
Abstract
In this research, we investigated whether secondhand smoking (SHS) increases the possibility of hypertension. We used data from the Shaanxi baseline survey of the Regional Ethnic Cohort Study in Northwest China (RECS). Active smoking and SHS were determined by questionnaires. Hypertension was defined as self-reported or objectively measured. Multivariable logistic regression model was performed to estimate the risk of hypertension under active smoking and SHS. Compared to never-smokers, exposure to SHS had a 9% (P = 0.005) higher possibility of hypertension. The adjusted OR for exposure time of ≤ 3 h/week, 3–12 h/week, and > 12 h/week were 1.03 (P = 0.545), 1.10 ( P = 0.040), and 1.15 (P = 0.015), respectively. The adjusted OR for frequency of SHS of 1–2 times/week, 3–5 times/week, and nearly every day were 0.94 (P = 0.421), 1.01 (P = 0.846), and 1.14 (P < 0.001), respectively. Compared to smokers, additional exposure to SHS had a more than threefold increased possibility of having hypertension. The adjusted OR for hypertension was 1.07 (P = 0.254), and 1.23 (P = 0.007) in only smokers and smokers with SHS, respectively. Our study provided evidence that SHS could be a risk factor for hypertension, and additional exposure of active smokers to SHS significantly increases the possibility of hypertension. Reducing the frequency or time of SHS may be effective in preventing hypertension.
Similar content being viewed by others

Introduction
Hypertension is a systemic ailment characterized by elevated arterial pressure, that not only poses a significant risk for many non-communicable diseases but also ranks as the foremost preventable cause of premature death worldwide1,2,3. According to a global study of individuals aged 30 to 79 from 1990 to 2019, the incidence of hypertension has escalated twofold over the past three decades, resulting in a huge burden of disease worldwide4. Although the heritability of blood pressure (BP) is estimated to be 30–50%, and 31–68% of the BP variation in the population may be determined by genes, the clustering effect of genetic loci had limited its role in hypertension prevention5,6,7. Therefore, modifiable lifestyle factors, which are also important factors causing hypertension, are crucial in the prevention, management, and treatment of hypertension.
SHS, also known as environmental tobacco smoke or passive smoking, encompasses the unintentional inhalation of both mainstream and side-stream smoke emanating from active smokers8. It contains more than 7,000 chemicals, including more than 250 known toxic substances and 69 teratogenic, carcinogenic, and mutagenic substances9. Worldwide, one-third of adults never smokers are exposed to SHS, causing more than 600 thousand deaths in 200410,11. In 2019, it increased to 7.7 million12. Previous studies have demonstrated that SHS has several adverse health effects on adults and children, including cardiovascular disease, atrial fibrillation, low birth weight, and sudden infant death13,14,15. However, the relationship between SHS and hypertension is still controversial. For instance, A study conducted in South Korea demonstrated that SHS increased the risk of stroke, angina, and hypertension16. Nevertheless, a National Health and Nutrition Examination Survey (NHANES) study demonstrated that SHS reduced the risk of hypertension in the male population17. The link between SHS and hypertension needs to be further clarified.
Notably, research on the health effects of SHS has drawn the government’s great deal of attention to the importance of tobacco control in preventing causes of disease and disability18,19,20. To diminish SHS exposure, some countries including China have implemented active smoking bans21,22,23, but the burden of disease caused by tobacco has not decreased and more than 90% of the world’s population still lives in countries without full smoke-free public health coverage regulations10,24. SHS remains an important contributor to the high disease burden. Besides, previous studies on SHS have focused on vulnerable groups and have not provided evidence to support which characteristic groups should be focused on when implementing tobacco control measures in the population25,26,27. Whereas people are often exposed to both active smoking and SHS, previous researches have been lacking on the combined effects of SHS and active smoking on hypertension. Furthermore, China has more than 300 million smokers, nearly a third of the world’s total. More than 700 million never-smokers in China, including about 180 million children, are exposed to secondhand smoke (SHS) at least once a day during the week. Based on this, our study used Shaanxi, a representative province in northwest China, to investigate the correlation between SHS and the risk of hypertension, the comprehensive influences of SHS and active smoking on hypertension, and identify the characteristic groups that should be focused on when controlling SHS to promote coordinated public health actions for improving the effective enforcement of smoke-free bans, whilst concomitantly curb hypertension and its associated medical costs. Our study may benefit from similar studies and the burden of hypertension in China.
Methods
Study design and population
The Regional Ethnic Cohort Study in Northwest China (RECS) is a prospective observational study conducted in 13 regions across five northwestern provinces of northwest China, namely Shaanxi, Gansu, Qinghai, Ningxia Hui Autonomous Region, and Xinjiang Uygur Autonomous Region. The study aims to investigate the lifestyle habits of Chinese residents and their relationship with health and disease, with the ultimate goal of promoting health. The RECS consists of 118,572 participants aged 35–74 years. More details of the RECS have been published elsewhere25.In brief, the first wave of RECS surveys, which included baseline assessments on socio-economic, demographic, basic information, and health-related lifestyle factors, was conducted between June 2018 and May 2019 by trained health workers.
In this study, we included 48,025 subjects from Shaanxi Province. In the analysis of SHS and hypertension risk, we selected never-smokers to eliminate the effect of active smoking on hypertension. Then we excluded participants who met any of the following criteria: (1) missing values for SHS; (2) missing values for both reported and measured hypertension; (3) under the age of 18; and (4) pregnant women. Finally, 30,778 subjects were included. In the analysis of the combined effect of active smoking and SHS on hypertension risk, subjects with missing active smoking data were excluded from all participants. Other exclusion criteria are the same as above. Finally, 34,738 subjects were included. The study flowchart is presented in Fig. 1 and Supplementary Fig. S1 online.

Flowchart of analyzing the relationship between SHS and hypertension.
Measures
In the initial survey questionnaire administered by the RECS, respondents were queried about the frequency of smoking and their exposure to SHS. For SHS, subjects were asked two questions. One was how many days per week have you been exposed to SHS in your home from people you live with during the past year? The other one was how many days per week have you typically been exposed to SHS from other smokers at work or in a public place during the past year? For our investigation, SHS was operationalized as exposure to SHS for more than one day per week, irrespective of the setting (i.e. at home, at work or in public places). The frequency of smoking in the past and present was divided into never, occasional smoking, smoking most days, and smoking in everyday categories. In our study, active smoking was defined as past or present smoking.
Our study’s primary outcome was hypertension, which was defined as self-reported or objectively measured. In our study, individuals who responded “yes” to the question “Have you been diagnosed with high hypertension” were classified as self-reported hypertensive. Additionally, the trained researchers recorded the participants’ systolic and diastolic blood pressure in the left arm. During the test, participants were measured twice at a five-minute interval, in a quiet and appropriate temperature environment. If the discrepancy between the two measurements exceeded 5 mmHg, a third measurement was taken, and the average of the two measurements with differences within 5 mmHg was used for analysis. Consistent with the Chinese Guidelines for the Management of Hypertension, We defined mean systolic blood pressure ≥ 140 mmHg or mean diastolic blood pressure ≥ 90 mmHg as measured hypertension26.
Drawing on our prior knowledge and relevant literature16,27, we identified a set of covariates that we deemed might confound the association between SHS and hypertension risk in our study. Specifically, we controlled for the following variables: age, sex (male and female), nationality (Han and other), body mass index (BMI) (< 18.5, 18.5–23.9, 24-27.9, and ≥ 28), level of education (primary school and below, middle school, and university and above), marriage status (married, single, divorced, and others), occupation status (unemployed, employed), household income (<¥10000, ¥10000-¥50000, ¥50000-¥100000, and >¥100000), drinking status (drinker and non-drinker), and physical activity. The general demographic and behavioral lifestyle variables mentioned above were collected through baseline questionnaires. BMI was computed by dividing weight (kg) by height (meters) squared (kg/m2). Physical activity was calculated by multiplying the metabolic equivalent of a particular type of physical activity by the number of hours spent per day28.
Statistic analysis
Baseline Characteristics of participants were described according to whether they were exposed to SHS or had hypertension, means ± standard deviations (SDs) and numbers (percentages) were used to present continuous and categorical variables, respectively. T-test and Pearson Chi-square test were used to compare the distribution characteristics of exposure and outcome indicators in the study population.
To estimate the relationship between SHS and hypertension, we employed multivariable logistic regression models to calculate OR and 95% CI. We instructed two models: Model 1 was a crude model that adjusted for age and sex; Model 2 was further adjusted for other general demographic and behavioral lifestyle characteristics. The fully adjusted model was fitted using restricted cubic spline regression (RCS) as a continuous variable of weekly SHS exposure time to further explore the dose-response relationship between SHS and hypertension29.
To ensure the validity of the study, we used the ROC curve to test the fit of multivariable logistic regression and further performed the effect correction test. In addition, based on the interaction results and to further explore the stability and specificity of the relationship between SHS and hypertension, we performed subgroup analyses based on baseline age, sex, household income, level of education, drinking status, BMI, occupation status, and marital status. We also performed multiple imputations for missing covariate data nationality (0.29% missing), household income (2.63% missing), level of education (0.29% missing), drinking status (0.17% missing), BMI (0.55% missing), physical activity (1.42% missing), marital status (0.54% missing), and drinking status (1.32% missing) to evaluate the statistical effect of missing data on the association between SHS and hypertension using the Fully Conditional Specification (FCS) method30. In brief, we generated twenty imputed datasets and combined the parameters of each imputed dataset computed by the standard statistical procedure to obtain the final results. All statistical analyses were conducted using SAS 9.4 software. P < 0.05 (two-tailed) was set as the statistical significance level.
Ethics approval and consent to participate
The Human Research Ethics Committee of Xi’an Jiaotong University (No: XJTU2016-411) approved this study and our study was performed in accordance with relevant regulations. All participants filled out informed consent forms before participating.
Results
Characteristics of subjects used to study the relationship between SHS and hypertension were presented in Table 1. 30,778 subjects were included in our study, with an average age of 50.60 (12.87) years. The majority of participants were female (80.10%) and of Han nationality (99.18%). In terms of lifestyle factors, 78.15% were drinkers and 27.82% were employed. Most participants were married (87.69%), had junior and senior high school education (37.60%), and had an annual household income of 10,000–50,000 (51.83%). The prevalence of overweight and obesity was 33.50% and 10.22%, respectively. About 29.89% of participants reported SHS and 29.17% reported hypertension. Participants who reported SHS were younger on average than those without exposure, and SHS was more common among women, those with obesity, ethnic minorities, those who were single, those with median household income, and those who were drinkers. Hypertension prevalence was higher in divorced families (40.28%), while single families had the lowest prevalence (12.69%). Characteristics of subjects used to explore the combined effect of SHS and active smoking on hypertension were presented in Supplementary Table S1 online.
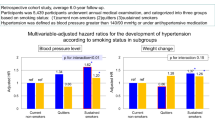
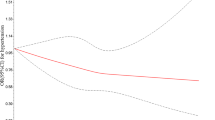
Based on Table 2, we found that SHS was significantly associated with an increased possibility of hypertension, with an adjusted OR of 1.09 (95% CI:1.03–1.16, P = 0.005) after adjusting for relevant covariates. Furthermore, we observed a significant dose-response relationship between the possibility of hypertension and the frequency and time of SHS, as well as the duration of exposure (as shown in Fig. 2). Supplementary Fig. S2 online showed the area under the ROC curve of the multivariable logistic model for examining the relationship between SHS and hypertension was 0.73. It could be considered that the fitting effect of the model was better. Based on Supplementary Table S2 online, we found sex affected the relationship between SHS and hypertension. Additional subgroup analysis presented in Supplementary Fig. S3 online presented there was a statistically significant trend between SHS and the possibility of hypertension among certain groups. Specifically, the trend was significant among middle age, females, non-drinkers, employed, middle-income, moderately educated, and married individuals. However, other groups observed no significant difference. The results of multiple imputation analyses were presented in Supplementary Table S3 online. It also supported the finding that SHS was associated with a higher possibility of hypertension, and the results remained robust and unchanged.

Dose-response relationship between time of SHS and hypertension in restricted cubic splines among participants. SHS, secondhand smoking; CL, confidence limit. Curves were fitted as a smooth term using a restricted cubic spline with 5 knots (5%, 25%, 50%, 75%, 95%). The reference value was the 2.5th percentile of weekly exposure to SHS. Models were adjusted for sex, age, nationality, BMI, degree of education, marital status, occupation, household income, drinking status, and physical activity.
Table 3 presented the combined effect of SHS and active smoking on hypertension, which showed that current smokers with additional exposure to SHS remarkably increased the possibility of hypertension prevalence. Specifically, the hypertension OR for never-smokers with SHS exposure was 1.08 (95% CI, 1.02–1.15, P = 0.010), while the OR for smokers without SHS was 1.07 (95% CI, 0.96–1.19, P = 0.254). However, when smokers were exposed to additional SHS, the possibility of hypertension increased to 1.23 (95% CI, 1.06–1.43, P = 0.007). Supplementary Fig. S4 online showed the area under the ROC curve of the multivariable logistic model was 0.73, indicating that the model had a good fitting. Supplementary Table S4 presented the interaction between SHS, smoking and hypertension and it suggested there was no effect modification.
Discussion
Any level of SHS exposure is harmful31. In this study, we observed a significant association between SHS and an increased possibility of hypertension. Subgroup analyses presented similar results in middle age, females, non-drinkers, employed, middle-income, moderately educated, and married individuals. We further found a dose-response relationship between the frequency and duration of SHS and the likelihood of the possibility of hypertension. More importantly, we found SHS exposure rather than active smoking was associated with a greater possibility of hypertension and a combined effect between SHS and active smoking on hypertension, with a more than threefold possibility when smokers have additional exposure to SHS. Our findings highlight the need for further improving the effective public health actions of smoke-free bans to reduce exposure to SHS and thereby decrease the burden of hypertensive disease.
Previous cohort studies with hypertension incidence as an endpoint have shown a similar positive correlation between SHS and hypertension risk32,33. Compared with never-smoked women, exposed to their husbands’ SHS had a 28% increased risk of hypertension34. Another prospective cohort study conducted in Korea showed that exposure to SHS displayed a 1.02-fold elevated risk of hypertension16. Furthermore, a national cross-sectional study from the US suggested that SHS contributed to the development of hypertension, with an adjusted odds of hypertension 1.038 (95% CI, 1.037, 1.040)17. Estimates of the increased risk of hypertension caused by SHS in this study are generally similar to a previously published study, with an adjusted OR of 1.09 (95% CI, 1.03 ~ 1.16) here among ever-smoked participants. Importantly, Research showed that children and adolescents with higher awareness of SHS had lower subsequent smoking behavior and lower risk of hypertension, implying we can reduce the health risks and disability of smoking by raising awareness about SHS35,36,37.
Notably, our study found that SHS, rather than active smoking, was more likely to increase the possibility of hypertension. Several previous epidemiological studies revealed that active smokers have the same or lower blood pressure levels than never-smokers38,39. Furthermore, the England Study also suggested that any independent chronic effect of active smoking on blood pressure is small40. The plausible reason for this phenomenon may be caused by the time of exposure. SHS persists in the air for a long time (1.4 h)41, long-term exposure to SHS can lead to damage to the endothelium of the blood vessels, and an increased inflammatory response, which increases the risk of hypertension42. Besides, exposure to SHS usually occurs in the workplace and at home, where poor ventilation often leads to longer and higher concentrations of exposure43. A study describing indoor air quality during sleep found that smokers’ bedrooms were found to have significantly higher levels of pollutants than never-smokers, showing the effect of SHS on indoor air quality deterioration44. In addition, previous studies have found that active smokers develop a tolerance to continuous nicotine stimulation and cotinine (a major metabolite of nicotine with a half-life of about 12 h) can cause peripheral vascular dilation, which is also an explanation for the lower blood pressure of active smokers45,46.
Previous studies have found sex differences, with women who smoked lightly appearing to have lower blood pressure levels, while SHS is associated with a higher risk of hypertension17,40. Research showed that light smoking was associated with lower body weight, whereas SHS had the opposite correlation47. BMI, which has well-established effects on hypertension may explain this phenomenon48. Compared to non-exposed women, women exposed to SHS had a higher serum total testosterone and free androgen index, which were associated with increased blood pressure49. In addition, exposure to SHS reduced female stamina and estrogen levels, which further increased the risk of hypertension and polycystic ovary syndrome50. Therefore, it is necessary to take steps to reduce the exposure of SHS in women, especially those who are pregnant.
Usually, SHS is predominantly a collective exposure, and individuals often have limited control over their exposure. Even smokers are at risk of SHS exposure. However, previous extensive knowledge explored in comprehensive studies or reviews mainly focused on the relationship between smoking and hypertension51,52,53. At present, there is still a lack of research on the combined effect between SHS and active smoking on hypertension. Our research filled this gap and revealed that additional exposure to SHS increased the 14% higher possibility of hypertension among smokers. This highlights the importance of avoiding SHS exposure to reduce the incidence of cardiovascular disease in smokers.
Additionally, our study demonstrated a dose-response relationship between the duration and frequency of SHS exposure and hypertension. This is similar to the outcomes of previous studies. Two cross-sectional investigations carried out in China proved that SHS was associated with the increased prevalence of hypertension, as well as a decrease in control rate, with a positive nonlinear dose-response relationship. Thus, reducing the frequency and duration of SHS exposure may be an effective strategy to control the prevalence of hypertension54,55.
Finally, we found a difference in the analysis of different age groups, with participants under 65 years showing an adverse relationship between SHS and the possibility of hypertension, which was inconsistent with previous studies54. It is may because middle-aged individuals are the main body of employment, and compared with older people, they are more exposed to SHS in the workplace. This is consistent with our observation that SHS increases the possibility of hypertension in the employed population. In the marriage groups, married individuals were more likely to develop hypertension. This may be related to the fact that married people have additional exposure to SHS at home. Besides, the detrimental effect of SHS on hypertension was more prominent in non-drinkers, middle-income, and moderately educated. One potential reason could be their low socioeconomic status56. This finding suggested that targeted intervention programs should focus on protecting these vulnerable groups from SHS exposure.
The potential mechanism of action of SHS on hypertension may be as follows. SHS exposes individuals to a higher concentration of toxic gas components, including nicotine and tar, than active smoking57 These components act as sympathetic stimulants, activating the central and peripheral nervous system and leading to increased heart rate, cardiac output, and blood pressure. Additionally, nicotine alters blood vessel activity, causing vascular remodeling and dysfunction that contribute to atherosclerosis58,59. Moreover, nicotine induces an increase in fat metabolism, leading to increased oxidation of atherogenic lipids and a decrease in high-density lipoprotein, while promoting the development of vascular endothelial injury and atherosclerosis60,61. Besides, SHS can also increase the risk of hypertension by increasing the number of red blood cells in the blood62. Carbon monoxide in tobacco enters the bloodstream, binding with hemoglobin and causing hypoxia, which increases the number of red blood cells and the viscosity of blood, accelerating plaque rupture and bleeding, all of which have a direct impact on high blood pressure60.
The study’s primary strength was its extensive sample size, which included individuals from a broad range of ages and residential areas in both urban and rural regions of Shaanxi province in northwest China. As a result, the study’s findings on the association between SHS and hypertension were more precise and representative of the population. Additionally, this was the first study to explore the combined effect of SHS and active smoking on hypertension among the whole population. Furthermore, our study further identified which characteristic populations should be focused on when preventing the harms of SHS. However, the current study had several limitations that should be taken into consideration.
Firstly, as a cross-sectional study design, it could only provide the hypothesis that SHS was a possible risk factor for hypertension without establishing a causal relationship. Therefore, Longitudinal cohort studies are needed to provide more conclusive evidence. Secondly, although we adjusted for some covariates in our study, there were other subsisting confounders, such as underlying risk of hypertension and family history of the disease. However, our study, based on a large multi-ethnic cohort in Northwest China, can still provide valuable information on the relationship between SHS and hypertension. Thirdly, our study used frequency and duration of exposure to SHS rather than serum nicotine concentrations. However, the approach we used to classify SHS exposure in our study has been used and validated in previous studies63. Fourthly, Hypertension was diagnosed as self-reported or objectively measured, ignoring the use of any antihypertensive medications. It may lead to certain deviations. Finally, the self-reported nature of exposure to SHS, limited to home and work environments, may lead to reporting and recall biases. Despite its limitations, our study provided a cost-effective and convenient way to prevent and control hypertension by reducing to exposure SHS.
In summary, Our study provided evidence that SHS could be a risk factor for hypertension. The dose-response relationship suggests that the Chinese government can reduce the risk of hypertension by reducing the frequency or duration of exposure to SHS in residents, particularly those under 65 years of age, women, non-drinkers, middle-income, moderately educated, and married. More importantly, active smoking combined with SHS exposure significantly increased the possibility of hypertension. Smoking-related disease burden and disability can be reduced by increasing the hazards of SHS. Our finding had an important revelation for public health interventions to prevent hypertension by reducing exposure to SHS.
Data availability
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Change history
28 November 2024
A Correction to this paper has been published: https://doi.org/10.1038/s41598-024-80582-0
References
Rudd, K. E. et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of Disease Study. Lancet. 395, 200–211. https://doi.org/10.1016/S0140-6736(19)32989-7 (2020).
Jin, M. et al. Passive smoking and insomnia in rural Chinese nonsmoking housewives: an environmental and genetic perspective. Environ. Int. 170, 107569. https://doi.org/10.1016/j.envint.2022.107569 (2022).
Fuchs, F. D. & Whelton, P. K. High blood pressure and Cardiovascular Disease. Hypertension. 75, 285–292. https://doi.org/10.1161/HYPERTENSIONAHA.119.14240 (2020).
Worldwide trends in. Hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 398, 957–980. https://doi.org/10.1016/S0140-6736(21)01330-1 (2021).
Munroe, P. B., Barnes, M. R. & Caulfield, M. J. Advances in blood pressure genomics. Circ. Res. 112, 1365–1379. https://doi.org/10.1161/CIRCRESAHA.112.300387 (2013).
Russo, A., Di Gaetano, C., Cugliari, G. & Matullo, G. Advances in the Genetics of Hypertension: the Effect of Rare variants. Int. J. Mol. Sci. 19, 688. https://doi.org/10.3390/ijms19030688 (2018).
Padmanabhan, S. & Dominiczak, A. F. Genomics of hypertension: the road to precision medicine. Nat. Rev. Cardiol. 18, 235–250. https://doi.org/10.1038/s41569-020-00466-4 (2021).
Ahijevych, K. & Wewers, M. E. Passive smoking and vascular disease. J. Cardiovasc. Nurs. 18, 69–74 (2003).
Soleimani, F., Dobaradaran, S., De-la-Torre, G. E., Schmidt, T. C. & Saeedi, R. Content of toxic components of cigarette, cigarette smoke vs cigarette butts: a comprehensive systematic review. Sci. Total Environ. 813, 152667. https://doi.org/10.1016/j.scitotenv.2021.152667 (2022).
Oberg, M., Jaakkola, M. S., Woodward, A., Peruga, A. & Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 377, 139–146. https://doi.org/10.1016/S0140-6736(10)61388-8 (2011).
Ma, C. et al. Global trends in the prevalence of secondhand smoke exposure among adolescents aged 12–16 years from 1999 to 2018: an analysis of repeated cross-sectional surveys. Lancet Glob Health. 9, e1667–e1678. https://doi.org/10.1016/S2214-109X(21)00365-X (2021).
Spatial Demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of Disease Study 2019. Lancet. 397, 2337–2360. https://doi.org/10.1016/S0140-6736(21)01169-7 (2021).
Wang, Y. T. et al. The Association between exposure to second-hand smoke and disease in the Chinese Population: a systematic review and Meta-analysis. Biomed. Environ. Sci. 36, 24–37. https://doi.org/10.3967/bes2023.003 (2023).
Ho, H., Ran, T. & Ji, X. Secondhand Smoking and Sudden Infant Death Syndrome: how can in Silico Pharmacokinetics and circulation models contribute? Front. Bioeng. Biotechnol. 9, 820404. https://doi.org/10.3389/fbioe.2021.820404 (2021).
Lin, G. M. et al. Secondhand tobacco smoke exposure, urine cotinine, and risk of incident atrial fibrillation: the multi-ethnic study of atherosclerosis. Prog Cardiovasc. Dis. 74, 38–44. https://doi.org/10.1016/j.pcad.2022.10.006 (2022).
Lee, W., Hwang, S. H., Choi, H. & Kim, H. The association between smoking or passive smoking and cardiovascular diseases using a bayesian hierarchical model: based on the 2008–2013 Korea Community Health Survey. Epidemiol. Health. 39, e2017026. https://doi.org/10.4178/epih.e2017026 (2017).
Akpa, O. M., Okekunle, A. P., Asowata, J. O. & Adedokun, B. Passive smoking exposure and the risk of hypertension among non-smoking adults: the 2015–2016 NHANES data. Clin. Hypertens. 27, 1. https://doi.org/10.1186/s40885-020-00159-7 (2021).
Guo, H. & Quan, G. Tobacco control in China and the road to Healthy China 2030. Int. J. Tuberc Lung Dis. 24, 271–277. https://doi.org/10.5588/ijtld.19.0106 (2020).
Toxværd, C. G., Pisinger, C., Lykke, M. B. & Lau, C. J. Making smoking history: temporal changes in support for a future smoking ban and increasing taxes in the general population of Denmark. Tob. Control. 32, 67–71. https://doi.org/10.1136/tobaccocontrol-2020-056067 (2023).
Willemsen, M. C. & Been, J. V. Accelerating tobacco control at the national level with the smoke-free Generation movement in the Netherlands. NPJ Prim. Care Respir Med. 32, 58. https://doi.org/10.1038/s41533-022-00321-8 (2022).
Burki, T. K. Stop-smoking services in the UK. Lancet Oncol. 21, 202. https://doi.org/10.1016/S1470-2045(20)30017-6 (2020).
Dyer, O. US to ban smoking in public housing. BMJ. 355, i6562. https://doi.org/10.1136/bmj.i6562 (2016).
Parry, J. China pushes ahead with ban on indoor smoking. BMJ 342, d1990. https://doi.org/10.1136/bmj.d1990. (2011)
Jaakkola, M. S. & Jaakkola, J. J. K. Impact of smoke-free workplace legislation on exposures and health: possibilities for prevention. Eur. Respir J. 28, 397–408 (2006).
Li, C. et al. Cohort Profile: Regional ethnic cohort study in Northwest China. Int. J. Epidemiol. 51, e18–e26. https://doi.org/10.1093/ije/dyab212 (2022).
Liu, J. Highlights of the 2018 Chinese hypertension guidelines. Clin. Hypertens. 26, 8. https://doi.org/10.1186/s40885-020-00141-3 (2020).
Chei, C. L., Loh, J. K., Soh, A., Yuan, J. M. & Koh, W. P. Coffee, tea, caffeine, and risk of hypertension: the Singapore Chinese Health Study. Eur. J. Nutr. 57, 1333–1342. https://doi.org/10.1007/s00394-017-1412-4 (2018).
Ainsworth, B. E. et al. Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc 43, 1575–1581. https://doi.org/10.1249/MSS.0b013e31821ece12 (2011).
Desquilbet, L. & Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 29, 1037–1057. https://doi.org/10.1002/sim.3841 (2010).
van Buuren, S. Multiple imputation of discrete and continuous data by fully conditional specification. Stat. Methods Med. Res. 16, 219–242 (2007).
Disparities in secondhand smoke exposure–United States. 1988–1994 and 1999–2004. MMWR Morb Mortal. Wkly. Rep. 57, 744–747 (2008).
Mahmud, A. & Feely, J. Effects of passive smoking on blood pressure and aortic pressure waveform in healthy young adults–influence of gender. Br. J. Clin. Pharmacol. 57, 37–43 (2004).
Keusch, S. et al. Tobacco smoke exposure in pulmonary arterial and thromboembolic pulmonary hypertension. Respiration. 88, 38–45. https://doi.org/10.1159/000359972 (2014).
Yang, Y. et al. Association of husband smoking with wife’s hypertension status in over 5 million Chinese females aged 20 to 49 years. J. Am. Heart Assoc. 6, e004924.https://doi.org/10.1161/JAHA.116.004924 (2017).
Levy, R. V. et al. Analysis of active and Passive Tobacco exposures and blood pressure in US children and adolescents. JAMA Netw. Open. 4, e2037936. https://doi.org/10.1001/jamanetworkopen.2020.37936 (2021).
Song, A. V., Glantz, S. A. & Halpern-Felsher, B. L. Perceptions of second-hand smoke risks predict future adolescent smoking initiation. J. Adolesc. Health. 45, 618–625. https://doi.org/10.1016/j.jadohealth.2009.04.022 (2009).
Hu, Z. et al. [Correlation between childhood hypertension and passive smoking before and after birth]. Wei Sheng Yan Jiu. 48, 751–756 (2019).
Liu, X. & Byrd, J. B. Cigarette smoking and subtypes of uncontrolled blood pressure among diagnosed hypertensive patients: paradoxical associations and implications. Am. J. Hypertens. 30, 602–609. https://doi.org/10.1093/ajh/hpx014 (2017).
Mikkelsen, K. L. et al. Smoking related to 24-h ambulatory blood pressure and heart rate: a study in 352 normotensive Danish subjects. Am. J. Hypertens. 10, 483–491 (1997).
Primatesta, P., Falaschetti, E., Gupta, S., Marmot, M. G. & Poulter, N. R. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension. 37, 187–193 (2001).
Lampos, S. et al. Real-time assessment of E-cigarettes and conventional cigarettes emissions: aerosol size distributions, mass and number concentrations. Toxics. 7, 45. https://doi.org/10.3390/toxics7030045 (2019).
Yuan, H. et al. The effects of second-hand smoke on biological processes important in atherogenesis. BMC Cardiovasc. Disord. 7, 1 (2007).
Carreras, G. et al. Burden of disease attributable to second-hand smoke exposure: a systematic review. Prev. Med. 129, 105833. https://doi.org/10.1016/j.ypmed.2019.105833 (2019).
Canha, N., Lage, J., Coutinho, J. T., Alves, C. & Almeida, S. M. Comparison of indoor air quality during sleep in smokers and non-smokers’ bedrooms: a preliminary study. Environ. Pollut. 249, 248–256. https://doi.org/10.1016/j.envpol.2019.03.021 (2019).
Benowitz, N. L., Jacob, P., Jones, R. T. & Rosenberg, J. Interindividual variability in the metabolism and cardiovascular effects of nicotine in man. J. Pharmacol. Exp. Ther. 221, 368–372 (1982).
Benowitz, N. L. & Sharp, D. S. Inverse relation between serum cotinine concentration and blood pressure in cigarette smokers. Circulation. 80, 1309–1312 (1989).
Noppa, H. & Bengtsson, C. Obesity in relation to smoking: a population study of women in Göteborg, Sweden. Prev. Med. 9, 534–543 (1980).
Zhou, Q. et al. BMI and risk of all-cause mortality in normotensive and hypertensive adults: the rural Chinese cohort study. Public. Health Nutr. 24, 5805–5814. https://doi.org/10.1017/S1368980021001592 (2021).
Li, J. et al. Effect of exposure to second-hand smoke from husbands on biochemical hyperandrogenism, metabolic syndrome and conception rates in women with polycystic ovary syndrome undergoing ovulation induction. Hum. Reprod. 33, 617–625. https://doi.org/10.1093/humrep/dey027 (2018).
Sanders, S. R., Cuneo, S. P. & Turzillo, A. M. Effects of nicotine and cotinine on bovine theca interna and granulosa cells. Reprod. Toxicol. 16, 795–800 (2002).
Luehrs, R. E. et al. Cigarette smoking and Longitudinal associations with blood pressure: the CARDIA Study. J. Am. Heart Assoc. 10, e019566. https://doi.org/10.1161/JAHA.120.019566 (2021).
Bowman, T. S., Gaziano, J. M., Buring, J. E. & Sesso, H. D. A prospective study of cigarette smoking and risk of incident hypertension in women. J. Am. Coll. Cardiol. 50, 2085–2092 (2007).
Carter, B. D. et al. Smoking and mortality–beyond established causes. N Engl. J. Med. 372, 631–640. https://doi.org/10.1056/NEJMsa1407211 (2015).
Wu, L. et al. Association between passive smoking and hypertension in Chinese non-smoking elderly women. Hypertens. Res. 40, 399–404. https://doi.org/10.1038/hr.2016.162 (2017).
Li, N. et al. Effects of passive smoking on hypertension in rural Chinese nonsmoking women. J. Hypertens. 33, 2210–2214. https://doi.org/10.1097/HJH.0000000000000694 (2015).
Weinberger, A. H. Socioeconomic status and Tobacco Use. Nicotine Tob. Res. 24, 805–806. https://doi.org/10.1093/ntr/ntac058 (2022).
Glantz, S. A. & Parmley, W. W. Passive smoking and heart disease. Epidemiology, physiology, and biochemistry. Circulation 83, 1–12. (1991).
Centner, A. M., Bhide, P. G. & Salazar, G. Nicotine in senescence and atherosclerosis. Cells. 9, 1035. https://doi.org/10.3390/cells9041035 (2020).
Gaemperli, O., Liga, R., Bhamra-Ariza, P. & Rimoldi, O. Nicotine addiction and coronary artery disease: impact of cessation interventions. Curr. Pharm. Des. 16, 2586–2597 (2010).
Ambrose, J. A. & Barua, R. S. The pathophysiology of cigarette smoking and cardiovascular disease: an update. J. Am. Coll. Cardiol. 43, 1731–1737 (2004).
Kershbaum, A., Bellet, S., Dickstein, E. R. & Feinbergl, J. Effect of cigarette smoking and nicotine on serum free fatty acids based on a study in the human subject and the experimental animal. Circ. Res. 9, 631–638 (1961).
Jo, W. K., Oh, J. W. & Dong, J. I. Evaluation of exposure to carbon monoxide associated with passive smoking. Environ. Res. 94, 309–318 (2004).
Khoramdad, M. et al. Association between passive smoking and cardiovascular disease: a systematic review and meta-analysis. IUBMB Life. 72, 677–686. https://doi.org/10.1002/iub.2207 (2020).
Acknowledgements
Data for this study came from the Regional Ethnic Cohort Study in Northwest China (RECS). We sincerely appreciate the efforts of every investigator involved in this work.
Funding
This work was supported by the Science and Technology Plan of Shaanxi Province [Grant Number:2023-CX-PT-47], the National Key Research and Development Program [Grant Number:2017YFC0907200, 2017YFC0907201], and the National Natural Science Foundation of China [Grant Number:82103944].
Author information
Authors and Affiliations
Contributions
BM, HY, SD, and SC designed the research. SC analyzed the data and wrote the paper. BM and SC contributed to the revision of the manuscript. JL, YH, HL, YW, BZ, KX, PY, HY, LZ, and SD provided additional interpretation of the data and results to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in Affiliation 1, which was incorrectly given as 'Department of Neurology, First Affiliated Hospital of Xi’an, Jiao Tong University, Xi’an, Shaanxi, China'. Full information regarding the corrections made can be found in the correction for this Article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cao, S., Liu, J., Huo, Y. et al. Secondhand smoking increased the possibility of hypertension with a significant time and frequency dose-response relationship. Sci Rep 14, 24950 (2024). https://doi.org/10.1038/s41598-024-76055-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76055-z
