
Abstract
While previous observational studies have suggested a link between leukocyte counts and vascular dementia (VD), the causal relationship between leukocyte counts and various subtypes of VD remains elusive. This study aimed to investigate the causal relationship between five types of leukocyte counts and VD, with the goal of improving prevention and treatment strategies. In this study, leukocyte counts were used as the exposure variable, with genome-wide association study (GWAS) data sourced from both the UK Biobank and the Blood Cell Consortium. Additionally, GWAS data for five subtypes of vascular dementia were obtained from the FinnGen database. We conducted rigorous statistical analysis and visualization using Mendelian randomization (MR) to elucidate the potential causal relationship between leukocyte counts and vascular dementia. This study, utilizing MR analysis with data from the UK Biobank and Blood Cell Consortium, identified significant causal associations between increased lymphocyte counts and VD. Specifically, lymphocyte counts were found to be causally related to multiple and mixed VD subtypes. Sensitivity analyses, including MR-Egger regression and MR-PRESSO tests, confirmed the robustness of these findings, with no evidence of reverse causality or significant horizontal pleiotropy detected. The results underscore a potential inflammatory or immunological mechanism in the pathogenesis of VD, highlighting lymphocytes as a key component in their etiology. This investigation establishes a robust association between elevated lymphocyte and leukocyte counts and an increased risk of VD, emphasizing the roles of inflammation, immune activation, and hematological factors in disease pathogenesis.
Similar content being viewed by others


Introduction
Vascular dementia (VD) is the second most prevalent form of age-related dementia, accounting for at least 20% of dementia cases worldwide, second only to Alzheimer’s disease (AD)1,2. It encompasses a range of brain disorders linked to cognitive impairment caused by vascular lesions, including ischemic stroke, hemorrhagic stroke, cerebral ischemia, and hypoxia3,4,5. The complexity of VD is reflected in its classification into subtypes such as post-stroke dementia (PSD), subcortical ischemic vascular dementia (SIVaD), multi-infarct dementia, and mixed dementia6,7.
Recent research highlights the role of inflammation and immunity in the development and progression of vascular dementia8,9. Neuroinflammation, involving interactions between immune cells from both the innate and adaptive systems, is considered a key factor in the pathogenesis of dementia, including VD and AD10. Peripheral inflammation and immune dysfunction can exacerbate neuroinflammation, contributing to neuronal damage11.
Blood leukocytes, key indicators of inflammation and immune function, play a significant role in the development of cerebrovascular diseases. Elevated leukocyte counts have been shown to correlate with psychomotor cognitive decline in the elderly12, while specific research highlights the intricate connection between leukocyte counts and vascular dementia13,14. Observational studies from the Framingham Heart Study reveal associations between elevated neutrophil-to-lymphocyte ratios and cognitive decline, decreased brain volume, and more severe microangiopathy13. Higher neutrophil levels may induce hypoperfusion by adhering to cerebral capillaries15.
Divergent findings regarding lymphocyte counts and the risk of VD have been reported. Some studies suggest that higher lymphocyte counts may act as a protective factor, lowering the risk of dementia, while others establish a connection between elevated lymphocyte levels and an increased risk of dementia14. Additionally, regulatory T cells, a specific subset of lymphocytes known for their immunomodulatory role, are implicated in influencing cognitive performance. They may play a key role in ongoing inflammatory responses, potentially affecting the risk of dementia16. The complex interplay between lymphocyte counts and dementia risk highlights the need for further research to elucidate the underlying mechanisms and clarify the contradictory observations in the literature.
However, the aforementioned studies are merely correlational and cannot establish causality. To better understand the association between leukocyte counts and VD, it is essential to employ methodologies that explore causal relationships, providing evidence for a more comprehensive clinical understanding of the disease’s risk factors. Mendelian Randomization (MR) analysis utilizes genetic variation (single nucleotide polymorphisms) as instrumental variables instead of external interventions, allowing for an unbiased assessment of causal associations between exposures and outcomes17,18. This approach offers potential avenues for targeted interventions, enabling early disease prevention and improving the quality of life in at-risk populations. Given the substantial overlap in neuropsychiatric features between AD and VD, and the emergence of vascular risk factors as major contributors to AD, we acquired comprehensive GWAS data encompassing leukocyte and their subtype counts alongside disease outcomes in both VD and AD. We investigated the bidirectional causality between these factors using two-sample MR analysis and multivariate MR analysis.
Methods
Study design
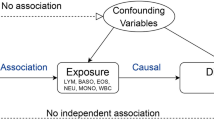
This study utilized leukocyte exposure data from two sources, along with outcome data for five subtypes of vascular dementia and Alzheimer’s disease (Fig. 1). The aim was to investigate the potential causal relationship between leukocyte counts and vascular dementia, providing insights for future disease prevention strategies. We employed the STROBE-MR (Strengthening the Reporting of Observational Studies in Epidemiology using Mendelian Randomization) guidelines to enhance the clarity of our research process. The white blood cell count data encompassed six primary categories: total white blood cells, eosinophils, basophils, monocytes, lymphocytes, and neutrophils. The vascular dementia outcomes were categorized into five groups: total, mixed, multiple infarct, subcortical, and undefined. Initially, we investigated the causal relationship between leukocytes and vascular dementia using a two-sample Mendelian Randomization method. Subsequently, we conducted a reverse validation to eliminate the influence of reverse causation and employed multivariate MR to control for confounders such as hypertension, smoking, diabetes, and C-reactive protein levels.

The flow chart about the analytical methods and how the Mendelian Randomization (MR) analysis was performed step-by-step.
Data sources
Exposure factors data: GWAS data on leukocyte counts and their four subtypes were obtained from the UK Biobank and the Blood Cell Consortium
The first leukocyte GWAS data originated from genome-wide association analyses involving 562,243 individuals of European ancestry from the UK Biobank and INTERVAL studies. The UK Biobank is a large-scale biomedical database and research resource containing de-identified genetic, lifestyle, and health information, as well as biological samples from half a million UK participants (http://www.ukbiobank.ac.uk). Additional data on white blood cell counts were sourced from the largest cross-racial meta-analysis conducted by the Blood Cell Consortium, encompassing 746,667 subjects and examining 15 hematological profiles19. Furthermore, the study incorporated adjustments for critical covariates, including gender, age, and alcohol intake, to enhance the reliability of the outcome data. The characteristics of the exposure data are outlined in Table 1.
Disease outcomes data: GWAS data for five subtypes of vascular dementia were obtained from the FinnGen database
The FinnGen study is a large-scale genomics program that has analyzed over 500,000 Finnish biobank samples, correlating genetic variants with health data to understand disease mechanisms and susceptibility20. We chose FinnGen data as the source of GWAS data for vascular dementia (F01), which is defined on the official website as a degenerative vascular disorder affecting the brain, caused by the blockage of blood supply to the brain, and manifested by a decline in memory and cognitive functions. Demographic characteristics can be found at https://r10.risteys.finregistry.fi/endpoints/F5_VASCDEM. Five subtypes coded according to ICD-10 are also included: subcortical (F01.2), mixed, multiple infarctions (F01.1), sudden onset (F01.0), and undefined (F01.9). This approach ensures that all genetic data come from individuals of European ancestry and selects data from different sources to fulfill the basic requirements of two-sample MR, thereby reducing the impact of sample overlap on the results. After adjusting for age, sex, genetic correlation, genotyping batch, and the first 10 principal components, the R10 version of this dataset included 2717 VD patients and 393,024 healthy controls. The number of SNPs ranged from 16,380,453 to 16,380,457 for each of the five VD types. Detailed information about the GWAS data for the VD diseases is presented in Table 2.
All data is accessible online through the IEU database (https://gwas.mrcieu.ac.uk/) and FinnGen database (https://www.finngen.fi/en/), and specific details regarding the concluding dataset are outlined in Table 1.
Selection of instrumental variables
The entire process of Mendelian randomization analysis revolves around three fundamental assumptions, ensuring that genetic variation can effectively serve as an instrumental variable, mimicking a natural randomized experiment for making causal inferences about exposure and outcome. The first crucial requirement is that the chosen instrumental variables must exhibit a strong correlation with the exposure factors, with a p-value of less than 5E-08 for the selected genetic variants21. Subsequently, it is imperative that these instrumental variables do not directly influence the occurrence of the outcome but instead exert their impact through the exposure factors, ensuring the robustness of the causal relationship between exposure and outcome22. To further enhance the reliability of the analysis, we carefully selected instrumental variables with chained unbalanced r2 values less than 0.001, thereby reducing correlations with other genetic variants and increasing their likelihood of effectively representing a single exposure factor. Additionally, to minimize the possibility of instrumental variables directly affecting the outcome, we verified that there was a substantial distance (> 10 MB) between the selected instrumental variables and the outcome23. We also established a minimum minor allele frequency (MAF) threshold of 0.3 for SNPs in this study. Instrumental variables with palindromic structures were excluded to maintain the integrity of the causal inference. Additionally, it was essential for the instrumental variables to remain unassociated with potential protective and risk factors for the outcome. We excluded instrumental variables (IVs) significantly associated with the outcome (p-value < 1E-5) and those where the second phenotype was directly associated with the outcome, ensuring the soundness of the analysis and adherence to the core assumptions of Mendelian randomization24. To mitigate the potential impact of weak instrumental variables on our findings, we established an F-statistic threshold greater than 10 for selecting SNPs as instrumental variables25.
Statistical analysis
The Inverse Variance Weighted (IVW) approach is the primary method for examining causal relationships, weighting the effects of individual instrumental variables to assess overall causal effects26. The weighted median and MR-Egger methods complement the IVW method and are better suited for situations involving horizontal pleiotropy in instrumental variables or when the three core assumptions are not met27. To address potential confounding introduced by the number and diversity of instrumental variables, we employed a combination of methods to enhance the robustness of our study outcomes. Cochran's Q statistic was used to assess heterogeneity among instrumental variables, ensuring no significant differences (p > 0.05) existed in the effect estimates between variables, thereby maintaining the reliability of the overall results28. The MR-Egger and MR-PRESSO methods were utilized to assess horizontal pleiotropy and identify potential outliers. MR-Egger regression computes an intercept parameter, with the absolute value reflecting the extent of bias introduced by horizontal pleiotropy29. The MR-PRESSO method involves three primary steps: outlier detection, correction of causal effects, and process reiteration30. Various visualization methods were employed to present the results, including forest plots to compare differences in study outcomes, funnel plots to assess the symmetry of instrumental variables, and scatter plots to explore relationships between variables. Leave-One-Out (LLO) analysis checks if a specific instrumental variable significantly impacts the outcome variable, enhances causal effect robustness by removing outliers, and generates LLO plots for visualizing the results31. Additionally, Phenoscanner was used to identify secondary phenotypes of instrumental variables that exhibited strong associations with exposure factors, thereby mitigating the influence of known confounding factors32.
Inverse Mendelian randomization and multivariate Mendelian randomization
To account for the potential impact of reverse causality on the study conclusions, we conducted a reverse MR analysis of the positive outcome pairs (leukocyte exposure-disease outcome). We adjusted the p-value to 1E-5 to ensure a sufficient number of SNPs, while maintaining the same setup conditions as the forward MR analysis. Additionally, we addressed the potential influence of confounding factors by including common variables affecting VD (such as hypertension, smoking status, diabetes, and C-reactive protein levels) in our multivariate MR analysis. Using both Inverse Variance Weighted (IVW) and Basic methods provided complementary insights, enhancing the robustness and reliability of our analysis.
The analytical process was conducted in R (version 4.3.1) using the “TwoSampleMR” and “MRPRESSO” packages for two-sample MR analysis and sensitivity testing.
Results
Bidirectional Mendelian randomization results
We selected GWAS data on leukocyte counts from two distinct datasets, with eligible instrumental variables (IVs) related to exposure comprising 5024 SNPs. The number of IVs per leukocyte type ranged from 193 to 500. To avoid weak instrumental variables, the mean F-statistics of our selected SNPs ranged from 90.63 to 168.45, ensuring they met the pre-assumption of F > 10. The mean R2 value consistently remained below 0.0005, minimizing potential confounding and reverse causation, and ensuring the three core assumptions in Mendelian randomization analyses were met (Tables S1, 3, 5, 7). A comprehensive description of the data sources is provided in Table 1. Ultimately, we established a causal relationship between eight leukocyte groups and the disease (Fig. 2).

The forest plot showed primary results of the causal association between leukocyte counts and vascular dementia and Alzheimer’s disease. Vascular dementia (mix): Vascular dementia (mixed), Vascular dementia (mul): Vascular dementia (multiple infarctations). OR, odds ratio; CI, confidence interval. Statistical significance: p < 0.05.
Using GWAS data for leukocyte counts from the UK Biobank, we identified significant associations between lymphocyte counts and both vascular dementia (VD) (OR = 1.198, 95% CI 1.050–1.367, P = 0.007) and multiple phenotypes (OR = 1.460, 95% CI 1.101–1.936, P = 0.009) using the IVW method. Similarly, lymphocyte counts were found to have a significant causal relationship with Alzheimer’s disease (AD), following the same trend (OR = 1.130, 95% CI 1.053–1.213, P = 0.001) (Fig. S1). Furthermore, increased leukocyte counts emerged as a risk factor for mixed VD (OR = 1.444, 95% CI 1.023–2.040, P = 0.037) (Fig. 3). Both the MR Egger and Weighted Median methods exhibited the same trends as the IVW results, further validating our findings (Tables S2, 4, 6, 8). In the subsequent reverse MR analysis, no evidence of reverse causality was found (Tables S9-12). After accounting for hypertension, smoking status, diabetes, and C-reactive protein levels, the results from basic multivariate MR still supported a causal relationship between lymphocyte counts and AD, VD, as well as its multiple infarction and mixed subtypes. However, the IVW multivariate MR only showed a significant association between lymphocyte counts and mixed VD (OR = 1.440, 95% CI 1.030–2.014, P = 0.033) (Table S13-14).

Scatter plots for the causal association between leukocyte counts and vascular dementia. Scatter plots showing the association of the SNP effects on Leukocyte Counts against the SNP effects on vascular dementia. The horizontal and vertical axes represent the effect of each genetic variation on Leukocyte Counts and vascular dementia. Each point on the scatter plot represents a SNP. The gray line around the black solid point indicates the corresponding 95% CI for the effect. The slopes of the solid lines reflects the size of the causal effect of Leukocyte Counts on vascular dementia. SNP: single nucleotide polymorphism. (a) Lymphocytes (UKB database)—vascular dementia, (b) Lymphocytes (Blood Cell Consortium)—vascular dementia, (c) Lymphocytes (UKB database)—vascular dementia (mixed), (d) White blood cell counts (UKB database)—vascular dementia (mixed), (e) Lymphocytes (UKB database)—vascular dementia (multiple infarctations), (f) Lymphocytes (Blood Cell Consortium)—vascular dementia (multiple infarctations).
Similar results were observed in the Blood Cell Consortium data (Tables S2, 4, 6, 8). The primary results indicated a significant causal relationship between lymphocyte counts and VD (OR = 1.156, 95% CI 1.010–1.323, P = 0.035), including its mixed (OR = 1.433, 95% CI 1.022–2.008, P = 0.037) and multiple infarctions subtypes (OR = 1.505, 95% CI 1.126–2.011, P = 0.006). Elevated lymphocyte counts also increased the risk of AD (OR = 1.100, 95% CI 1.022–1.185, P = 0.011). Additionally, the MR Egger method suggested a potential causal relationship between lymphocytes and the multiple infarctions subtype of VD (OR = 1.841, 95% CI 1.016–3.336, P = 0.045). No evidence of reverse causality was found, further underscoring the reliability of our findings (Table S9-12). After adjusting for four conventional factors, basic multivariate MR continued to support a causal association between lymphocytes and AD, VD, and their mixed subtypes. The IVW multivariate MR results confirmed a significant association between lymphocytes and AD (OR = 1.106, 95% CI 1.014–1.208, P = 0.023) (Tables S13-S14).
Sensitivity analysis
Out of the eight positive findings, Cochran’s Q test identified heterogeneity (p < 0.05) in two results, possibly due to the small sample size of disease outcomes, while the remaining six results showed no significant differences. To ensure the scientific validity of the results, we primarily analyzed these two outcomes using the random effects model of the IVW method. To address horizontal pleiotropy, which can introduce confounding and reverse causality, we employed a combination of MR-Egger regression and MR-PRESSO outlier tests to detect and eliminate the presence of outliers (Table 3). Notably, after excluding the outliers (rs748113, rs13199519, rs36084354, rs67516712, rs7976110, rs36084354, and rs36030790), no substantial horizontal pleiotropy was detected. In our LLO analyses, we did not identify any additional outliers, and the funnel plots displayed a predominantly symmetrical pattern (Fig. 4 and S2). The use of multiple conditioning methods further assured the sensitivity and robustness of our results.

Funnel plots for the causal association between leukocyte counts and vascular dementia. The funnel plots assess the presence of bias and the robustness of the findings. They are used to determine whether the associations observed are noticeably heterogeneous. A symmetrical funnel plot suggests that there is no publication bias. Asymmetry might indicate bias. Vertical Line represents no effect. Points evenly distributed around this line and within the funnel shape boundaries suggest that the reported effects are consistent and unbiased. (a) Lymphocytes (UKB database)—vascular dementia, (b) Lymphocytes (Blood Cell Consortium)—vascular dementia, (c) Lymphocytes (UKB database)—vascular dementia (mixed), (d) White blood cell counts (UKB database)—vascular dementia (mixed), (e) Lymphocytes (UKB database)—vascular dementia (multiple infarctations), (f) Lymphocytes (Blood Cell Consortium)—vascular dementia (multiple infarctations).
Discussion
This study comprehensively investigated the potential causal relationship between leukocyte counts and different subtypes of VD using Two-Sample MR analysis and multivariate MR. The findings suggest that elevated lymphocyte counts are associated with increased risks of VD, including its multi-infarct and mixed subtypes, while a higher overall white blood cell count correlates with a heightened risk of mixed vascular dementia. The genetic results were generated using individual-level data from the UK Biobank (562,243 participants), the Blood Cell Consortium (746,667 individuals), and the FinnGen database (395,741 individuals). Our study indicates that increased levels of lymphocytes and white blood cells may play a critical role in the pathogenic mechanisms of VD.
The association between white blood cell counts and vascular dementia, particularly in the mixed subtype, was initially highlighted in earlier studies that underscored the correlation between systemic inflammation and the onset of neurodegenerative disorders. A seminal work by Moti Haim et al. in 2004, through a prospective cohort study, revealed that elevated white blood cell count was linked to a higher risk of VD, particularly among individuals with cardiovascular diseases33. Building upon this pioneering study, numerous investigations across diverse cohorts worldwide have further explored this association. In a comprehensive follow-up study within the Framingham Heart Study cohort34, individuals aged 60 and above with white blood cell counts in the highest quartile exhibited a significantly elevated risk of developing VD. This finding was further corroborated by the Rotterdam Study35,36,37, which included participants aged 55 and older, showing a notable increase in the incidence of vascular dementia among those with elevated white blood cell counts. Our current investigation, building upon this existing body of literature, utilized two large-scale datasets from the UK Biobank (562,243 participants) and the Blood Cell Consortium (746,667 individuals). We observed a consistent pattern, with elevated white blood cell counts significantly associated with an increased risk of VD, particularly in the mixed subtype. The robustness of our findings is underscored by the alignment of results across different datasets, providing further support for the notion that increased white blood cell counts are linked to VD.
The mechanisms underlying vascular dementia involve a complex interplay between chronic inflammation, microvascular dysfunction, immune activation, blood–brain barrier (BBB) disruption, hematological factors, and leukocyte-endothelial dysfunction38,39. These interconnected processes contribute to the pathogenesis and progression of VD, with implications for subtype-specific manifestations. In a state of chronic inflammation, inflammatory mediators like C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6) activate endothelial cells40,41. This activation prompts the expression of adhesion molecules such as intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1), facilitating the adhesion of circulating white blood cells to the vascular wall42,43,44. Subsequently, leukocytes migrate through the endothelial layer, guided by chemotactic factors like interleukin-8 (IL-8), ultimately penetrating the vessel wall tissue45. The interaction of leukocytes with endothelial cells induces endothelial dysfunction, leading to impaired regulatory functions46. Activated endothelial cells may release reduced amounts of nitric oxide (NO), contributing to oxidative stress and affecting vascular dilation and blood flow47. Additionally, this activation and dysfunction can increase vascular permeability, allowing easier penetration of white blood cells and inflammatory mediators into the surrounding tissues48. Chronic inflammation and vascular damage can lead to vascular narrowing, abnormal platelet activation, thrombus formation, and disturbances in the coagulation system, contributing to insufficient blood supply to the brain and resulting in ischemic injury49,50,51. Immune cell-mediated inflammation also promotes atherosclerosis and plaque formation, inducing arterial stiffness and narrowing that impede normal blood flow to the brain52,53. These interconnected mechanisms collectively contribute to the development of VD.
Lymphocyte counts demonstrated significant associations with vascular dementia, particularly in the context of multiple infarctions and mixed vascular dementia. These findings align with the evolving understanding of the role lymphocytes play in the inflammatory response and their potential involvement in the vascular pathology associated with dementia54,55,56. Studies in the population-based MINDSET cohort further supported this association, demonstrating a heightened risk of vascular dementia in individuals with elevated lymphocyte counts within the normal range38. Our present study, conducted on a diverse and sizable dataset, reinforces these observations by revealing a consistent and notable association between lymphocyte counts and VD, particularly in cases involving multiple infarctions. Multiple infarct vascular dementia is mainly caused by atherosclerosis, arterial stenosis, and the continuous shedding of atherosclerotic plaques, leading to recurrent cerebral infarctions and cognitive impairment57. Research has shown that different lymphocyte subsets, especially T cells, play a significant role in modulating the immune response during the development and progression of atherosclerosis58. All T cell subsets (CD4 + , CD8 + , NK, and follicular helper T cells) have been identified in atherosclerotic plaques in humans59. Furthermore, T lymphocytes can promote the progression of inflammation in different stages of atherosclerosis by influencing risk factors such as hyperlipidemia60. Lymphocytes might trigger cerebral tissue ischemia and hypoxia, exacerbating brain cell damage and necrosis, leading to cognitive impairment. Recognizing lymphocytes as key players in the inflammatory and immune response provides a valuable framework for understanding the underlying mechanisms contributing to the vascular pathology associated with dementia.
This study also identified a significant association between lymphocytes and Alzheimer’s disease (AD), supporting the hypothesis that the peripheral adaptive immune response mediated by lymphocytes plays a critical role in the pathogenesis of AD. Lymphocyte infiltration results in increased microglial activation, neuroinflammation, and neurodegeneration61. Helena C. Brigas and colleagues reported an accumulation of interleukin-17 (IL-17)-producing lymphocytes, which appears to precede both BBB disruption and the onset of amyloid-beta or tau pathology, suggesting an early involvement of lymphocytes and IL-17 in AD pathology62. BBB dysfunction in AD is recognized as a facilitating factor for T cell infiltration, and the degree of neuronal loss in AD correlates with the density of T cells. Specifically, in areas exhibiting tau pathology—both in tauopathy-afflicted mice and human AD brains—a marked increase in lymphocytes, particularly T cells, has been observed63,64. This relationship implies that peripheral immune cell infiltration and their interactions with resident brain cells are instrumental in AD pathogenesis. Our findings indicate an overlap in neuropathological molecular mechanisms between VD and AD, suggesting that cerebrovascular dysfunction is implicated not only in vascular causes of cognitive impairment but also in AD. These insights could pave the way for further research into disease mechanisms and the development of immune-related biomarkers or therapeutic strategies. Luo et al. have also explored the correlation between leukocyte counts and AD. Consistent with our research, their study suggests that genetically lower counts of blood monocytes were associated with a modestly increased risk of AD65. It has been observed that patrolling monocytes in the blood target and eliminate amyloid-beta (Aβ) by migrating into the walls of Aβ-positive veins. Selective removal of these monocytes leads to an accumulation of Aβ in the brain66. Furthermore, monocytes migrate into the brain where they differentiate into microglia-like, bone marrow-derived macrophages, which clear Aβ more effectively than resident microglial cells67. Monocyte activation promotes the clearance of amyloid proteins in the blood, thereby reducing the accumulation of Aβ in the brain and potentially exerting a neuroprotective effect68. Further research is required to fully elucidate the relationship between leukocyte counts, their subtypes, and AD. Given the current discrepancies in findings, further investigation is warranted to elucidate the relationship between AD and leukocytes, including their subtypes, as well as the associated inflammatory and immunological pathomechanisms.
We outline below some of the notable advantages of this study: The choice of instrumental variables (IVs) is a critical aspect of MR69. his study meticulously selected IVs based on stringent criteria, including strong correlation with exposure factors, minimal influence on the outcome, and independence from potential confounding factors. The exclusion of weak instrumental variables, palindromic structures, and those associated with protective and risk factors for the outcome adds rigor to the analysis. Careful consideration of factors such as allele frequency, distance from the outcome, and the use of an F-statistic threshold further enhances the reliability of the instrumental variable selection process. The statistical analysis employed a combination of methods to address potential challenges, such as horizontal pleiotropy and heterogeneity among instrumental variables. The use of Cochran's Q statistic to assess heterogeneity, MR-Egger regression to detect and quantify horizontal pleiotropy, and MR-PRESSO outlier tests to identify and correct for potential outliers contribute to the robustness of the study outcomes. Visualization methods, including forest plots, funnel plots, and scatter plots, provide a comprehensive presentation of the results.
However, several considerations and limitations should be noted. The study focused on individuals of European ancestry, which may limit the generalizability of the findings to other populations. The use of GWAS data means that the observed associations are based on genetic variation, so caution is needed when extrapolating these findings to interventions or treatments. Additionally, despite the meticulous selection of instrumental variables and adjustment for key covariates, the potential impact of unmeasured confounding factors cannot be entirely ruled out.
Conclusions
This study confirms the causal relationship between elevated white blood cell counts, particularly lymphocytes, and an increased risk of VD using MR. Specific emphasis was placed on two subtypes of dementia: mixed dementia and multi-infarct dementia. The findings highlight potential mechanisms in the pathogenesis of vascular dementia involving inflammation, immune activation, and hematologic factors. The results of multivariate MR and inverse MR further strengthen the evidence for a causal relationship. Our study provides a solid foundation for future research, emphasizing the importance of subtype-specific exploration and rigorous research methods to understand and address the complexities of VD.
Data availability
All statistical results were available in supplementary tables. The datasets analyzed during the current study are available in the IEU database[https://gwas.mrcieu.ac.uk/] and specific details regarding the concluding dataset are outlined in Table 1. The exposure datasets generated during the current study are available in the UK Biobank and Blood Cell Alliance repository. [https://www.ukbiobank.ac.uk/] and [http://abc.sklehabc.com/]. The outcome datasets generated during the current study are available in the Finngen database [https://r10.finngen.fi/].
References
Iadecola, C. et al. Vascular cognitive impairment and dementia: JACC scientific expert panel. J. Am. Coll. Cardiol. 73, 3326–3344 (2019).
Wolters, F. J. & Ikram, M. A. Epidemiology of vascular dementia. Arterioscler Thromb. Vasc. Biol. 39, 1542–1549 (2019).
Iadecola, C. The pathobiology of vascular dementia. Neuron 80, 844–866 (2013).
Inoue, Y., Shue, F., Bu, G. & Kanekiyo, T. Pathophysiology and probable etiology of cerebral small vessel disease in vascular dementia and Alzheimer’s disease. Mol. Neurodegener 18, 46 (2023).
Yang, Y., Zhao, X., Zhu, Z. & Zhang, L. Vascular dementia: A microglia’s perspective. Ageing Res. Rev. 81, 101734 (2022).
Prajjwal, P. et al. Vascular dementia subtypes, pathophysiology, genetics, neuroimaging, biomarkers, and treatment updates along with its association with Alzheimer’s dementia and diabetes mellitus. Dis. Mon. 69, 101557 (2023).
Skrobot, O. A. et al. Progress toward standardized diagnosis of vascular cognitive impairment: Guidelines from the vascular impairment of cognition classification consensus study. Alzheimers Dement. 14, 280–292 (2018).
Rajeev, V. et al. Pathophysiology of blood brain barrier dysfunction during chronic cerebral hypoperfusion in vascular cognitive impairment. Theranostics 12, 1639–1658 (2022).
Zhang, Y.-R. et al. Peripheral immunity is associated with the risk of incident dementia. Mol. Psychiatry 27, 1956–1962 (2022).
van der Willik, K. D. et al. Balance between innate versus adaptive immune system and the risk of dementia: A population-based cohort study. J. Neuroinflamm. 16, 68 (2019).
Prinz, M. & Priller, J. The role of peripheral immune cells in the CNS in steady state and disease. Nat. Neurosci. 20, 136–144 (2017).
Kao, T.-W. et al. White blood cell count and psychomotor cognitive performance in the elderly. Eur. J. Clin. Investig. 41, 513–520 (2011).
Fang, Y. et al. Cross-sectional association between blood cell phenotypes, cognitive function, and brain imaging measures in the community-based framingham heart study. J. Alzheimers Dis. 87, 1291–1305 (2022).
Lombardi, G. et al. Leukocyte-derived ratios are associated with late-life any type dementia: A cross-sectional analysis of the Mugello study. Geroscience 43, 2785–2793 (2021).
Cruz Hernández, J. C. et al. Neutrophil adhesion in brain capillaries reduces cortical blood flow and impairs memory function in Alzheimer’s disease mouse models. Nat. Neurosci. 22, 413–420 (2019).
Fohner, A. E. et al. Association of peripheral lymphocyte subsets with cognitive decline and dementia: The cardiovascular health study. J. Alzheimers Dis. 88, 7–15 (2022).
O’Donnell, C. J. & Sabatine, M. S. Opportunities and challenges in mendelian randomization studies to guide trial design. JAMA Cardiol. 3, 967 (2018).
Davies, N. M., Holmes, M. V. & Davey Smith, G. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 362, k601 (2018).
Chen, M.-H. et al. Trans-ethnic and ancestry-specific blood-cell genetics in 746,667 individuals from 5 global populations. Cell 182, 1198-1213.e14 (2020).
Kurki, M. I. et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature 613, 508–518 (2023).
Burgess, S., Small, D. S. & Thompson, S. G. A review of instrumental variable estimators for Mendelian randomization. Stat. Methods Med. Res. 26, 2333–2355 (2017).
Sekula, P., Fabiola Del Greco, M., Pattaro, C. & Köttgen, A. Mendelian randomization as an approach to assess causality using observational data. J. Am. Soc. Nephrol. 27, 3253–3265 (2016).
Brion, M.-J.A., Shakhbazov, K. & Visscher, P. M. Calculating statistical power in Mendelian randomization studies. Int. J. Epidemiol. 42, 1497–1501 (2013).
Bowden, J. & Holmes, M. V. Meta-analysis and Mendelian randomization: A review. Res. Synth. Methods 10, 486–496 (2019).
Burgess, S., Thompson, S. G., CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int. J. Epidemiol. 40, 755–764 (2011).
Larsson, S. C., Burgess, S. & Michaëlsson, K. Association of genetic variants related to serum calcium levels with coronary artery disease and myocardial infarction. JAMA 318, 371–380 (2017).
Bowden, J., Davey Smith, G., Haycock, P. C. & Burgess, S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet. Epidemiol. 40, 304–314 (2016).
Hoaglin, D. C. Misunderstandings about Q and ‘Cochran’s Q test’ in meta-analysis. Stat. Med. 35, 485–495 (2016).
Bowden, J., Davey Smith, G. & Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 44, 512–525 (2015).
Verbanck, M., Chen, C.-Y., Neale, B. & Do, R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat. Genet. 50, 693–698 (2018).
Cheng, H., Garrick, D. J. & Fernando, R. L. Efficient strategies for leave-one-out cross validation for genomic best linear unbiased prediction. J. Anim. Sci. Biotechnol. 8, 38 (2017).
Staley, J. R. et al. PhenoScanner: A database of human genotype-phenotype associations. Bioinformatics 32, 3207–3209 (2016).
Haim, M., Boyko, V., Goldbourt, U., Battler, A. & Behar, S. Predictive value of elevated white blood cell count in patients with preexisting coronary heart disease: The Bezafibrate Infarction Prevention Study. Arch. Intern. Med. 164, 433–439 (2004).
Hu, Z.-B. et al. Higher total white blood cell and neutrophil counts are associated with an increased risk of fatal stroke occurrence: The Guangzhou biobank cohort study. BMC Neurol. 21, 470 (2021).
de Jong, F. J. et al. Retinal vascular caliber and risk of dementia: The Rotterdam study. Neurology 76, 816–821 (2011).
Vlasov, V. et al. Subclinical vascular disease and the risk of parkinsonism: The Rotterdam study. Parkinsonism Relat. Disord. 43, 27–32 (2017).
Fani, L. et al. Thyroid status and brain circulation: The Rotterdam study. J. Clin. Endocrinol. Metab. 107, e1293–e1302 (2022).
Lecordier, S., Manrique-Castano, D., El Moghrabi, Y. & ElAli, A. Neurovascular alterations in vascular dementia: Emphasis on risk factors. Front Aging Neurosci. 13, 727590 (2021).
Shabir, O., Berwick, J. & Francis, S. E. Neurovascular dysfunction in vascular dementia, Alzheimer’s and atherosclerosis. BMC Neurosci. 19, 62 (2018).
Wen, Y. et al. Chronic inflammation, cancer development and immunotherapy. Front Pharmacol. 13, 1040163 (2022).
Kaneko, N., Kurata, M., Yamamoto, T., Morikawa, S. & Masumoto, J. The role of interleukin-1 in general pathology. Inflamm. Regen. 39, 12 (2019).
Müller, N. The role of intercellular adhesion molecule-1 in the pathogenesis of psychiatric disorders. Front Pharmacol. 10, 1251 (2019).
Pickett, J. R., Wu, Y., Zacchi, L. F. & Ta, H. T. Targeting endothelial vascular cell adhesion molecule-1 in atherosclerosis: Drug discovery and development of vascular cell adhesion molecule-1-directed novel therapeutics. Cardiovasc. Res. 119, 2278–2293 (2023).
Marinović Kulišić, S., Takahashi, M., Himelreich Perić, M., Mužić Radović, V. & Jurakić Tončić, R. Immunohistochemical analysis of adhesion molecules E-selectin, intercellular adhesion molecule-1, and vascular cell adhesion molecule-1 in inflammatory lesions of atopic dermatitis. Life (Basel) 13, 933 (2023).
Schwartz, A. B. et al. Elucidating the biomechanics of leukocyte transendothelial migration by quantitative imaging. Front Cell Dev. Biol. 9, 635263 (2021).
Sun, H.-J., Wu, Z.-Y., Nie, X.-W. & Bian, J.-S. Role of endothelial dysfunction in cardiovascular diseases: The link between inflammation and hydrogen sulfide. Front Pharmacol. 10, 1568 (2019).
Shu, X. et al. Endothelial nitric oxide synthase in the microcirculation. Cell Mol. Life Sci. 72, 4561–4575 (2015).
Botts, S. R., Fish, J. E. & Howe, K. L. Dysfunctional vascular endothelium as a driver of atherosclerosis: Emerging insights into pathogenesis and treatment. Front Pharmacol. 12, 787541 (2021).
Levi, M., Keller, T. T., van Gorp, E. & ten Cate, H. Infection and inflammation and the coagulation system. Cardiovasc. Res. 60, 26–39 (2003).
Malekmohammad, K., Bezsonov, E. E. & Rafieian-Kopaei, M. Role of lipid accumulation and inflammation in atherosclerosis: Focus on molecular and cellular mechanisms. Front Cardiovasc. Med. 8, 707529 (2021).
Chen, Y. et al. Role of inflammation in vascular disease-related perivascular adipose tissue dysfunction. Front Endocrinol. (Lausanne) 12, 710842 (2021).
Chen, Y., Zhong, H., Zhao, Y., Luo, X. & Gao, W. Role of platelet biomarkers in inflammatory response. Biomark. Res. 8, 28 (2020).
Margraf, A. & Zarbock, A. Platelets in inflammation and resolution. J. Immunol. 203, 2357–2367 (2019).
Koyasu, S. & Moro, K. Role of innate lymphocytes in infection and inflammation. Front. Immunol. 3, 101 (2012).
Alsbrook, D. L. et al. Neuroinflammation in acute ischemic and hemorrhagic stroke. Curr. Neurol. Neurosci. Rep. 23, 407–431 (2023).
DeMaio, A., Mehrotra, S., Sambamurti, K. & Husain, S. The role of the adaptive immune system and T cell dysfunction in neurodegenerative diseases. J. Neuroinflamm. 19, 251 (2022).
Li, C., Wang, Y., Yan, X.-L., Guo, Z.-N. & Yang, Y. Pathological changes in neurovascular units: Lessons from cases of vascular dementia. CNS Neurosci. Ther. 27, 17–25 (2021).
Saigusa, R., Winkels, H. & Ley, K. T cell subsets and functions in atherosclerosis. Nat. Rev. Cardiol. 17, 387–401 (2020).
Abdolmaleki, F., Gheibi Hayat, S. M., Bianconi, V., Johnston, T. P. & Sahebkar, A. Atherosclerosis and immunity: A perspective. Trends Cardiovasc. Med. 29, 363–371 (2019).
Wang, Y. et al. Interleukin-17-producing CD4+ T cells promote inflammatory response and foster disease progression in hyperlipidemic patients and atherosclerotic mice. Front Cardiovasc. Med. 8, 667768 (2021).
Jorfi, M. et al. Infiltrating CD8+ T cells exacerbate Alzheimer’s disease pathology in a 3D human neuroimmune axis model. Nat. Neurosci. 26, 1489–1504 (2023).
Brigas, H. C. et al. IL-17 triggers the onset of cognitive and synaptic deficits in early stages of Alzheimer’s disease. Cell Rep. 36, 109574 (2021).
Zeng, J. et al. T cell infiltration mediates neurodegeneration and cognitive decline in Alzheimer’s disease. Neurobiol. Dis. 193, 106461 (2024).
Chen, X. et al. Microglia-mediated T cell infiltration drives neurodegeneration in tauopathy. Nature 615, 668–677 (2023).
Luo, J., Thomassen, J. Q., Nordestgaard, B. G., Tybjærg-Hansen, A. & Frikke-Schmidt, R. Blood leukocyte counts in Alzheimer disease. JAMA Netw. Open 5, e2235648 (2022).
Michaud, J.-P., Bellavance, M.-A., Préfontaine, P. & Rivest, S. Real-time in vivo imaging reveals the ability of monocytes to clear vascular amyloid beta. Cell Rep. 5, 646–653 (2013).
Simard, A. R., Soulet, D., Gowing, G., Julien, J.-P. & Rivest, S. Bone marrow-derived microglia play a critical role in restricting senile plaque formation in Alzheimer’s disease. Neuron 49, 489–502 (2006).
Thome, A. D. et al. Functional alterations of myeloid cells during the course of Alzheimer’s disease. Mol. Neurodegener 13, 61 (2018).
Sekula, P., Fabiola Del Greco, M., Pattaro, C. & Köttgen, A. Mendelian randomization as an approach to assess causality using observational data. J. Am. Soc. Nephrol. JASN 27, 3253–3265 (2016).
Acknowledgements
We would like to express our gratitude to the participants and investigators of the FinnGen study. Thanks also to the UK Biobank and Blood Cell Alliance for publishing the leukocyte GWAS data.
Funding
This work is, in part, supported by the Grants from the National Natural Science Foundation of China (82001873 and 82027804).
Author information
Authors and Affiliations
Contributions
SFL and CWZ conceived and designed the study, CWZ, and YKZ and SFL contributed to obtaining the data and analysis. CWZ and YKZ provided support in the visualization of results. SFL and CWZ drafted the manuscript. SJL, ZFW, PW, SYT, MZ, LML, RNW, LL, HZL, JFZ, and XLM critically revised this article. All authors gave final approval for the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, S., Zhang, C., Zhang, Y. et al. Causal association between blood leukocyte counts and vascular dementia: a two-sample bidirectional Mendelian randomization study. Sci Rep 14, 19582 (2024). https://doi.org/10.1038/s41598-024-70446-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-70446-y
