
Abstract
The 5-year survival is poor for stage IV non-small cell lung cancer (NSCLC). Recently, cell immunotherapy has emerged as a new treatment strategy. This study aimed to evaluate the efficacy and safety of Immune killer cells (IKC) in patients with stage IV NSCLC after the failure of prior chemotherapy. This study enrolled 26 patients with stage IV NSCLC who failed at least two lines of chemotherapy with or without targeted therapy. The IKC was given alone weekly for 24 weeks. The primary endpoint was progression-free survival (PFS). Secondary outcomes included overall survival (OS), pain intensity, quality of life (QOL), and safety. The median PFS for the intent-to-treat (ITT) population (i.e., all enrolled patients) was 3.8 month. In the per-protocol (PP) population (i.e., patients receiving > 12 IKC infusions), the median PFS was 5.6 months. Moreover, the ITT population showed a 1-year survival rate of 60.0%, while that for the PP population was 85.7%. Only 7 out of 200 AEs (3.5%) were related to the IKC infusion, and they were all rated as grade 1 in severity. The IKC infusion was well tolerated. This novel immunotherapy prolonged the PFS and improved the survival compared with historical data. It might be a potential treatment strategy for stage IV NSCLC patient who failed prior chemotherapy.
ClinicalTrials.gov identifier: NCT03499834.
Similar content being viewed by others
Introduction
Lung cancer is the leading cause of cancer death worldwide1. Most patients are diagnosed with an advanced stage due to the late appearance of symptoms2. Despite recent advances in treatment for lung cancer, the five-year survival rate remains poor3. Currently, the primary treatment modalities for lung cancer include tyrosine kinase inhibitors (TKIs), immune checkpoint inhibitors, and chemotherapy agents, among others. If a patient has a driver mutation, TKIs are used as the initial treatment. If no driver mutation is present, chemotherapy combined with immunotherapy is recommended. The treatments after tyrosine kinase inhibitor (TKI) failure or immunotherapy failure currently still are chemotherapy. However, the response to this is poor4. Therefore, new strategies for lung cancer treatment are needed.
Cancer treatment with immune cells infusion, in which the cells are cultured and engineered ex vivo, has been used since the 1980th. Previous studies have demonstrated that, via IL-2 stimulation and TCR-CD3 engagement, Th2 lymphocytes would convert to the Th1 type and restore anti-tumor killing of the autologous tumor. These results suggest that non-small cell lung cancer patients may have their immunosuppressed status reversed5,6,7. Other studies have cultured and stimulated mononuclear cells from peripheral blood via IL-2, IFN-α, or IFN-γ and have then transfused the blood cells back to the patient for cancer treatment. All of these studies have reported improvements in either progression free survival (PFS), overall survival (OS), or quality of life (QOL)8,9,10,11.
Many studies have demonstrated that immune cell therapies are efficient. Immune cell therapies may be efficient for lung cancer because the lungs are richly endowed with immune cells12,13. Our previous studies have demonstrated that cytokine-stimulated cytotoxic T cells exhibit high levels of cytotoxic activities against autologous tumor cells6,7. Further, there is adoptive T-cell therapy in checkpoint inhibitor-resistant cancer14. A pilot study has established that immune checkpoint inhibitors increase the anti-tumor activity of adoptive T cells for lung cancer in vivo, as well15. Therefore, it is reasonable to explore these immune killer cells (IKC) as an efficient option for lung cancer treatment either to be used alone or in combination with immune checkpoint inhibitors.
Immune cell therapies are increasingly being recognized as a treatment option. Most immune cell therapies employ similar methods of ex vivo expansion and culture and activation of immune cells from patients’ peripheral blood mononuclear cells (PBMCs) in an external environment. Unlike traditional cancer treatments that aim to eradicate cancer cells, immune cell therapies focus on the improvement of the patients’ own anti-cancer abilities16,17,18. However, the efficacy of IKC treatment for lung cancer is not clear.
The aim of this single-arm, multi-center, phase II trial is to evaluate the safety and efficacy of immune killer cells (IKCs) in patients with stage IV non-small cell lung cancer (NSCLC) who have undergone at least two lines of chemotherapy, with or without targeted therapy. These IKCs were prepared using a patented process, involving the isolation of mononuclear cells from peripheral blood, their culture with specific reagents, stimulation with IL-2, and subsequent harvesting.
Materials and methods
Study design
This was an open-labeled, single-arm, multicenter, phase II trial conducted at Taipei Veterans General Hospital and Tri-service General Hospital in Taiwan. This study enrolled patients with stage IV (by American Joint Committee on Cancer 7th edition staging criteria) NSCLC. These patients must have undergone at least two lines of chemotherapy. For patients with an EGFR mutation, they should have received EGFR-TKI therapy. All eligible patients received IKC infusion as a monotherapy once a week for 24 weeks, and were followed up to 6 months after the last IKC infusion.
This study was approved by the institutional review board (IRB) at Taipei Veterans General Hospital (IRB No: 2017-05-007B) and Tri-service General Hospital (IRB No: 2-106-04-001). All study procedures were conducted in accordance with the Good Clinical Practice guidelines, the principles of the Declaration of Helsinki, and local laws. All patients provided written informed consent before enrollment (ClinicalTrials.gov identifier: NCT03499834). The date of first trial registration was 17/04/2018.
Study population
Patients aged at least 20 years old and diagnosed with histologically or pathological confirmed stage IV NSCLC, regardless of EGFR mutation status, were eligible for this study. For patients harboring EGFR mutation, those who experienced disease progression following EGFR-TKI treatment and at least two previous chemotherapy regimens (with one of them being platinum-based chemotherapy) were enrolled. For patients with wild-type EGFR, those with two failed chemotherapy regimens (one must contained platinum-based chemotherapy) were eligible. Eligibility criteria also included Eastern Cooperative Oncology Group (ECOG) performance status 0–2, measurable disease per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, and adequate liver, renal, and bone marrow functioning.
Exclusion criteria included recent major surgery, whole blood transfusion, chemotherapy, hormone therapy, targeted therapy, immune-modulating medications, immunotherapy, or other investigational products within 4 weeks of the peripheral blood collection; metastasis involving the central nervous system, pancreas, colon, or rectum; prior organ transplantation; severe infection; uncontrolled hypertension; congestive heart failure; myocardial infarction; stroke; coronary/peripheral artery bypass surgery; uncontrolled arrhythmia; human immunodeficiency virus infection; active tuberculosis; autoimmune disease; other active malignancies; or any disease rendering them unsuitable to join this study. Pregnant or breast-feeding women and women planning to get pregnant were also excluded.
IKC preparation
Peripheral blood (30 mL) for manufacturing the individualized IKC was collected 2 weeks before beginning the IKC therapy, and every week thereafter for 24 weeks.
The IKC was prepared by Ivy Life Sciences Co. Ltd. following a patented manufacturing process (USPTO Patent Certificate: US 9222072; Invention Name: Manufacturing Method of Immune Killer Cells) in compliance with Good Tissue Practices (GTP). Mononuclear cells were briefly isolated from peripheral blood and incubated in AIM-V (Thermo Fisher Scientific, Grand Island, NY) culture medium containing 200–1000 IU/mL proleukin (Boehringer Ingelheim RCV GmbH & Co KG, Vienna, Austria), 0.1–30 g/mL concanavalin A (Sigma-Aldrich, Saint Louis, USA), and 5–12% autologous human serum (by patient) at a density of 0.5–2 × 106 cells/mL, at 37 °C in a 5% CO2, 95% humidified atmosphere for 2–6 days. Next, the mononuclear cells were transferred to a new culture medium and stimulated with 200–600 IU/mL IL-2 (Boehringer Ingelheim RCV GmbH & Co KG, Vienna, Austria). Fresh medium with 100–500 IU/mL IL-2 (Boehringer Ingelheim RCV GmbH & Co KG, Vienna, Austria) was added every 2–3 days to maintain the concentration of cells at 0.6–2 × 106 cells/mL. On Day 14, the IKCs were harvested and analyzed for phenotype and cytotoxicity. Quality control and a sterility test were performed during the courses of cell culture.
All products were free of mycoplasma, bacterial, and fungal contamination; and contained < 0.25 EU/mL endotoxin and < 31.2 pg/mL IL-2. Each IKC cell consisted of 0.5–2.5 × 109 cells, with cell viability > 70%.
Phenotype detection
The phenotype of IKC was detected according to the IKC Standard Operating Procedures (SOP) protocol. Briefly, 1 × 106 cells (100 µL) were incubated with antibodies (CD3 FITC/CD56 PE/γδ PC7, CD8 FITC/CD4 PE/CD28 PC7, and IgG1 FITC/PE/PC7 from Beckman Coulter In, [Brea, CA, USA]) for 20 min at 20–25 °C away from light. After incubation, cells were centrifuged for 1 min at 2000× rpm at 4 °C and washed with Ice-Buffer (Normal Saline with 2% FBS, 0.5 mL). The cell population was analyzed using flow cytometry (Cytomics FC500 Flow Cytometer; Beckman Coulter, Inc.).
For the evaluation of the immune status of IKCs, cluster of differentiation CD3− CD56+, CD3+ CD56+, CD3+ CD56−, CD4, CD8, and CD28 cells were determined respectively. Cells were stained according to the IKC SOPs protocol. Data were analyzed using CXP Analysis Software (V2.2; Beckman Coulter, Inc.). The IKCs contained cytotoxic T lymphocyte (CTL, CD3+CD4-CD8+, 20–95%), Natural killer T cells (NKT) cells (CD56+CD3+, 3–80%), NK cells (> 0–45%), and γδT cells (> 0–45%).
Cytotoxicity assay
First, the target cells, K562 cells, were labelled with 5-μM CFSE for 20 min in a 5% CO2 incubator at 37 °C. After labelling, target cells (1 × 106 cells/mL) were incubated with effector cells at a ratio of effector to target cells of 1:1, 5:1, and 25:1 in triplicate sets for 4 h in a 5% CO2 incubator at 37 °C. At the end of incubation, each well was mixed with the nucleic acid stain (Propidium iodide) for 30 min in the dark. The IKCs were then analyzed for cytotoxicity using flow cytometry (Cytomics FC500 Flow Cytometer; Beckman Coulter, Inc.). The percentage of specific lysis (%) was calculated as follows: 100%× (cell lysis in the presence of effector cells minus cell lysis in the absence of effector cells/100 minus cell lysis in the absence of effector cells).
Efficacy evaluation
The primary end point is to evaluate progression-free survival (PFS) after receiving IKC treatment. A previous study reported that the PFS among those patients who received salvage chemotherapy was around 1.1 months19. We expected the PFS of IKC infusion to be at least 1 month better than historical control for consideration as a potential effective treatment. The second set of outcome measures included: the overall survival (OS) after IKC treatment, health related quality of life (HRQOL) before and after IKC treatment, and safety.
Treatment
Peripheral blood was collected beginning at the second visit and then every week thereafter for 24 weeks. After collection, the blood was sent to be cultured for 2 weeks. The first IKC infusion was performed at the 4th visit and then every week thereafter until the 27th visit (for a total of 24 times). The IKCs were infused weekly until the tumor progression was observed. Patients were not allowed to participate in this trial if their IKCs were less than 0.5 × 109 after culturing the first instance. IKC infusion was a monotherapy for this trial. None of the following treatments were allowed to be combined with IKC infusion: chemotherapy, radiotherapy, immunotherapy, hormone therapy, targeted therapy, traditional Chinese medicine, or high dose steroids (more than 20 mg per day).
Study assessment
Chest CT scans (including the liver and adrenal glands) were performed before the IKC infusion to serve as baseline. Radiological assessments were performed every 8 weeks. PFS was measured from the day patients began IKC infusions until termination of the trial. Disease progression was defined as either tumor progression or all-cause mortality, which means all deaths regardless of the cause, during the trial. OS were calculated from the day patients began IKC infusions until patients died or lost follow up. Quality of life was compared with the baseline to observe the change. Safety analysis was based on the incidence, rate of adverse effects, serious adverse effects, severity of effects, and patient numbers.
Statistical analysis
The primary outcome of this trial was PFS. The minimum follow up time was 7 months. In order for Type I Error to be 0.05 and statistical power to be 80%, 22 patients needed to be recruited. The dropout rate was expected to be 15%, so 26 patients needed to be enrolled. PFS and OS were obtained by using Kaplan–Meier methods. Quality of life and safety were evaluated by the Wilcoxon signed-rank test.
Results
Patients
In total, 26 patients were enrolled between Dec 15th, 2017, and Feb 11th, 2020. All patients had previously received at least 2 lines of chemotherapy. The first line is usually platinum-based doublet chemotherapy. The second line chemotherapies included docetaxel, gemcitabine, navelbine, pemetrexed, etc. One patient died before possible IKC treatment. A total of 25 patients received at least one IKC infusion. These patients were defined as the intention to treat (ITT) population. Fourteen patients received more than 50% IKC infusion of planned injection cycles and they were defined as the per protocol (PP) population (Fig. 1). Demographic data are listed in Table 1. The median age, gender, height, body weight, HBsAg, HCV, HIV, and ECOG were similar between the ITT and PP populations.

Consort diagram. Total 26 patients were enrolled. One patient died before IKC infusion. During IKC infusion, 11 patients withdrawal because of disease progression or by physician’s judgement. 14 patients received ≧ 12 times of IKC infusion and was defined as per protocol (PP) population. NSCLC non-small cell lung cancer, TKI tyrosin kinase inhibitor, IKC immune killer cells, ITT intention to treat population, PP per protocol population.
Treatment response
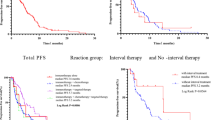
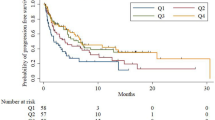
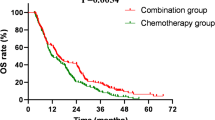
The median PFS of the ITT population and the PP population were 3.8 months and 5.6 months, respectively (Fig. 2). The one-year survival rate was 60%. The median OS is not reached among our patients (Fig. 3). The infused cells were mostly composed of CTL and NKT (Fig. 4). The response rate is listed in Table 2. The median tumor size was initially 36 mm (12–158 mm). After treatment, the median tumor size was 51 mm (16–149 mm). Overall, the best response to the treatment was a partial response in one patient. The tumor was stable among 14 patients. Five patients suffered from progression of their disease. In this study, 9 patients were EGFR mutated, 6 patients were EGFR wild type, and the status of 5 patients were unknown. The response rate was not correlated with the numbers of CTL, the numbers of NKT, or EGFR status. The waterfall plot of best response is illustrated in Fig. 4.

Progression free survival curve of ITT Population (upper) and PP population (lower).

Overall survival curve of ITT population (upper) and PP population (lower).

Waterfall plot of IKC infusion. The objective response rate were not associated with EGFR status, infused IKC amount, CTL percentage, or NKT percentage.
Pain visual analogue scale (VAS) and quality of life (QOL)
The baseline pain VAS scale was 2.0 (± 1.6) and 1.9 (± 1.6) among the ITT and the PP populations, respectively. The record of VAS scale is displayed in Supplement 1. The changes in VAS scale between baseline VAS and IKC infusion did not reflect significant differences. The baseline QOL was 93.7 (± 13.5) and 97.5 (± 13.3) among the ITT and the PP population, respectively. The QOL at each visit did not differ significantly compared with the baseline. The record is illustrated in Supplement 2.
Safety
There was a total of 200 AEs reported during our trial, but 177 of these AEs were unrelated to IKC treatment (see Supplement 3). Among the reported AEs, most were Grade 1. However, 135 AEs (67.5%) required medical treatment and 19 AEs required hospitalization (see Table 3). AEs most often affected the respiratory system (72.0%), followed by the gastrointestinal system (48.0%) and administration site (48.0%). Among the respiratory system AEs, the most common symptoms were cough (44.0%) and dyspnea (28.0%).
There were seven AEs that were probably/possibly related to IKC infusions in four patients. Two patients exhibited Grade 1 fatigue, one patient exhibited Grade 1 fatigue on two occasions, one patient experienced Grade 1 myalgia, and two patients experienced Grade 1 cough. No Grade 2 or higher severities were reported. Other AEs were related Gastrointestinal disorder, infections, metabolic disorders, respiratory disorders, and cancer itself.
Discussion and conclusion
In this phase II trial, the PFS was 5.6 months among the PP population. In addition, the PFS was 3.8 months among the ITT population. These results were better than the historical control of similar NSCLC patients who received salvage therapy as third line treatment19.
In this study, PFS and objective response rate were not correlated with EGFR status, the number of IKC cells injected per cycle, CTL percentage, or NKT percentage. Despite the progress of cancer genomics, immunology, and cell manufacturing, the number of successful cases of adoptive cell treatment for solid tumors is still limited20. Patient responses to adoptive cell transfusions have varied in different trials21,22,23. However, there are no biomarkers that could have predicted the response of adoptive cell treatment. Also, it is difficult to draw a conclusion based on our limited number of patients. However, there may be a hint that the response of IKC infusions was not associated with EGFR status or CTL/NKT cell percentage. Further study of the predictive biomarkers of IKC treatment is needed.
Immunotherapy recently has achieved impressive outcomes for patients with NSCLC24,25. The response rate of second line immunotherapy is around 10–20%26,27. For patients with driver mutations, the response rate for later line treatment after TKI failure is ≤ 10%19,28,29. In this trial, one participant achieved a partial response, resulting in a response rate of 7% in the Per-Protocol (PP) population and 5% in the Intention-to-Treat (ITT) population. These results are similar to the results of previous studies. Moreover, additionally, 14 participants achieved stable disease or better, leading to an overall disease control rate of 100% in the PP population and 75% in the ITT population. Most of the trials for NSCLC focus on immune checkpoint inhibitors. Because the immune system is suppressed and/or insufficient among cancer patients, the goal of checkpoint inhibitor is to resume anti-cancer immunity in patients. If this goal is reached, activation of the immune system could lead to eradication of cancer cells. Lin and colleagues combined pemrolizumab with NK cells in patients with NSCLC. The results demonstrated better overall survival in patients with previously treated NSCLC30. Our study supports the notion that IKC infusion is an efficient strategy for lung cancer treatment. In addition, IKC combined with immune checkpoint inhibitors may also benefit patients with advanced NSCLC. Additional research focusing on IKC combined with immune checkpoint inhibitors is warranted.
The pain VAS scale and QOL after IKC treatments were not significantly different from the baseline levels. Wintner et al. demonstrated that later chemotherapy is associated with a worse QOL. Declines in QOL have generally been attributed to chemotherapy itself and, especially, third-line or higher treatments are responsible for QOL impairment31. Therefore, IKC should be considered for lung cancer treatment to achieve a higher QOL as compared to conventional chemotherapy.
There are some limitations in this study. First, the population of this study is small. NSCLC patients who received the IKC-based therapy are heterogeneous. Second, more trials are needed to determine the optimal manufacturing process for IKC and to establish the infusion dosage that achieves the best therapeutic outcome. Finally, the best regimen of IKC treatment is unknown. There is no trial focus on IKC monotherapy or IKC combination for patients with NSCLC. A large, prospective, randomized control trial is necessary to confirm the idea of IKC treatment for patients with NSCLC.
In conclusion, IKC treatment in patients with NSCLC was well tolerated and it may result in a longer PFS. IKC infusions should be an option for patients who have received at least two lines of chemotherapy, and further study of IKC treatment of lung cancer, either alone or in combination with other immune checkpoint inhibitors, is warranted.
Data availability
All relevant data are within the manuscript. The data underlying the findings of this study are retained at the study institutes, Taipei Veterans General Hospital and Tri-service General Hospital; and will not be made openly accessible because of ethical and privacy concerns. Professor Yuh-Min Chen should be contacted if someone wants to request the data from this study.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249. https://doi.org/10.3322/caac.21660 (2021).
Allemani, C. et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391, 1023–1075. https://doi.org/10.1016/S0140-6736(17)33326-3 (2018).
Luo, Y. H. et al. 5-year overall survival in patients with lung cancer eligible or ineligible for screening according to US Preventive Services Task Force criteria: A prospective, observational cohort study. Lancet Oncol. 20, 1098–1108. https://doi.org/10.1016/S1470-2045(19)30329-8 (2019).
Tseng, Y. H. et al. Efficacy of chemotherapy in epidermal growth factor receptor (EGFR) mutated metastatic pulmonary adenocarcinoma patients who had acquired resistance to first-line EGFR tyrosine kinase inhibitor (TKI). J. Chemother. 28, 50–58. https://doi.org/10.1179/1973947815Y.0000000027 (2016).
Chen, Y. M., Yang, W. K., Whang-Peng, J., Kuo, B. I. & Perng, R. P. Elevation of interleukin-10 levels in malignant pleural effusion. Chest 110, 433–436. https://doi.org/10.1378/chest.110.2.433 (1996).
Chen, Y. M. et al. Cross regulation by IL-10 and IL-2/IL-12 of the helper T cells and the cytolytic activity of lymphocytes from malignant effusions of lung cancer patients. Chest 112, 960–966. https://doi.org/10.1378/chest.112.4.960 (1997).
Chen, Y. M. et al. Restoration of the immunocompetence by IL-2 activation and TCR-CD3 engagement of the in vivo anergized tumor-specific CTL from lung cancer patients. J. Immunother. 20, 354–364. https://doi.org/10.1097/00002371-199709000-00004 (1997).
Liu, L. et al. Randomized study of autologous cytokine-induced killer cell immunotherapy in metastatic renal carcinoma. Clin. Cancer Res. 18, 1751–1759. https://doi.org/10.1158/1078-0432.CCR-11-2442 (2012).
Li, R. et al. Autologous cytokine-induced killer cell immunotherapy in lung cancer: A phase II clinical study. Cancer Immunol. Immunother. 61, 2125–2133. https://doi.org/10.1007/s00262-012-1260-2 (2012).
Matera, L. et al. In vivo migration of labeled autologous natural killer cells to liver metastases in patients with colon carcinoma. J. Transl. Med. 4, 49. https://doi.org/10.1186/1479-5876-4-49 (2006).
Jiang, J. T. et al. Increasing the frequency of CIK cells adoptive immunotherapy may decrease risk of death in gastric cancer patients. World J. Gastroenterol. 16, 6155–6162. https://doi.org/10.3748/wjg.v16.i48.6155 (2010).
Hervier, B., Russick, J., Cremer, I. & Vieillard, V. NK cells in the human lungs. Front. Immunol. 10, 1263. https://doi.org/10.3389/fimmu.2019.01263 (2019).
Schoenhals, J. E. et al. Uncovering the immune tumor microenvironment in non-small cell lung cancer to understand response rates to checkpoint blockade and radiation. Transl. Lung Cancer Res. 6, 148–158. https://doi.org/10.21037/tlcr.2017.03.06 (2017).
Borch, T. H. et al. Future role for adoptive T-cell therapy in checkpoint inhibitor-resistant metastatic melanoma. J. Immunother. Cancer 8, 668. https://doi.org/10.1136/jitc-2020-000668 (2020).
Fang, L. et al. Targeting late-stage non-small cell lung cancer with a combination of DNT cellular therapy and PD-1 checkpoint blockade. J. Exp. Clin. Cancer Res. 38, 123. https://doi.org/10.1186/s13046-019-1126-y (2019).
Durrieu, L. et al. Implication of different effector mechanisms by cord blood-derived and peripheral blood-derived cytokine-induced killer cells to kill precursor B acute lymphoblastic leukemia cell lines. Cytotherapy 16, 845–856. https://doi.org/10.1016/j.jcyt.2013.12.010 (2014).
Gammaitoni, L. et al. Cytokine-induced killer cells kill chemo-surviving melanoma cancer stem cells. Clin. Cancer Res. 23, 2277–2288. https://doi.org/10.1158/1078-0432.CCR-16-1524 (2017).
Wei, F. et al. Cytokine-induced killer cells efficiently kill stem-like cancer cells of nasopharyngeal carcinoma via the NKG2D-ligands recognition. Oncotarget 6, 35023–35039. https://doi.org/10.18632/oncotarget.5280 (2015).
Miller, V. A. et al. Afatinib versus placebo for patients with advanced, metastatic non-small-cell lung cancer after failure of erlotinib, gefitinib, or both, and one or two lines of chemotherapy (LUX-Lung 1): A phase 2b/3 randomised trial. Lancet Oncol. 13, 528–538. https://doi.org/10.1016/S1470-2045(12)70087-6 (2012).
Morotti, M. et al. Promises and challenges of adoptive T-cell therapies for solid tumours. Br. J. Cancer 124, 1759–1776. https://doi.org/10.1038/s41416-021-01353-6 (2021).
Weber, J. et al. White paper on adoptive cell therapy for cancer with tumor-infiltrating lymphocytes: A report of the CTEP subcommittee on adoptive cell therapy. Clin. Cancer Res. 17, 1664–1673. https://doi.org/10.1158/1078-0432.CCR-10-2272 (2011).
Dudley, M. E. et al. Adoptive cell therapy for patients with metastatic melanoma: Evaluation of intensive myeloablative chemoradiation preparative regimens. J. Clin. Oncol. 26, 5233–5239. https://doi.org/10.1200/JCO.2008.16.5449 (2008).
Saberian, C. et al. Randomized phase II trial of lymphodepletion plus adoptive cell transfer of tumor-infiltrating lymphocytes, with or without dendritic cell vaccination, in patients with metastatic melanoma. J. Immunother. Cancer 9, 449. https://doi.org/10.1136/jitc-2021-002449 (2021).
Paz-Ares, L. et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N. Engl. J. Med. 379, 2040–2051. https://doi.org/10.1056/NEJMoa1810865 (2018).
Gandhi, L. et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378, 2078–2092. https://doi.org/10.1056/NEJMoa1801005 (2018).
Chen, Y. M. Immune checkpoint inhibitors for nonsmall cell lung cancer treatment. J. Chin. Med. Assoc. 80, 7–14. https://doi.org/10.1016/j.jcma.2016.08.005 (2017).
Xu, F. et al. A TP53-associated gene signature for prediction of prognosis and therapeutic responses in lung squamous cell carcinoma. Oncoimmunology 9, 1731943. https://doi.org/10.1080/2162402X.2020.1731943 (2020).
Katakami, N. et al. LUX-Lung 4: A phase II trial of afatinib in patients with advanced non-small-cell lung cancer who progressed during prior treatment with erlotinib, gefitinib, or both. J. Clin. Oncol. 31, 3335–3341. https://doi.org/10.1200/JCO.2012.45.0981 (2013).
Schuler, M. et al. Afatinib beyond progression in patients with non-small-cell lung cancer following chemotherapy, erlotinib/gefitinib and afatinib: Phase III randomized LUX-Lung 5 trial. Ann. Oncol. 27, 417–423. https://doi.org/10.1093/annonc/mdv597 (2016).
Lin, M. et al. Pembrolizumab plus allogeneic NK cells in advanced non-small cell lung cancer patients. J. Clin. Investig. 130, 2560–2569. https://doi.org/10.1172/JCI132712 (2020).
Wintner, L. M. et al. Quality of life during chemotherapy in lung cancer patients: Results across different treatment lines. Br. J. Cancer 109, 2301–2308. https://doi.org/10.1038/bjc.2013.585 (2013).
Acknowledgements
The authors acknowledge the assistance of medical writer, Ching-Ya Huang from Formosa Biomedical Technology Corp. CRO Division in the editorial support. Ching-Ya Huang did not receive any funding or support personally; and the company, Formosa Biomedical Technology Corp. CRO Division have no influence on the production of the manuscript. The authors also thanked the contribution of The National Health Research Institutes in data analysis.
Author information
Authors and Affiliations
Contributions
YMC: Investigation, Resources, Validation, Formal analysis, Data curation, Writing—original draft, Writing—review and editing. YCC, SJC, CJW: Conceptualization, Methodology, Funding acquisition. CLH, CFC, CLC, HSC, CLT, WCP: Investigation, Resources, Validation. CFH, MHC, KHK: Formal analysis, Data curation. YHT: Formal analysis, Data curation, Writing—original draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tseng, YH., Ho, CL., Chian, CF. et al. Immune killer cells treatment for previously treated stage IV NSCLC patients. Sci Rep 14, 19374 (2024). https://doi.org/10.1038/s41598-024-69587-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-69587-x
