
Abstract
The aim of this study was to investigate the measurement of the incident angle of the main blood vessel, and the benefits of its integral with ultrasound malignant features of breast nodules for the assessment of breast malignancy based on BI-RADS. The incident angles of main blood vessels of 185 breast nodules in 185 patients who underwent breast nodule surgical excision or biopsy were quantitatively measured using color Doppler ultrasound from October 2022 to October 2023 in a tertiary hospital, and related data were collected and analyzed. Based on histopathology as the gold standard, the breast nodules were classified into benign and malignant groups. The incident angle values of both groups were compared, Receiver Operating Characteristic (ROC) curves were plotted, and the optimal cutoff value for distinguishing between benign and malignant breast nodules was determined. The malignancy risk of the breast nodules was assessed using the incident angle of the breast main vessel, BI-RADS classification, and a combination of ultrasound malignant features with the incident angle. The areas under the ROC curves (AUC) for each method were calculated and compared. The average incident angle of the main vessel of the breast nodule for the benign and malignant breast nodule groups was (41.47 ± 14.27)° and (22.65 ± 11.09)°, respectively, with a statistically significant difference (t = 10.027, P < 0.001). There was a significant negative correlation between the breast nodule vessel incident angle and histopathological malignancy (r = – 0.593, P < 0.001). The ROC curve and Youden index suggested that the optimal cutoff value for distinguishing between benign and malignant breast nodules using the vascular incident angle was 26.9°, with a sensitivity of 76.34%, specificity of 84.78%, positive predictive value of 83.53%, negative predictive value of 78.00%, and AUC of 0.853. The diagnostic performance of BI-RADS classification based on ultrasound malignant features of the breast nodules alone in assessing the malignancy risk of breast nodules showed a sensitivity of 78.50%, specificity of 92.39%, positive predictive value of 91.25%, negative predictive value of 79.95%, and AUC of 0.905. The integral of ultrasound malignant features and vascular incident angle for BI-RADS based assessment for breast nodule malignancy risk demonstrated a sensitivity of 90.32%, specificity of 89.13%, positive predictive value of 89.36%, negative predictive value of 90.11%, and AUC of 0.940. The differences in negative predictive value and AUC between ultrasound malignant features BI-RADS classification alone and the combination of ultrasound malignant features BI-RADS classification with the incident angle of the main vessel of the breast nodule were all statistically significant (x2 = 3.243, P = 0.042; Z = 2.955, P = 0.003). Measuring the incident angle of the main blood vessel of breast nodules and combining this measurement with ultrasound malignant features for BI-RADS classification can enhance the effectiveness of malignancy risk assessment of breast nodules, increase the negative predictive value, and potentially reduce unnecessary biopsies.
Similar content being viewed by others

Introduction
Breast cancer is the most common cancer among women globally and the leading cause of cancer related death in women, with a prevalence accounting for 11.6% of all cancers in 20221. Currently, there are no effective measures to prevent the occurrence of breast cancer, but early detection and effective treatment through screening can reduce the mortality rate of breast cancer2,3,4. Mammography and color Doppler ultrasonography are important screening methods, with the latter being radiation-free, without contraindications, and cost-effective, widely used in recent decades5,6,7,8. The Breast Imaging Reporting and Data System (BI-RADS) established by the American College of Radiology (ACR) has been widely used worldwide for the assessment of malignancy risk of breast nodules and is known for its high accuracy, sensitivity, and specificity6,8,9,10. The 5th edition of BI-RADS released in 2013 includes contrast-enhanced magnetic resonance imaging (MRI) assessment categories and lexicons for interpreting the vascular distribution and blood perfusion of solid breast nodules or breast cancer. However, the description of the vascular distribution of breast nodules in its ultrasound assessment categories and lexicons is relatively simple, limited to the absence of vascularity, internal vascularity, and vessels in the rim of the breast nodule, lacking detailed characterization. Vascularity is important for tumor growth and its characteristics are associated much with the tumor biological behavior11,12. Therefore, further study of the vascularity characteristics of breast nodules are meaningful for the malignancy evaluation of the breast nodules. Color Doppler Flow Imaging (CDFI) and Power Doppler Imaging (PDI) can detect the vascular distribution in the breast solid nodules13,14. The size, shape, density, and distribution of blood vessels inside and around benign and malignant breast nodules are different11,12,13,14. The main blood vessels (arteries) feeding malignant solid breast nodules may change direction or become tortuous upon entering the nodule due to the tumor’s vertical growth, infiltration of surrounding tissues, and the resulting traction effect and high stromal stiffness. In contrast, the main blood vessels (arteries) of benign solid nodules generally do not experience external traction or internal compression, leading to a more natural vessel course15,16,17,19,20. Based on these, we hypothesize that displaying the main blood vessels and branches of breast nodules using CDFI or PDI and analyzing the characteristics of the main vessel course could provide more information for the color Doppler ultrasound diagnosis of breast cancer. The aim of the present study was to measure the incident angle of the main blood vessels in breast nodules using color Doppler ultrasound and to compare the diagnostic performance of ultrasound malignant features of the breast nodules based BI-RADS classification with the combination of the incident angle of the main blood vessels and ultrasound malignant features of the breast nodules based BI-RADS classification, determining the value of the main blood vessel incident angle in assessing the malignancy risk of breast nodules.
Materials and methods
Study population
A prospective study was conducted, and 21,398 patients who underwent ultrasound examinations at the First Affiliated Hospital of Hainan Medical University from October 2022 to October 2023 were included. Inclusion criteria: (1) Patients underwent ultrasound examination of the breast, with breast nodules classified as BI-RADS 3-5; (2) The main blood vessels of the breast nodules were detected by CDFI or PDI; (3) Patients underwent surgery or biopsy with definitive histopathological results; (4) Age ≥ 18 years. Exclusion criteria: (1) The blood vessels detected by CDFI and PDI did not meet the characteristics of the main vessel of the breast nodule; (2) Patients with breast nodules who had a history of radiation therapy, chemotherapy, or other drug treatments. A total of 185 patients (185 nodules) were finally included, all female, aged between 18 and 74 years (mean age 43.65 ± 12.91 years). The maximum length of the breast nodules ranged from 7.3 to 47.8 mm(mean 21.52 ± 9.2mm). There were 185 main blood vessels (arteries) in the breast nodules. Based on the gold standard of histopathological results, the breast nodules were assigned to benign and malignant groups.
Ethical approval
This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Hainan Medical University [Approval No. 2022 (Scientific Research L) No. 177], and the study was conducted in accordance with the Declaration of Helsinki (Version 2013). Written informed consent was obtained from all patients.
Measurement of the main artery incident angle in breast nodules
Color Doppler ultrasound diagnostic systems of GE Logiq E9, Mindray Resona7, and Philips Epiq5 were used for the study, with linear array high-frequency transducers, and the operating frequencies ranged from 9 to 15 MHz. Clinical data such as age, height, weight, family history of breast cancer, palpability or pain of the breast nodule, nipple discharge, skin edema of the breast, and enlarged axillary lymph nodes were recorded. The breast screening was performed by six physicians specialized in breast ultrasound with experience of more than 4 years, and the incident angle of the main artery in the breast nodule was measured by one designated physician (Kailiang Chen). During the ultrasound examination, patients were positioned supine with arms raised to fully expose the breast. Using the high-frequency ultrasound probe, the breast was scanned radially from the nipple towards the outer edge in each quadrant to locate the nodule. The maximum diameter, position, shape, margin, internal echogenicity, posterior acoustic features, presence of microcalcifications, and edema (peripheral high echoic halo) of the nodule were determined through longitudinal, transverse, and oblique multi-sectional scanning. Subsequently, CDFI and/or PDI modes were activated. The sampling frame was adjusted to an appropriate size to fully display blood vessels within and around the nodule, and color gain and pulse repetition frequency were adjusted to adequately display blood flow signals within the vessels. Vascular density distribution in the breast nodules was classified into four categories: no vascularity (no blood flow signal), a few vascularity, (1–2 blood flow signals shown on the optimal section), moderate vascularity (3–4 blood flow signals shown on the optimal section), and abundant vascularity (more than 5 blood flow signals shown on the optimal section). When multiple vessels were visible within the breast nodule on CDFI or PDI, the vessel with the largest diameter and longest length was selected for Doppler spectral analysis using pulsed wave Doppler (PW), and the one presenting an arterial spectrum was defined as the main artery of the breast nodule. Referring to Kujiraoka et al.21, the incident angle of the main artery in the breast nodule was determined. This involved drawing two lines at the point where the vessel entered the nodule: a tangent line and its perpendicular line, with the angle between the perpendicular line and the main artery being measured (Fig. 1). Representative images were stored on the Picture Archiving and Communication System (PACS). Before the regular measurement of the incident angle of the main artery in the breast nodule, twenty patients with breast nodules were randomly selected, and the incident angle was measured three times for each breast nodule for consistency assessment. The incident angle of the main artery in the breast nodule was measured using the built-in software of the ultrasound system, with each angle measured three times and the average taken. The angle range was 0–90°.

(A) Schematic diagram of the measurement of the incident angle of the main blood vessels of the breast nodules. The A line represents the tangent line of the penetration point of the main blood vessel, the B line represents the vertical line of the tangent line, the dashed line represents the direction of the main blood vessel, and the angle between the B line and the dashed line is the incident angle (28.5°). (B) Breast nodules with the main blood vessel and vascular branches corresponding to the (A).
Ultrasound BI-RADS based malignancy risk stratification of the breast nodules
According to the ACR 2013 version of ultrasound BI-RADS9, the lexicon for suspicious malignant features of breast nodules included: irregular shape, non-parallel orientation, ambiguous/lobulated/spiculated margin, microcalcifications, posterior acoustic shadowing, and edema (peripheral high echoic halo of the nodule). Based on the lexicon, breast nodules were classified into the following categories: category 3 (no suspicious malignant feature); category 4a (one malignant feature); category 4b (two malignant features); category 4c (three malignant features); and category 5 (four malignant features and/or distant metastasis). The above six features were analyzed by two ultrasound physicians with over 12 years of experience. In cases where opinions differed, a consensus was reached through discussion between the two physicians. In conjunction with the above features, a certain incident angle of the main artery in the breast nodule obtained in this study was used as an additional malignant feature for the categorization of the malignancy risk of the breast nodules.
Statistical analysis
The statistical analysis was conducted using SPSS 26.00 and Medcalc 15.8.7 software. Quantitative data following a normal distribution were expressed as mean ± standard deviation (M ± SD) and compared using an independent samples t-test. For quantitative data not following a normal distribution, they were expressed as interquartile range (IQR, median) and compared using the Mann–Whitney U test. Count data were expressed as a number (percentage) and compared using the chi-square test with or without continuity correction. The intraclass correlation coefficient (ICC) was used to assess the consistency of the angle measurements. Spearman's rank correlation analysis was used to evaluate the correlation between preoperative clinical data, incident angles, and the pathological nature of the breast nodules. Receiver Operating Characteristic (ROC) curves for the individual incident angle, the BI-RADS classification, and an integration of the individual incident angle and ultrasound malignant features for BI-RADS classification were plotted, and the areas under the curve (AUC) were calculated and compared using the Z-test, respectively. The optimal cutoff value for the incident angle for the malignancy risk assessment of breast nodules was determined using the Youden index (sensitivity + specificity−1). A two-sided P value of < 0.05 was considered statistically significant.
Results
Final sample of the study
Out of 21,398 patients who underwent ultrasound examinations, 15,978 patients were found to have breast nodules. Among these, 12,669 patients had solid breast nodules. Among these patients, 2534 patients had lesions with blood flow signals(vascularity). Out of these, 507 patients underwent surgical treatment with histopathological results. In this group, 185 patients had the incident angle of the main artery in the breast nodule measured; 93 of these patients had malignant lesions, and 92 patients had benign lesions. 5420 patients without lesions were excluded, along with 2556 patients with BI-RADS category 2, 428 patients under the age of 18, 325 patients with a history of radiation, chemotherapy, or other drug treatments, and 10,135 patients with breast nodules showing no blood flow signals (vascularity). The demographic and baseline characteristics of the study patients are summarized in Table 1. A flow chart of the patient enrollment and study is shown in Fig. 2.

The flowchart shows the reasons the patients were excluded from this study.
Outcome of statistical analysis
The mean ages of the malignant and benign groups were (50.87 ± 10.12) years and (36.35 ± 11.26) years, respectively, with a significant difference (t = − 9.228, P < 0.001, 95% CI = − 17.628 to − 11.418). The median BMI of the malignant group was 22.89 (21.08, 25.31) and for the benign group was 22.27 (19.69, 24.32), with a significant difference in overall BMI distribution (Z = − 2.079, P = 0.038). The prevalence of a family history of breast cancer was higher in the malignant group (9.7%) compared to the benign group (1.1%), with a significant difference (χ2 = 5.100, P = 0.024). The mean incident angles for the benign and malignant groups were (41.47 ± 14.28)° and (22.65 ± 11.09)°, respectively, with a significant difference (t = 10.027, P < 0.001, 95% CI = 15.114–22.535). The palpable rate of nodules was higher in the malignant group (83.9%) than in the benign group (63.0%), with a significant difference (χ2 = 10.303, P < 0.002). The rate of abnormal axillary lymph nodes was significantly higher in the malignant group (24.7%) compared to the benign group (5.4%) (x2 = 13.407, P < 0.001). There were no significant differences in breast nodule pain, nipple discharge, breast skin edema, nodule location, quadrant, and length between the two groups (each P > 0.05), as shown in Table 1 and Figs. 3 and 4. The pathological distribution of breast nodules is shown in Table 2. The ICC was 0.975, P < 0.001. Spearman’s rank correlation analysis showed a significant positive correlation between age (r = 0.620, P < 0.001), BMI (r = 0.214, P = 0.013), family history (r = 0.190, P = 0.010), palpable nodules (r = 0.236, P = 0.001), abnormal axillary lymph nodes (r = 0.291, P < 0.001) and the pathological malignancy of breast nodules; and a significant negative correlation between incident angle and pathological malignancy (r = − 0.593, P < 0.001). For the 185 breast nodules, the ultrasound BI-RADS classification was as follows: 37 nodules were assigned to category 3, 27 nodules were assigned to category 4a, 41 nodules were assigned to category 4b, 42 nodules were assigned to category 4c, and 38 nodules were assigned to category 5, as compared with their corresponding pathological results, as shown in Table 3. Based on histopathological results as the gold standard, the breast nodules were classified for malignancy, and ROC curves were plotted to assess the evaluation efficacy of the incident angle, BI-RADS classification, and their combination on the malignancy risk of breast nodules. The results showed that the best cutoff value for distinguishing benign and malignant breast nodules using the vessel incident angle was 26.9°, with a sensitivity of 76.34%, specificity of 84.78%, positive predictive value of 83.53%, negative predictive value of 78.00%, and AUC of 0.853. The diagnostic performance of BI-RADS classification alone in assessing the malignant risk of breast nodules showed a sensitivity of 78.50%, specificity of 92.39%, positive predictive value of 91.25%, negative predictive value of 79.95%, and AUC of 0.905. The combined BI-RADS classification and vessel incident angle assessment for breast nodule malignancy risk demonstrated a sensitivity of 90.32%, specificity of 89.13%, positive predictive value of 89.36%, negative predictive value of 90.11%, and AUC of 0.940. The differences in sensitivity, negative predictive value, and AUC between BI-RADS classification alone and the combination of BI-RADS classification and vascular incident angle were all statistically significant (χ2 = 4.943, P = 0.026; χ2 = 3.243, P = 0.042; Z = 2.955, P = 0.003), as shown in Table 4 and Fig. 5.

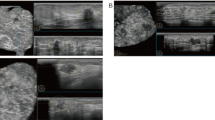
A 62-year-old female with ductal invasive carcinoma of the right breast. (A) The left panel shows the incident angle of the main blood vessels of the breast nodule is 11.5°; (B) the right panel shows histopathology (HE × 200).

A 26-year-old woman with fibroadenoma of the right breast. (A) The left panel shows the incident angle of the main vessel of the breast nodule is 68.7°; (B) the right panel shows histopathology (HE × 200).

The ROC curves of malignancy risk of breast nodules assessed by the two methods.
Discussion
The 2013 edition of the BI-RADS classification has been widely used in the stratification of malignancy risk in breast nodules. However, in the ultrasound BI-RADS classification imaging lexicon, the vascularity condition of the breast nodule is categorized as an “associate features” with only general descriptions, such as absence of vascularity, internal vascularity, and vessels in the rim of the breast nodule, which are somewhat vague9. The blood vessel density, distribution, and structure in malignant tumors have been extensively studied. Samejima et al. found that the blood vessel density around the breast cancers did not change in association with an increase in tumor size, suggesting that blood vessels around a breast cancer may increase correspondingly with the increase of the square of the tumor diameter11. Some studies have shown that, compared to normal breast vessels, malignant breast tumor vessels have more branches and are more tortuous; in comparison with benign breast tumors, the vascular distribution in malignant tumors is disordered and tortuous12,18. Watanabe et al.15 found that the absence of vascularity, presence of peripheral vascularity, or predominantly peripheral vascularity, suggest likelihood of a benign breast nodule; whereas the presence of internal vascularity or predominantly internal vascularity suggests a high likelihood of a malignant breast nodule. Chang et al.19,20 found that compared to benign breast tumors, malignant breast tumors often have wider internal vessel diameters, more disordered distribution, and the vessels may be curved or intertwined. A study by Gu et al.8 found that there are significant differences in the vascular distribution types between benign and malignant breast nodules, with a positive predictive value of 56.4% (648/1148) for those displayed inside the breast nodule. Thus, the vascularity display pattern can provide important information for assessing the malignant risk of breast nodules.
The vascularity distribution patterns of breast nodules were characterized as absent, internal, or peripheral in the previous studies8,9,15. The vascularity in the inside of the breast nodule is diversifying in coursing, but if we only give an overall description, the more detailed characteristics of its distribution in benign and malignant nodules might not be fully reflected, potentially leading to bias.A further study by Chang et al.16 using three-dimensional Doppler ultrasound imaging technology and comprehensive quantitative analysis found not only differences in the morphology, tortuosity, internal diameter, distribution, and direction of vessels within benign and malignant tumors, but also significant differences in the vascular parameters of the surrounding breast tissue of benign and malignant tumors. Compared to benign tumors, the vascular density around malignant tumors is higher, with more vascularity, thicker main vessel diameters, and longer lengths. Comparing the morphological characteristics of benign and malignant breast nodules, there are significant differences, affecting the analysis of vascular characteristics around the tumors. Therefore, when analyzing the vascular features of the surrounding tissue of benign and malignant tumors, the morphological characteristics of the tumor should also be considered16.
This study used CDFI to detect the vascularity distribution in breast nodules and quantitatively measured the incident angle of the main artery in the breast nodules, and the correlation between the incident angle and the malignancy risk of breast nodules was obtained through statistical analysis, making the methodology was more scientifically sound and reliable. In this study, the ICC for measuring the incident angle of the main artery was 0.975, indicating good consistency and repeatability in the measurement method. The study results showed that the average incident angle for benign nodules was (41.47 ± 14.27)° and for malignant nodules was (22.65 ± 11.09)°, with a significant difference (P < 0.001). Spearman’s rank correlation analysis showed a significant negative correlation between the incident angle size and pathological malignancy (r = − 0.593, P < 0.001). It was inferred that malignant breast nodules have a smaller incident angle, predominantly displaying internal vascularity pattern, while benign nodules have a larger incident angle, predominantly displaying a peripheral vascularity pattern. This conclusion is consistent with the findings by Watanabe et al.15. There is some overlap in the incident angles between benign and malignant breast nodules. The best cutoff value for distinguishing the benign and malignant breast nodules using only the vascular incident angle was 26.9°, with a sensitivity of 76.34%, specificity of 84.78%, positive predictive value of 83.53%, negative predictive value of 78.00%, and AUC of 0.853 (95% CI 0.794–0.901). This suggests that the incident angle aids in improving the assessment of the benign or malignant nature of breast nodules, similar to the findings of Kujiraoka et al.21.
The present study results showed that the negative predictive values obtained from the vessel incident angle, BI-RADS classification, and their combination for the evaluation of the breast nodules were 78.00%, 79.95%, and 90.11%, respectively, all higher than those in a previous study8. The negative predictive value of the combined vascular incident angle and BI-RADS classification in assessing the malignancy risk of breast nodules (90.11%) was significantly higher than that of the BI-RADS classification alone (79.95%), with a statistically significant difference (P < 0.05). Therefore, combining the main arterial incident angle and BI-RADS classification for the evaluation of breast nodules provides a new perspective for clinical practice, potentially reducing many unnecessary biopsies.
By comparing the AUC of BI-RADS classification with the combined main arterial incident angle and BI-RADS classification in assessing the malignancy risk of breast nodules, we found that the AUC of the combined method (0.940) was higher than that of the sole BI-RADS classification (0.905), with a statistically significant difference (P < 0.05). Thus, introducing the incident angle of the main artery of breast nodules for assessing their malignancy risk has additional value in improving assessment efficacy.
This study has some limitations: (1) The sample size is relatively small, and most breast nodules with lower BI-RADS classifications were not included in the study due to the lack of histopathological results; (2) Some breast nodules were excluded from CDFI and/or evaluation due to the absent display of vascularity or non-compliance with requirements; (3) The size of the breast nodules included in this study was relatively large, and most nodules smaller than 1 cm were not included due to difficulty in displaying vessels. These factors may lead to selection bias in the sample; (4) There was no investigation of the pathophysiology of differences in vascular angles between benign and malignant breast nodules, and further exploration is needed in the future; (5) The fact that a significant number of solid breast nodules without color Doppler detectable blood vessels may impact the utility of the present study results, and using the incident angle of the main artery of breast nodules for the assessment of malignany risk only suitable for those with visible main blood vessel. In the future, using superb microvascular imaging may improve the visualization of the breast vascularity and the identification of the penetrating and branching vessels, and augmenting the utility of measuring the incident angle of the main artery of breast nodules12.
Conclusion
Measuring the incident angle of the main artery of breast nodule using color Doppler ultrasound can improve the efficacy of assessing the malignant risk of breast nodules. Combining the main arterial incident angle with BI-RADS classification can significantly increase the negative predictive value of breast nodule assessment, and may reduce unnecessary biopsies.
Data availability
The data that support the findings of this study are available within the paper and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at the PACS and HIS.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263 (2024).
Guo, Q. et al. Assessing risk category of breast cancer by ultrasound imaging characteristics. Ultrasound Med. Biol. 44, 815–824 (2018).
Duggan, C. et al. The breast health global initiative 2018 global summit on improving breast healthcare through resource-stratified phased implementation: Methods and overview. Cancer 126, 2339–2352 (2020).
Tabár, L. et al. The incident of fatal breast cancer measures the increased effectiveness of therapy in women participating in mammography screening. Cancer 125, 515–523 (2019).
Shi, X. Q. et al. A set of shear wave elastography quantitative parameters combined with ultrasound BI-RADS to assess benign and malignant breast lesions. Ultrasound Med. Biol. 41, 960–966 (2015).
Li, X. L. et al. Value of virtual touch tissue imaging quantification for evaluation of ultrasound breast imaging-reporting and data system category 4 lesions. Ultrasound Med. Biol. 42, 2050–2057 (2016).
Wang, M. et al. Differential diagnosis of breast category 3 and 4 nodules through BI-RADS classification in conjunction with shear wave elastography. Ultrasound Med. Biol. 43, 601–606 (2017).
Gu, Y. et al. The utility of the fifth edition of the BI-RADS ultrasound lexicon in category 4 breast lesions: A prospective multicenter study in China. Acad. Radiol. 29, 26–34 (2022).
Mendelson, E. B. et al. ACR BI-RADS® ultrasound. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System (American College of Radiology, 2013).
He, X. et al. Development and validation of a prediction model for the diagnosis of breast cancer based on clinical and ultrasonic features. Gland. Surg. 12, 736–748 (2023).
Samejima, F. et al. A study on the vascular proliferation in tissues around the tumor in breast cancer. Jpn. J. Surg. 18(3), 235–242 (1988).
Zhu, A. et al. A comparative study on superb microvascular imaging and conventional ultrasonography in differentiating BI-RADS 4 breast lesions. Oncol. Lett. 18(3), 3202–3210 (2019).
Darlington, C. D. et al. Squamous cell carcinoma of the breast mimicking chronic breast abscess. Niger. J. Surg. 25, 101–103 (2019).
Cilekar, M. et al. An atypical cause of rapidly progressing breast lump with abscess formation: Pure squamous cell carcinoma of the breast. J. Cancer Res. Ther. 11, 1023 (2015).
Watanabe, T. et al. Multicenter prospective study of color doppler ultrasound for breast masses: Utility of our color doppler method. Ultrasound Med. Biol. 45, 1367–1379 (2019).
Chang, Y. C. et al. Vascular morphology and tortuosity analysis of breast tumor inside and outside contour by 3-D power Doppler ultrasound. Ultrasound Med. Biol. 38, 1859–1869 (2012).
Zanotelli, M. R. et al. Mechanical forces in tumor angiogenesis. Adv. Exp. Med. Biol. 1092, 91–112 (2018).
Huang, S. F. et al. Analysis of tumor vascularity using three-dimensional power Doppler ultrasound images. IEEE Trans. Med. Imaging 27, 320–330 (2008).
Chang, R. F. et al. Computer algorithm for analysing breast tumor angiogenesis using 3-D power doppler ultrasound. Ultrasound Med. Biol. 32, 1499–1508 (2006).
Chang, R. F. et al. Solid breast masses: Neural network analysis of vascular features at three-dimensional power Doppler US for benign or malignant classification. Radiology 243, 56–62 (2007).
Kujiraoka, Y. et al. Incident angle of the plunging artery of breast tumors. In Research and development in breast ultrasound (eds Ueno, E. et al.) p72-75 (Springer, 2005).
Author information
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, K., Wu, S. Integrating the incident angle of main vessel of breast nodule with BI-RADS can improve the efficacy of breast malignancy evaluation. Sci Rep 14, 20783 (2024). https://doi.org/10.1038/s41598-024-71567-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71567-0
