
Abstract
Dual cognitive-walking treadmill training (DTT), designed to replicate real-life walking conditions, has shown promise effect in individuals with Parkinson’s disease (PD). This study aims to compare the effects of DTT versus single treadmill training (STT) on cognitive and walking performance under both single and dual task conditions, as well as on fall, patients’ subjective feeling, and quality of life. Sixteen individuals with PD were randomly assigned to DTT or STT group and underwent 8 weeks of training. The DTT group received treadmill training with cognitive loads, while the STT group received treadmill training without cognitive load. Outcome measures included gait parameters (speed, step length) and cognitive performance (reaction time, accuracy, composite score) under both single and dual task conditions. Unified Parkinson’s Disease Rating Scale-part III (UPDRS-III), Falls Efficacy Scale (FES), Patient Global Impression of Change (PGIC), and Parkinson’s Disease Questionnaire (PDQ-39) were also measured. Both DTT and STT groups showed increased comfortable walking speed and step length. Only the DTT group demonstrated significant improvements in cognitive composite score under both single and dual task conditions, as well as UPDRS-III, FES, and PDQ-39(p < 0.05). DTT can enhance cognitive function without compromising walking ability and also have real-world transferability.
Similar content being viewed by others

Introduction
Parkinson’s disease (PD) is a common neurodegenerative disease in the elderly with the second highest prevalence after Alzheimer’s disease1. Among individuals aged 65 and older, over 2% are afflicted by this disorder, and the average onset occurs between 50 and 60 years of age2,3. In addition to the cardinal signs of Parkinson’s, including tremor, bradykinesia, rigor and postural instability, gait disturbances represent a significant and debilitating3 symptom in Parkinson’s disease. This can lead to a loss of mobility, an increased risk of falls4, and a detrimental impact on the independence and overall quality of life5.
Safe walking is challenging for PD patients. In the past ten years, treadmill is the most employed training method to promote normal gait. Literatures with high evidence showed treadmill training of 16–35 min each time, 2–3 times a week, for a total of 5–8 weeks resulted in significant improvements in walking speed, step length, balance and other gait parameters6,7,8. However, treadmill training does not actually reflect the complexity of community walking environment, which requires varied dual-task walking abilities. Hence, it is valuable to investigate whether the effects of treadmill training can be transferred to challenging conditions that are likely to arise in real-world community environments, thus enhancing the quality of life in this population.
Recent studies showed executive dysfunction and automatic movement dysfunction significantly influenced gait and balance performance and rehabilitation in people with Parkinson’s disease9,10,11,12. Dual-task walking is an important functional ability that requires walking while concurrently performing cognitive tasks such as memorizing shopping lists and doing calculations. Walking under cognitive load requires automatic control of walking due to the competition of attentional resources for walking and cognitive tasks. Patients of PD often present difficulties for tasks that require simultaneously planning, cognitive flexibility, generating strategies, and spatial memory which leads to negative impacts on their daily activities13. The degree of impairment on tasks requiring spatial working memories and planning abilities was found to be correlated to the severity of Parkinson’s disease14. A recent study showed that mild to moderate PD patients with postural instability and gait difficulty subtype sustained deficits in spatial cognition, attentional flexibility and organizational planning, as well as whole-body spatial memory domains15. Our recent study showed that the cognitive-walking test using visual-spatial memory cognitive task exacerbated performances related to gait automaticity function and sharpened the cognitive deficits for early-stage PD patients16. This serves the dual cognitive walking paradigm an important training strategy for gait automaticity in PD.
The task specificity principle, which suggests that training should mimic the functional tasks individuals need to perform in their daily lives, suggesting that cognitive-walking dual task training might be superior to single task walking training. Dual-task training had been suggested to improve mobility, functional performance, and cognition in elder faller17. Researchers have pointed out that in a single walking task, patients with Parkinson’s disease mainly rely on the cerebral cortex to control walking and use attention resources to achieve safe walking18. Thus, single walking training may not significantly improve walking automation capabilities. Cognitive dual task training might enhance the executive function and attention distribution practice. Previous studies have shown that dual-task training can improve gait parameters and cognitive function in various populations, including older adults and individuals with PD. Mirelman et al. (2016) using VR treadmill training on individuals with idiopathic fall elder adults, Parkinson disease, and mild cognitive impairments and found the incident rate of falls decreased more than treadmill training group19. Authors explained that VR add cognitive loads during training, suggesting that cognitive-treadmill training might be crutial to improve the balance and gait in real life condition. However, the amount of cognitive load provided on VR is not controlled and specified and the allocation of patients’ attention was hard to control during VR training, making the effect of training hardly attributed to cognitive-walking dual task training.
In short, the decline in executive function could deteriorate dual task walking performance, while impaired walking and poor balance abilities may cause vulnerabilities to falls in PD, thereby compromising their quality of life. Cognitive-walking training, which mimics daily-life situations might be optimal for PD patients to translate the training effect to real life environments and improve their quality of life. However, due to the resource-competition feature in cognitive-walking dual task training, motor learning, which is required in walking training, might be interfered. The comparative effects of cognitive-walking dual task training and single task training on walking performance, their applications to daily life activities, and quality of life need to be explored. Therefore, we aimed to investigate the effect of dual cognitive-walking training versus single task walking training on both cognitive and walking performance under both single and dual task conditions, and on fall, patients’ subjective feeling, and quality of life. At the same time, spatial memory, which was considered to be highly related to executive function20, was employed as cognitive load to compare the performance difference with and without cognitive load training.
Methods
Research design
This study is a single blind randomize controlled study. A total of 16 participants with PD were recruited from the Division of Movement Disorders in the Department of Neurology at the Chang Gung Memorial Hospital in Linkou, a referring medical center in Taiwan. Patients with idiopathic PD is diagnosed by a neurologist specialized in movement disorders according to the diagnostic criteria proposed by Gelb et al.21, The inclusion criteria included age between 45 and 70 years, asymmetrical onset of at least two of three cardinal signs, early-stage PD (mHYS30 from 1 to 2.5 during the off-state), and Montreal cognitive assessment score of 26 or higher. Patients were excluded if they have history of neurological disease other than PD, previous neurosurgery for PD, moderate-to-severe dyskinesia, unstable medical or psychiatric comorbidities, and orthopedic conditions restricting exercise, or performing aerobic exercise for longer than 20 min at least three times weekly prior to the study22,23. Patients maintained their usual medical treatment throughout the study. The sample size was estimated by referring to the speed of the double arithmetic task in the previous article24 with the power set to 0.8. The protocol of this study was approved by the Research Ethics Committee of the Chang Gung Medical Foundation in accordance with the Helsinki Declaration, and written informed consent was obtained from all participants.
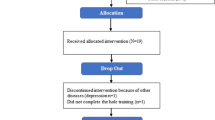
After inclusion, participants were randomly assigned to either the single treadmill training (STT) or dual cognitive-walking treadmill training (DTT) group using a computer-generated randomization table. Pre-randomize table is a random order run out by a computer to ensure that the order is different and to prevent subjects from drawing the same order every time they are redrawn. This process was conducted by an independent researcher who was not involved in the recruitment, assessment, or training of participants to minimize selection bias. As each participant was enrolled in the study, the independent researcher referred to the pre-generated randomization table to determine their group assignment. The researcher then informed the participant of their group assignment without revealing the sequence to the study team. This randomization process was designed to ensure that the groups were comparable at baseline and that the study’s findings were not influenced by selection bias. Participants were blind to the purpose of the study. Demographic data included subject number, name, age, sex, education level, height, weight, age, H&Y stage, medication, and daily dopamine equivalent dose of patients with Parkinson’s disease25 were obtained. The research flowchart is as shown in Fig. 1. Setting dual cognitive walking with treadmill training instead of outdoor or real-world walking as a rehabilitation strategy based on several reasons. The treadmill setting allows for a controlled environment where variables such as walking speed, cognitive task complexity, and session duration can be precisely regulated. It would be more challenging in an outdoor or real-world setting due to the varying environmental factors, making it difficult to replicate the training conditions in future sessions and achieve similar results. Besides, for individuals with PD, the risk of falls and injuries is a significant concern. Treadmill training, conducted in a safe and supervised setting, minimizes these risks compared to outdoor walking.

Flow chart of participant enrollment.
Participants in both groups then received a single cognitive test, a single walking test, and a dual walking test. In the single cognitive test, subjects were tested in sitting position. The spatial memory task required subjects to memorize the positions and order of three yellow squares in a blank nine-square grid. After the yellow squares disappeared, subjects had to recite the three corresponding numbers in the nine-square grid. Wireless headset microphone (Aibo, Mini A8, LY-MIC-BTA8, New Taipei City, Taiwan) was used to record the oral response to analyze the reaction time and accuracy. The experimental environment settings can be referred to our previous study16. The duration of the evaluation, including instructions, was kept under 1.5 h to ensure that subjects could tolerate it.
In single and dual walking tests, a pressure mat (GAITRite, CIR systems Inc, Franklin, NJ, USA) was used for measuring the temporal-spatial analysis of gait. The pressure mat is 3.66 m long by 0.9 m wide contain pressure sensors. It was considered as one of the gold standards in gait analyses with very high accuracy and reliability in older adults26. For the dual-walking test, the subject walked at a comfortable speed on a pressure mat while simultaneously performing a previously described spatial memory cognitive task projected on a big screen in front of him/her. No task prioritization was assigned during this dual-walking test. The duration of total evaluation session, including instructions, was less than 1.5 h to make sure subjects could tolerate it.
For evaluation of the translational effects of training to daily life, four questionnaires/scales were used. There are the Unified Parkinson’s Disease Rating Scale-part III (UPDRS-III), Falls Efficacy Scale International (FES), Parkinson’s Disease Questionnaire (PDQ-39), and Patient Global Impression of Change (PGIC). The evaluation was performed by a trained clinician. The UPDRS-III is a rating tool used to gauge the motor severity of Parkinson’s disease which contains 14 questions with a full score of 56 points7,27. The lower the score, the better the action function. The minimum clinically important difference (MCID) is 2.5 points28. FES was used to evaluate the level of attention to fear of falling. There are a total of 16 questions with a full score of 64 points. The higher the score, the higher the degree of attention required. A total score greater than 23 points indicates a high degree of fear of falling29. PDQ-39 was used to assess the quality of life of patients with PD. It contains 8 aspects: mobility, activities of daily living, emotional wellbeing, stigma, social support, cognitive impairment, communication and bodily discomfort with a total of 39 questions. The total score of all aspects is 156 points30. The higher the score, the less quality of life. PGIC was first proposed by Guy in 197631. It is a patient-reported outcome instrument filled out by patients to evaluate the severity of their disease or the treatment effects. It is a seven-point scale that a score of one represents great improvement, and a score of seven represents extreme deterioration32.
After the pre-training evaluation, subjects received 8 weeks of STT or DTT according to the groups assigned. The training was performed under medication. The training protocol was 25–45 min for each session, 2 times a week for 8 weeks. The treadmill training intensity for both the STT and DTT groups was the same, gradually increasing over the eight-week period to align with the participants’ physical progress. In the first two weeks, the speed was set at 100% of the level walking speed, and the exercise duration was 25 min. In the third and four weeks, the speed was set at 100% of the level walking speed, and the exercise duration was 35 min. In the fifth and sixth weeks, the speed was set at 110% of the level walking speed, and the exercise duration was 40 min. In the seventh and eight weeks, the speed was remained at 110% of the level walking speed, and the exercise duration was 45 min. The training time included 5 min of warm-up and 5 min of cool-down, with no rest periods. This incremental dosage design was referenced according to the methodology employed in the earlier study conducted by Dorfman et al. 201417.
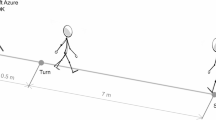
For the DTT group, the treadmill intensity was set to match that of the STT group, but spatial memory cognitive tasks were displayed on a big screen in front of the treadmill during the training. To avoid learning effect, the cognitive tasks used for DTT were different from that used for pre and post training evaluation. Throughout the training sessions, participants were engaged in the memorization of items situated in different locations, encompassing categories. Following the disappearance of the items, participants orally identified the name of the items previously shown on a marked location. The level of difficulty for this task progressed every two weeks, i.e., from memorizing the positions of three items in a square grid to a more challenging six-square grid. (Fig. 2) The cognitive tasks were excluded from the warm-up and cool-down periods, and no specific instructions were provided to prioritize these tasks during the overall process. One week after concluding the 8-week training period, participants underwent a post-training evaluation, utilizing the same assessment items employed in the pre-training assessment.

The cognitive training paradigm for DTT group.
Data analysis
Response accuracy, reaction time, and the trade-off effect were analyzed for cognitive performance. Response accuracy, quantified as the rate of correct responses, was computed by dividing the count of accurate responses by the total stimuli and multiplying the result by 100, with the unit expressed as a percentage (%). Reaction time, indicating the duration from stimulus initiation to response, was measured in milliseconds (ms). The inherent trade-off between speed and accuracy in cognitive tasks was assessed employing the cognitive composite score proposed by Springer et al. (2006)33 which is calculated as follows: response correct rate divided by reaction time, multiplied by 100, with the unit expressed as a percentage (%). A higher cognitive composite score indicates superior performance, providing an overall evaluation of cognitive task efficiency. For gait outcomes, step length, velocity, and the coefficient of variation (CV) of step length and gait were analyzed. Cadence was not analyzed, as it can be a misleading indicator of gait improvement in PD patients34. Additional outcome variables include Part III of the Unified Parkinson’s Disease Rating Scale, the Self-Fall Attention, the PDQ-39, and the VAS of the Overall Patient Improvement Scale.
Statistical analysis
Due to the non-normal distribution of the data, we employed the Mann-Whitney U test to compare group differences. To evaluate the training effects within each group, we utilized both the Friedman test and the Wilcoxon signed-rank test. The significance level was set at p < 0.05.
Results
Patient characteristics
A total of 16 participants 8 in the DTT group (4 female, 4 male, average age 62.63 ± 5.32 years), and 8 in the STT group (7 female, 1 male, average age 63.63 ± 6.48 years) completed the training. There was no statistically significant difference between the disease related baseline characteristics in two groups (Table 1).
The effect of training on cognitive and walking performance
In terms of cognitive performance, we observed a significant training effect in the DTT group. When tested in a seated position, the cognitive composite score displayed a significant improvement (p = 0.021), and similar enhancements were also existed during walking (p = 0.044) after training (Fig. 3A,B). Reaction time decreased (p = 0.03) (Fig. 3C,D), while response accuracy remained unaltered (p = 0.368) in seated position (Fig. 3E,F). Conversely, in the STT group, we did not identify any significant changes in cognitive performance, whether measured in terms of composite score, reaction time, or accuracy, either when assessed in a seated position or during walking (Fig. 3).

Comparison of the cognitive performance between DTT and STT group under single task test and dual task test conditions before pre, after 4 weeks, and post training. * significant difference with pre (p < .05). # DTT group showed significant difference with STT group (p < .05).
For walking performance, comfortable walking speed increased in both DTT group (p = 0.03) and in STT group (p = 0.002) (Fig. 4A). Both groups showed improvement in step length (DTT: p = 0.034, STT: p = 0.002) (Fig. 4C). During fast walking, neither group showed improvement in walking speed, and step length (Fig. 4B, D). While under dual walking test, the STT group showed little but significant improvement in walking speed (p = 0.021) and step length (p = 0.034) (Fig. 4E, F). For step length CV, no significant changes were found in either the DTT or STT groups during comfortable walking (DTT: P = 0.197; STT: P = 0.197). During fast walking, step length CV also did not show significant improvement in either group (DTT: P = 0.325; STT: P = 0.607). Similarly, for the dual walking test, no significant changes were observed (DTT: P = 0.417; STT: P = 0.882). For walking speed CV, no significant changes were noted in either group during comfortable walking (DTT: P = 0.687; STT: P = 0.417). During fast walking, the STT group showed a significant improvement in walk speed CV (P = 0.01), while the DTT group did not (P = 1). For the dual walking test, no significant changes were found in walking speed CV for either group (DTT: P = 0.223; STT: P = 0.135) (Table 2).

Comparison of the walking performance between DTT and STT group under single task test and dual task test conditions before pre, after 4 weeks, and post training. * significant difference with pre (p < .05).
The general functional outcomes
According to Table 3, participants in the DTT group showed a significant improvement in the UPDRS-III (p = 0.003), the FES (p = 0.023) and the PDQ-39 (p = 0.009) compared to pre-training. However, no significant changes were found in the STT group.
For the PGIC, participants in both DTT (p = 0.001) and STT (p = 0.001) groups showed significant improvements after training while participants in the DTT group achieved greater improvement than participants in STT group (p = 0.039).
Discussion
The main finding of this study was that the DTT group improved in comfortable walking speed and step length under single walking condition and PGID after training. DTT group also showed improvements in cognitive performance under both single and dual walking conditions, and in several motor function and daily life related scales, including motor score, FES, and PDQ-39. The STT group showed slight increased walking speed and step length but not cognitive performance if tested in dual-walking condition.
Our study showed that after both DTT and STT training, the comfortable walking speed improved, and the improvement was mainly due to the increase of step length. These results suggest that treadmill training can improve the gait of patients with PD no matter cognitive load is given or not. Previous studies showed that, after dual-task training, some gait parameters in the single-task condition improved, including speed, step length, achieved walking distance35,36,37, but not cadence or step length variability35,36,38. A systemic study with patients of PD showed that the DTT training group demonstrated significantly increased single-task gait speed and stride length when compared to the controls (participating in general exercise)37,39,40. Our study compared the effect of DTT training with STT training and showed similar improvement in gait parameters, suggesting that the training effect was possibly mainly from treadmill training, and DTT training did not sacrifice the beneficial impact of treadmill training on self-selected walking. The mechanism could involve treadmills providing constant-paced cues via the proprioceptive information generated by the belt movement, to foster consistent stride durations41,42, which in turn adjust the relationship between stride length and stride time.
Our study did not show the training effect on gait speed when assessed under the fastest walking speed. It is possibly due to the fact that the fastest speed walking is not a natural activity in daily life. Individuals with PD might use cortical control to override gait control during the fastest speed walking test. Thus, the impaired gait automaticity might be compensated which makes this test not sensitive to the PD patients. Comfortable walking speed might be a better indicator of daily living functions such that clinical functional walking test ( e.g. 6 min walking test ) used a comfortable walking speed43.
Our study showed that the walking speed under dual walking test condition improved in STT group. However, this should not be interpreted as the STT training could improve dual walking test performance better than DTT training. While tested in dual walking test condition, the cognitive composite score decreased in STT group, suggesting a shift of attention occurred in this group. The plausible explanation is that the improvement of walking speed under dual walking test condition was under the cost of cognitive performance rather than the overall improvement.
We found that there was no significant improvement in step length CV and walking speed CV in individuals with PD after 8 weeks of training. Although there is a downward trend, the lack of significance may be caused by several factors. Firstly, PD is a progressive neurological disorder characterized by motor and cognitive impairments, which can make significant changes in gait parameters challenging to achieve within a relatively short training period. Eight weeks may not be sufficient time to observe substantial improvements in these specific measures. Another factor could be the complexity of dual-task training itself. While DTT aims to improve both cognitive and motor functions, the simultaneous engagement in cognitive tasks and walking might initially increase gait variability as participants adapt to the dual-task demands. Over time, this adaptation could stabilize, but the short duration of the study may not have allowed sufficient time for these adaptations to fully manifest as significant improvements. Moreover, the sensitivity of the outcome measures used to detect changes in gait variability might also play a role. While the GAITRite system is a robust tool for measuring gait parameters, subtle improvements in gait variability might require more sensitive or specific assessment tools to detect. Lastly, a trend towards improvement indicated that with a longer training period or a larger sample size, significant improvements might have been observed. Future studies with extended training durations and larger cohorts could provide more definitive evidence of the benefits of DTT on gait variability in PD patients.
In terms of cognitive function, our study found that only the DTT group showed improvement in composite scores. The improvement of cognitive function not only showed in single cognitive task condition but also in dual walking test condition as well.
There are very limited previous studies that evaluate the effect of DTT on cognitive function in individuals with PD. Our previous study demonstrated that cognitive-cycling training could improve cognitive function22. Research by Jacob J. Sosnoff (2017) found that individuals with multiple sclerosis showed a trend for the dual-task training group to outperform the control group on visuospatial memory and gait speed44. Similarly, Hagovska and Olekszyova (2016) found that dual-task training improved cognitive functions and gait parameters in stroke survivors45. These findings suggest that dual-task training can be effective across populations with neurological impairments.
In older adults, interventions combining virtual reality-augmented treadmill training have been shown to reduce fall risk, improve mobility, and enhance cognitive function17,46. Valenzuela et al. studied the effects of 20 sessions of mixed cognitive and dual-task training on individuals with PD and found a trend toward improvement, though no significant changes in cognitive performance were observed47. This lack of significant findings could be attributed to differences in assessment methods. Valenzuela et al. used the Frontal Assessment Battery and the Trail Making Test (parts A and B), whereas our study used a composite score from a spatial memory task, which controlled for speed-accuracy trade-offs and may be more sensitive in detecting changes in executive function.
Our study is novel that out study assessed cognitive function not only under single-task conditions but also during dual-task walking. Testing cognitive function during dual-task conditions can help avoid the compensatory effect of task prioritization. As previously mentioned, the cognitive-walking paradigm frequently occurs in community walking. DTT aligns with this principle by integrating cognitive tasks with walking, simulating real-world scenarios where individuals must manage cognitive demands while walking, such as navigating complex environments or engaging in conversations. Improvement in cognitive function during walking could provide clinically meaningful benefits for community mobility.
The neurophysiological mechanism for dual-task training to be more effective than Single-task training in cognitive function cannot be attributed to the resource relocation of dual tasks since our research results showed that DTT can enhance cognitive function without affecting walking ability compared with the STT group. One possible mechanism could be due to that dual-task training is more powerful to activate multiple brain regions48. Wu et al. found that when performing dual task training compared with performing a single task training, PD patients are activated on both sides of the anterior cuneiform lobes49. Szameitat et al. found that cortical areas of the posterior lateral prefrontal cortex along with the inferior frontal sulcus and middle frontal gyrus are involved in the co-ordination and re-organisation of the processing of two concurrent tasks50. PD patients are believed to require more brain processing resources to compensate for basal ganglia dysfunction when performing dual tasks51. The cognitive walking training might allow PD patients more chances to activate these dual-task related brain areas and, thus, improve cognitive function without compromising their walking function. The findings from our study suggest that DTT can significantly improve both motor and cognitive functions in individuals with PD. This supports the integration of DTT into standard rehabilitation programs for PD, providing a more holistic approach that addresses the complex needs of these patients. Clinicians can utilize DTT as a targeted intervention to enhance gait stability and safety in daily activities or maintain cognitive functions in PD patients. We will further investigate the long-term effects of DTT to determine the sustainability of the observed benefits over time. Longitudinal research will provide insights into how DTT can be integrated into ongoing management plans for PD. Besides, while our study focused on PD patients without cognitive impairments in the study, future research should explore the effects of DTT on those with varying degrees of cognitive decline. This would help to generalize the findings and potentially broaden the applicability of DTT in the PD population. Additionally, the detail discussion of the brain mechanism for DTT to be superior than STT is beyond the scope of current research and is suggested in future studies.
In contrast to the DTT group, STT group did not show improvement in cognitive function. Previous studies showed inconsistent results after single task exercise training on cognitive function. Cruise et al. (2011) found that 12- week exercise training of the experimental group did not result in significant difference of their cognitive function from the control group52. Other studies showed improved cognitive function after exercise training53,54,55. The inconsistency might be due to different assessment tools used, patient selection, exercise types, and cognitive test used.
One may suggest that the control group should also receive single cognitive training. However, we used single treadmill training as the control because it is a very common form of rehabilitation. Adding single cognitive training to the control would sacrifice the equivalent total training time. It is believed that dual-task training is not merely the sum of two single trainings, as dual-task training involves resource allocation and bottleneck theories, among others. Our study demonstrates that dual-task training can yield more beneficial effects compared to conventional single treadmill training within the same duration. Future research should explore the optimal sequence of cognitive, motor, and combined training in different study designs.
Our study found that PGIC improved in both STT and DTT group after training, and the post training PGIC was better in DTT group than STT group. In UPDRS-III, FES, and PDQ-39, only DTT group showed significant improvement after training. These suggested that the dual cognitive-walking training effects could translate to fall improvement, patients’ subjective feeling, and quality of life. This might be due to dual cognitive-walking training improved the ability to coordinate different interfering tasks which is a crucial ability for everyday life. Herman et al. reported that six weeks of single treadmill training improved the scores of UPDRS-III and PDQ-3956, whereas our study did not find significant improvement in STT group. The difference is possibly due to the disease severity. In Herman et al’s study, the initial score of UPDRS-III were 29, whereas in our study it was around 11 for both groups. The higher score means more severe in symptom which suggested our subjects were in earlier stage than those in Herman et al’s study. It is possible that single treadmill training is not powerful enough for early-stage PD patients.
In terms of fear of fall, Delbaere et al. suggested the cut-off point of FES was 23, that a score greater than 23 indicated a high degree of fear of falling57, In our study, although DTT group significantly decreased the FES score to 26 after DTT training, it was still greater than 23, suggesting the patients were fear of falling. Fall intervention of patients with PD might require further training or incorporation with other fall prevention programs that are suggested to be explored in future studies.
Our approach has some inherent potential limitations. First, The PD patients recruited in this study were of mild to moderate severity and were evaluated and trained under the medication status, so the results could not be inferred to more severe PD patients, and the performance under medication withdrawal state. Second, the current study focuses on participants with PD who do not have cognitive impairments, so the training may not directly apply to those with cognitive impairments. Since cognitive impairments are common as the disease progresses, it remains unclear whether this training could influence the long-term progression of cognitive decline. Future studies with different designs are suggested to address this issue. Third, our data may not offer sufficient insights into the optimal training duration, despite conducting midterm measurements at four weeks. Future studies with a longitudinal design are recommended to explore this aspect more comprehensively.
Conclusion
This study concludes that treadmill training with or without cognitive load could improve walking ability in PD patients. Only dual cognitive-walking treadmill training could improve cognitive function without trade off on walking ability. The effect of dual cognitive-walking treadmill training could translate to better motor function, patients’ subjective feeling, and quality of life possibly because it allows more practice of cognitive walking, which is an essential activity in everyday life. The underlying brain mechanism should be explored in future studies of different design.
Data availability
The data that support the findings of this study are available on request from the corresponding author, Ya-Ju, Chang.
References
Kalia, L. V. & Lang, A. E. Parkinson’s disease. Lancet 386, 896–912 (2015).
de Lau, L. M. & Breteler, M. M. Epidemiology of Parkinson’s disease. Lancet Neurol. 5, 525–535 (2006).
O’Sullivan SB, S. T. in Parkinson’s Disease (ed O’Sullivan SB) 853–856 (F.A. Davis, Philadelphia, 2007).
Duncan, R. P. & Earhart, G. M. Measuring participation in individuals with Parkinson disease: Relationships with disease severity, quality of life, and mobility. Disabil. Rehabil. 33, 1440–1446 (2011).
Hausdorff, J. M., Cudkowicz, M. E., Firtion, R., Wei, J. Y. & Goldberger, A. L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 13, 428–437 (1998).
Bello, O. et al. The effects of treadmill or overground walking training program on gait in Parkinson’s disease. Gait Posture 38, 590–595 (2013).
Cakit, B. D., Saracoglu, M., Genc, H., Erdem, H. R. & Inan, L. The effects of incremental speed-dependent treadmill training on postural instability and fear of falling in Parkinson’s disease. Clin. Rehabil. 21, 698–705 (2007).
Schlick, C. et al. Visual cues combined with treadmill training to improve gait performance in Parkinson’s disease: A pilot randomized controlled trial. Clin. Rehabil. 30, 463–471 (2016).
Wu, T. et al. Attention to automatic movements in Parkinson’s disease: Modified automatic mode in the striatum. Cereb. Cortex 25, 3330–3342 (2015).
Wu, T. & Hallett, M. A functional MRI study of automatic movements in patients with Parkinson’s disease. Brain 128, 2250–2259 (2005).
Rowe, J. et al. Attention to action in Parkinson’s disease: Impaired effective connectivity among frontal cortical regions. Brain 125, 276–289 (2002).
Parker, K. L., Lamichhane, D., Caetano, M. S. & Narayanan, N. S. Executive dysfunction in Parkinson’s disease and timing deficits. Front. Integr. Neurosci. 7, 75 (2013).
Yogev-Seligmann, G., Hausdorff, J. M. & Giladi, N. The role of executive function and attention in gait. Mov. Disord. 23, 329–342; quiz 472 (2008).
Pantelis, C. et al. Frontal-striatal cognitive deficits in patients with chronic schizophrenia. Brain 120(Pt 10), 1823–1843 (1997).
Lally, H. et al. Association between motor subtype and visuospatial and executive function in mild-moderate Parkinson disease. Arch. Phys. Med. Rehabil. 101, 1580–1589 (2020).
Lin, Y. P. et al. The executive-function-related cognitive-motor dual task walking performance and task prioritizing effect on people with Parkinson’s disease. Healthcare 11, 567 (2023).
Dorfman, M. et al. Dual-task training on a treadmill to improve gait and cognitive function in elderly idiopathic fallers. J. Neurol. Phys. Ther. 38, 246–253 (2014).
Jones, D. et al. Everyday walking with Parkinson’s disease: Understanding personal challenges and strategies. Disabil. Rehabil. 30, 1213–1221 (2008).
Mirelman, A. et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): A randomised controlled trial. Lancet 388, 1170–1182 (2016).
Rabinovici, G. D., Stephens, M. L. & Possin, K. L. Executive dysfunction. Continuum (Minneap Minn) 21, 646–659 (2015).
Gelb, D. J., Oliver, E. & Gilman, S. Diagnostic criteria for Parkinson disease. Arch. Neurol. 56, 33–39 (1999).
Hsiu-Chen, C. et al. The effects of dual-task in patients with Parkinson’s disease performing cognitive-motor paradigms. J. Clin. Neurosci. 72, 72–78 (2020).
Chang, H. C. et al. An 8-week low-intensity progressive cycling training improves motor functions in patients with early-stage Parkinson’s disease. J. Clin. Neurol. 14, 225–233 (2018).
Brauer, S. G. & Morris, M. E. Can people with Parkinson’s disease improve dual tasking when walking?. Gait. Posture 31, 229–233 (2010).
Tomlinson, C. L. et al. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 25, 2649–2653 (2010).
Webster, K. E., Wittwer, J. E. & Feller, J. A. Validity of the GAITRite walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 22, 317–321 (2005).
Yogev-Seligmann, G., Giladi, N., Brozgol, M. & Hausdorff, J. M. A training program to improve gait while dual tasking in patients with Parkinson’s disease: A pilot study. Arch. Phys. Med. Rehabil. 93, 176–181 (2012).
Shulman, L. M. et al. The clinically important difference on the unified Parkinson’s disease rating scale. Arch. Neurol. 67, 64–70 (2010).
Dewan, N. & MacDermid, J. C. Fall Efficacy Scale-International (FES-I). J. Physiother. 60, 60 (2014).
Peto, V., Jenkinson, C. & Fitzpatrick, R. Determining minimally important differences for the PDQ-39 Parkinson’s disease questionnaire. Age Ageing 30, 299–302 (2001).
Guy, W. ECDEU Assessment for Psychopharmacology, Revised Edition. (Rockville, MD., 1976).
Busner, J. & Targum, S. D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry (Edgmont (Pa. : Township)) 4, 28–37 (2007).
Springer, S. et al. Dual-tasking effects on gait variability: The role of aging, falls, and executive function. Mov. Disord. 21, 950–957. https://doi.org/10.1002/mds.20848 (2006).
Zanardi, A. P. J. et al. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 11, 752 (2021).
Wollesen, B. et al. A feasibility study of dual-task strategy training to improve gait performance in patients with Parkinson’s disease. Sci. Rep. 11, 12416 (2021).
Conradsson, D. et al. The effects of highly challenging balance training in elderly with Parkinson’s disease: A randomized controlled trial. Neurorehabil. Neural Repair. 29, 827–836 (2015).
Fok, P., Farrell, M. & McMeeken, J. The effect of dividing attention between walking and auxiliary tasks in people with Parkinson’s disease. Hum. Mov. Sci. 31, 236–246 (2012).
Canning, C. G., Ada, L. & Woodhouse, E. Multiple-task walking training in people with mild to moderate Parkinson’s disease: A pilot study. Clin Rehabil 22, 226–233 (2008).
Fok, P., Farrell, M. & McMeeken, J. Prioritizing gait in dual-task conditions in people with Parkinson’s. Hum. Mov. Sci. 29, 831–842 (2010).
Mirelman, A. et al. Virtual reality for gait training: Can it induce motor learning to enhance complex walking and reduce fall risk in patients with Parkinson’s disease?. J. Gerontol. A Biol. Sci. Med. Sci. 66, 234–240 (2011).
Frenkel-Toledo, S. et al. Treadmill walking as an external pacemaker to improve gait rhythm and stability in Parkinson’s disease. Mov. Disord. 20, 1109–1114 (2005).
Bello, O., Marquez, G., Camblor, M. & Fernandez-Del-Olmo, M. Mechanisms involved in treadmill walking improvements in Parkinson’s disease. Gait Posture 32, 118–123 (2010).
Chuang, C.-Y., Lin, S.-Y., Li, M.-H., Chang, Y.-J. & Hsu, M.-J. Six-minute walk test in community-dwelling older adults: Treadmill versus corridor walking distances. Top. Geriatr. Rehabil. 35, 266–272. https://doi.org/10.1097/tgr.0000000000000243 (2019).
Sosnoff, J. J. et al. Dual task training in persons with Multiple Sclerosis: A feasability randomized controlled trial. Clin. Rehabil. 31, 1322–1331. https://doi.org/10.1177/0269215517698028 (2017).
Hagovska, M. & Olekszyova, Z. Impact of the combination of cognitive and balance training on gait, fear and risk of falling and quality of life in seniors with mild cognitive impairment. Geriatr. Gerontol. Int. 16, 1043–1050. https://doi.org/10.1111/ggi.12593 (2016).
Mirelman, A. et al. V-TIME: A treadmill training program augmented by virtual reality to decrease fall risk in older adults: study design of a randomized controlled trial. BMC Neurol. 13, 15 (2013).
San Martin Valenzuela, C., Moscardo, L. D., Lopez-Pascual, J., Serra-Ano, P. & Tomas, J. M. Effects of dual-task group training on gait, cognitive executive function, and quality of life in people with Parkinson disease: Results of randomized controlled DUALGAIT trial. Arch. Phys. Med. Rehabil. 101, 1849–18561841 (2020).
Swartz, J., Scholl, J., McNamara, C. & Kott, A. Is live face-to-face UPDRS part III training more effective than remote training methodology in Parkinson’/INS; s disease clinical trials?. J. Neurol. Sci. 333, e136 (2013).
Wu, T. & Hallett, M. Neural correlates of dual task performance in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 79, 760–766 (2008).
Szameitat, A. J., Lepsien, J., von Cramon, D. Y., Sterr, A. & Schubert, T. Task-order coordination in dual-task performance and the lateral prefrontal cortex: An event-related fMRI study. Psychol. Res. 70, 541–552 (2006).
Tan, J., Wu, S., Xu, L., Wang, L. & Chen, A. Prefrontal cortex with executive functions involved in dual-task performance. Adv. Psychol. Sci. 21, 2127 (2013).
Cruise, K. E. et al. Exercise and Parkinson’s: Benefits for cognition and quality of life. Acta Neurol. Scand. 123, 13–19 (2011).
Silveira, C. R. A., Roy, E. A., Intzandt, B. N. & Almeida, Q. J. Aerobic exercise is more effective than goal-based exercise for the treatment of cognition in Parkinson’s disease. Brain Cogn. 122, 1–8 (2018).
McKee, K. E. & Hackney, M. E. The effects of adapted tango on spatial cognition and disease severity in Parkinson’s disease. J. Mot. Behav. 45, 519–529 (2013).
Pompeu, J. E. et al. Effect of Nintendo Wii-based motor and cognitive training on activities of daily living in patients with Parkinson’s disease: A randomised clinical trial. Physiotherapy 98, 196–204 (2012).
Herman, T., Giladi, N., Gruendlinger, L. & Hausdorff, J. M. Six weeks of intensive treadmill training improves gait and quality of life in patients with Parkinson’s disease: A pilot study. Arch. Phys. Med. Rehabil. 88, 1154–1158 (2007).
Delbaere, K. et al. The Falls Efficacy Scale International (FES-I) A comprehensive longitudinal validation study. Age Ageing 39, 210–216 (2010).
Acknowledgements
This study was supported by the National Science and Technology Council, Taiwan (NSTC 111-2314-B-182-035-MY3, and 112-2622-8-003-005-SP), Chang Gung Medical Foundation (CMRPD1M0231), and Healthy Aging Research Center, Chang Gung University (EMRPD1M0411).
Author information
Authors and Affiliations
Contributions
YL, IL, HCC, and YC: Conceptualization. IL, WC, and YC: validation. YL, IL, WC, HCC, and YC: formal analysis. RC, CL, HCC, HLC, YL, and YC: investigation. IL, WC, and YC: data curation. YL, and YC writing—original draft preparation. All authors contributed to the development of the methodology and have reviewed, edited, and approved the final manuscript.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lin, YP., Lin, II., Chiou, WD. et al. Optimizing rehabilitation strategies in Parkinson’s disease: a comparison of dual cognitive-walking treadmill training and single treadmill training. Sci Rep 14, 25210 (2024). https://doi.org/10.1038/s41598-024-75422-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-75422-0
Keywords
This article is cited by
-
Effects of a gait training program with the Fisior® sequential square mat on balance and gait in patients with Parkinson’s disease: a randomized clinical trial
BMC Complementary Medicine and Therapies (2026)
