
Abstract
Unilateral Nephrectomy is one of the most common treatments for surgical diseases of the kidney but often results in postsurgical acute kidney injury (AKI). In the current study, we aimed to investigate the risk factors for AKI in patients who have received Unilateral Nephrectomy. We retrospectively analysed 528 patients who underwent Unilateral Nephrectomy for different etiologies between January 2013 and December 2018 at the Affiliated Hospital of Qingdao University. We recorded the prevalence and severity of AKI, age, gender, diabetes, body mass index (BMI), hypertension, preoperative renal function, etiology, performed surgically, anaemia, albumin, coagulation, lactate dehydrogenase, nitrogen (BUN), and uric acid. Univariate and multivariate logistic regression analyses were used to investigate the predictors of AKI in patients with Unilateral Nephrectomy. Overall, 218 of the 528 patients (41.2%) developed AKI during their hospitalisation. Univariate analysis showed that AKI was significantly associated with gender (male, OR = 1.866, P = 0.001), overweight (OR = 2.19, P = 0.0002), and surgical approach (OR = 1.7, P = 0.018), while multivariate logistic regression analysis showed that male gender (OR = 1.953, P = 0.001), overweight (OR = 2.176, P = 0.001), and preoperative renal function (OR = 0.507, P = 0.001) were independent factors for AKI. Regression analysis among different etiologies showed significant differences in postoperative AKI. After Unilateral nephrectomy, AKI is more likely to occur in overweight male patients with normal kidney function. AKI occurred more frequently in patients who are kidney donors, but rarely in those with non-function kidneys.
Similar content being viewed by others


Introduction
Unilateral Nephrectomy is one of the most common treatments for surgical diseases of the kidney1, with indications including renal cell carcinoma, renal pelvic tumour, ureter tumour, and non-functioning kidney. Donor Nephrectomy is also the surgical method of choice for living kidney donors. The contralateral kidney undergoes compensatory enlargement within hours of Unilateral Nephrectomy, and the subsequent decrease in glomerular filtration rates can be transient or subclinical2. However, some patients who undergo Unilateral Nephrectomy suffer from acute kidney injury (AKI) after surgery, which is attributable to several factors, including elderly age, male gender, preoperative chronic kidney disease (CKD) and diabetes mellitus3,4,5,6,7,8,9,10.
Some scholars have found that AKI is a leading risk factor for the initiation and progression of CKD11. And AKI is associated with several negative outcomes, including cardiovascular/cerebrovascular diseases, poor health-related quality of life, rehospitalizations, and even death12. Moreover, Unilateral Nephrectomy is a crucial factor in postoperative AKI13. Indeed, a previous study suggested that AKI after Nephrectomy for RCC leaves sequelae in the remaining kidneys, which is a strong risk factor for irreversible kidney dysfunction8,9,10. Furthermore, the transition to CKD after Nephrectomy is associated with both all-cause14,15 and cancer-specific mortality, and represents an increasing concern clinically. However, despite the extensive literature on AKI, few studies have reported on postoperative AKI after Unilateral nephrectomy. This may lead us to underestimate the risk of AKI.
Therefore, we retrospectively analysed 528 patients who underwent Unilateral Nephrectomy for different etiologies between January 2013 and December 2018 at the Affiliated Hospital of Qingdao University, with the aim to explore the risk factors of AKI in patients with Unilateral Nephrectomy and identify high-risk groups to improve early predictions.
Materials and methods
Patients
We conducted a retrospective single-center study of patients who underwent Unilateral Nephrectomy at the Affiliated Hospital of Qingdao University between January 2013 and December 2018. The study received ethical approval from the Institutional Review Board (IRB) at the Ethics Committee of the affiliated hospital of Qingdao University. The number is QYFY WZLL 29,096. All methods were performed in accordance with the relevant guidelines and regulations.
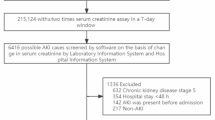
All included patients underwent radical nephrectomy from to 2013–2018, and Five etiologies were included in this study: renal carcinoma, renal pelvic tumor, ureter tumor, non-function kidney, and kidney donation. Among the causes of non-functioning kidneys are factors other than renal cancer, ureteral cancer, and renal pelvis cancer. The exclusion criteria were as follows: (1) age < 18 years, (2) incomplete clinical data. (3) Severe multiple organ failure (4) Metastatic tumors were reduced by Reduction Surgery 5) Severe postoperative complications. In the end, a total of 528 patients were enrolled in our study.
The patient characteristics at the time of Unilateral Nephrectomy and clinical data and laboratory investigations are listed in Table 1. The median age of the included patients was 61 (21–93) years. The study population comprised 193 patients (36.6%) with hypertension, 78 patients (14.8%) with diabetes, and 309 patients with normal renal function. Moreover, 88 cases (16.7%) had anaemia and 85 (16.1%) had abnormal coagulation function before surgery. Among all included patients, 114 (21.6%) had increased urea nitrogen, 119 (22.5%) had increased uric acid, 382 (72.3%) had overweight, 378 (71.6%) had renal carcinoma, 45 (8.5%) had renal pelvis malignancies, 53 (10%) had ureteral malignancies, 40 (7.6%) had non-functional kidney, and 12 (2.3%) were kidney donors. The medical records consisted of 114 (21.6%) cases of laparoscopic assisted surgery and 414 (78%) cases of traditional open surgery. Additionally, 218 patients (41.2%) experienced postoperative AKI.
This study was approved by the Institutional Review Board of QingDao University and the institutional review boards. The provisions of the ethics committee and ethics guidelines in China did not require written consent given the retrospective nature of the study.
Clinical data and laboratory investigations
Preoperative characteristics, including age, gender, body mass index (BMI), serum creatinine concentration, estimated eGFR, diabetes mellitus, hypertension, performed surgery, anaemia, albumin, coagulation, lactate dehydrogenase, nitrogen (BUN), and uric acid, were extracted from the patients’ medical records and an electronic database. Five etiologies were included in this study: renal carcinoma, renal pelvic tumor, ureter tumor, non-function kidney, and kidney donation. The estimated GFRs were calculated using the abbreviated Modification in Diet and Renal Disease (MDRD) Study equation: eGFR = 186 × (serum creatinine) 1.154 × (age) 0.203, from which the result is multiplied by 0.742 for female patients. According to the standards of the World Health Organization, the blood pressure standards of normal adults are: 90-140mmHg systolic blood pressure and 60-90mmHg diastolic blood pressure, and The World Health Organization’s diagnostic criteria for diabetes are fasting blood glucose ≥ 7.0mmol/L and glucose tolerance test ≥ 11.1mmol/L for 2 h.
According to the criteria of the World Health Organization, the patients were divided into underweight (< 18.5 kg/m2), normal (18.5–23.9 kg/m2), and overweight (> 24 kg/m2), and the renal function was staged as CKD I–V according to the American standard stages of renal function. The patients were divided into normal renal function (CKD I) and abnormal renal function (CKD II–V). The main predictor was the occurrence of postoperative AKI, as defined according to the KDIGO 2012 guidelines: increase in plasma creatinine > 26.5 µmol/L within 48 h or an increase in plasma creatinine > 1.5-fold of baseline, which is known or presumed to have occurred within the prior 48 h. The highest serum creatinine level within 48 h of Nephrectomy was compared with the preoperative serum creatinine level to assess the occurrence of AKI.
Statistical analysis
SPSS25.0 statistical software was used for processing, categorical data was described by case number (or percentage %), numerical variables are expressed as the median and interquartile ranges. The measurement data were described by means of standard deviation (x ± s). Univariate and multivariate logistic regression analyses were used to identify independent predictors of postoperative AKI. P-values < 0.05 were taken as statistically significant.
Results
First, we conducted a single factor regression analysis of different influencing factors and the occurrence of postoperative AKI, and then, the multivariate logistic regression analysis was performed for the factors with statistically significant univariate results. Multivariate analysis revealed that male gender (OR = 1.95, P = 0.001), overweight (OR = 2.18, P = 0.001), and normal preoperative eGFR (OR = 0.51, P = 0.001) were independent risk factors for postoperative AKI (Table 2). However, age was not significantly associated with AKI in our study (OR = 0.92, P = 0.65).
We found differences in preoperative renal function between different etiologies. Therefore, pairwise comparisons were made between etiologies, with significant differences in postoperative AKI found between the five etiologies. We conducted pairwise comparisons between the different etiologies. As a result, we found no significant differences between the patients with RCC and renal pelvis, but did find significant differences between the patients with RCC and ureter tumours, non-function kidney patients, and kidney donations. Moreover, no significant differences were observed between the patients with ureter tumours patients and renal pelvic. Additionally, patients with non-functional kidney and donor kidney showed significant differences compared to other causes (Table 3).
Our study conducted a unified analysis on patients with five different etiologies. In order to validate the credibility of our conclusions and eliminate confounding factors within different etiology groups, we divided into 5 subgroups based on different etiologies and conducted a multifactorial analysis within the subgroups, as shown in Table 4 and Supplementary Tables S1–S5. We found that, apart from preoperative renal function, BMI, and gender, there were no statistically significant differences in other relevant parameters.
Discussion
The occurrence of AKI after Unilateral Nephrectomy is a situation that cannot be ignored. We considered that the occurrence of AKI will cause many adverse consequences, so we conducted this study.
In this study, we assessed the incidence of AKI following Unilateral Nephrectomy and found that AKI developed in 41.2% of our study patients. Univariate analysis revealed that gender, overweight, preoperative renal function, and Laparoscopic surgery were significantly associated with AKI. Multivariate analysis revealed that male gender, overweight, and normal preoperative eGFR were independent risk factors for postoperative AKI. Although the surgeries of urothelial carcinoma and renal carcinoma vary in terms of the procedure and scope of excision. The scope of urothelial carcinoma includes the kidney, the entire ureter, and part of the bladder. The removal of one kidney is the most important effect on the body16,17, so we believe that they can be combined for analysis and comparison.
Recently, a study proposed that AKI is a frequent complication after radical nephrectomy, with an incidence of up to 53.9%, and is associated with the development of CKD18. Older age, male gender, higher BMI, and higher preoperative GFR were identified as independent risk factors for postoperative AKI9. Although age was not significantly associated with AKI in our study, the other factors were in good accordance with the results observed in our study.
These findings have a possible explanation. First, as there is a given number of nephrons for the same patient, obesity places greater strain on the kidneys leading overweight patients to develop AKI more commonly19. Similarly, as men have a stronger metabolic capacity than women, the kidney load is also greater, so they are more likely to develop AKI. However, we reported that patients with normal preoperative renal function showed an increased risk of postoperative AKI. Surprised by the effect that preoperative renal function had on the occurrence rate of AKI, We took further analysis (Figs. 1, 2 and 3). We found differences in preoperative renal function between different etiologies. And we found an interesting phenomenon that the higher the probability of CKD, the lower the probability of AKI. Therefore, we further studied the relationship between different etiologies and postoperative AKI (Table 3).

Preaopreative and postoperative creatinine ratios.

Preopreative eGFR.

The probability of AKI occurrence in different etiologies.
We believe that this question is interesting and warrants further investigation. In this study, the incidence of AKI was lowest in patients with non-functional kidneys and highest in those who received kidney donation. As it has been shown that the contralateral kidney undergoes compensatory hypertrophy after Unilateral nephrectomy, we made several hypotheses2. The renal function of diseased kidneys in patients with non-functional kidneys declined gradually owing to their ability to contribute to compensatory growth processes in the contralateral kidney. Consequently, the opposite kidney adapted to the body’s needs, leading to a lower probability of AKI after contralateral Unilateral Nephrectomy. However, the kidney function of donors is normal, and the contralateral kidney cannot compensate in time after sudden loss of a kidney; therefore, the probability of AKI is higher after performing a contralateral Unilateral Nephrectomy.
Because the renal function of patients before and after surgery was inconsistent, we next conducted a comparative analysis. In some patients, renal function will increase after surgery, mainly in patients with non-functional kidneys. Patients with non-function kidneys have undergone a prolonged contralateral renal compensation before surgery; therefore, we believe that preoperative compensation of the contralateral kidney is an important factor affecting the occurrence of postoperative AKI (Fig. 1).
Patients who had ureter tumours had a lower probability of AKI than patients with renal carcinoma, but a higher probability than patients with non-function kidneys. Therefore, we believe that the diseased kidney in patients with ureter tumours exhibits hydronephrosis to some extent, leading to compensatory growth of the contralateral kidney. However, the tumours are usually expansive and outward growing in patients with renal carcinoma, which is less damaging to kidney function20. In our study, preoperative renal function decreased in 60.3% of patients with ureteral tumours, but in only 36.8% of those with renal carcinoma. However, the data collection and analysis of the patients with kidney cancer in this study were insufficient, and the tumour size, pathological diagnosis of the tumour, tumour grade, and affected renal function are also required. Therefore, further studies are needed to test the proposed hypothesis.
Taken together, the occurrence of postoperative AKI was closely related to the residual renal function of the affected kidney before surgery, and certain compensatory changes in the contralateral kidney before surgery were closely related to the occurrence of postoperative AKI. For patients undergoing Unilateral nephrectomy, it would be a predictor of postoperative AKI occurrence. This strategy could be employed to develop novel therapies for the prevention of AKI. Patients undergoing upper urinary tract urothelial carcinoma and some patients with advanced renal cells will require postoperative adjuvant therapy21. Renal function is an important index in postoperative adjuvant therapy22,23. After hospital admission, early prediction of AKI can provide an opportunity to prevent patients from developing AKI and to determine appropriate interventions, if any, which may benefit the recovery of renal function.
We used the KDIGO criteria to define AKI, this can be judged by the change in blood creatinine value, as well as by monitoring the urine volume of patients 6–24 h after surgery. However, in retrospective studies and in clinical practice, the urine volume at 6 and 12 h is often difficult to obtain; thus, no urine volume criteria were used for the definition of AKI in the present study, which makes it difficult to draw definitive conclusions. In addition, this paper is a retrospective study, due to the retrospective nature of the data used, there is a possibility of bias in data analysis. Therefore, we will carry out further prospective research to further demonstrate the research results of this paper.
Conclusion
The incidence and odds of postoperative AKI were higher after Unilateral surgery in male patients who were overweight and had normal kidney function. Additionally, we noted a significant difference in the risk of AKI in patients undergoing Unilateral nephrectomy for different etiologies. Renal AKI occurred more frequently in kidney donation, and the probability of intra-renal AKI in non-function kidneys was much lower than that in other etiologies. Therefore, we believe that the residual renal function of the diseased kidney and the compensatory status of the opposite kidney are important factors in the occurrence of postoperative AKI.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Mithani, M. S., Hassan, W. & Mithani, M. H. A. A review of the First 100 cases of laparoscopic nephrectomy: a single-center experience. Cureus. 14, e20964 (2022).
Rojas-Canales, D. M., Li, J. Y., Makuei, L. & Gleadle, J. M. Compensatory renal hypertrophy following nephrectomy: when and how? Nephrol. (Carlton). 24, 1225–1232 (2019).
Bhindi, B. et al. Predicting Renal function outcomes after partial and radical nephrectomy. Eur. Urol. 75, 766–772 (2019).
Zhang, Z. et al. Acute kidney Injury after partial nephrectomy: role of Parenchymal Mass reduction and ischemia and impact on subsequent functional recovery. Eur. Urol. 69, 745–752 (2016).
Kim, N. Y. et al. Development of a risk scoring system for predicting acute kidney injury after minimally invasive partial and radical nephrectomy: a retrospective study. Surg. Endosc. 35, 1626–1635 (2021).
Schmid, M. et al. Predictors of 30-day acute kidney injury following radical and partial nephrectomy for renal cell carcinoma. Urol. Oncol. 32, 1259–1266 (2014).
Schmid, M. et al. Trends of acute kidney injury after radical or partial nephrectomy for renal cell carcinoma. Urol. Oncol. 34, 293 e291–293 e210 (2016).
Garofalo, C. et al. Effect of post-nephrectomy acute kidney injury on renal outcome: a retrospective long-term study. World J. Urol. 36, 59–63 (2018).
Cho, A. et al. Post-operative acute kidney injury in patients with renal cell carcinoma is a potent risk factor for new-onset chronic kidney disease after radical nephrectomy. Nephrol. Dial Transpl. 26, 3496–3501 (2011).
Martini, A. et al. A Nomogram to predict significant estimated glomerular filtration rate reduction after robotic partial nephrectomy. Eur. Urol. 74, 833–839 (2018).
Chawla, L. S., Eggers, P. W., Star, R. A. & Kimmel, P. L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N Engl. J. Med. 371, 58–66 (2014).
Neyra, J. A. & Chawla, L. S. Acute kidney disease to chronic kidney disease. Crit. Care Clin. 37, 453–474 (2021).
Wang, S., Liu, Z., Zhang, D., Xiang, F. & Zheng, W. The incidence and risk factors of chronic kidney disease after radical nephrectomy in patients with renal cell carcinoma. BMC Cancer. 22, 1138 (2022).
Lane, B. R. et al. Survival and Functional Stability in chronic kidney Disease due to Surgical removal of nephrons: Importance of the new baseline glomerular filtration rate. Eur. Urol. 68, 996–1003 (2015).
Streja, E. et al. Radical versus partial nephrectomy, chronic kidney disease progression and mortality in US veterans. Nephrol. Dial Transpl. 33, 95–101 (2018).
Meyer, J. P., Delves, G. H., Sullivan, M. E. & Keoghane, S. R. The effect of nephroureterectomy on glomerular filtration rate. BJU Int. 98, 845–848 (2006).
Tafuri, A., Marchioni, M., Cerrato, C., Mari, A., Tellini, R., & Odorizzi, K. Changes in renal function after nephroureterectomy for upper urinary tract carcinoma: Analysis of a large multicenter cohort (radical nephroureterectomy outcomes (RaNeO) Research Consortium). World J. Urol. (2022).
Kim, W. H. et al. Robust Association between Acute Kidney Injury after Radical Nephrectomy and Long-term renal function. J. Clin. Med. 9, 619 (2020).
Truche, A. S., Bailly, S., Fabre, O., Legrand, R. & Zaoui, P. A specific high-protein weight loss program does not impair renal function in patients who are Overweight/Obese. Nutrients 14 (2022).
Fukatsu, A. et al. Growth pattern, an important pathologic prognostic parameter for clear cell renal cell carcinoma. Am. J. Clin. Pathol. 140, 500–505 (2013).
Birtle, A. et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): a phase 3, open-label, randomised controlled trial. Lancet. 395, 1268–1277 (2020).
Shao, I. H. et al. Risk factors associated with ineligibility of adjuvant cisplatin-based chemotherapy after nephroureterectomy. Drug Des. Devel Ther. 8, 1985–1990 (2014).
Galsky, M. D. et al. Treatment of patients with metastatic urothelial cancer unfit for cisplatin-based chemotherapy. J. Clin. Oncol. 29, 2432–2438 (2011).
Author information
Authors and Affiliations
Contributions
Yongchao Yan performed the data analyses and wrote the manuscript. Bin Li, Yunbo Liu, Shang Xu and Haotian Du did the pathological analysis and helped doing clincal management. Xinning Wang revised the manuscript critically for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study received ethical approval from the Institutional Review Board (IRB) at the Ethics Committee of the affiliated hospital of Qingdao University. The number is QYFY WZLL 29096.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yan, Y., Liu, Y., Li, B. et al. Analysis of influencing factors of acute kidney injury after unilateral nephrectomy. Sci Rep 14, 24423 (2024). https://doi.org/10.1038/s41598-024-76121-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76121-6
