
Abstract
Cavities are characteristic radiological features related to increased mycobacterial burden and poor prognosis in Mycobacterium avium complex pulmonary disease (MAC-PD). However, cavity changes following treatment and their clinical implications remain unknown. We aimed to elucidate whether cavity obliteration or reduction in cavity size or wall thickness correlates with microbiological cure. In total, 136 adult patients with cavitary MAC-PD treated for ≥ 6 months between January 1st, 2009, and December 31st, 2021, in a tertiary referral centre in South Korea were enrolled. The cavity with the largest diameter at treatment initiation was tracked for size and thickness changes. Following median treatment of 20.0 months, 74 (54.4%) patients achieved microbiological cure. Cavity obliteration, achieved in 58 (42.6%) patients at treatment completion, was independently associated with microbiological cure. In patients with persistent cavities, size reduction of ≥ 10% was significantly associated with microbiological cure, whereas thickness reduction was not. Five-year mortality rates in patients with cavity obliteration, persistent but reduced cavity, and persistent cavity without shrinkage were 95.6%, 72.1%, and 65.3%, respectively (P < 0.001). In conclusion, cavity obliteration or shrinkage at treatment completion is associated with microbiological cure and reduced mortality in MAC-PD, suggesting that cavity changes could serve as a proxy indicator for treatment response.
Similar content being viewed by others
Introduction
Nontuberculous mycobacterial pulmonary disease (NTM-PD) is a chronic lung condition caused by mycobacteria other than Mycobacterium tuberculosis complex and Mycobacterium leprae1,2. After exclusion of other pulmonary diseases, diagnosis is established when patients exhibit pulmonary or systemic symptoms together with radiological features consistent with NTM-PD, as well as multiple positive NTM cultures from respiratory specimens1,2. NTM-PD can be classified into three clinical phenotypes: fibrocavitary, cavitary nodular bronchiectatic, and non-cavitary nodular bronchiectatic3. As implied by their names, the presence of cavitary changes is a characteristic radiological feature associated with disease progression and an unfavourable prognosis in patients with NTM-PD4.
Cavities are abnormal air-filled spaces that replace the normal lung parenchyma and are surrounded by inflammatory cells and fibrosis5,6,7. A concerted effort by macrophages, lymphocytes, and multinucleated giant cells to sequester mycobacteria and inhibit their spread results in the formation of granulomas6. The hypoxic and nutrient-deprived environment within these granulomas induces central necrosis, and subsequent expulsion of caseous necrotic materials into nearby bronchial trees leads to the development of cavities8. The presence of cavity is frequently associated with men, heavy smokers, patients with alcohol use disorder, and immunocompromised hosts with disturbed cell-mediated immunity9,10,11.
Patients with cavities observed on chest computed tomography (CT) are approximately five times more likely to experience disease progression necessitating antimycobacterial treatment12. Moreover, presence of cavities has consistently been associated with diminished health-related quality of life and increased mortality13,14. Consequently, current international treatment guidelines suggest initiating treatment in patients with cavitary lung disease rather than adopting a watchful waiting approach, after careful consideration of comorbidities, infecting species, patient priorities, and discussing the potential adverse effects and uncertain benefits of antibiotic therapy1.
Meanwhile, the changes in cavitary lesions following treatment and their clinical implications are largely unknown. The frequency of cavitary obliteration or reduction in size and wall thickness after treatment, as well as the impacts of these changes on the clinical outcomes of patients, remain unclear. The present study aimed to investigate the changes in cavitary lesions after treatment and clarify their relationships with treatment outcomes and long-term survival in patients with Mycobacterium avium complex pulmonary disease (MAC-PD), the most common form of NTM-PD.
Methods
Ethics statement
The study was approved and the requirement for informed consent was waived by the Institutional Review Board of Seoul National University Hospital (approval number: H-2311-030-1483) due to the retrospective nature of the study design. The study was performed in accordance with the principles of the Declaration of Helsinki.
Study population
We analysed consecutive patients treated for MAC-PD between January 1st, 2009 and December 31st, 2021 at a tertiary referral centre in South Korea. The following inclusion criteria were applied: (a) age ≥ 19 years, (b) satisfying the diagnostic criteria for NTM-PD1,2, (c) identification of MAC species by molecular methods15, (d) receipt of guideline-based therapy with a macrolide in combination with one or more of ethambutol, rifampicin, amikacin or streptomycin, and clofazimine for ≥ 6 months, and (e) confirmed presence of ≥ 1 cavitary changes annotated by a radiologist on a chest CT scan at initiation of treatment. The exclusion criteria were absence of chest CT scans at the start and end of treatment within a window period of 4 months, and performance of acid-fast bacilli (AFB) cultures fewer than three times during the treatment period, hindering assessment of the treatment response. Our study included patients whose cavitary lesions were diagnosed by their attending physicians as attributable to MAC-PD and not to other causes, including tuberculosis, fungal infections, or malignancies. Cases where alternative aetiologies were identified were excluded. We also included patients with antibiotic resistance, including resistance to macrolides. Some patients from our previous studies were included16,17,18,19.
Data collection, follow-up, and outcome definition
We retrospectively collected demographic, clinical, bacteriological, and laboratory data including age, sex, body mass index (BMI), erythrocyte sedimentation rate, AFB smear positivity, mycobacterial culture results, causative species, macrolide resistance, comorbidities, smoking history, antibiotics usage, treatment duration, and performance of surgical resection. Patients undergoing treatment were followed up every 1–3 months. At each visit, sputum was collected for AFB smear analysis and mycobacterial culture, and chest radiographs, complete blood counts, and hepatic and renal function tests were performed. Chest CT scans were obtained at 6–12 months following treatment initiation. The primary outcome, microbiological cure, was defined as having ≥ 3 consecutive negative cultures collected ≥ 4 weeks apart20 and maintaining negative cultures until completion of treatment17. The secondary outcome was all-cause mortality. Data on survival status and date of death were obtained from a database verified by the Ministry of the Interior and Safety, South Korea.
Evaluation of cavity characteristics
We analysed chest CT scans using a picture archiving and communication system with a preset CT assessment protocol21,22,23. After an educational and Q&A session prior to data collection, a group of board-certified pulmonologists blinded to treatment outcomes obtained information regarding the number, lobar distribution, and bilateral occurrence of cavities on chest CT scans at treatment initiation and completion. The left upper and lingular divisions were counted as distinct lobes23. The cavity with the largest diameter was tracked for changes in size and wall thickness. The maximum transverse diameter, determined by measuring the longest outer diameter including wall thickness on axial images with a slice thickness of 1.00 or 1.25 mm served as the cavity size22. The greatest wall thickness on the CT section where the transverse diameter was measured was noted as the wall thickness21. Uncertainties in measurement were resolved after consultation with the first and corresponding authors. Cavity obliteration was defined as closure or healing of cavities resulting in the absence of abnormal air-filled spaces, and usually transforming into a fibrous scar or nodule (Fig. 1)24. Patients who underwent complete surgical resection of cavities leading to absence of residual lesions were also considered to have achieved cavity obliteration and were included in this study to provide a more comprehensive view of current treatment options and outcomes.

Examples of cavity obliteration. Serial chest computed tomography (CT) scans of patients who achieved cavity obliteration following treatment. (A) Baseline CT scan of a woman in her seventies infected with Mycobacterium intracellulare reveals a cavity in her right lower lobe. After 18 months of antibiotic treatment, her cavity was obliterated and transformed into a nodular lesion, and she achieved microbiological cure. (B) Despite treatment with antibiotics for almost 3 years, a woman in her sixties infected with M. intracellulare had persistently positive mycobacterial cultures with minimal radiological improvement. She underwent video-assisted thoracoscopic surgery to remove the lingular division, the left lower lobe superior segment, and parts of the left lower lobe postero- and latero-basal segments. She continued antibiotic treatment for another 18 months after surgery and achieved microbiological cure.
Statistical analysis
Demographic and clinical characteristics at treatment initiation were compared between patients who achieved microbiological cure and those who did not. Categorical variables were presented as frequency with proportion and compared using Pearson’s χ2 test or Fisher’s exact test as indicated. Non-parametric continuous variables were presented as median with interquartile range (IQR) and compared using the Mann–Whitney U test.
We conducted logistic regression analysis to investigate the association between cavity obliteration at the end of treatment and microbiological cure in the entire study cohort. Subsequently, we analysed the associations between changes in size or wall thickness and microbiological cure among patients with persistent cavities. We employed three methods to examine the association between changes in size or wall thickness and microbiological cure. First, we explored the relationship between changes in size or wall thickness and microbiological cure as continuous variables. Second, we determined the minimal clinically important difference (MCID) and assessed changes in microbiological cure for reductions surpassing the MCID. The MCID was calculated by the receiver operating characteristic (ROC) method using microbiological cure as an anchor and the standard error of measurement (SEM) method for a distribution-based approach25,26, and the final MCID was determined by selecting the smaller of the two values. Third, we examined the association between a specific percentage reduction or increase and microbiological cure, with the specified percentage being the mean of the percentage change for each group. We also performed a sensitivity analysis after excluding patients who underwent surgical resection. Variable adjustments for multivariable analyses were based on clinical relevance, considering the associations with microbiological cure, and the inclusion criterion was set at a significance level < 0.1.
For survival analysis, the patients were categorised into three groups: (1) cavity obliteration, (2) persistent cavity with size reduction, and (3) persistent cavity without size reduction. We compared the survival rates in the three groups using Kaplan–Meier curves and log-rank test.
A value of P < 0.05 for two-tailed tests was considered statistically significant. All analyses were conducted using R software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
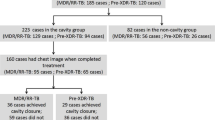
A total of 261 patients with cavitary MAC-PD treated for ≥ 6 months were identified during the study period. After excluding 21 patients without chest CT scans at baseline, 90 patients lacking chest CT scans at treatment completion, and 14 patients with fewer than three available AFB culture results during treatment, 136 patients (median age, 62.6 [IQR, 55.6–71.4] years; 30.1% men) were included in the analysis (Table 1). Fifty-two-point two percent of patients were infected with M. avium, 46.3% with M. intracellulare, and 1.5% with M. chimaera. The median number of cavities was 1 (IQR, 1–3). The median transverse diameter and wall thickness of the largest cavity were 25.8 (IQR, 16.1–42.0) mm and 6.8 (IQR, 3.8–9.4) mm, respectively (Table 2). No significant differences were observed between patients infected with M. avium and those with M. intracellulare (Supplementary Material).
After a median treatment duration of 20.0 (IQR, 15.3–28.2) months, 74 (54.4%) patients achieved microbiological cure. Patients who achieved microbiological cure were significantly younger than those who did not (P = 0.011). Other clinical characteristics including sex, BMI, macrolide resistance, prior tuberculosis, comorbidities, smoking history, and immunosuppressant use were comparable (Table 1). None of the patients in our study had HIV/AIDS. During a median follow-up period of 4.4 (IQR, 1.8–6.2) years, 23 patients died.
Cavity obliteration and treatment outcomes
No significant differences in baseline cavity characteristics, including size and wall thickness, were found between patients who achieved microbiological cure and those who did not (Table 2). Among the 136 patients, 58 (42.6%), including 16 patients with surgical resection, achieved obliteration of the largest cavity. The median time to obliteration was 13.3 (IQR, 10.7–19.7) months, and 12.9 (IQR, 10.7–16.5) months after excluding patients who underwent surgical resection. All but one patient maintained cavity obliteration until the end of treatment. Even in that patient, re-obliteration occurred by the completion of treatment. In the univariable analyses, cavity obliteration was associated with microbiological cure (odds ratio [OR], 2.88; 95% confidence interval [CI], 1.41–5.87; P = 0.004) (Table 3). Even after adjustment for relevant clinical factors, including age and M. intracellulare as causative species, cavity obliteration was independently associated with microbiological cure (adjusted OR, 2.41; 95% CI, 1.12–5.15; P = 0.024) (Table 3). The sensitivity analysis excluding 16 patients who underwent surgical resection showed similar results, and the significance was maintained (adjusted OR, 2.74; 95% CI, 1.18–6.37; P = 0.019) (Table 3).
Changes in cavity size or wall thickness and treatment outcomes
Among patients with persistent cavities, the mean change in transverse diameter of the largest cavity was − 1.24 [standard deviation (SD), ± 15.04] mm following treatment. The mean change in cavity diameter differed significantly by microbiological cure status [cured: mean, − 5.0 mm (− 12%); uncured: mean, + 1.7 mm (+ 11%); P = 0.035]. Decrease in cavity diameter, when considered as a continuous variable, was not significantly associated with microbiological cure (adjusted OR, 1.04; 95% CI, 1.00–1.08; P = 0.053) (Table 3), but a trend was suggested. Reduction in cavity size surpassing the MCIDs (ROC method, − 1.8 mm; SEM method, 2.1 mm) was significantly associated with microbiological cure (Table 3). Furthermore, ≥ 10% reduction in size was associated with microbiological cure (adjusted OR, 4.27; 95% CI, 1.52–12.03; P = 0.006), while ≥ 10% increase in size was associated with unfavourable outcome (adjusted OR, 0.23; 95% CI, 0.07–0.72; P = 0.012). Size reduction at 6 and 12 months was maintained through treatment completion in 81.6% (31/38) and 80% (24/30) of patients, respectively.
The mean change in wall thickness of the largest cavity was − 1.54 (SD, ± 5.51) mm following treatment. The mean change in wall thickness did not differ significantly between patients who achieved microbiological cure and those who did not (cured: mean ± SD, − 1.98 ± 4.54 mm; uncured: mean ± SD, − 1.20 ± 6.18 mm; P = 0.73). Regardless of reduction or increase, a change in wall thickness was not associated with microbiological cure (Table 3).
Cavity obliteration or change in cavity size and survival
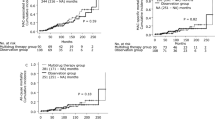
When Kaplan–Meier curves stratified by cavity status were plotted, the survival curves diverged significantly (P < 0.001). The 5-year mortality rates in patients with cavity obliteration, persistent cavity with size reduction, and persistent cavity without size reduction were 95.6% (95% CI, 89.8%–100%), 72.1% (95% CI, 56.7%–91.6%), and 65.3% (95% CI, 49.1%–87.0%), respectively (Fig. 2).

Cavity obliteration or size changes and survival. Kaplan–Meier survival curves of patients with cavity obliteration (black), persistent cavity with size reduction (red), and persistent cavity without size reduction (blue). The 5-year mortality rates in patients with cavity obliteration, persistent cavity with size reduction, and persistent cavity without size reduction were 95.6% (95% CI, 89.8–100%), 72.1% (95% CI, 56.7–91.6%), and 65.3% (95% CI, 49.1–87.0%), respectively.
Discussion
In this cohort study involving 136 patients with cavitary MAC-PD, we examined the associations of changes in cavity characteristics with treatment outcomes. Cavity obliteration, characterised by closure or complete removal of abnormal air-filled spaces, was significantly associated with microbiological cure. Meanwhile, patients with a reduction in cavity size despite cavity persistence had a higher likelihood of achieving microbiological cure. Patients with cavity obliteration exhibited the longest survival, followed by those with reduced cavity size despite cavity persistence and those with persistent cavity without size reduction.
Our findings have clinical significance because, to date, limited data have been available regarding the dynamic changes in cavities during treatment and their clinical implications. Previous studies have primarily focused on the radiological characteristics, including cavitation, at the start of treatment3,27. The lack of longitudinal data has meant that understanding of how cavities evolve during treatment and the potential clinical implications of the changes have remained unclear. In the present study, a substantial proportion (42.6%) of the patients experienced cavity obliteration after treatment. Among the remaining patients with persistent cavities, more than half (57.7%) experienced a reduction in size. In addition, cavity obliteration and shrinkage were associated with microbiological cure and, eventually, survival. Our results demonstrate that cavities do not remain static but rather change dynamically with treatment, and that the changes are closely related to microbiological and long-term outcomes.
The cavities in MAC-PD represent the frontline for encounters between host immunity and pathogens, similar to the case for pulmonary tuberculosis8. Consequently, cavity obliteration signifies that the host immune system has achieved successful containment and suppression of the pathogen, coupled with antibiotic treatment. This achievement mitigates inflammation and diminishes the risk of additional bacilli dissemination. The median time to cavitary obliteration was approximately 13 months in our study. Once cavity obliteration was achieved, it was highly unlikely to aggravate afterwards. Among patients with non-obliterated cavities, 80% of patients whose cavity size was reduced at 12 months of treatment maintained this trend until treatment completion. However, if cavity was enlarged after 12 months of treatment, the chance of further improvement was significantly rare. These findings suggest that obtaining CT scans around one year of treatment might be a reasonable option. Additional CT scans may be unnecessary for patients whose cavities are obliterated or reduced in size at 12 months. Conversely, additional interventions, such as surgical removal of the cavity, should be discussed with patients whose cavities are unresponsive to more than 12 months of antibiotic treatment28.
In the present study, change in wall thickness was not associated with treatment response. Because thicker cavity walls have been linked to higher degrees of AFB smear positivity in pulmonary tuberculosis29, we hypothesised that wall thickness may indirectly represent the mycobacterial burden. In our analysis, wall thickness decreased with treatment regardless of the microbiological outcome, suggesting its responsiveness to treatment. Our findings further demonstrated that, rather than the inner wall thickness composed of necrotic cellular debris and cholesterols, the transverse diameter of cavities reflecting the entire granulomatous inflammation constructed by the host defence mechanism may be a more suitable indicator of treatment response.
Our finding that cavity obliteration following treatment is associated with microbiological cure suggests that the cavities in MAC-PD reflect the overall bacillary burden, similar to the case for pulmonary tuberculosis8. Based on our previous observation that microbiological cure is associated with long-term survival irrespective of cavity presence at treatment completion17, the prolonged survival observed in patients experiencing cavity obliteration may be attributed to a reduction in the mycobacterial burden. Hence, it is reasonable to assume that cavity changes can be a surrogate measure for the mycobacterial burden rather than an independent prognostic factor for survival. In this context, our findings demonstrate that cavity changes can serve as an additional proxy indicator for evaluation of treatment response, complementing mycobacterial culture results. Assessment of changes in cavity size during treatment could be especially useful when evaluating the treatment response in patients who cannot expectorate sputum20.
The strength of this study lies in the utilisation of longitudinal CT scan data in a cohort of patients with cavitary MAC-PD to shed light on the changes in cavity characteristics after treatment associated with microbiological response and long-term survival. However, a major limitation is that a substantial number of patients were excluded from the analysis due to the unavailability of CT scans at treatment completion. Furthermore, few (1.5%) patients were infected with M. chimaera, which is relatively rare in Korean cohorts30,31. Since virulence and clinical course can vary by species32, our findings may have limited applicability in regions where the prevalence of causative species differs. We also included patients who underwent surgical resection during antibiotic treatment to provide a more comprehensive view of current treatment options and outcomes. However, the characteristics of these patients may differ from those who received only medical treatment, such as having more localized disease or being less frail. Nonetheless, results were maintained even after excluding surgical patients in the sensitivity analysis.
In conclusion, cavity obliteration or size reduction at the end of treatment in patients with MAC-PD is associated with microbiological cure and reduced mortality. Cavity changes have the potential to serve as a surrogate marker for treatment response supplementing microbiological culture data.
Data availability
The datasets used in the current study are available from the corresponding author on reasonable request after Institutional Review Board approval.
Change history
07 November 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-27032-7
References
Daley, C. L. et al. Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clin. Infect. Dis. 71, e1–e36 (2020).
Griffith, D. E. et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 175, 367–416 (2007).
Koh, W.-J. et al. Outcomes of Mycobacterium avium complex lung disease based on clinical phenotype. Eur. Respir. J. 50(3), 1602503 (2017).
Jhun, B. W. et al. Prognostic factors associated with long-term mortality in 1445 patients with nontuberculous mycobacterial pulmonary disease: a 15-year follow-up study. Eur. Respir. J. 55(1), 1900798 (2022).
Gadkowski, L. B. & Stout, J. E. Cavitary pulmonary disease. Clin. Microbiol. Rev. 21, 305–333 (2008).
Ihms, E. A., Urbanowski, M. E. & Bishai, W. R. Diverse cavity types and evidence that mechanical action on the necrotic granuloma drives tuberculous cavitation. Am. J. Pathol. 188, 1666–1675 (2018).
Hansell, D. M. et al. Fleischner society: Glossary of terms for thoracic imaging. Radiology 246, 697–722 (2008).
Urbanowski, M. E., Ordonez, A. A., Ruiz-Bedoya, C. A., Jain, S. K. & Bishai, W. R. Cavitary tuberculosis: The gateway of disease transmission. Lancet Infect. Dis. 20, e117–e128 (2020).
Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Medical Section of the American Lung Association. Am. J. Respir. Crit. Care Med. 156, S1–25 (1997).
Lee, Y. et al. CT findings of pulmonary non-tuberculous mycobacterial infection in non-AIDS immunocompromised patients: A case-controlled comparison with immunocompetent patients. Br. J. Radiol. 86, 20120209 (2013).
Henkle, E. & Winthrop, K. L. Nontuberculous mycobacteria infections in immunosuppressed hosts. Clin. Chest Med. 36, 91–99 (2015).
Kim, S. J. et al. Characteristics associated with progression in patients with of nontuberculous mycobacterial lung disease : A prospective cohort study. BMC Pulm. Med. 17, 5 (2017).
Kim, H. J. et al. BACES score for predicting mortality in nontuberculous mycobacterial pulmonary disease. Am. J. Respir. Crit. Care Med. 203, 230–236 (2021).
Ogawa, T. et al. Longitudinal validity and prognostic significance of the St George’s Respiratory Questionnaire in Mycobacterium avium complex pulmonary disease. Respir. Med. 185, 106515 (2021).
CLSI. Laboratory Detection and Identification of Mycobacteria (2nd ed.) CLSI guideline M48 (Clinical and Laboratory Standards Institute, 2018).
Kim, J. Y. et al. Outcomes of adjunctive surgery for nontuberculous mycobacterial pulmonary disease. BMC Pulm. Med. 21, 312 (2021).
Kim, J. Y. et al. Microbiological cure at treatment completion is associated with longer survival in patients with Mycobacterium avium complex pulmonary disease. Chest 164, 1108–1114 (2023).
Kim, J. Y. et al. Impact of treatment on long-term survival of patients with Mycobacterium avium complex pulmonary disease. Clin. Infect. Dis. 77, 120–126 (2023).
Kim, J. Y. et al. Post-treatment radiographic severity and mortality in Mycobacterium avium complex pulmonary disease. Ann. Am. Thorac. Soc. 21, 235–242 (2024).
van Ingen, J. et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: an NTM-NET consensus statement. Eur. Respir. J. 51(3), 1800170 (2018).
Cheon, H. Comparison of CT findings of between MDR-TB and XDR-TB: A propensity score matching study. Imaging Med. 9, 125–129 (2017).
Kang, H. R. et al. Clinical implications of size of cavities in patients with nontuberculous mycobacterial pulmonary disease: A single-center cohort study. Open Forum Infect. Dis. 8(3), ofab087 (2021).
Kim, H. S. et al. Serial CT findings of Mycobacterium massiliense pulmonary disease compared with Mycobacterium abscessus disease after treatment with antibiotic therapy. Radiology 263, 260–270 (2012).
Tokugawa, H. The cavity healing in pulmonary tuberculosis. Keio J. Med. 4, 65–92 (1955).
Tahira, D. et al. Evaluating the credibility of anchor based estimates of minimal important differences for patient reported outcomes: Instrument development and reliability study. BMJ 369, m1714 (2020).
Terwee, C. B. et al. Mind the MIC: Large variation among populations and methods. J. Clin. Epidemiol. 63, 524–534 (2010).
Rawson, T. M. et al. Factors which influence treatment initiation for pulmonary non-tuberculous mycobacterium infection in HIV negative patients; A multicentre observational study. Respir. Med. 120, 101–108 (2016).
Kim, J. Y., Lee, H. W., Yim, J. J. & Kwak, N. Outcomes of adjunctive surgery in patients with nontuberculous mycobacterial pulmonary disease: A systematic review and meta-analysis. Chest 163, 763–777 (2023).
Ors, F. et al. High-resolution CT findings in patients with pulmonary tuberculosis: Correlation with the degree of smear positivity. J. Thorac. Imaging 22, 154–159 (2007).
Kim, M. J. et al. Identification of nontuberculous mycobacteria in patients with pulmonary diseases in Gyeongnam, Korea, using multiplex PCR and multigene sequence-based analysis. Can. J. Infect. Dis. Med. Microbiol. 2021, 8844306 (2021).
Kim, S. Y. et al. Distribution and clinical significance of Mycobacterium avium complex species isolated from respiratory specimens. Diagn. Microbiol. Infect. Dis. 88, 125–137 (2017).
Boyle, D. P., Zembower, T. R., Reddy, S. & Qi, C. Comparison of clinical features, virulence, and relapse among Mycobacterium avium complex species. Am. J. Respir. Crit. Care Med. 191, 1310–1317 (2015).
Author information
Authors and Affiliations
Contributions
J-YK: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Visualization, Writing-original draft, Writing-review & editing; JB: Methodology, Investigation, Data curation, Writing-review & editing; KH: Data curation, Writing-review & editing; IL: Data curation, Writing-review & editing; H-JP: Data curation, Writing-review & editing; SYK: Data curation, Writing-review & editing; K-EL: Data curation, Writing-review & editing; YHA: Data curation, Writing-review & editing; SMY: Data curation, Writing-review & editing; NK: Data curation, Methodology, Resources, Writing-review & editing; J-JY: Conceptualization, Data curation, Methodology, Project administration, Resources, Supervision, Visualization, Writing-review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the IRB approval number in the Ethics statement, in the Methods section. It now reads: “The study was approved and the requirement for informed consent was waived by the Institutional Review Board of Seoul National University Hospital (approval number: H-2311-030-1483) due to the retrospective nature of the study design. The study was performed in accordance with the principles of the Declaration of Helsinki.”
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kim, JY., Bae, J., Hyung, K. et al. Significance of changes in cavity after treatment in Mycobacterium avium complex pulmonary disease. Sci Rep 14, 21133 (2024). https://doi.org/10.1038/s41598-024-71971-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-71971-6
