
Abstract
Sex and gender differences play a crucial role in health and disease outcomes. This study used data from the National Health and Nutrition Examination Survey to explore how environmental exposures affect health-related traits differently in males and females. We utilized a sex-stratified phenomic environment-wide association study (PheEWAS), which allowed the identification of associations across a wide range of phenotypes and environmental exposures. We examined associations between 272 environmental exposures, including smoking-related exposures such as cotinine levels and smoking habits, and 58 clinically relevant blood phenotypes, such as serum albumin and homocysteine levels. Our analysis identified 119 sex-specific associations. For example, smoking-related exposures had a stronger impact on increasing homocysteine, hemoglobin, and hematocrit levels in females while reducing serum albumin and bilirubin levels and increasing c-reactive protein levels more significantly in males. These findings suggest mechanisms by which smoking exposure may pose higher cardiovascular risks and greater induced hypoxia for women, and greater inflammatory and immune responses in men. The results highlight the importance of considering sex differences in biomedical research. Understanding these differences can help develop more personalized and effective health interventions and improve clinical outcomes for both men and women.
Similar content being viewed by others

Introduction
Sex and gender differences are crucial in health and disease outcomes1. These differences in disease prevalence, risk factors, progression, and treatment response underscore the importance of considering sex and gender differences in biomedical research. For instance, females are at greater risk of developing immune diseases, while males have a higher risk of non-reproductive cancers2. Additionally, cardiovascular diseases have different pathologic mechanisms across sexes3, and females are more susceptible to chronic obstructive pulmonary disease (COPD)4.
While some sex and gender differences are well-documented across various health outcomes, significant gaps remain in our understanding of how environmental factors contribute to these disparities. This gap is particularly evident in research on environmental influences on health, which has yet to explore how these exposures differentially affect males and females extensively5. For example, sex differences in response to environmental exposures, such as those observed in occupational asthma and smoking-related lung function decline, highlight the need for more comprehensive studies in this area6,7,8,9,10.
Some sex differences, such as the difference in occupational asthma, might be explained by different degrees of environmental exposure between sexes, which might be attributed to gender differences6. In contrast, other differences, such as mortality and lung function differences between male and female smokers, are due to differential effects of the same environmental exposure10. Differential biological pathways, interactions with sex hormones, or genetic and epigenetic mechanisms might mediate the latter type of differences11.
Sex refers to the biological attributes that distinguish male and female organisms, including chromosomes, hormone levels, and reproductive anatomy. These biological differences are typically categorized as male or female but include intersex. Gender, on the other hand, refers to the roles, behaviors, activities, expectations, and norms that cultures and societies consider appropriate for men, women, and gender-diverse people. It is crucial to understand the distinction and the potential for interaction between sex and gender in biomedical research, as both can influence health outcomes and provide different interpretative scopes1,12.
Adopting research methodologies that capture the complex interplay between sex, environmental exposures, and health outcomes is essential to addressing these gaps. Genome-wide association studies (GWAS) and phenome-wide association studies (PheWAS) have been pivotal in identifying genetic and phenotypic associations, respectively, across diverse populations13,14,15,16,17,18,19,20. Environment-wide association studies (EWAS) have expanded on these methodologies and explored the associations between numerous environmental exposures and health outcomes21,22,23,24,25. While evaluating associations between multiple exposures and a single phenotype in EWAS has proven valuable, considering phenotypes in isolation can hinder the ability to detect exposures with cross-phenotype associations or associations between a single environmental exposure and multiple phenotypes.
Understanding the sex-specific effects of environmental exposures is crucial for assessing environmental risks, guiding therapeutic recommendations, and generating new biological hypotheses. To address this knowledge gap, we conducted a sex-stratified phenomic environment-wide association study (PheEWAS) to investigate the associations between environmental exposures and clinically relevant phenotypes. PheEWAS is a hypothesis-free approach that tests for significant associations between multiple environmental exposures and multiple phenotypes. By examining these associations across a broad range of phenotypes, this study aims to uncover sex-specific mechanisms that could inform precision health strategies and improve clinical outcomes. Utilizing data from the National Health and Nutrition Examination Survey (NHANES), we evaluated 18,937 participants across 58 phenotypes and 272 environmental exposures. By classifying sex-different exposure-phenotype associations into pure, quantitative, and qualitative categories26, we aim to elucidate the mechanisms underlying these associations and provide insights that could inform precision health approaches. Our results suggest promising avenues to explore exposures that pose differential risks to the sexes, elucidate biological pathways with significant sex-based differences, and open the road to more personalized therapeutics.
Materials and methods
NHANES data sets
This study utilized data from NHANES to identify sex-specific exposure-phenotype associations. NHANES is a program of studies that uses data from physical examinations and interviews to assess the health and nutritional status of adults and children in the U.S. The physical examination includes medical, dental, and physiological measurements and laboratory tests. The interview includes demographic, socioeconomic, dietary, and health-related questions.
We analyzed 1191 variables and 41,474 participants from four survey periods (1999–2000, 2001–2002, 2003–2004, and 2005–2006),27,28, using a discovery (1999–2000 and 2001–2002) and replication (2003–2004 and 2005–2006) design29,30, split by sex into four cohorts: discovery females (df), discovery males (dm), replication females (rf), and replication males (rm).
To select relevant phenotypes and exposures, we focused on 84 routine clinical measurements, including blood and urine biomarkers and hormones, and 739 exposures related to health outcomes, such as tobacco and alcohol use, heavy metals, and volatile compounds. PheEWAS, as a hypothesis-generating approach, relies on a wide selection of exposures and phenotypes, only restricted to retaining high-quality variables. Data cleaning procedures described below ensured high-quality phenotypes and exposures.
We applied survey weights according to NHANES guidelines, using 4-year weights for the discovery cohorts and adjusted 2-year weights for the replication cohorts. We excluded three phenotypes and 116 exposures lacking survey weight data. Data cleaning, QC, and analyses were done using CLARITE software30. All analytical steps and code are available in Zenodo (DOI: 10.5281/zenodo.6483503), along with replication instructions and package details.
Data quality control
The QC process was conducted independently in each of the four cohorts, but if a variable was removed in one cohort, it was removed from all. Participants aged 18 and older, with no upper age limit, and complete covariate data were included (\(N=18{,}937, N_{df}=4724, N_{dm}=4339, N_{rf}=5123, N_{rm}=4751\)). Low-density lipoprotein values (NHANES code name: LBDLDL) were adjusted by dividing by 0.7 for participants on statins.
Variables were categorized using CLARITE as constant, binary, categorical, and continuous. Constants (single-value variables that were not covariates or phenotypes), variables with only missing data, and continuous variables with less than ten unique values were removed. Filters ensured proper sample sizes and high-quality variables in each cohort. Variables with fewer than 200 non-missing values, binary or categorical variables with fewer than 200 observations per category, and continuous variables with more than 90% of values at zero were excluded. This left 59 phenotypes and 281 exposures.
Continuous variables were log2 transformed and z-score normalized to address skewed distributions while retaining biologically meaningful values. Briefly, transforming raw values into their base 2 logarithms provides a way to produce symmetric distributions and keep easily interpretable values because changes in a one-unit increase in a log2-transformed variable correspond to a doubling of the original value31,32. On the other hand, z-score normalization makes variables comparable even when measured on different scales or units, allowing comparisons across exposure-phenotype results. Outliers, defined as values three standard deviations from the mean, were treated as missing and re-filtered, removing nine additional exposures. A Pearson correlation was used to detect identical transformed variables, leading to the removal of one phenotype. The final dataset for PheEWAS included eight covariates, 58 phenotypes, and 272 exposures. Summary statistics for all covariates are available in Table 1.
Statistical methods
PheEWAS
Following the preparation and cleaning of the dataset, statistical analyses were conducted to explore the associations between exposures and phenotypes. A sex-stratified PheEWAS was conducted to estimate associations between 58 phenotypes and 272 exposures, adjusting for eight covariates, including age, socioeconomic status (SES), body mass index (BMI), survey year, and four race/ethnicity categories. Analyses were performed separately for each cohort using generalized linear models adjusted for survey weights. A minimum of 200 complete observations were required for a successful regression. Finally, observations were dropped in each regression if they had missing values in the phenotype or exposure or missing survey weight information. An inverse variance meta-analysis was used to generate sex-specific results in the female and male cohorts26,33.
Sex difference analysis
Sex differences in exposure-phenotype associations were assessed by comparing \(\beta\) values between males and females. Differences were categorized as pure (significant in one sex but not the other), quantitative (significant in both sexes with differing effect sizes), or qualitative (significant in both sexes with opposing effect directions). Two approaches were used to detect sex differences:
-
Full Evaluation Approach: all possible exposure–phenotype associations were tested for sex differences using the following formula
$$\begin{aligned} Z_{diff} = \frac{\beta _{f} - \beta _{m}}{\sqrt{se^2_{f} + se^2_{m}}} \end{aligned}$$(1)where \(\beta _{f}\) and \(\beta _{m}\) are the effect sizes in the female and male cohorts, respectively, and \(se_{f}\) and \(se_{m}\) are their standard errors. Significant sex differences were identified using a Bonferroni-corrected \(\alpha _{diff}\) based on M total number of tests, such that \(\alpha _{diff} = \frac{0.05}{M}\).
-
Filtering-First Approach: associations significant across both sexes were filtered first using the following formula
$$\begin{aligned} Z_{overall} = \frac{\frac{\beta _{f} }{se^2_{f} } + \frac{\beta _{m} }{se^2_{m} } }{\sqrt{ \frac{1}{se^2_{f} } + \frac{1}{se^2_{m} } } } \end{aligned}$$(2)Associations with \(p_{overall} < 10^{-5}\) were retained for sex difference testing using formula 1. A Bonferroni-corrected \(\alpha _{diff}\) was applied based on N number of filtered tests, such that \(\alpha _{diff} = \frac{0.05}{N}\).
Both approaches were employed to capture different types of sex differences, providing a comprehensive evaluation. Specifically, the full evaluation approach is better suited to detect qualitative sex differences, whereas the filtering-first approach is better suited to detect quantitative and pure sex differences26. Differences significant by either approach were classified into pure, quantitative, or qualitative categories.
Age stratification
To assess the robustness of our findings and account for potential confounding effects of hormonal changes across the lifespan, we replicated the analysis by excluding participants 46 years or older. We retained 10,149 participants, with sample sizes across cohorts of \(N_{df}=2650; N_{dm}=2248; N_{rf}=2822; N_{rm}=2429\). This exclusion criterion removes the influence of age-related hormonal transitions on the observed associations between environmental exposures and health outcomes.
Results
We conducted 15,999 association tests in each of the four NHANES cohorts: discovery females, discovery males, replication females, and replication males. For further details on the sample sizes of each cohort, please refer to the “Materials and methods” section. The number of converged tests varied slightly across cohorts because some tests had fewer than 200 complete observations (between 15,470 in the replication males cohort and 15,994 in the discovery females and discovery males cohorts). From the successful tests, 15,466 exposure-phenotype associations converged across all cohorts and were used to estimate sex differences. We identified 119 significant sex-specific associations, of which 49 were classified as pure, 45 as quantitative, and 25 as qualitative.
Among the 58 phenotypes evaluated, 35 showed sex-specific associations with at least one exposure. Serum albumin levels had the highest number of sex-specific associations, with 30 different exposures, including smoking-related exposures (e.g., blood cotinine levels, number of cigarettes smoked daily, and whether anyone smokes in the household), nutrients (e.g., folate, vitamins A, D, and E), supplements (e.g., folic acid, calcium, vitamin C), and heavy metals and volatile compounds. Other phenotypes with notable associations included red cell count and C-reactive protein levels, which had sex-specific associations with heavy metals like cadmium and lead, and volatile compounds such as ethylbenzene and toluene (Figs. 1, 2).

Miami Plot from PheEWAS results stratified by sex. The Y axis shows the -log of the p-value, and the X axis is sorted by exposure categories. Significant sex differences are highlighted in color, and categorized as pure, quantitative, and qualitative sex differences. Relevant exposure-phenotype associations discussed in the manuscript are annotated.
Of the 272 exposures evaluated, 53 had sex-specific associations with at least one phenotype. Exposures to heavy metals (e.g., lead and cadmium), nutrients (e.g., vitamins A and E, lutein and zeaxanthin), and smoking behaviors were most frequently associated with phenotypes such as serum albumin, C-reactive protein, and red cell count. Lead exposure, for example, was associated with 11 different phenotypes, underscoring its widespread impact on various clinically relevant measurements (Figs. 1, 2). Supplementary Table 1 shows the complete set of results in more detail.

Circos plot of significant exposure-phenotype associations divided by sex and type of sex difference. In each circos plot, exposures are in the upper section and phenotypes in the lower section of the circle. The presence of a line connecting an exposure and phenotype indicates a significant association. Red lines indicate a negative association and blue lines indicate a positive association. The width of the line indicates the effect size, with greater width indicating a greater absolute effect size.
Pure sex differences
We identified 53 pure sex-specific associations, with a slight bias toward males. In females, exposures in pure associations were primarily heavy metals, food component recall, nutrients, and volatile compounds, associated with phenotypes like red cell count, lymphocyte percent, albumin, HDL cholesterol, and homocysteine. For example, blood levels of the volatile compounds ethylbenzene (\(\beta _{f}=0.096, \beta _{m}=-0.020, P_{diff}=1.53E-05\)) and toluene (\(\beta _{f}=0.115, \beta _{m}=-0.015, P_{diff}=3.91E-06\)) were both associated with red cell counts in females. In contrast, lead was associated with albumin (\(\beta _{f}=0.084, \beta _{m}=-0.028, P_{diff}=4.31E-09\)), creatinine (\(\beta _{f}=0.076, \beta _{m}=-0.005, P_{diff}=1.96E-06\)), and sodium levels (\(\beta _{f}=0.07, \beta _{m}=-0.024, P_{diff}=4.49E-06\)). In males, exposures in pure associations were often categorized as nutrients, smoking behavior, and supplement use, with albumin showing associations with 17 different exposures (Figs. 2, 3; Table 2).
Nineteen pure associations involved smoking-related exposures. For example, cotinine levels were associated with albumin levels (\(\beta _{f}=0.005, \beta _{m}=-0.089, P_{diff}=2.36E-13\)) and osmolality (\(\beta _{f}=-0.015, \beta _{m}=-0.086, P_{diff}=8.16E-06\)) in males and with red cell count (\(\beta _{f}=0.074, \beta _{m}=-0.006, P_{diff}=3.9E-06\)) in females. Similarly, “Does anyone smoke in home?” was associated with albumin levels (\(\beta _{f}=-0.020, \beta _{m}=-0.179; P_{diff}=0.1E-06\)) in males and with HDL cholesterol (\(\beta _{f}=-0.280, \beta _{m}=-0.051, P_{diff}=3.38E-06\)) and red cell count (\(\beta _{f}=0.186, \beta _{m}=0.002, P_{diff}=4.52E-06\)) in females. Two of the ten survey questions related to smoking behavior were positively associated with homocysteine levels in females. In contrast, seven were associated with albumin and one with C-reactive protein in males (Fig. 3).

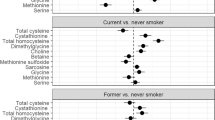
Forest plot showing the effect sizes and 95% confidence intervals in males and females. Exposures are defined on the left side and phenotypes on the right. Plots are divided into the three sex difference categories of pure, quantitative, and qualitative.
Quantitative sex differences
Forty-five quantitative sex-specific associations were identified, with greater effect sizes observed more frequently in males. Notably, heavy metal exposures like cadmium had greater effect on males on phenotypes like monocyte number (\(\beta _{f}=0.092, \beta _{m}=0.166, P_{diff}=7.48E-06\)), segmented neutrophils number (\(\beta _{f}=0.111, \beta _{m}=0.206, P_{diff}=2.2E-08\)), C-reactive protein level (\(\beta _{f}=0.045, \beta _{m}=0.144, P_{diff}=6.01E-09\)), mean cell hemoglobin level (\(\beta _{f}=0.047, \beta _{m}=0.135, P_{diff}=1.01E-09\)), mean cell volume (\(\beta _{f}=0.057, \beta _{m}=0.145, P_{diff}=1.27E-10\)), and white blood cell count (\(\beta _{f}=0.151, \beta _{m}=0.252, P_{diff}=9.7E-10\)); while in females it had greater effect on red cell count (\(\beta _{f}=0.127, \beta _{m}=0.027, P_{diff}=6.97E-11\)). On the other hand, lead exposure had greater effect on females on bone alkaline phosphatase level (\(\beta _{f}=0.233, \beta _{m}=0.049, P_{diff}=5.87E-14\)), homocysteine level (\(\beta _{f}=0.210, \beta _{m}=0.130, P_{diff}=5.17E-06\)), red cell count (\(\beta _{f}=0.190, \beta _{m}=0.071, P_{diff}=1.1E-09\)), and alkaline phosphatase level (\(\beta _{f}=0.193, \beta _{m}=0.064, P_{diff}=7.9E-12\)) (Figs. 2, 3; Table 3).
Smoking-related exposures, including cotinine levels, “Does anyone smoke in home?”, and “Current or Past Cigarette Smoker?” had greater positive effects on hematocrit in females. Similarly, associations between current or past cigarette smoking and hemoglobin level (\(\beta _{f}=0.429, \beta _{m}=0.236, P_{diff}=1.25E-06\)) and between the average number of cigarettes smoked per day during the past 30 days and homocysteine level (\(\beta _{f}=0.154, \beta _{m}=0.038, P_{diff}=2.71E-06\)) had greater effects in females. Conversely, all other quantitative associations between smoking-related exposures and bilirubin level, creatinine level, segmented neutrophils number, mean cell hemoglobin level, and white blood cell count had greater effects in males (Fig. 3).
Quantitative associations involving serum albumin, triglyceride, and GGT levels tended to have larger effects in males. For example, the associations between g-tocopherol and GGT level (\(\beta _{f}=0.066, \beta _{m}=0.129, P_{diff}=2.08E-05\)), g-tocopherol and triglyceride level (\(\beta _{f}=0.20, \beta _{m}=0.319, P_{diff}=1.35E-10\)), retinyl palmitate and triglyceride level (\(\beta _{f}=0.273, \beta _{m}=0.394, P_{diff}=7.65E-11\)), vitamin A and albumin level (\(\beta _{f}=0.145, \beta _{m}=0.258, P_{diff}=8.65E-11\)), and vitamin E and GGT level (\(\beta _{f}=0.032, \beta _{m}=0.145, P_{diff}=4.3E-07\)) had greater effects sizes in males. Conversely, associations with homocysteine and urine albumin tended to have greater effects in females than in males. For example, the associations between iron supplement use and homocysteine level (\(\beta _{f}=-0.127, \beta _{m}=-0.064, P_{diff}=1.78E-07\)) and between cesium level in urine and urine albumin level (\(\beta _{f}=0.504, \beta _{m}=0.362, P_{diff}=2.74E-09\)) had greater effect sizes in females.
Qualitative sex differences
Twenty-five qualitative sex differences were identified, mostly involving nutrient exposure, food component recall, and heavy metals. Exposures to lead, lutein and zeaxanthin, retinyl palmitate, and vitamin A were associated with more than one phenotype, whereas the phenotypes albumin, C-reactive protein, and lymphocyte percent were associated with more than one exposure. Notably, various folate and iron measurements were negatively associated with albumin levels in females and positively associated in males (Fig. 3). Moreover, lead exposure was differentially associated with osmolality (\(\beta _{f}=0.044, \beta _{m}=-0.061, P_{diff}=5.91E-08\)), bilirubin levels (\(\beta _{f}=0.068, \beta _{m}=-0.029, P_{diff}=6.11E-07\)), and C-reactive protein levels (\(\beta _{f}=-0.075, \beta _{m}=0.049, P_{diff}=8.48E-10\)) (Figs. 2, 3; Table 4).
Age stratification
When analyzing participants younger than 46, we identified 107 significant sex-specific associations: 43 were classified as qualitative, 27 as quantitative, and 37 as pure. Supplementary Table 2 contains the complete set of results for the young cohort. We identified 54 exposure-phenotype pairs replicated from the entire cohort, 34 of which showed the same type of sex difference classification, and 20 were classified differently. Notable examples of replicated findings with the same sex difference classification were the effects of cadmium on segmented neutrophils number (\(\beta _{f}=0.11, \beta _{m}=0.20, P_{diff}=1.18E-05\)), C-reactive protein (\(\beta _{f}=0.03, \beta _{m}=0.12, P_{diff}=4.10E-06\)), mean cell volume (\(\beta _{f}=0.05, \beta _{m}=0.14, P_{diff}=5.45E-06\)), and albumin (\(\beta _{f}=-0.002, \beta _{m}=-0.08, P_{diff}=2.47E-06\)), and the effect of smoking behavior (number of cigarettes smoked per day now and average number of cigarettes per day during past 30 days) and lead on homocysteine (\(\beta _{f}=0.21, \beta _{m}=0.03, P_{diff}=3.06E-06; \beta _{f}=0.20, \beta _{m}=0.05, P_{diff}=2.02E-05; \beta _{f}=0.23, \beta _{m}=0.12, P_{diff}=7.22E-06\)). Albumin also showed consistent results, specifically in its association with lead, cadmium, and smoking behavior (current or past cigarette smoker)(\(\beta _{f}=0.10, \beta _{m}=-0.02, P_{diff}=1.88E-07; \beta _{f}=0.002, \beta _{m}=-0.08, P_{diff}=2.47E-06; \beta _{f}=0.04, \beta _{m}=-0.17, P_{diff}=1.65E-07\)).
Even though 54 results were replicated in the younger cohort, 20 had different sex difference classifications. Notable examples were the associations of cotinine with red cell count (\(\beta _{f}=0.053, \beta _{m}=-0.04, P_{diff}=2.28E-05\)) and albumin (\(\beta _{f}= 0.03, \beta _{m}=-0.08, P_{diff}=3.38E-10\)) which were classified as pure sex differences in the entire cohort, but as qualitative in the young cohort. Similarly, the association between smoking behavior (number of days smoked cigarettes during the past 30 days) and albumin (\(\beta _{f}=0.04, \beta _{m}=-0.10, P_{diff}=1.65E-05\)) was classified as pure in the entire cohort, but qualitative in the young cohort.
On the other hand, we identified 53 novel exposure-phenotype pairs compared to the entire cohort. Of these, 12 associations were classified as quantitative, 22 as qualitative, and 19 as pure. Notable examples were the association between the FTC nicotine and tar content of the participants’ preferred cigarette brand and smoking behavior (how many years smoked this amount) with homocysteine (\(\beta _{f}=0.18, \beta _{m}=0.03, P_{diff}=5.44E-06; \beta _{f}=0.18, \beta _{m}=0.03, P_{diff}=2.54E-06\)), which showed a significant association only in females. Similarly, FTC carbon monoxide content of participants’ preferred cigarette brand, cotinine, and smoking family (does anyone smoke in home?) were positively associated with homocysteine across sexes but with greater effect sizes in females (\(\beta _{f}=0.18, \beta _{m}=0.04, P_{diff}=1.42E-05; \beta _{f}=0.16, \beta _{m}=0.07, P_{diff}=2.40E-05; \beta _{f}=0.30, \beta _{m}=0.08, P_{diff}=8.17E-07\)).
Discussion
We conducted a PheEWAS to identify sex-specific associations between 58 phenotypes and 272 environmental exposures among more than 18,000 NHANES participants. Our study identified environmental exposures with sex-specific effects on several blood phenotypes. Our analysis’s high-throughput and agnostic nature provides avenues for further research into the biological, environmental, and mechanistic aspects of these sex differences. Furthermore, our study demonstrates the utility of using an explicit PheEWAS framework to target potential differences between sexes instead of evaluating sex differences as a complementary analysis.
We identified 119 exposure-phenotype associations that significantly differed between sexes, many of which were related to smoking behaviors, familial smoking, and cotinine levels. Tobacco smoke is a significant source of exposure to heavy metals, such as cadmium and lead34,35,36,37, and volatile compounds like benzene, toluene, ethylbenzene, and xylene38. Exposure to these substances can be interpreted as exposure to both active and passive tobacco smoke. Our findings indicate that the effects of heavy metals and volatile compounds on phenotypes, such as serum albumin, closely mirror the impacts of smoking behaviors, as reflected in cotinine levels and self-reported smoking information. For instance, cadmium exposure in males had a similar impact on albumin levels as direct measures of smoking, such as cotinine.
Previous studies have documented sex differences in the prevalence and health impacts of smoking39,40. Our research further supports these differences, showing that smoking-related exposures have distinct associations with various phenotypes in males and females. For example, smoking is associated with elevated homocysteine (Hcy) levels41, and smoking and elevated Hcy levels have been associated with increased risks of cardiovascular disease and COPD42,43,44,45. Although males generally have higher Hcy levels than females, smoking exacerbates Hcy levels more in females, potentially due to hormonal mechanisms, including estrogen’s role in methionine metabolism46. Therefore, females might be at greater risk of the harmful effects of elevated Hcy levels than males41,47, including cardiovascular disease3,48 and COPD4. Our study’s findings support sex differences in the effects of tobacco smoke exposure on Hcy. For example, the number of cigarettes currently smoked per day and the frequency of cigarette smoking during the past 30 days were positively associated with plasma Hcy levels only in females. Similarly, the average number of cigarettes smoked per day in the last 30 days had a greater effect on Hcy levels in females.
Smoking exposure has been linked to elevated levels of red blood cell populations, including hematocrit, hemoglobin, and red cell counts49,50. This increase is thought to result from carbon monoxide inhalation, which induces hypoxia and triggers a compensatory rise in hemoglobin, hematocrit, and red cell counts to maintain oxygen transport51,52,53. Our study found that smoking behavior, familial smoking, cotinine levels, and blood concentrations of cadmium, lead, ethylbenzene, and toluene were positively associated with hematocrit, hemoglobin, and red cell counts in females, consistent with prior research. However, to our knowledge, this study is the first to identify potential sex differences in the impact of tobacco smoke exposure on red blood cell populations.
On the other hand, tobacco smoke exposure significantly impacts inflammation and oxidative stress, primarily due to the presence of reactive oxygen species (ROS) that induce oxidative stress, leading to cellular apoptosis and senescence54. Typically, plasma antioxidants like albumin and bilirubin increase in response to oxidative stress as a protective mechanism55. However, studies have shown that smoking is associated with reduced levels of these antioxidants, even in a dose-dependent manner56,57,58,59,60,61,62,63. The excessive free radical production and extreme oxidative stress from smoking likely lead to the breakdown and depletion of these antioxidants, resulting in their lower levels64,65. Furthermore, smokers have also been found to exhibit elevated levels of inflammatory markers compared to non-smokers, including C-reactive protein (CRP), white blood cell count, and interleukin-662,66,67,68. Although the exact mechanisms are unclear, albumin levels tend to decrease in response to acute inflammation69. The combined oxidative stress and inflammatory responses to tobacco smoke exposure elevate the risk of chronic diseases such as cancer, COPD, and cardiovascular disease54,70.
In our study, smoking behavior, familial smoking, cotinine levels, and cadmium exposure were negatively associated with serum albumin levels in males but not in females. Additionally, smoking behavior, including the number of cigarettes smoked daily and the average number of cigarettes smoked daily over the past month, was negatively associated with bilirubin levels, with stronger effects observed in males. Moreover, smoking behavior and blood cadmium levels were positively associated with CRP levels and white blood cell counts, again with greater effect sizes in males. These findings align with previous research highlighting the role of tobacco smoke in promoting oxidative stress and inflammation. However, only a few studies have reported sex differences in the associations between tobacco smoke exposure and inflammatory markers or antioxidants56,71. Our findings suggest that males may experience a heightened inflammatory and oxidative stress response to tobacco smoke exposure compared to females. Notably, most observed differences were quantitative, indicating that these effects also occur in females but are less pronounced.
The findings from this study underscore the significant sex differences in the biological mechanisms underlying tobacco smoke exposure. These differences manifest in various processes, including inflammation, oxidative stress, hypoxia, and Hcy metabolism. Future research and prevention strategies must consider these sex-specific variations. For instance, methodological designs should go beyond merely controlling for sex and actively account for these differences. In this study, tobacco smoke exposure was assessed using multiple measures, including direct blood cotinine levels and self-reported smoking behavior. The consistent observation of sex differences across these varied metrics reinforces the robustness of our results. Going forward, researchers can leverage the extensive NHANES dataset to develop more detailed exposure metrics that distinguish between primary and secondary exposure and capture the duration and intensity of exposure.
We found that serum albumin levels seem more susceptible to environmental exposures in males than in females. Of the 22 pure or quantitative sex-specific associations involving serum albumin levels, 20 were exclusive to males or had a greater effect size in males. By contrast, associations involving serum Hcy levels tended to be specific to females. In all five pure or quantitative sex-specific associations involving serum Hcy, the effect was either exclusive to females or stronger in females than males. These results suggest that sex-specific mechanisms might underlie the metabolism of Hcy and serum albumin, implicating sex differences in methionine catabolism and inflammatory responses.
Our study identified three distinct types of sex differences in the associations between environmental exposures and phenotypes: pure, quantitative, and qualitative. Each type of difference has unique implications for understanding sex-specific environmental effects and developing targeted interventions. Pure sex differences occur when a significant association is observed in one sex but not in the other. This type of difference suggests that the biological mechanisms underlying the response to this exposure are either absent or not as pronounced in one sex. Pure sex differences often point to sex-specific biological pathways that may be influenced by factors such as sex hormones or genetic differences. Understanding these mechanisms can help identify potential targets for therapeutic interventions that are tailored to one sex. On the other hand, quantitative sex differences occur when an association is present in both sexes but with varying magnitudes of effect, suggesting that while both sexes are affected, the impact is greater in one sex. Quantitative differences highlight the need for sex-specific thresholds or guidelines in clinical practice. For example, our findings suggest that smoking exposure has a greater effect on Hcy levels in females, which can lead to more tailored interventions. Finally, qualitative sex differences occur when the direction of the association is opposite in males and females. Such opposite effects suggest fundamentally different biological responses to the same exposure in each sex, which have significant implications for tailored interventions and therapeutic guidance.
Of the 119 significant sex-specific associations identified in our PheEWAS, 94 were pure or quantitative, and only 25 were classified as qualitative. This favor toward quantitative and pure sex differences suggests that males and females tend to differ in the degree of associations but not in the direction of effects. Furthermore, quantitative and pure sex differences suggest associations with the same underlying mechanisms in males and females, whereas qualitative differences suggest associations with different mechanisms in males and females. Some differences, which are, in fact, quantitative, might have been misclassified as pure because of a lack of power to detect a significant association in one of the sexes. On the other hand, qualitative differences suggest completely different mechanisms or responses in each sex. The different underlying mechanisms of qualitative sex differences and pure or quantitative sex differences might also explain why qualitative differences were rarer and more heterogeneous than pure or quantitative differences. Pure and quantitative sex differences showed greater similarities than qualitative sex differences in the exposures and phenotypes involved, for example, smoking-related exposures. The observed bias can have implications for future research, particularly in suggesting experimental designs and analyses that privilege detecting differences in effect sizes between sexes. Nevertheless, the bias towards pure and quantitative sex differences might be due to the higher power to detect pure and quantitative sex differences at the expense of qualitative differences.
We replicated 54 exposure-phenotype associations using a younger cohort that retained roughly half of the participants. These replicated findings corroborated the results obtained in the entire cohort regarding the differential effects of tobacco smoke exposure between sexes. The non-replicated exposure-phenotype might be due to the lower sample sizes and, therefore, the reduced power to detect those differences. The unique exposure-phenotype associations that were present only in the young cohort might be due to age-specific differences, including differences in exposure rates in younger versus older participants. Nevertheless, our study did not rigorously test differences between the full and young cohorts, which is beyond the scope of our study. This requires a two-way interaction between sex and age, necessitating substantial sample sizes to estimate and detect significant differences. Therefore, these differences remain speculative, and comparisons between the full and young cohorts are only descriptive.
While this study provides valuable insights into sex-specific associations between environmental exposures and health outcomes, several limitations that could affect the interpretation of our findings must be acknowledged. One of the primary limitations of this study is the exclusion of participants with missing data on covariates, which was necessary to maintain the integrity and consistency of the dataset. While this approach helps ensure that all included participants have complete data for the variables under consideration, it may introduce selection bias, potentially affecting the study’s findings. In short, excluding participants with missing data can lead to a non-random sample that might not fully represent the broader population. This selection bias could manifest in several ways, including underestimating or overestimating associations, reduced generalizability, and losing statistical power. Future studies could employ several strategies to mitigate these potential biases, including multiple imputation techniques and sensitivity analyses.
PheEWAS involves testing thousands of associations simultaneously, which increases the risk of Type I errors (false positives). Although we applied the Bonferroni correction to account for multiple comparisons, a widely used method for controlling the risk of false positives, it is overly conservative, particularly in studies with many comparisons. This conservativeness can increase the risk of Type II errors (false negatives), where true associations may be overlooked because the adjusted p-value threshold is too stringent72. In the context of our study, this could result in missing potentially sex-specific associations between environmental exposures and phenotypes. Given the limitations of the Bonferroni correction, alternative methods such as False Discovery Rate (FDR) can be used in future studies that balance the risk of Type I and Type II errors more effectively but still may lead to some false discoveries73.
Another caveat to our study is that sex differences in the range of variation of the exposures might be observed as sex differences in the association between exposures and phenotypes. For example, if males have a minimal range of variation in a given exposure, there might not be enough variation to detect an association with a given phenotype. In contrast, if females have a greater range of variation in the exposure, it can reveal a positive association between the exposure and the phenotype. In such a case, a phenotype-exposure association would differ between males and females only because of the different degrees of exposure and not necessarily because of different underlying mechanisms. Future research might benefit from detecting significant sex differences in the distributions of the exposures and either removing those exposures or flagging them for potential manual inspection.
Although we identified several exposure-phenotype associations, because of the cross-sectional nature of the data, we can only determine correlations between exposures and phenotypes and not causality74. Furthermore, although we adjusted for several known confounders, residual confounding may still exist due to unmeasured or unknown factors. Finally, reverse causality remains an issue, as in EWAS more generally74. For example, several sex-different associations might be due to differential behaviors that men and women deploy in the face of similar events. In other words, individuals with pre-existing health conditions may alter their behaviors or environments in ways that influence their exposure levels. Such behavioral differences are not trivial in analyses of sex differences because studies have shown gender differences in health-related behaviors such as healthcare seeking and medication intake and adherence75,76,77. Therefore, our results cannot easily be ascribed simply to sex differences if we understand them solely based on biology.
Finally, the generalizability of our findings may be limited by the demographic characteristics of the NHANES sample, which, while representative of the U.S. population, may not capture the full diversity of global populations. Factors such as ethnicity and environmental exposures vary widely across different populations, and the associations observed in this study may not apply universally22.
Our study unveils novel insights into the sex-specific effects of environmental exposures on health outcomes, highlighting this research’s unique and significant contribution to the field. First, it underscores the need for a deeper understanding of biological mechanisms driving these differences. Identifying sex differences is the first step in discovering potential biological mechanisms that might include hormonal, genetic, and epigenetic influences. With a better understanding of these mechanisms, sex differences become a crude reflection of a more nuanced underlying biology. Second, our study underscores the pressing need for a precision medicine approach that not only relies on genetic background but also on low-throughput demographic information, such as sex, to assess differences in treatments, diagnoses, and prognoses, thereby providing a practical framework for healthcare professionals and policymakers. It also foregrounds the relevance of targeted public health policies. For example, public health policies might address the needs of diverse subgroups differently to mitigate risks produced by environmental exposures, such as tobacco smoke. Finally, future studies have the potential to address two crucial missing pieces in our study: longitudinal variation and multidimensional exposures and phenotypes, thereby paving the way for further significant advancements in this field. We have taken a more straightforward approach in our study by taking a snapshot of the effects of environmental exposures on endophenotypes, but differences in intensities, duration of exposures, and lifespan window can modulate these effects. Furthermore, multiple exposures can affect multiple phenotypes in non-linear and more complex ways.
Data availability
The datasets analysed during the current study are available in the DataDryad repository, under the following DOI: https://doi.org/10.1038/sdata.2016.96. All the code used during the current study are available in the Zenodo repository, under the following DOI: https://zenodo.org/doi/10.5281/zenodo.6483502.
References
Mauvais-Jarvis, F. et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 396, 565–582 (2020).
Klein, S. L. & Flanagan, K. L. Sex differences in immune responses. Nat. Rev. Immunol. 16, 626–638 (2016).
Regitz-Zagrosek, V. & Kararigas, G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol. Rev. 97, 1–37 (2017).
DeMeo, D. L. et al. Women manifest more severe COPD symptoms across the life course. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 3021–3029 (2018).
Mallampalli, M. P. et al. Role of environment and sex differences in the development of autoimmune diseases: A roundtable meeting report. J. Womens Health 22, 578–586 (2013).
Raghavan, D. & Jain, R. Increasing awareness of sex differences in airway diseases. Respirology 21, 449–459 (2015).
DeBolt, C. & Harris, D. The impact of social determinants of health on gender disparities within respiratory medicine. Clin. Chest Med. Gender Respir. Dis. 42, 407–415 (2021).
McHugh, M. .K., Symanski, E., Pompeii, L. .A. & Delclos, G. .L. Prevalence of asthma by industry and occupation in the U.S. working population. Am. J. Ind. Med. 53, 463–475 (2010).
Centers for Disease Control and Prevention (CDC). Annual smoking-attributable mortality, years of potential life lost, and economic costs—United States, 1995–1999. MMWR Morb. Mortal. Wkly. Rep. 51, 300–303 (2002).
Gan, W. Q., Man, S. P., Postma, D. S., Camp, P. & Sin, D. D. Female smokers beyond the perimenopausal period are at increased risk of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Respir. Res. 7, 52 (2006).
Pollard, K. M. Gender differences in autoimmunity associated with exposure to environmental factors. J. Autoimmun. 38, J177–J186 (2012) (Special Issue: Gender, Sex Hormones, Pregnancy and Autoimmunity).
Shannon, G. et al. Gender equality in science, medicine, and global health: Where are we at and why does it matter?. Lancet 393, 560–569 (2019).
Liu, L. Y., Schaub, M. A., Sirota, M. & Butte, A. J. Sex differences in disease risk from reported genome-wide association study findings. Hum. Genet. 131, 353–364 (2012).
Bush, W. S., Oetjens, M. T. & Crawford, D. C. Unravelling the human genome-phenome relationship using phenome-wide association studies. Nat. Rev. Genet. 17, 129–145 (2016).
Dumitrescu, L. et al. Sex differences in the genetic predictors of Alzheimer’s pathology. Brain 142, 2581–2589 (2019).
Hu, Y. et al. Rs34331204 regulates TSPAN13 expression and contributes to Alzheimer’s disease with sex differences. Brain 143, e95 (2020).
Ostrom, Q. T. et al. Sex-specific glioma genome-wide association study identifies new risk locus at 3p21.31 in females, and finds sex-differences in risk at 8q24.21. Sci. Rep. 8, 7352 (2018).
Winkler, T. W. et al. The influence of age and sex on genetic associations with adult body size and shape: A large-scale genome-wide interaction study. PLoS Genet. 11, e1005378 (2015).
Rask-Andersen, M., Karlsson, T., Ek, W. E. & Johansson, Å. Genome-wide association study of body fat distribution identifies adiposity loci and sex-specific genetic effects. Nat. Commun. 10, 339 (2019).
Choquet, H. et al. A large multiethnic GWAS meta-analysis of cataract identifies new risk loci and sex-specific effects. Nat. Commun. 12, 3595 (2021).
Zheng, Y. et al. Design and methodology challenges of environment-wide association studies: A systematic review. Environ. Res. 183, 109275 (2020).
Patel, C. J., Bhattacharya, J. & Butte, A. J. An environment-wide association study (EWAS) on type 2 diabetes mellitus. PLoS ONE 5, e10746 (2010).
Hall, M. A. et al. Environment-wide association study (EWAS) for type 2 diabetes in the Marshfield Personalized Medicine Research Project Biobank. Biocomputing 2014, 200–211 (2013).
Zhuang, X. et al. Toward a panoramic perspective of the association between environmental factors and cardiovascular disease: An environment-wide association study from National Health and Nutrition Examination Survey 1999–2014. Environ. Int. 118, 146–153 (2018).
McGinnis, D. P., Brownstein, J. S. & Patel, C. J. Environment-wide association study of blood pressure in the National Health and Nutrition Examination Survey (1999–2012). Sci. Rep. 6, 30373 (2016).
Winkler, T. W. et al. Approaches to detect genetic effects that differ between two strata in genome-wide meta-analyses: Recommendations based on a systematic evaluation. PLoS ONE 12, e0181038 (2017).
Patel, C. J. et al. A database of human exposomes and phenomes from the US National Health and Nutrition Examination Survey. Sci. Data 3, 160096 (2016).
Patel, C. J. et al. Data from: A database of human exposomes and phenomes from the US National Health and Nutrition Examination Survey 2016 (2020).
Hall, M. A. et al. Detection of pleiotropy through a phenome-wide association study (PheWAS) of epidemiologic data as part of the Environmental Architecture for Genes Linked to Environment (EAGLE) study. PLoS Genet. 10, e1004678 (2014).
Lucas, A. M. et al. CLARITE facilitates the quality control and analysis process for EWAS of metabolic-related traits. Front. Genet. 10, 1240 (2019).
West, R. M. Best practice in statistics: The use of log transformation. Ann. Clin. Biochem. 59, 162–165 (2022).
Archer, K. J., Dumur, C. I. & Ramakrishnan, V. Graphical technique for identifying a monotonic variance stabilizing transformation for absolute gene intensity signals. BMC Bioinform. 5, 60 (2004).
Willer, C. J., Li, Y. & Abecasis, G. R. METAL: Fast and efficient meta-analysis of genomewide association scans. Bioinformatics 26, 2190–2191 (2010).
Nordberg, G. F., Fowler, B. A. & Nordberg, M. Handbook on the Toxicology of Metals (Academic Press, 2014). ISBN: 978-0-12-397339-9.
Pappas, R. S. Toxic elements in tobacco and in cigarette smoke: Inflammation and sensitization. Metallomics 3, 1181–1198 (2011).
Apostolou, A. et al. Secondhand tobacco smoke: A source of lead exposure in US children and adolescents. Am. J. Public Health 102, 714–722 (2012).
Mannino, D. M., Homa, D. M., Matte, T. & Hernandez-Avila, M. Active and passive smoking and blood lead levels in U.S. adults: Data from the Third National Health and Nutrition Examination Survey. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 7, 557–564 (2005).
Chambers, D. M., Ocariz, J. M., McGuirk, M. F. & Blount, B. C. Impact of cigarette smoking on volatile organic compound (VOC) blood levels in the U.S. population: NHANES 2003–2004. Environ. Int. 37, 1321–1328 (2011).
McHugh, R. K., Votaw, V. R., Sugarman, D. E. & Greenfield, S. F. Sex and gender differences in substance use disorders. Clin. Psychol. Rev. Gender Mental Health 66, 12–23 (2018).
Appelman, Y., van Rijn, B. B., ten Haaf, M. E., Boersma, E. & Peters, S. A. E. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis 241, 211–218 (2015).
Nygård, O., Refsum, H., Ueland, P. M. & Vollset, S. E. Major lifestyle determinants of plasma total homocysteine distribution: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 67, 263–270 (1998).
O’Callaghan, P., Meleady, R., Fitzgerald, T., Graham, I. & European COMAC Group. Smoking and plasma homocysteine. Eur. Heart J. 23, 1580–1586 (2002).
Chaudhary, D., Sharma, N. & Senapati, S. Serum homocysteine could be used as a predictive marker for chronic obstructive pulmonary disease: A meta-analysis. Front. Public Health 7, 69 (2019).
Forey, B. A., Thornton, A. J. & Lee, P. N. Systematic review with meta-analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC Pulm. Med. 11, 36 (2011).
Chrysant, S. G. & Chrysant, G. S. The current status of homocysteine as a risk factor for cardiovascular disease: A mini review. Expert Rev. Cardiovasc. Ther. 16, 559–565 (2018).
Finkelstein, J. D. & Martin, J. J. Homocysteine. Int. J. Biochem. Cell Biol. 32, 385–389 (2000).
Stanisławska-Sachadyn, A. et al. Evidence for sex differences in the determinants of homocysteine concentrations. Mol. Genet. Metab. 93, 355–362 (2008).
Huxley, R. R. & Woodward, M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: A systematic review and meta-analysis of prospective cohort studies. Lancet (London, England) 378, 1297–1305 (2011).
Van Tiel, E. D. et al. Quitting smoking may restore hematological characteristics within five years. Ann. Epidemiol. 12, 378–388 (2002).
Malenica, M. et al. Effect of cigarette smoking on haematological parameters in healthy population. Med. Arch. 71, 132–136 (2017).
Helman, N. & Rubenstein, L. S. The effects of age, sex, and smoking on erythrocytes and leukocytes. Am. J. Clin. Pathol. 63, 35–44 (1975).
Fricker, M. et al. Chronic cigarette smoke exposure induces systemic hypoxia that drives intestinal dysfunction. JCI Insight 3, 1–19 (2018).
Pedersen, K. M. et al. Smoking and increased white and red blood cells. Arterioscler. Thromb. Vasc. Biol. 39, 965–977 (2019).
Caliri, A. W., Tommasi, S. & Besaratinia, A. Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer. Mutat. Res. Rev. Mutat. Res. 787, 108365 (2021).
Amir Aslani, B. & Ghobadi, S. Studies on oxidants and antioxidants with a brief glance at their relevance to the immune system. Life Sci. 146, 163–173 (2016).
Hoydonck, P. G. V., Temme, E. H. & Schouten, E. G. Serum bilirubin concentration in a Belgian population: The association with smoking status and type of cigarettes. Int. J. Epidemiol. 30, 1465–1472 (2001).
Schwertner, H. A. Association of smoking and low serum bilirubin antioxidant concentrations. Atherosclerosis 136, 383–387 (1998).
Jo, J., Kimm, H., Yun, J. E., Lee, K. J. & Jee, S. H. Cigarette smoking and serum bilirubin subtypes in healthy Korean men: The Korea Medical Institute Study. J. Prev. Med. Public Health 45, 105–112 (2012).
Kodal, J. B. et al. Smoking reduces plasma bilirubin: Observational and genetic analyses in the Copenhagen General Population Study. Nicotine Tob. Res. 22, 104–110 (2020).
Nelson, J. J. et al. Serum albumin level as a predictor of incident coronary heart disease: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 151, 468–477 (2000).
Shaper, A. G., Wannamethee, S. G. & Whincup, P. H. Serum albumin and risk of stroke, coronary heart disease, and mortality: The role of cigarette smoking. J. Clin. Epidemiol. 57, 195–202 (2004).
Bakhru, A. & Erlinger, T. P. Smoking cessation and cardiovascular disease risk factors: Results from the Third National Health and Nutrition Examination Survey. PLoS Med. 2, e160 (2005).
Jang, E. S. et al. Effects of coffee, smoking, and alcohol on liver function tests: A comprehensive cross-sectional study. BMC Gastroenterol. 12, 1–12 (2012).
Zhou, J. F. et al. Effects of cigarette smoking and smoking cessation on plasma constituents and enzyme activities related to oxidative stress. Biomed. Environ. Sci. 13, 44–55 (2000).
Yildiz, L., Kayaoğlu, N. & Aksoy, H. The changes of superoxide dismutase, catalase and glutathione peroxidase activities in erythrocytes of active and passive smokers. Clin. Chem. Lab. Med. 40, 612–615 (2002).
Sopori, M. Effects of cigarette smoke on the immune system. Nat. Rev. Immunol. 2, 372–377 (2002).
Stämpfli, M. R. & Anderson, G. P. How cigarette smoke skews immune responses to promote infection, lung disease and cancer. Nat. Rev. Immunol. 9, 377–384 (2009).
Wannamethee, S. G. et al. Associations between cigarette smoking, pipe/cigar smoking, and smoking cessation, and haemostatic and inflammatory markers for cardiovascular disease. Eur. Heart J. 26, 1765–1773 (2005).
Chien, S.-C., Chen, C.-Y., Lin, C.-F. & Yeh, H.-I. Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark. Res. 5, 31 (2017).
Kotlyarov, S. The role of smoking in the mechanisms of development of chronic obstructive pulmonary disease and atherosclerosis. Int. J. Mol. Sci. 24, 8725 (2023).
Fröhlich, M. et al. Independent association of various smoking characteristics with markers of systemic inflammation in men: Results from a Representative Sample of the General Population (MONICA Augsburg Survey 1994/95). Eur. Heart J. 24, 1365–1372 (2003).
Armstrong, R. A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 34, 502–508 (2014).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 57, 289–300 (1995).
Patel, C. J. & Ioannidis, J. P. A. Studying the elusive environment in large scale. JAMA 311, 2173–2174 (2014).
Thompson, A. E. et al. The influence of gender and other patient characteristics on health care-seeking behaviour: A QUALICOPC study. BMC Fam. Pract. 17, 1–7 (2016).
Chen, S.-L., Lee, W.-L., Liang, T. & Liao, I.-C. Factors associated with gender differences in medication adherence: A longitudinal study. J. Adv. Nurs. 70, 2031–2040 (2014).
Manteuffel, M. et al. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J. Womens Health 23, 112–119 (2014).
Acknowledgements
We thank the editor and two anonymous reviewers for their comments and feedback that have improve this manuscript considerably.
Author information
Authors and Affiliations
Contributions
T.G.Z., M.A.H., N.E.P., D.K., and L.S. contributed to the conception and design of the study. N.E.P. and T.G.Z. performed the cleaning of the databases and the analysis. T.G.Z. wrote the first draft of the manuscript. All authors contributed to the revision of the manuscript, and read and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
González Zarzar, T., Palmiero, N.E., Kim, D. et al. Differential effects of environmental exposures on clinically relevant endophenotypes between sexes. Sci Rep 14, 21453 (2024). https://doi.org/10.1038/s41598-024-72180-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-72180-x
