
Abstract
In order to explore the association of oxidative balance score (OBS) with female asthma among U.S. adults, we applied multiple logistic regression models, restricted cubic spline, and subgroup analysis using a cross-sectional study from the National Health and Nutrition Examination Survey (NHANES). 17,582 female out of the 91,351 participants from 2001 to 2018 in NHANES were enrolled in the analysis and 2,795 female participants had asthma. In three models, the OBS was negatively associated with female asthma incidence with the odds ratios (OR) = 0.99. When comparing the ratio of Q2, Q3, and Q4 of OBS quartiles against the Q1 quartile, the adjusted OR with 95% confidence intervals (95%CI) were 0.88 (0.75–1.03), 0.84 (0.73–0.97), and 0.82 (0.70–0.96) respectively, with p < 0.01 in the all covariates adjusted models. The restricted cubic splines indicated a linear relationship between OBS and female asthma. Subgroup analysis revealed no significant interaction effects except in the smoke group (p < 0.001), and there was a significant difference in the former smoker with OR 0.97 (0.96–0.99). We observed that there is negative relationship between OBS score and female asthma incidence, which suggests OBS probably is a protective factor for female on-set asthma. According to the subgroup analysis, smoking should be recommended to reduce asthma morbidity.
Similar content being viewed by others

Introduction
Globally it is estimated that around 3,000,000 people suffer from asthma, which causes a heavy burden on public health system1. Female adults are prone to have a higher prevalence of asthma, and the number is around 20% higher than male adults. Females who have asthma will develop more frequent attacks, more severe, and higher mortality as compared to men2,3,4. Except for the heterogeneous incidences of gender differences, the major risk factors for such prevalence differences are sex hormones and obesity according to the studies in5,6. Very few studies have investigated other relevant factors rather than the gender-related health issues to understand the risk factor of female adult asthma.
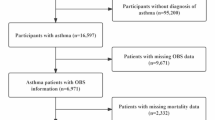
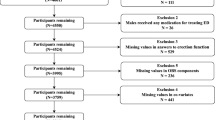
Oxidative stress refers to the imbalance between the pro-oxidant and antioxidant process, and such imbalance will lead to oxidative damage, which provides the basis for various diseases such as inflammatory diseases, aging, metabolic diseases, cancer, etc7,8,9,10. In asthma such imbalance between pro-oxidants and antioxidants play a role. People who develop asthma is characterized as increased oxidant production and reduced antioxidant defenses11. Meanwhile, it has been shown that there is oxidative stress linked to dietary and lifestyle factors, which are evaluated using the Oxidative Balance Score (OBS)12. Smoking, drinking, obesity, and vitamins (A, C, and E, depending on doses) et al. are pro-oxidant factors, while antioxidant dietary, normal weight, non-smoking, alcohol-free, physical activities, etc. are antioxidant factors12,13. OBS has been suggested to be related to many diseases like osteoarthritis, renal disease, cardiovascular disease, chronic obstructive pulmonary disease, and cancers14,15,16,17. We therefore aimed to investigate if OBS can be an indicator for female on-set asthma. Thus, this study was designed to investigate the association between OBS and female asthma by using the National Health and Nutrition Examination Survey (NHANES). Flow chart of the study was shown in Fig. 1.

Flow chart of the study design. The selection of the participated in this project. We have a total 17,582 female adults, and among these females, 2,795 have asthma and 14,787 are asthma-free.
Results
Participant characteristics
A total of 91,351 individuals participated in this project in the beginning, of whom 50,201 individuals aged ≥ 20 years, and they were remained in the project. There were 14,622 persons with incomplete covariates and 268 with incomplete OBS information. After 17,729 Male participants were excluded, 17,582 Female participants with OBS > 0 were ultimately enrolled. Among the final subjects, 2,795 asthma and 14,787 non-asthma subjects remained in our research.
From NHANES(2001–2018), 17,852 Female participants were selected for the study, among whom 2,795 had asthma and 14,787 did not suffer from asthma. There were significant differences between asthma and non-asthma in OBS, age, poverty, waist, BMI, education, Race, smoking, alcohol, diabetes, hypertension, coronary heart disease, and family history of asthma. Asthma subjects had lower OBS, age, and poverty but higher BMI and waist (p < 0.05). The percentage of non-Hispanic White participants who suffered from asthma was more significant than non-Hispanic Black, Mexican American, and other ethnicity (p < 0.05). People with a high level of education were prone to asthma. In accordance with Poverty income ratio (PIR), wealthy people were more susceptible to asthma than poor people. The baseline characteristics of Female participants are shown in Table 1. All variables were statistically significant between different quartiles of OBS, as shown in Table 2 (p < 0.05).
Associations between OBS and female asthma
Three Models were constructed. No covariate was adjusted in Model (I) Age, education, Race, and PIR were adjusted for Model (II) In contrast, all covariates including age, education, Race, PIR, diabetes, hypertension, coronary heart disease, and family history of asthma were adjusted in Model III.
Negative correlations between OBS and Female asthma were in all Models. OR (95% CI) of Model III was 0.99 (0.98, 1.00). Similarly, a negative association remained in all models when the OBS was grouped by quartiles. In Model III, when comparing the Q4, Q3, and Q2 groups to the reference Q1 group, O.R.s (95% C.I.s) for asthma risk were 0.82(0.70,0.96), 0.84(0.73,0.97) and 0.88(0.75,1.03), respectively (p for trend = 0.01) (Table 3). A restricted cubic spline showed a linear relationship between OBS and Female asthma(p-nonlinear = 0.1627). The adjusted O.R.s for Female asthma decreased as increasing OBS (Fig. 2).

The relationship between OBS and Female asthma prevalence.
Subgroup analysis
The results of the subgroup analysis are shown in Fig. 3, stratified by age, education level, Race, PIR, smoke, alcohol, waist, hypertension, coronary heart disease, diabetes and family history of asthma. Except for the smoke subgroup, there was no significant interaction in other groups with the link between OBS and Female asthma. Specifically, the interaction was significant in the smoke group (p for interaction < 0.001) and a negative association was found in former smoke individuals and Female asthma prevalence(OR (95% CI), 0.97 (0.96, 0.99))(Fig. 3).

Subgroup analysis of the association between OBS and Female asthma.
Age, education level, Race, PIR, smoking, alcohol, waist, hypertension, coronary heart disease, diabetes, and family history of asthma were stratified except for the covariate corresponding subgroup.
Discussion
Asthma is a heterogeneous disease characterized by airway hyperresponsiveness, chronic airway inflammation, and reversible airway remodeling. It is the most common chronic respiratory disease with high prevalence and mortality globally. The different endotypes and phenotypes in asthma pose challenges for treating and controlling this disorder1. At the same time, the recurrence and difficulty in controlling asthma squander a lot of public health resources. Thus, understanding the associations between risk factors and asthma is necessary to prevent and control asthma. Asthma prevalence also varies by several variables such as age, sex, Race, poverty, country, etc. Interestingly, asthma is more common in boys in childhood, while Female adults are more likely to develop asthma18. The explanation for the above phenomenon is that sex hormones and obesity may play critical roles in the susceptibility and severity of women’s asthma2,6. Of course, there are other relevant risk factors for the higher incidence of Female adults asthma that we are not yet aware of.
That oxidation products like reactive oxygen species(ROS) and reactive nitrogen species (RNS) overcoming antioxidant defenses lead to oxidative stress in asthma have been shown in a variety of studies11,19. We speculate that anti- and pro-oxidant balance may have a connection with Female asthma prevalence. Calculating the anti- and pro-oxidant components of diets and lifestyles, OBS can assess an individual’s oxidative/antioxidant condition and become a more accurate indicator in epidemiological investigations, especially in chronic disease studies20. In OBS, antioxidants contribute positively while pro-oxidants play negatively, which means a higher OBS has a stronger antioxidant exposure. Previous studies demonstrated higher OBS was negatively associated with the risk of gastric cancer21. That individuals with higher OBS had a lower risk of hypertension was discovered in a prospective cohort22. Antioxidant diets and lifestyles were proven to reduce sleep problems in a cross-study from NHANES23. The phenomenon that the higher the OBS, the lower risk of chronic obstructive pulmonary disease (COPD) frailty, especially in women, was found17. Likely, the higher OBS had a connection to a lower risk of osteoporosis in postmenopausal women24. Accordingly, the relationship between OBS and Female asthma was investigated in our study.
In the present study, we found that OBS was negatively associated with Female adults after adjusting for all covariates. Of note, the O.R.s of Female asthma decreased as OBS increased in the OBS quartile groups, which suggested antioxidant diets and lifestyles could contribute to reducing asthma morbidity and provided new ideas for preventing asthma. RCS analysis displayed no nonlinear relationship between OBS and Female asthma. Meanwhile, we also explored if the subgroup can interact with the associations of OBS and Female asthma prevalence. Although menopause was related to lung function has been shown in many previous studies, in our study, age groups have no significant interaction in the subgroup analysis suggesting that age did not affect the incidence of Female asthma25.In a NHANES study, Waist was found to be negatively associated with FVC and FEV1 and positively associated with FEV1/FVC26. In our study, asthma subjects had higher waist, however, there was no significant interaction in the waist groups (normal group and abdominal obesity group) in the subgroup analysis suggesting that waist groups did not affect the incidence of Female asthma. We have added the relevant data in Table 1; Fig. 3, along with the explanations in the discussion section. Only the smoke group had interactions (p for interaction < 0.001) and a negative association was found in former smoke individuals and Female asthma prevalence(OR (95% CI), 0.97 (0.96, 0.99)).Cotinine is an important component of OBS. In Table 2, the higher OBS the lower cotinine exposure which indicating cotinine plays vital oxidation.It can be inferred that smoking cessation may be a useful lifestyle to reduce the onset of Female asthma.
Likewise, there are some limitations. Firstly, the study is cross-sectional and could not provide the causality between OBS and Female asthma. Secondly, all the confounders could not be completely ruled out in our investigation. Thirdly, there may be recall bias because of the definition of asthma from self-reports. Fourthly, there are different definitions of OBS with varied defined ranges and cutoff thresholds. Also, other potential anti- and pro-oxidant diet and lifestyle factors need to be taken into account.
Controlling risk factors is a crucial step for asthma prevention and management. In the present study, we found that the Oxidative Balance Score was negatively linked to the onset of Female asthma. In other words, when antioxidants of diet and lifestyle factors are dominant, the Female asthma rate becomes lower. Antioxidant diet and antioxidant lifestyle maybe important measures but easy for preventing and managing Female asthma, although Female asthma is severe and difficult to control.
Materials and methods
Study design and population
The study is covered by the ethical permit, the approval of the National Center for Health Statistics Institutional Review Board. The participants were selected by a multistage, stratified probabilistic sampling approach. After written informed consent, the enrolled subjects participated in the following sections including answering questionnaires, interviews, physical examinations, and laboratory testing. We further conducted this study to verify the association between OBS and female asthma, using the data gathered from NHANES (2001–2018), which could be traced back to the website http://www.cdc.gov/nchs/nhanes.htm27.All methods were performed in accordance with the relevant guidelines and regulations of NHANES Tutorials provided by NHANES.
Definition of OBS
OBS is calculated based on 16 different nutrients and 4 different lifestyles as described in12. These 16 different nutrients include fiber, carotene-retinol equivalent (RE), riboflavin, niacin, total folate, vitamin B6, vitamin B12, vitamin C, vitamin E, calcium, magnesium, zinc, copper, selenium, iron, and total fat. These 16 types of nutrients were be examined on the first two days among the interviews with no supplementary nutrients in dietary. In the dietary OBS components, iron and total fat were defined as pro-oxidants, while the other 14 nutrients were considered antioxidants. In lifestyle OBS components, physical activity had an antioxidant effect, while alcohol from 24-hour dietary recall interviews (24 h), body mass index (BMI), and serum cotinine were antioxidant factors. BMI was calculated as weight divided by height squared (kg/m2). The weekly metabolic equivalent (MET) resulted from the household interview data of the individual leisure-time activities during the past 30 days.
According to its distribution, each component was divided into three groups for Males and Females, respectively. According to groups, antioxidants were recorded from 0 to 2, while pro-oxidants were counted from 2 to 0. Points of each component discussed above were summed in OBS, and the higher the OBS, the more potent antioxidant12.
Definition of asthma
Asthma was identified when participants answered “YES” both for the Medical Condition Questionnaire (MCQ010: Ever been told you have asthma? ) and MCQ035(Still have asthma? )28. If they answered “YES” to “Blood relatives have asthma?” they were believed to have a family history of asthma.
Covariates
The covariates contained age, poverty, Race, education, smoking (never, former, and now), alcohol (never, former, mild, moderate, and heavy), hypertension, diabetes, coronary heart disease, and family history of asthma. Race was categorized as non-Hispanic white, non-Hispanic black, Mexican American and others. Education was graded into less than high school(less than 9th grade), high school(including 9-11th grade, 12th grade with no diploma and high school grad) and more than high school(college graduate or above). The PIR was grouped as low (PIR ≤ 1.3), moderate (1.3 < PIR < 3.5), and high (PIR ≥ 3.5)29. The factor of smoke was classified as never (never smoked or smoked < 100 cigarettes during lifetime), former(smoked ≥ 100 cigarettes ever and quit smoking completely now) and now (smoked ≥ 100 cigarettes and kept smoking currently)30. Alcohol was grouped 5 levels such as never: <12 drinks in all; former: ≥12 drinks in 1 year and had no drink last year; mild: one drink/day for females, two drinks/day for males; moderate: ≥two drinks/day for females and ≥ three drinks/day for males or 2 ≤ binge drinking < 5 /month; heavy:≥three drinks/day for females and ≥ four drinks/day for males or ≥ four drinks for females and ≥ five drinks for males on same occasion31. BMI was regrouped as under/normal (BMI < 25), overweight (25 ≤ BMI < 30), and obese (BMI ≥ 30)32. Abdominal obesity was defined as waist ≥ 88 cm for females according to ATP-III criteria33. When participants answered “YES” to “Ever told you had diabetes/hypertension/coronary heart disease”, they were considered to have diabetes, hypertension and coronary heart disease, respectively.
Statistical methods
R 4.3.2 was used to process raw data analyzing by “nhanesR” packages (version 0.9.5.0). The continuous variables were expressed as mean ± standard deviation (S.D.) and analyzed by t-test, while non-continuous variables were displayed as percentages (%) and analyzed by chi-square test. The correlations between OBS and asthma were analyzed by multivariate logistic regression, expressed as odds ratios (O.R.s) and 95% confidence intervals (C.I.s). Three Models were constructed as follows: Model I(no covariates were adjusted), Model II(only demographic covariates were adjusted) and Model III(all covariates were adjusted). The nonlinear relationship was investigated by restricted cubic spline (RCS) and interactions were explored by subgroup analysis. p < 0.05(two-sided) indicated significance.
Data availability
Data is provided within the manuscript and can be dated on the NHANES - National Health and Nutrition Examination Survey Homepage (cdc.gov).
References
Stern, J., Pier, J. & Litonjua, A. A. Asthma epidemiology and risk factors. Semin. Immunopathol.42, 5–15. https://doi.org/10.1007/s00281-020-00785-1 (2020).
Melgert, B. N., Ray, A., Hylkema, M. N., Timens, W. & Postma, D. S. Are there reasons why adult asthma is more common in females? Curr. Allergy Asthma Rep.7 (2), 143–150. https://doi.org/10.1007/s11882-007-0012-4 (2007).
Baibergenova, A. et al. Sex differences in hospital admissions from emergency departments in asthmatic adults: a population-based study. Ann. Allergy Asthma Immunol.96 (5), 666–672. https://doi.org/10.1016/S1081-1206(10)61063-0 (2006).
Leynaert, B. et al. Gender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: a population-based cohort. Thorax. 67, 625–631. https://doi.org/10.1136/thoraxjnl-2011-201249 (2012).
Lauzon-Joset, J. F. et al. Oestrogen amplifies pre‐existing atopy‐associated Th2 bias in an experimental asthma model. Clin. Experimental Allergy. 50, 391–400. https://doi.org/10.1111/cea.13544 (2019).
Chen, Y., Dales, R., Tang, M. & Krewski, D. Obesity may increase the incidence of asthma in women but not in men: longitudinal observations from the Canadian National Population Health surveys. Am. J. Epidemiol.155 (3), 191–197. https://doi.org/10.1093/aje/155.3.191 (2002).
Cano Sanchez, M., Lancel, S., Boulanger, E. & Neviere, R. T. Oxidative stress and mitochondrial dysfunction in the treatment of impaired Wound Healing: a systematic review. Antioxidants. 7 (8), 98. https://doi.org/10.3390/antiox7080098 (2018).
Singh, A., Kukreti, R., Saso, L. & Kukreti, S. Oxidative stress: a key modulator in neurodegenerative diseases. Molecules. 24 (8), 1583. https://doi.org/10.3390/molecules24081583 (2019).
Bhatti, J. S., Bhatti, G. K. & Reddy, P. H. Mitochondrial dysfunction and oxidative stress in metabolic disorders — a step towards mitochondria based therapeutic strategies. Biochim. et Biophys. Acta (BBA) - Mol. Basis Disease. 1863, 1066–1077. https://doi.org/10.1016/j.bbadis.2016.11.010 (2017).
Moloney, J. N. Cotter TG.ROS signalling in the biology of cancer. Semin Cell. Dev. Biol.80, 50–64. https://doi.org/10.1016/j.semcdb.2017.05.023 (2018).
Erzurum, S. C. New insights in Oxidant Biology in Asthma. Annals Am. Thorac. Soc.13, S35–S39. https://doi.org/10.1513/AnnalsATS.201506-385MG (2016).
Hernández-Ruiz, Á. et al. Oxidative balance scores (OBSs) integrating nutrient, Food and Lifestyle dimensions: Development of the NutrientL-OBS and FoodL-OBS. Antioxidants. 11. https://doi.org/10.3390/antiox11020300 (2022).
Bjørklund, G. & Chirumbolo, S. Role of oxidative stress and antioxidants in daily nutrition and human health. Nutrition. 33, 311–321. https://doi.org/10.1016/j.nut.2016.07.018 (2017).
Lee, J-H. et al. Relationship between oxidative balance score and quality of life in patients with osteoarthritis. Medicine. 98. https://doi.org/10.1097/md.0000000000016355 (2019).
Ilori, T. O. et al. Oxidative balance score and the risk of end-stage Renal Disease and Cardiovascular Disease. Am. J. Nephrol.45, 338–345. https://doi.org/10.1159/000464257 (2017).
He, X. et al. Association between oxidative balance score and frailty in chronic obstructive pulmonary disease. Heliyon. 10. https://doi.org/10.1016/j.heliyon.2024.e25750 (2024).
Li, J., Yang, C. & Xiang, K. Association between oxidative balance score and prostate specific antigen among older U.S. adults. Front. Public. Health. 11. https://doi.org/10.3389/fpubh.2023.1336657 (2024).
Dharmage, S. C., Perret, J. L. & Custovic, A. Epidemiology of asthma in children and adults. Front. Pead. 7. https://doi.org/10.3389/fped.2019.00246 (2019).
Comhair, S. A. & Erzurum, S. C. Redox control of asthma: molecular mechanisms and therapeutic opportunities. Antioxid. Redox Signal.12 (1), 93–124. https://doi.org/10.1089/ars.2008.2425 (2010).
Hernández-Ruiz, Á. et al. A review of a Priori defined oxidative balance scores relative to their components and impact on Health outcomes. Nutrients. 11. https://doi.org/10.3390/nu11040774 (2019).
Kim, J., Lee, J., Choi, I. J., Kim, Y-I. & Kim, J. Gastric cancer risk is reduced by a predominance of antioxidant factors in the oxidative balance: a hospital-based case-control study in Korea. Epidemiol. Health. 44. https://doi.org/10.4178/epih.e2022089 (2022).
Lee, J-H., Son, D-H. & Kwon, Y-J. Association between oxidative balance score and new-onset hypertension in adults: a community-based prospective cohort study. Front. Nutr. 9. https://doi.org/10.3389/fnut.2022.1066159 (2022).
Lei, X., Xu, Z. & Chen, W. Association of oxidative balance score with sleep quality: NHANES 2007–2014. J. Affect. Disord.339, 435–442. https://doi.org/10.1016/j.jad.2023.07.040 (2023).
Shahriarpour, Z. et al. Oxidative balance score and risk of osteoporosis among postmenopausal Iranian women. Archives Osteoporos. 16. https://doi.org/10.1007/s11657-021-00886-w (2021).
Pata, O. et al. The effects of hormone replacement therapy type on pulmonary functions in postmenopausal women.Maturitas(2003) 46(3):213–218. https://doi.org/10.1016/s0378-5122(03)00191-9
Xu, Z. et al. Association between waist circumference and lung function in American middle-aged and older adults: findings from NHANES 2007–2012. J. Health Popul. Nutr.43 (1), 98. https://doi.org/10.1186/s41043-024-00592-6 (2024).
Jayanama, K., Theou, O., Blodgett, J. M., Cahill, L. & Rockwood, K. Frailty, nutrition-related parameters, and mortality across the adult age spectrum. BMC Med. 16. https://doi.org/10.1186/s12916-018-1176-6 (2018).
Zhang, W., Li, W. & Du, J. Association between dietary carotenoid intakes and the risk of asthma in adults: a cross-sectional study of NHANES, 2007–2012. BMJ Open. 12. https://doi.org/10.1136/bmjopen-2021-052320 (2022).
Liu, Q. et al. Asthma prevalence is increased in patients with high metabolism scores for visceral fat: study reports from the U.S. Front. Endocrinol. 14. https://doi.org/10.3389/fendo.2023.1162158 (2023).
Liu, X. et al. Association between a body shape index and prostate cancer: a cross-sectional study of NHANES 2001–2018. Int. Urol. Nephrol.https://doi.org/10.1007/s11255-023-03917-2 (2024).
Hicks, C. W., Wang, D., Matsushita, K., Windham, B. G. & Selvin, E. Peripheral neuropathy and all-cause and Cardiovascular Mortality in U.S. adults. Ann. Intern. Med.174, 167–174. https://doi.org/10.7326/m20-1340 (2021).
Haslam, D. W., James, W. P. T. & Obesity Lancet366: 1197–1209. doi:https://doi.org/10.1016/s0140-6736(05)67483-1. (2005).
Sarathy, H. et al. Abdominal obesity, race and chronic kidney disease in young adults: results from NHANES 1999–2010.PLoS one(2016) 11(5):e0153588. https://doi.org/10.1371/journal.pone.0153588
Acknowledgements
We thank all the participants and staff of NHANES.
Funding
The study was supported by the Young Talent Development Plan of the Changzhou Health Commission (No. CZQM2021025) and the Science and Technology Development Foundation of the affiliate hospitals of Xuzhou Medical university(No. XYFY202305).
Author information
Authors and Affiliations
Contributions
Writing original draft and Methodology: Xiao Qi, Tianlei Zhou, supervision and design: Jianlei Tang.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The raw data and informed consent can be dated on the NHANES - National Health and Nutrition Examination Survey Homepage (cdc.gov).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Qi, X., Zhou, T. & Tang, J. Correlations between oxidative balance score and female asthma among U.S. adults. Sci Rep 14, 22451 (2024). https://doi.org/10.1038/s41598-024-73533-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-73533-2
