant. Other covariate significance did not change (supplemental table S4).
Fast duration and hypophosphatemia
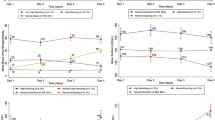
For hypophosphatemia development, we considered only baseline variables. Fast duration should be considered as an intermediate variable. i.e., a variable that is changed throughout the hospitalization; moreover, it might be affected by the phosphate level which might change over time. Hence, fast duration was not used as a covariate in the models presented above. Therefore, we evaluated hypophosphatemia occurrence in several different fasting durations. For each fast duration examined, we compared hypophosphatemia occurrence between patients who fasted for the specified duration and those who did not. Hypophosphatemia developed more often in the non-fasting patients, in each fast interval examined. However, these differences in hypophosphatemia rates were not significant between fasting and non-fasting patients, in all fasting intervals examined (see Table 4 and Fig. 2).

Hypophosphatemia rates among fasting and not-fasting patient in different fasting intervals.
Hypophosphatemia and mortality
To examine the association of hypophosphatemia and mortality, we performed a survival analysis with hypophosphatemia as a time varying covariate. Among covariates examined age, APACHE2 and SOFA24 score were found to be significantly associated with ICU mortality; BMI and hypophosphatemia were found to be inversely significantly associated with ICU mortality. Table 5a describes the hazard ratios of the different covariates with 95% confidence intervals. Survival analysis for 90 days mortality (Table 5b) showed similar results, excluding BMI as a significant covariate. Substituting SOFA24 score with kidney SOFA24 score as a covariate showed similar results with an exception in both models (ICU mortality and 90d mortality)—the kidney SOFA24 score was not found to be significantly associated with the outcome (Supplement table S5a and b). Supplement 6 describes further models regarding the interaction between kidney SOFA24, phosphate status, and mortality.
Energy delivery and patient outcomes
Table 6 describes the energy delivery and clinical outcomes of the patients. To describe differences between patients who developed hypophosphatemia and those who did not, it is based on the competing risk analysis possible outcomes. Therefore, parameters are calculated until event time (hypophosphatemia for patients who developed it; and either deathor discharge for patients who did not develop hypophosphatemia). Patients who developed hypophosphatemia had shorter durations of fasting. They were delivered less energy per hour during their admission. Their LOS and LOV were longer.
Discussion
Associated factors with hypophosphatemia development
Identifying risk factors for hypophosphatemia development in critically ill patients is challenging. Several clinical conditions predisposing to hypophosphatemia have been suggested, such as younger age12,21, higher APACHE score10,27, lower APACHE score21 medical reason of ICU admission10,27,28, and female sex27. Other works demonstrated no difference in these (or other) characteristics between patients who developed hypophosphatemia and those who did not1,29,30. As so, there is no consensus regarding the predisposing factors for hypophosphatemia development. Unlike previous studies1,11,21,27,28,29,30, in this study, we performed a multivariate analysis considering mortality as a competing risk, demonstrating several factors associated with increased risk for hypophosphatemia: Lower BMI, lower APACHE2 score, and shorter hospital LOS before ICU admission. Transplantation admission reason is associated with lower risk, while other admission reasons (compared to medical admission reason) carry no risk difference. There is no simple explanation for these effects—neither in our work nor in the other studies mentioned.
Fast duration before nutritional support initiation cannot be used as a covariate in this model, as it is an intermediate variable31. However, we found no difference in the rate of hypophosphatemia occurrence between fasting and non-fasting patients, in 6 different fasting intervals up to 72 h of fasting. To our knowledge, the effect of fasting duration before nutrition initiation has not been evaluated in critically ill patients. These results suggest that initiation of nutritional support (with restrictive energy delivery protocol as performed in our ICU) in a critically ill patient is safe (regarding hypophosphatemia development), at least within 72 h of admission. Studies evaluating energy delivery, usually involving ventilated patients21,28,30,32 (as precise energy delivery of unventilated patients is more challenging to document and may be inaccurate) are scarce; these studies focus on the association between energy delivery/deficit, hypophosphatemia and mortality, but not on fast duration before hypophosphatemia.
Energy delivery is another intermediate variable. In a previous study, we found higher energy delivery throughout ICU admission in patients who developed hypophosphatemia21. The results from the current study are somewhat contradictory, as the average hourly energy delivery to the patients who developed hypophosphatemia (30.50 ± 19.28 kcal/h) was lower compared to patients who did not develop hypophosphatemia (both survivors (38.35 ± 14.70 kcal/h) and non-survivors (33.21 ± 21.16 kcal/h). Adjusting energy delivery rate to patient weight reveals this difference is even smaller (see Table 6). It should be noted that we calculated hourly energy delivery to a patient until time of hypophosphatemia (in patients who developed it) and until death/discharge time (in patients who did not develop hypophosphatemia). Therefore, the slightly lower hourly energy delivery in the patients who developed hypophosphatemia merely reflects our restrictive energy delivery protocol. We start nutritional support in our ICU according to a locally developed protocol, mainly initiating nutrition in a slow rate of energy delivery, and progress to the energy target within 1–2 days according to patient status (in line with current guidelines suggesting restrictive energy delivery16, aiming to prevent hypophosphatemia). Thus, it is possible that comparing average hourly energy delivery until event time only emphasizes the lower energy delivery until achieving the caloric goal. Comparing energy delivery after hypophosphatemia development is not relevant to its development. Nevertheless, total energy delivered is larger in patients who developed hypophosphatemia 21. As the patients still have an energy deficit, it seems reasonable to assume a very low likelihood of overfeeding in these patients. This is reflected in this study in the weight and length of stay adjusted energy delivery, which is not greater than 0.5 kcal/Kg*h, a number reflecting average energy delivery of 12 kcal/Kg*d.
Hypophosphatemia and admission outcomes
The increased LOV and LOS, in patients who develop hypophosphatemia, is well described1,7,33, and are supported by our findings.
As for mortality, stating the obvious, multivariate analysis found age, APACHE2, and SOFA24 as significant factors associated both with ICU and 90 days mortality. BMI was associated with decreased ICU mortality (but not 90 days mortality). Hypophosphatemia was significantly associated with decreased ICU and 90 days mortality. The association between hypophosphatemia and mortality is a matter of debate in current literature7. Some works demonstrated higher mortality with hypophosphatemia28,29, while others found no effect of hypophosphatemia on mortality9,12,13,27, or decreased mortality10,21. Mortality from RFS is mostly due to cardiac arrhythmias, secondary to electrolytes disturbances. The mortality rate from RFS decreased from 38% in past reports to 17% in modern reports. The likely explanation is restrictive energy delivery, which was not as common in the past34.
The different effect of hypophosphatemia on mortality might be explained by different possible etiologies of hypophosphatemia (sepsis, burns, respiratory alkalosis, RFS) and their impact on mortality7. As the hazard ratio of hypophosphatemia and the associated risk of ICU mortality was 0.45 (95% CI 0.28–0.71) and 0.51 (95% CI 0.37–0.7) for 90 days mortality, and the effect of age and prognostic score on this association was much more subtle (the highest hazard ratio for 90 day mortality was of SOFA24 score, 1.13 (95% CI 1.07–1.19), it is possible to assume that in certain cases hypophosphatemia development might serve as a marker of recovery. A lower APACHE score was found to be associated with hypophosphatemia. Hence, one can assume that the protective effect of hypophosphatemia is merely the effect of the lower APACHE score. However, multivariate analysis found both APACHE and hypophosphatemia to be significantly associated with mortality (in opposite directions).
Hypophosphatemia is treated in our ICU according to a locally developed protocol. All ventilated patients are screened daily for hypophosphatemia development. Mild hypophosphatemia is treated with energy delivery decrement (or cessation) and/or enteral phosphate supplementation. Moderate and severe hypophosphatemia are treated with energy delivery cessation and enteral or parenteral phosphate supplementation (moderate or severe hypophosphatemia, respectively). The more severe the hypophosphatemia, the more aggressive the treatment, thus providing an explanation for the shorter duration of time in which patients are found with severe and moderate hypophosphatemia. This correction might mitigate the hypophosphatemia deterioration to cardiac arrhythmias, and explain the lower mortality with hypophosphatemia development, in contrast to what is expected regarding RFS mortality.
Fast, nutritional support, hypophosphatemia, and mortality
Fasting and hypophosphatemia are intermediate variables and thus an attempt at finding an association between them may introduce bias. However, we managed to identify several factors associated with hypophosphatemia development, including BMI, lower APACHE2 score, and lower hospital LOS before ICU admission. We did not observe a difference in hypophosphatemia rates in fasting and non-fasting patients. Also, the small difference in energy delivery to patients who developed hypophosphatemia is probably negligible. Hence, it seems reasonable to assume that progressive initiation of nutritional support, when prescribed based on a restrictive caloric goal, in mixed general critically ill patients, does not contribute to hypophosphatemia development. Aggressive hypophosphatemia screening and correction allows for avoiding some of hypophosphatemia’s adverse effects, suggesting a protective effect from mortality due to hypophosphatemia, even after adjusting to other severity scores. Whether hypophosphatemia can be considered as a marker of recovery21, is beyond the scope of this study.
Strengths and limitations
Our work has several limitations. First, its retrospective nature, makes it difficult to assess causality between factors. Second, we could not statistically estimate the interaction and influence of several intermediate variables, such as hypophosphatemia occurrence and initiation of nutritional support during an admission. Therefore, we performed only descriptive statistics for these variables. Third, we could not estimate the effect of energy delivered to the patient on hypophosphatemia. The main reason for this is the retrospective nature of the study, as a comparison cannot be made between patients who developed hypophosphatemia and those who didn’t due to the unclear direction and even the existence of a causal relationship between energy delivered and phosphate levels. Theoretically, this can be estimated only in a prospective study. Fourth, we have no data regarding energy delivery and fasting duration prior to ICU admission, nor regarding energy delivered from hidden calories; hidden calories were shown in a previous study to be quite common in the ICU, while supplying a median of 205 kcal/d35 or 2.6 kcal/Kg*d36. It seems reasonable to assume that this amount of calories can be considered as a substantial undernourishment to qualify as RFS risk factor. Therefore, as energy provided by hidden calories is not close to meeting caloric goal, it seems reasonable to consider the period when a patient doesn’t receive nutritional support as fast. However, we could find one report demonstrating lower phosphate levels only during first 2 days of treatment in COVID-19 patients with high doses of propofol (5000 mg/d) compared to non COVID-19 patients treated with a lower dose of propofol (1800 mg/d)37. It is possible that “hidden calories” ight have alter the results. Fifth, we did not fully assess the effects acute kidney injury and/or hyperphosphatemia might have on the results. patients suffering from acute kidney injury are highly unlikely to develop hypophosphatemia, yet their prognosis is generally considered worse. Moreover, they are also likely to develop hyperphosphatemia (emphasizing the fact that a patient who did not develop hypophosphatemia was not necessarily normophosphatemic throughout admission. However, multivariate analysis for mortality using kidney SOFA24 score (instead of SOFA24 score) demonstrated that kidney SOFA24 score is not associated with mortality. Moreover, several models examining only Kidney SOFA24, and phosphate status, demonstrated that phosphate status (whether hypophosphatemia or hyperphosphatemia) is an important factor in the clinical pathway between increased kidney SOFA24 and mortality (see supplement 6). We have no data regarding kidney injury developed during the admission.
Nevertheless, this work has several strengths. First, it represents a diverse critically ill patient population. Second, by considering mortality as a competing risk, we can avoid overestimation of hypophosphatemia occurrence, and better describe its associated factors. Third, by considering phosphate level as a time-varying covariate for mortality analysis, we can assume avoiding of immortal life bias. Fourth, our data showed no association between fast duration and hypophosphatemia—a finding with direct implications on clinical practice.
Conclusion
We found that higher BMI, higher APACHE2 score, and longer hospital LOS before ICU admission—are all inversely associated with hypophosphatemia development. Hypophosphatemia occurrence is similar in each fast duration before nutrition support initiation. Hypophosphatemia was found to have an inverse association with mortality which might suggest it has a protective effect.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
30 January 2026
The original online version of this Article was revised: The original version of this Article contained an error in affiliations, where the order of Affiliations 2 and 3 were swapped. The correct order of affiliations is “2 Industrial Engineering and Management, Ariel University, Ari’el, Israel.” and “3 Institute for Nutrition Research, Felsenstein Medical Research Centre, Petah Tikva, Israel.” The original article has been corrected.
References
Marik, P. E. & Bedigian, M. K. Refeeding hypophosphatemia in critically ill patients in an intensive care unit. A prospective study. Arch. Surg. 131(10), 1043–1047 (1996).
da Silva, J. S. V. et al. ASPEN consensus recommendations for refeeding syndrome. Nutr. Clin. Pract. 35(2), 178–195 (2020).
Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. 2006 [updated 2017] [Internet]. National Institute for Health and Care Excellence; 2017 [cited 2023 Apr 4]. Available from: https://www.nice.org.uk/guidance/cg32
Rinninella, E. et al. Incidence and impact of refeeding syndrome in an internal medicine and gastroenterology ward of an Italian tertiary referral center: A prospective cohort study. Nutrients 14(7), 1343 (2022).
Cioffi, I. et al. The incidence of the refeeding syndrome. A systematic review and meta-analyses of literature. Clin. Nutr. 40(6), 3688–3701 (2021).
Berger, M. M. et al. Prevalence of hypophosphatemia in the ICU—Results of an international 1-day point prevalence survey. Clin. Nutr. 40(5), 3615–3621 (2020).
Reintam Blaser, A. et al. Hypophosphatemia in critically ill adults and children—A systematic review. Clin. Nutr. 40(4), 1744–1754 (2020).
Friedli, N. et al. Revisiting the refeeding syndrome: Results of a systematic review. Nutrition. 35, 151–160 (2017).
Sin, J. C. K. et al. Hypophosphatemia and outcomes in ICU: A systematic review and meta-analysis. J. Intensive Care Med. 12, 885066620940274 (2020).
Wang, L., Xiao, C., Chen, L., Zhang, X. & Kou, Q. Impact of hypophosphatemia on outcome of patients in intensive care unit: A retrospective cohort study. BMC Anesthesiol. 19(1), 86 (2019).
Hoffmann, M., Zemlin, A. E., Meyer, W. P. & Erasmus, R. T. Hypophosphataemia at a large academic hospital in South Africa. J. Clin. Pathol. 61(10), 1104–1107 (2008).
Federspiel, C. K., Itenov, T. S., Thormar, K., Liu, K. D. & Bestle, M. H. Hypophosphatemia and duration of respiratory failure and mortality in critically ill patients. Acta Anaesthesiol. Scand. 62(8), 1098–1104 (2018).
Cohen, J. et al. Hypophosphatemia following open heart surgery: Incidence and consequences. Eur. J. Cardio-Thoracic Surg. 26(2), 306–310 (2004).
Mehanna, H. M., Moledina, J. & Travis, J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. 336(7659), 1495–1498 (2008).
Kraft, M. D., Btaiche, I. F. & Sacks, G. S. Review of the refeeding syndrome. Nutr. Clin. Pract. 20(6), 625–633 (2005).
Doig, G. S. et al. Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: A randomised, parallel-group, multicentre, single-blind controlled trial. Lancet Respir. Med. 3(12), 943–952 (2015).
Lubart, E., Leibovitz, A., Dror, Y., Katz, E. & Segal, R. Mortality after nasogastric tube feeding initiation in long-term care elderly with oropharyngeal dysphagia—The contribution of refeeding syndrome. Gerontology. 55(4), 393–397 (2009).
Dror, Y. et al. The impact of refeeding on blood fatty acids and amino acid profiles in elderly patients: A metabolomic analysis. JPEN J. Parenter. Enteral. Nutr. 37(1), 109–116 (2013).
Chen, L. J. Refeeding syndrome in Southeastern Taiwan: Our experience with 11 cases. WJG. 20(30), 10525 (2014).
Matthews-Rensch, K., Capra, S. & Palmer, M. Systematic review of energy initiation rates and refeeding syndrome outcomes. Nutr. Clin. Pract. 36(1), 153–168 (2021).
Statlender, L. et al. Correlations between first 72 h hypophosphatemia, energy deficit, length of ventilation, and mortality—A retrospective cohort study. Nutrients. 14(7), 1332 (2022).
Knaus, W. A., Draper, E. A., Wagner, D. P. & Zimmerman, J. E. APACHE II: A severity of disease classification system. Crit. Care Med. 13(10), 818–829 (1985).
Ho, K. M. et al. Comparison of acute physiology and chronic health evaluation (APACHE) II score with organ failure scores to predict hospital mortality. Anaesthesia. 62(5), 466–473 (2007).
Vincent, J. L. et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine (see contributors to the project in the appendix). Intensive Care Med. 22(7), 707–710 (1996).
Fine, J. P. & Gray, R. J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 94(446), 496–509 (1999).
Austin, P. C., Latouche, A. & Fine, J. P. A review of the use of time-varying covariates in the Fine-Gray subdistribution hazard competing risk regression model. Stat. Med. 39(2), 103–113 (2020).
Suzuki, S. et al. Hypophosphatemia in critically ill patients. J. Crit. Care. 28(4), 536.e9-536.e19 (2013).
Miller, C. J. et al. Impact of serum phosphate in mechanically ventilated patients with severe sepsis and septic shock. J. Intensive Care Med. 35(5), 485–493 (2020).
Shor, R. et al. Severe hypophosphatemia in sepsis as a mortality predictor. Ann. Clin. Lab. Sci. 36(1), 67–72 (2006).
Olthof, L. E. et al. Impact of caloric intake in critically ill patients with, and without, refeeding syndrome: A retrospective study. Clin. Nutr. 37(5), 1609–1617 (2018).
Ananth, C. V. & Schisterman, E. F. Confounding, causality, and confusion: The role of intermediate variables in interpreting observational studies in obstetrics. Am. J. Obstet. Gynecol. 217(2), 167–175 (2017).
Coşkun, R., Gündoğan, K., Baldane, S., Güven, M. & Sungur, M. Refeeding hypophosphatemia: A potentially fatal danger in the intensive care unit. Turk. J. Med. Sci. 44, 369–374 (2014).
Alsumrain, M. H. et al. Association of hypophosphatemia with failure-to-wean from mechanical ventilation. Ann. Clin. Lab. Sci. 40(2), 144–148 (2010).
Boateng, A. A., Sriram, K., Meguid, M. M. & Crook, M. Refeeding syndrome: Treatment considerations based on collective analysis of literature case reports. Nutrition. 26(2), 156–167 (2010).
Bousie, E., Van Blokland, D., Lammers, H. J. W. & Van Zanten, A. R. H. Relevance of non-nutritional calories in mechanically ventilated critically ill patients. Eur. J. Clin. Nutr. 70(12), 1443–1450 (2016).
Slingerland-Boot, R., Kummerow, M., Arbous, S. M. & Van Zanten, A. R. H. Association between first-week propofol administration and long-term outcomes of critically ill mechanically ventilated patients: A retrospective cohort study. Clin. Nutr. 43(1), 42–51 (2024).
Viana, M. V. et al. Specific nutrition and metabolic characteristics of critically ill patients with persistent COVID-19. J. Parenter Enteral. Nutr. 46(5), 1149–1159 (2022).
Author information
Authors and Affiliations
Contributions
LS & OR equally contributed to this manuscript. LS—Conceptualization, Methodology, Investigation, Data curation, Writing—Original Draft, Writing—Review & Editing; OR—Conceptualization, Methodology, Investigation, Data curation, Writing—Original Draft, Writing—Review & Editing; TS—Methodology, Software, Validation, Formal Analysis, Writing—Review & Editing; ER—Data curation, Writing—Review & Editing; MH—Investigation, Data curation; IB—Investigation, Data curation; GF—Investigation, Data curation, PS—Conceptualization, Writing—Original Draft, Writing—Review & Editing, Supervision; IK—Conceptualization, Writing—Review & Editing, Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Statlender, L., Raphaeli, O., Shochat, T. et al. Contributing factors to hypophosphatemia development in critically Ill ventilated patients: a retrospective cohort study. Sci Rep 14, 19771 (2024). https://doi.org/10.1038/s41598-024-68688-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-68688-x
