
Abstract
Bronchiolitis is a significant factor contributing to bronchial asthma in infants and young children. After treatment, recurrent wheezing symptoms often occur, especially in children with atopic constitution, who tend to have more severe conditions and poorer prognosis. Therefore, exploring the prognostic value of total serum immunoglobulin E (tIgE) and fractional exhaled nitric oxide (FeNO) levels in children with atopic constitution who suffer from bronchiolitis is of great significance. A total of 260 children with bronchiolitis admitted to our hospital from October 2020 to June 2022 were regarded as the research subjects with prospective study, according to whether the children had atopic constitution, they were grouped into non atopic constitution group (n = 156) and atopic constitution group (n = 104); after 6 months of treatment, children with atopic constitution were grouped into a good prognosis group (n = 58) and a poor prognosis group (n = 46) based on their prognosis; in addition, 260 healthy children who underwent physical examination and had clinical data consistent with those of children with bronchiolitis were regarded as the reference group. The serum tIgE and FeNO levels of each group were compared; multivariate Logistic regression was applied to analyze the prognostic factors of children with atopic constitution bronchiolitis; ROC curve was applied to analyze the predictive value of tIgE and FeNO levels after treatment for the prognosis of children with atopic constitution bronchiolitis. The tIgE levels in the control group, non-atopic group, and atopic group [(123.54 ± 29.62) IU/mL, (245.71 ± 30.59) IU/mL, (316.46 ± 31.78) IU/mL, respectively] increased sequentially, with statistically significant differences (F = 1766.954, P = 0.000). The FeNO levels in the control group, non-atopic group, and atopic group [(8.36 ± 3.57) ppb, (15.28 ± 3.69) ppb, (19.84 ± 3.58) ppb, respectively] also increased sequentially, with statistically significant differences (F = 765.622, P = 0.000). The tIgE, FeNO, proportion of patients with asthma family history, and proportion of patients with allergic family history in the poor prognosis group were obviously higher than those in the good prognosis group (P < 0.05). Multivariate Logistic regression analysis showed that family history of asthma, family history of allergies, tIgE, and FeNO were influencing factors for the prognosis of children with atopic bronchiolitis (P < 0.05). The AUC of the combination of tIgE and FeNO in predicting the prognosis of children with atopic constitutional bronchiolitis was 0.910, with a sensitivity of 78.26% and a specificity of 93.10%, which was superior to the independent prediction of tIgE and FeNO (Zcombined detection−tIgE = 2.442, Zcombined detection−FeNO = 3.080, P = 0.015, 0.002). The levels of tIgE and FeNO in children with atopic constitution bronchiolitis are obviously increased, and the combination of the two has high predictive value for the prognosis of atopic constitution bronchiolitis.
Similar content being viewed by others


Introduction
Bronchiolitis is a viral lower respiratory tract infection common in infants under the age of 2, causing inflammation and edema in the small airways and leading to symptoms such as low fever, rapid breathing, chest retraction, reduced oral intake, accompanied by bilateral lung wet rales, wheezing, etc.1. Bronchiolitis has brought a huge clinical burden. It is estimated that globally, it causes more than 30 million cases in children under 5 years old every year, with over 3 million hospitalizations2. Bronchiolitis is an important factor leading to bronchial asthma in infants and young children, and after treatment, there is a tendency for recurrent wheezing symptoms, especially in children with atopic constitutions, with approximately 30–40% of hospitalized severe bronchiolitis patients developing asthma during childhood3. Therefore, finding serum biomarkers related to the prognosis of children with atopic constitution bronchiolitis, timely adjusting treatment plans, and improving prognosis are of great significance. Immunoglobulin E (IgE) is an important mediator in the occurrence and maintenance of allergic inflammation, expressed on tissue mast cells, blood eosinophils, airway smooth muscle cells, antigen-presenting cells, etc., and is widely used to assess the atopic state4. Exhaled nitric oxide (FeNO) is mainly derived from bronchial epithelium, produced in large quantities by inducible nitric oxide synthase, and is a biomarker of airway hyperresponsiveness and eosinophilic inflammation, also related to the severity of the condition5. Serum tIgE and FeNO have good application in children with bronchiolitis, but the prognostic value of tIgE and FeNO combined with atopic constitution in children with bronchiolitis is still unclear. Therefore, this study analyzes the relationship between the expression levels of IgE and FeNO in the serum of children with atopic constitution bronchiolitis and patient prognosis by detecting them, providing a reference for improving the prognosis of children.
Research subjects and methods
Research subjects
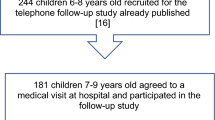
260 children with bronchiolitis treated in our hospital from October 2020 to June 2022 were selected as research subjects with prospective study. According to the diagnostic criteria for atopic constitution6, those with a personal history of allergic diseases,elevated serum tIgE, or positive specific IgE indicates atopic constitution were considered to have atopic constitution and were divided into non-atopic constitution group (n = 156) and atopic constitution group (n = 104). Six months after treatment, children with atopic constitution were followed up at outpatient clinics once a month to monitor the occurrence of wheezing. According to whether wheezing recurred, they were divided into good prognosis group (The condition is under control, and there has been no recurrence of asthma, n = 58) and poor prognosis group (The condition is not under control, and asthma has recurred, n = 46). Inclusion criteria: (1) Meet the diagnostic criteria for bronchiolitis7; (2) Age 36 days to 24 months; (3) The child's guardian is well informed about the content of this research and voluntarily signs the consent form. Exclusion criteria: (1) Children with a history of bronchiolitis; (2) Children who used immunosuppressor or steroids in the period before enrollment; (3) Children with respiratory malformations; (4) Children with incomplete clinical data. This study was reviewed and approved by the Ethics Committee of our hospital and followed the Declaration of Helsinki by the World Medical Association. In addition, 260 healthy children who underwent physical examinations in the same period with clinical data consistent with those of children with bronchiolitis were selected as the control group. The control group included 134 males and 126 females, aged (11.48 ± 2.67) months. There were 76 males and 80 females, aged (11.72 ± 2.74) months in the non-atopic constitution group. In the atopic constitution group, 55 males and 49 females were (12.05 ± 2.89) months old. There was no significant difference in age and sex among the three groups, which was comparable. The case flow chart is shown in Fig. 1.

Case Flow Chart.
Methods
tIgE level detection
The morning after admission for children with bronchiolitis and on the day of physical examination for the control group, about 3–5 mL of venous blood was collected, centrifuged at a radius of 12 cm for 10 min, and stored in a − 80 °C freezer for later testing. Serum tIgE levels were detected by chemiluminescence.
FeNO level detection
After receiving routine treatments such as anti infection, oxygen therapy, and cough relief to control the stability of the condition,FeNO levels in children with bronchiolitis and the control group were detected using a FeNO detector. Food and water were prohibited for 3 h before the test, and strenuous exercise was avoided for 1 h before the test. In a state of sedation for infants, after guiding the child to expel the air from their lungs, immediately have them tightly cover the filter device with their mouth, exhale deeply, and breathe steadily,connected tightly to the gas sampling bag, and breathing was conducted for 30–60 s until the bag was half full. Then the sample bag was sealed, and the collected gas was tested within 4 h. A dry box was used to remove moisture and connected to the main analyzer, the level of FeNO was measured, and the machine automatically read the value, with results expressed in parts per billion (ppb).
Statistical methods
Data were statistically analyzed using SPSS 25.0 software. Quantitative data such as tIgE and FeNO, indicators that do not conform to a normal distribution are converted logarithmically to approximate a normal distribution (to make the results concise, the pre transformation data is still used), were described as (\(\overline{x}\) ± \(s\)), and comparisons between two groups were made using independent samples t-tests. One-way ANOVA was used for comparisons of quantitative data among multiple groups, with further pairwise comparisons using Snk-q tests. Count data such as family history of asthma and allergy were expressed as cases (n) and percentages (%), and \(\chi^{2}\) chi-square tests were used for group comparisons. Multifactorial logistic regression analysis was used to analyze factors affecting the prognosis of children with atopic constitution bronchiolitis. ROC curve analysis was performed to evaluate the predictive value of post-treatment tIgE and FeNO levels for the prognosis of children with atopic constitution bronchiolitis, with P < 0.05 indicating statistically significant differences.
Results
Comparison of tIgE and FeNO levels among three groups
The tIgE levels in the control group, non-atopic group, and atopic group [(123.54 ± 29.62) IU/mL, (245.71 ± 30.59) IU/mL, (316.46 ± 31.78) IU/mL, respectively] increased sequentially, with statistically significant differences (F = 1766.954, P = 0.000). The FeNO levels in the control group, non-atopic group, and atopic group [(8.36 ± 3.57) ppb, (15.28 ± 3.69) ppb, (19.84 ± 3.58) ppb, respectively] also increased sequentially, with statistically significant differences (F = 765.622, P = 0.000). See Fig. 2.

Comparison of tIgE and FeNO levels among the three groups (\(\overline{x}\) ± \(s\)). Note: Compared with the control group, aP < 0.05; compared with the non-atopic constitution group, bP < 0.05.
Univariate analysis of prognosis in children with atopic constitution bronchiolitis
The proportion of patients with a history of asthma, a history of allergies, and levels of tIgE and FeNO in the poor prognosis group were significantly higher than those in the good prognosis group (P < 0.05); there were no significant differences between the two groups in age, gender, BMI, or duration of illness (P > 0.05). See Table 1.
Multifactorial logistic regression analysis of factors influencing the prognosis of children with atopic constitution bronchiolitis
With the prognosis of children with atopic constitution bronchiolitis as the dependent variable (poor prognosis = 1, good prognosis = 0), and a history of asthma (yes = 1, no = 0), a history of allergies (yes = 1, no = 0), tIgE (continuous variable), and FeNO (continuous variable) as independent variables, multifactorial logistic regression analysis showed that a history of asthma, a history of allergies, tIgE, and FeNO were influencing factors for the prognosis of children with atopic constitution bronchiolitis (P < 0.05). See Table 2.
Predictive value of serum tIgE and FeNO levels for the prognosis of children with atopic constitution bronchiolitis
The area under the curve (AUC) for serum tIgE in predicting the prognosis of children with atopic constitution bronchiolitis was 0.826, and the AUC for serum FeNO was 0.798. The combined prediction for the prognosis of children with atopic constitution bronchiolitis had an AUC of 0.910. The combined prediction was superior to that of tIgE or FeNO alone (Zcombined test−tIgE = 2.442, Zcombined test−FeNO = 3.080, P = 0.015, 0.002). See Table 3 and Fig. 3.

ROC curves for predicting the prognosis of children with atopic constitution bronchiolitis based on serum IgE and FeNO levels.
Discussion
Bronchiolitis is an inflammation of the small bronchioles and their surrounding tissues induced by viruses, commonly caused by the respiratory syncytial virus. It primarily affects infants and young children, with symptoms peaking 3–5 days after onset, leading to respiratory difficulty in the affected children8. Each year, 150 million new cases of bronchiolitis are reported globally, with 2–3% requiring hospitalization. China, as a developing country with the world’s second-largest child population, faces significant health pressure and a high socioeconomic burden due to bronchiolitis9. Viral infections often cause airway hyperreactivity in children, related to recurrent wheezing and the onset of asthma. Due to individual variability, children with atopic constitutions have more severe conditions and poorer prognoses10. Therefore, it is urgently important to find serum biomarkers related to the prognosis of children with atopic constitution bronchiolitis.
IgE is an important regulatory factor for allergic diseases, affecting about 30% of the global population with various forms of IgE-related allergic diseases11. Recent data indicate that levels of allergen-specific IgE in the serum of allergic patients are maintained by two distinct mechanisms: one induced by allergen exposure and the other persisting even without the allergen stimuli that maintain IgE levels12. Bronchiolitis is a highly heterogeneous syndrome. IgE can damage the innate antiviral immune response of children with bronchiolitis by cross-linking high-affinity IgE receptors, leading to severe viral infections and subsequent asthma development. Higher IgE levels are associated with an increased risk of rhinovirus infection developing asthma 13. Mitri et al.14 in a study of 1016 children hospitalized for bronchiolitis across 17 hospitals in the United States, found that IgE levels in children with bronchiolitis positively correlated with the severity of the condition. Hasegawa et al.15 discovered that children with bronchiolitis from allergenic sensitizing viral infections had significantly elevated serum IgE levels, a higher risk of sensitization, and a higher probability of recurrent wheezing and developing asthma. This study found that the tIgE levels in the atopic constitution group were significantly higher than those in the non-atopic constitution group and the control group; tIgE levels in the non-atopic constitution group were significantly higher than those in the control group, and tIgE levels in the poor prognosis group were significantly higher than in the good prognosis group, suggesting that high tIgE expression may impair the patient's immunity, mediate the development of allergies and asthma, leading to poor prognosis in patients.
Endogenous NO, produced by airway cells such as macrophages, neutrophils, epithelial cells, endothelial cells, and vascular smooth muscle cells, can lead to increased bronchial hyperresponsiveness and excess mucus secretion when elevated, enhancing vascular permeability, reducing ciliary beating, promoting free radical production, and causing airway inflammation and tissue damage. NO is exhaled in human respiration and is a marker of airway inflammation16. FeNO can be measured in a standardized manner and is simple, convenient, and repeatable, aiding in the diagnosis of asthma, predicting the response to inhaled corticosteroids, monitoring the response to inhaled corticosteroids, and determining the optimal dose for asthma control, and it can also serve as an indicator of therapeutic efficacy17. Nomura et al.18 found that high FeNO expression in children with bronchiolitis complicated by refractory asthma is common for pathogenic bacterial airway colonization and infection events, with a higher frequency of antibiotic use. Ruiz et al.19 discovered that FeNO is significantly overexpressed in patients with bronchiolitis combined with viral infections, leading to decreased lung function, increased allergenic sensitization, and a higher incidence of asthma. This study found that FeNO levels sequentially increased significantly in the control group, non-atopic constitution group, and atopic constitution group, with the expression level in the poor prognosis group significantly higher than in the good prognosis group, suggesting that FeNO may mediate airway inflammation and tissue damage in children with bronchiolitis, leading to the occurrence of the disease and poor prognosis in children with atopic constitution. Related studies indicate that both tIgE and FeNO are involved in the progression of asthma and inflammation, both being biomarkers of asthma development20. This study further shows that the combined prediction of tIgE and FeNO for the prognosis of children with atopic constitution bronchiolitis has an AUC of 0.910, a sensitivity of 78.26%, and a specificity of 93.10%, superior to the individual predictions of tIgE and FeNO, suggesting that both tIgE and FeNO may mediate the progression of the disease in children with atopic constitution bronchiolitis. The combined prediction of both has high sensitivity and specificity and can serve as serum biomarkers for poor prognosis in children with atopic constitution bronchiolitis. Further research has found that a family history of asthma and allergies are factors influencing the development and poor prognosis of bronchiolitis in children, possibly related to the child's genetics21. This study found that the proportions of patients with a family history of asthma and allergies in the poor prognosis group were significantly higher than in the good prognosis group; multifactorial logistic regression analysis shows that a family history of asthma, allergies, tIgE, and FeNO are influencing factors for the prognosis of children with atopic constitution bronchiolitis, suggesting that clinicians should closely monitor these factors and adjust treatment plans in a timely manner to improve patient prognosis.
In summary, both tIgE and FeNO are significantly elevated in children with atopic constitution bronchiolitis, and the combined prediction of both has high predictive value for the prognosis of these children. In addition, this study has issues such as small sample size, single sample source, different age groups were not included, and unclear specific mechanisms of tIgE and FeNO involvement in atopic constitution in children with bronchiolitis. Further experimental design is needed for further research.
References
Gill, P. J., Chanchlani, N. & Mahant, S. Bronchiolitis. CMAJ 194(6), E216 (2022).
Kuitunen, I., Kiviranta, P., Sankilampi, U., Salmi, H. & Renko, M. Helium-oxygen in bronchiolitis—A systematic review and meta-analysis. Pediatr. Pulmonol. 57(6), 1380–1391 (2022).
Fujiogi, M. et al. Integrated associations of nasopharyngeal and serum metabolome with bronchiolitis severity and asthma: A multicenter prospective cohort study. Pediatr. Allergy Immunol. 32(5), 905–916 (2021).
Jang, J.-H. et al. Increased serum free IgE levels in patients with chronic spontaneous urticaria (CSU). World Allergy Organ. J. 15(2), 100629 (2022).
Marcos, M. C. & Cisneros, S. C. What is the added value of FeNO as T2 biomarker?. Front. Allergy 3, 957106 (2022).
Relić, T. et al. Respiratory syncytial virus infection and bronchial hyperreactivity in children up to two years of age in correlation with atopy. Vojnosanitetski Pregl. 73(1), 59–65 (2016).
Vinci, R. & Bauchner, H. Bronchiolitis, deception in research, and clinical decision making. JAMA 312(7), 699–700 (2014).
Bergroth, E. et al. Rhinovirus type in severe bronchiolitis and the development of asthma. J. Allergy Clin. Immunol. Pract. 8(2), 588-595.e4 (2020).
Tian, J. et al. Clinical epidemiology and disease burden of bronchiolitis in hospitalized children in China: A national cross-sectional study. World J. Pediatr. 19(9), 851–863 (2023).
Fan, Y. H., Zhang, P. L., Huang, Y. J., Xie, C. & Ai, T. Risk factors for recurrent wheezing after bronchiolitis. BMC Pediatr. 23(1), 317 (2023).
Zhang, X. et al. IgE contributes to atherosclerosis and obesity by affecting macrophage polarization, macrophage protein network, and foam cell formation. Arterioscler. Thromb. Vasc. Biol. 40(3), 597–610 (2020).
Eckl-Dorna, J. et al. Tracing IgE-producing cells in allergic patients. Cells 8(9), 994 (2019).
Shibata, R. et al. Immunoglobulin E-virus phenotypes of infant bronchiolitis and risk of childhood asthma. Front. Immunol. 14, 1187065 (2023).
Mitri, E. J. et al. Blood eosinophils, specific immunoglobulin E, and bronchiolitis severity. Pediatr. Pulmonol. 56(9), 2997–3004 (2021).
Hasegawa, K. et al. Association of rhinovirus C bronchiolitis and immunoglobulin E sensitization during infancy with development of recurrent wheeze. JAMA Pediatr. 173(6), 544–552 (2019).
Loewenthal, L. & Menzies-Gow, A. FeNO in asthma. Semin. Respir. Crit. Care Med. 43(5), 635–645 (2022).
Escamilla-Gil, J. M., Fernandez-Nieto, M. & Acevedo, N. Understanding the cellular sources of the fractional exhaled nitric Oxide (FeNO) and its role as a biomarker of type 2 inflammation in asthma. Biomed. Res. Int. 2022, 5753524 (2022).
Nomura, N. et al. Nationwide survey of refractory asthma with bronchiectasis by inflammatory subtypes. Respir. Res. 23(1), 365 (2022).
Ruiz, S., Calvo, C., Pozo, F., Casas, I. & García-García, M. L. Lung function, allergic sensitization and asthma in school-aged children after viral-coinfection bronchiolitis. Sci. Rep. 12(1), 7552 (2022).
Badar, A. et al. Association between FeNO, total blood IgE, peripheral blood eosinophil and inflammatory cytokines in partly controlled asthma. J. Asthma Allergy. 13, 533–543 (2020).
Dong, Z. et al. Type 2 cytokine genes as allergic asthma risk factors after viral bronchiolitis in early childhood. Front. Immunol. 13, 1054119 (2022).
Funding
Natural Science Foundation of Hunan Province (2020JJ8033).
Author information
Authors and Affiliations
Contributions
H.W. and Y.Y. designed the research study. H.W., H.X. and F.T. collected data. T.J., Z.L., H.D. and Y.Y. analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study has been approved by the ethics committee of The Affiliated First Hospital of Shaoyang University(Approval Number: 2020031) and informed consent was signed by the guardian of every subject.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wen, H., Xia, H., Tao, F. et al. Prognostic value of serum total IgE and FeNO levels in children with atopic constitution bronchiolitis. Sci Rep 14, 21160 (2024). https://doi.org/10.1038/s41598-024-72236-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-72236-y
