
Abstract
This study aimed to explore the role of the three-dimension (3D) printed models in orthopedic resident training of tibial plateau fractures. A total of 41 residents from our institution were divided into two groups. The intervention group, consisting of 20 residents, had access to 3D-printed models illustrating thirteen tibial plateau fractures. In contrast, the control group, comprising 21 residents, received digital images of thirteen identical tibial plateau fractures. Evaluation of learning outcomes included the accurate identification of tibial plateau fracture patterns, deduction of traumatic mechanisms, preoperative plan, assessment time, and subjective questionnaire responses. The participants with 3D printed models scored significantly higher in both the Schatzker classification and Luo three-column classification compared to those without 3D printed models. Residents in the intervention group performed better in accuracy in deducing traumatic mechanisms compared to the control group. In addition, the sum score of preoperative plan in the intervention group was significantly higher than that in the control group. Specifically, participants with 3D printed models scored higher in surgical approach choice and implants placement than these in the control group. Residents exposed to 3D printed models also spent less time to complete the assessment than those with access only to digital imaging. Subjective assessments indicated that 3D-printed models boosted confidence in fracture identification, improved preoperative plan for fracture management and enhanced the understanding in injury mechanism of tibial plateau fractures. Furthermore, residents agreed that the use of 3D-printed models heightened their interest in learning tibial plateau fractures. Therefore, the addition of 3D printed models significantly contributed to a comprehensive understanding of tibial plateau fractures, the improvement in fracture identification, inferring injury mechanisms and preoperative plan.
Similar content being viewed by others


Introduction
Tibial plateau fractures are common intra-articular injuries with a diverse range of presentations, which accounts for approximately 1% of all fractures and 18.6% of tibial fractures1,2. Fracture presentations range from simple to complex, depending on whether the trauma is high or low energy. The tibial plateau, consisting of medial plateau and lateral plateau, is one of the most critical weight-bearing surface in the human body. Fractures of tibial plateau typically resulted from a combination of axial, varus, valgus and rotation force, leading to articular shear and depression and limb malalignment3. Management of tibial plateau fracture remains a significant challenge due to the complexity of fracture patterns and the severity of accompanying soft tissue injuries. Complex tibial plateau fractures are closely associated with a high incidence of posttraumatic arthritis4. The ultimate goal of tibial plateau fracture treatment is to achieve anatomic reduction of articular surface and restore limb alignment5.
The Surgical intervention has established as a reliable treatment, ensuring anatomical reduction, stable fixation, early mobilization, and favorable outcomes6. Both orthopedic residents and experienced surgeons typically rely on plain radiography, two-dimensional CT (2D), and three-dimensional reconstructions CT (3D) to identify tibial plateau fracture patterns and plan surgeries7. However, the intricate nature of tibial plateau fractures poses a challenge, especially for junior orthopedic residents, who often struggle to use traditional radiography for accurate classification and understanding of traumatic mechanisms8. This complexity extends to selecting appropriate surgical approaches and correctly placing hardware9. Consequently, there exists a pressing need for a visual model that accurately represents real tibial plateau fracture patterns, particularly for the more complex cases, to enhance residents’ learning outcomes.
Recent advancements in 3D printing technology have revolutionized the orthopedic field, enabling the production of personalized medical instruments and implants, facilitating preoperative planning, and enhancing patient comprehension of their surgical conditions10,11. Moreover, documented benefits of 3D-printed models include reduced intraoperative fluoroscopy, decreased operative time, and minimized blood loss12. While previous studies have demonstrated the positive impact of 3D-printed models on medical education for pelvic fractures, calcaneal fractures, and acetabular fractures13,14,15, there is a noticeable gap in the literature regarding the efficacy of 3D-printed models in educating orthopedic residents about tibial plateau fractures.
This study aims to fill this gap by investigating whether 3D-printed models can improve fracture identifying patterns, traumatic mechanisms understanding, and preoperative planning among orthopedic residents within our institution.
Materials and methods
Ethics statement
Following approval by the ethics review committee of the Second Xiangya Hospital of Central South University for this prospective (Institutional Ethics Board approval code: LYEC2024-K0050), randomized, unblinded study, written informed consents were obtained from all voluntary participants. We confirm that all methods were performed in accordance with the relevant guidelines and regulations of Institutional Ethics Board of the Second Xiangya Hospital of Central South University.
Participants
A total of 41 trainees in a three-year Orthopedic Surgery residency program at Central South University were included. As established in 2014, the standardized residency training system in mainland China required orthopedic residents complete 3 years of training. Therefore, the residents in years 1 to 2 were regarded as junior residents. The residents in years 3 were considered as senior residents. In total, 28 junior and 13 senior orthopeadic residents were enrolled and randomized into control and intervention groups (Table 1). To mitigate the potential bias associated with the PGY level of training, randomization was stratified based on the years of training. The control group (without 3D printed models) had 21 residents, while there were 20 participants in the intervention group (access to 3D printed models).
3D printed model generation
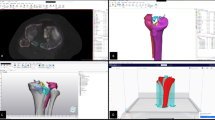
After obtaining institutional ethics approval, we reviewed patients with closed tibial plateau fractures who underwent surgical treatment in our department. Thirteen common types of tibial plateau fractures were selected from our institution’s record files. The Schatzker classification and Luo three-column classification of these fractures were verified by two senior attending orthopedic surgeons specializing in tibial plateau fracture management. Additionally, the senior attending orthopedic surgeons provided information on the injury mechanism and the appropriate surgical plan for each of the thirteen fractures. Two-dimensional CT scans (axial, sagittal, and coronal planes) and reconstructed 3D images were collected from our imaging system. As illustrated in Fig. 1, the images provide a comprehensive view of a tibial plateau fracture for resident training. Figures 1A–C presented the coronal, axial, and sagittal CT image of tibial plateau fracture for resident training, respectively. Additionally, the reconstructed 3D images of the same patient with tibial plateau fracture were showed in Fig. 1D–F.

Representative CT image of tibial plateau fracture for resident training. (A) Coronal view of tibial plateau fracture. (B) Axial views of tibial plateau fracture. (C) Sagittal view of tibial plateau fracture. (D–F) Multiple views of 3D virtual rendering of tibial plateau fracture.
Reconstructed 3D images of the tibial plateau were reconstructed based on the DICOM files derived from the original data of the 2D CT scan images. To generate the 3D printed models, the 2D CT files were saved as DICOM series and processed into STL (Stereolithography) files using Materialise Mimics16.0 software. The STL files were then exported to the 3D printer (Lite 600, SLA 3D printer, UnionTech) to produce the 3D printed models containing tibial plateau fractures using stereolithography technology. As shown in Fig. 2, a three-dimensional printing model of complex tibial plateau fracture was displayed from various viewing angles. Each 3D model was printed with polylactic acid filament based on the STL files.

Example of three-dimensional printing models of complex tibial plateau fracture.
Study design and assessment
A 30-minute didactic lecture was delivered to all enrolled residents, providing fundamental knowledge of tibial plateau anatomy, the concept of the Schatzker classification and the Three-Column classification system (Table 2), and the injury mechanism of tibial plateau fractures. Subsequently, residents from the same PGY training level were randomized into two groups: the control group, without receiving 3D printed models, and the intervention group, with 3D printed models. Twenty one residents in the control group received digital X-rays, 2D CT scan images, and reconstructed 3D images of thirteen tibial plateau fractures. The remaining twenty students in the intervention group received 3D printed models along with identical 3D digital and 2D CT scan images of the thirteen fractures. A test comprising five questions was administered to both groups of residents (Table 3).
For each fracture, participants were asked to record their diagnoses according to the Schatzker classification and the Three-Column classification. Additionally, residents were required to identify the injury mechanism and their surgical plan. For surgical plan, there were four crucial aspects included. As considered as the most two crucial elements in preoperative plan, the surgical approach choice and implants placement were weighted 2:1 compared to the other components of the preoperative plan. Each question was scored one points, while the surgical approach and implants placement sections were scored two points. The total score for preoperative plan was calculated by summing the scores for four aspects: implants placement, access to joint depression and address alignment of fracture, and bone graft.
All residents were timed during the assessment. Furthermore, a 5-item questionnaire was designed to gather feedback from all participants regarding their subjective learning experience with the 3D printed models, using a 5-point Likert-type scale (ranging from strongly disagree to strongly agree).
Statistical analysis
Data were analyzed using GraphPad Prism v8.0.2 (GraphPad Software, San Diego, USA). Continuous variables are presented as mean and standard deviation (SD). A two-tailed unpaired t-test was utilized to compare continuous data between the two groups. Normal distribution was assessed using the D’Agostino-Pearson test. For categorical data, Fisher’s exact test was employed. The level of statistical significance was set at p < 0.05 for all analyses.
Results
Characteristics of residents enrolled
As shown in Table 1, baseline characteristics were quite similar between the two groups, indicating that stratified randomization was successfully obtained. In total, forty one orthopedic residents from PGY1, PGY2, and PGY3 of training level were enrolled. Twenty one residents with 19 males and 2 females were randomized into the control group. Similarly, the intervention group had 19 males and 1 female. The mean age of residents was 24.38 years in the control group and 24.15 years in the intervention group, which revealed no significant difference. The control group had 14 junior residents (PGY-1 and 2) and 7 senior trainees (PGY-3). Fourteen junior residents (PGY-1 and 2) and 6 senior trainees (PGY-3) were randomized into the intervention group.
3D printed models of tibial plateau fracture
In total, thirteen closed tibial plateau fractures treated with open reduction and internal fixation in our department were used. Of these fractures, there were 2 Schatzker Type I fractures, 2 Schatzker Type II fractures, 3 Schatzker Type III fractures, 2 Schatzker Type IV fractures, 2 Schatzker Type V fractures, and 2 Schatzker Type VI fractures according to Schatzker classification system16. Based on the Luo three-column concept17, we included 9 one-column fractures, 2 two-column fracture, and 2 three-column fractures. All thirteen tibial plateau fracture models were reconstructed by 3D printing technology. As shown in Fig. 2, a representing 3D printing model of complex tibial fracture was displayed from various viewing angles. Each 3D printed model costs $150.
Primary outcomes of assessment
As shown in Table 2, the residents with the addition of 3D printed models tended to have the higher mean scores compared to the participants without 3D printed models, regardless of the type of tibial plateau fracture classifications (p = 0.01, Schatzker classification; p = 0.009, Three-Column classification scores).
The residents in the intervention group performed better in score on injury mechanism inferring than these in the control group (10.4 vs. 8.62, p = 0.0007). Similarly, the use of 3D printed models significantly affected the mean total scores of the preoperative plan among orthopedic residents (Table 4). The mean total score on of preoperative plan in the intervention group was higher than that of the control group (80.75 vs. 75.19, p < 0.0001). In brief, we observed a significant improvement in the values for surgical incision and implant placement with the addition of 3D printed models. Specifically, the mean score of surgical approach was 21.33 for the control group. There was a significant increase to 23 for the intervention group (p = 0.01). The residents who had the access to 3D printed models scored the average 23.2 in implants placement, which was significantly higher than these in the control group with mean score of 21.24 (p = 0.01). We did not observe the significant differences in scores on access to joint depression, address alignment of fracture and bone graft.
The residents in the control group required 764.7 ± 32.41 s to answer the questions, whereas those in the intervention groups took 618.1 ± 11.12 s. The difference in time consumption for answering questions reached statistical significance (p < 0.0001) (Table 4).
Subjective survey
The results of the subjective survey are depicted in Fig. 3, which illustrated the residents’ subjective feedback regarding 3D printed models using a five-point Likert scale. The percentage of residents responding to the statement “3D printed models aided in the preoperative plan for tibial plateau fracture” with “agree” or “strongly agree” were 29.27% and 46.34%, respectively. Meanwhile, 70.73% of participants agreed with the fact that 3D-printed models were able to assist in inferring to the injury mechanism of tibial plateau fractures. In addition, 65.85% of residents agreed or strongly agreed that access to 3D-printed models would improve their confidence in tibial plateau fracture pattern identification. Interestingly, 87.81% of responders stated that exposure to the 3D-printed models enhanced their understanding of tibial plateau fractures. Residents also reached an agreement (80.49%) that interaction with 3D-printed models would increase their learning interest in tibial fractures.

Residents’ subjective feedback regarding 3D printed models on a five-point Likert scale.
Discussion
This study demonstrates that the utilization of 3D printed models representing authentic tibial plateau fractures significantly improves the accuracy of identifying Schatzker and Luo three-column classifications among orthopedic residents. Furthermore, all participating residents exhibited a noteworthy enhancement in comprehending injury mechanisms and making appropriate choices regarding the operative approach and hardware placement for tibial plateau fractures when aided by 3D-printed models. Additionally, residents reported increased confidence in identifying tibial plateau fractures, attributing this to the superior accuracy of the 3D printed models compared to digital 3D renderings.
Several recent studies have highlighted the advantages of incorporating 3D printed models in orthopedic education, particularly in aiding trainees to comprehend complex anatomy and fractures13,14. Goyal et al. reported a notable improvement in fracture understanding among 16 trainees when 3D-printed models of acetabular fractures were introduced18. Similarly, Spencer et al. documented enhanced confidence among trainees in understanding calcaneal fracture patterns, irrespective of their residency experiences, with the use of 3D printed models14. Our prior research involved presenting data from a cohort of 100 medical undergraduate students who were exposed to either 3D digital renderings or 3D printed models of pelvic fractures15. The results revealed that the use of 3D-printed models led to improved accuracy in classifying and identifying the injury mechanisms of pelvic fractures. Moreover, these models significantly increased students’ learning interest and enthusiasm. In another study comparing the diagnosis of complex acetabular fractures using 3D printed models, radiography, and computed tomography, Omer et al. found that residents utilizing 3D printed models exhibited an enhanced understanding of complex cases and classification systems13.
When utilizing 3D printed models, we observed a significant improvement in the identification of Schatzker and Luo’s three-column classifications of tibial plateau fractures among residents. Consistent with our findings, Jellina et al. demonstrated that the incorporation of 3D printed models enhanced interobserver agreement in Schatzker, Luo three-column concept, and AO/OTA classifications19. The 3D printed models offer a realistic representation of actual tibial plateau fractures, providing residents with tactile sensations and visual feedback of the structure and fracture fragments10. Additionally, the interactive learning facilitated by 3D printed model contributes to trainees’ understanding of tibial plateau fractures pattern and promotes learning retention. Furthermore, residents can observe the accurate representation of the fracture’s 3D space from any angle with 3D printed model, aiding junior residents in classifying complex tibial plateau fractures.
Our data indicated that the use of 3D-printed models enhanced the accuracy of injury mechanism interpretation, the selection of appropriate surgical approaches and implant placement among all residents, irrespective of their year of training. Consistent with this observation, Huang et al.. reported that students provided with 3D printed models exhibited a higher percentage of correct deductions regarding the injury mechanism of acetabular fractures compared to those relying solely on CT imaging20. Studies have highlighted the importance of understanding injury mechanisms to achieve satisfactory clinical outcomes in tibial plateau fractures, especially for complex cases21.
For residents lacking experience in the operative management of tibial plateau fractures, inferring to the traumatic mechanism based on displaced fracture fragments in X-ray radiography or CT scans remains a significant challenge. Deducing the traumatic mechanism and selecting the appropriate surgical approach and placement of implant for tibial plateau fractures are closely tied to critical thinking and a comprehensive understanding of fractures. By converting 2D images into solid models with a 1:1 ratio, 3D-printed models provide the real morphology of the fracture and the accurate relative position of fracture fragments22. This aids residents in gaining a comprehensive understanding of the fracture condition and facilitating the preoperative plan.
In addition to enhancing residents’ understanding of the fracture condition, 3D-printed models representing real fractures allow residents to touch the fracture line and feel the contours and edges of fracture fragments18. The tactile feedback from 3D printed models helps residents integrate information from intact to broken tibial plateau. Therefore, the interactive experience with hand-held 3D printed models improves critical thinking about fracture mechanisms, the choice of surgical approaches and implant placement.
Interestingly, we found that residents who received 3D-printed models took less time to answer questions compared to those who only had access to digital imaging. This finding is consistent with Li et al.., where residents using 3D printed models spent less time answering questions about spinal fractures than those relying on radiographic images23. With a heightened understanding of tibial plateau fractures, residents with 3D-printed models felt more confident in classifying fractures, deducing traumatic mechanisms, and making appropriate operative plan. This may explain why residents with 3D printed models demonstrated an advantage over those with only digital images in answering all questions.
In the subjective assessments, the 3D printed model not only assisted residents in fracture classification, injury mechanism inference, and surgical plan selection but also enhanced their confidence and interest in tibial plateau fracture learning. Consistent with our findings, previous study has shown that 3D printing is a valuable and enjoyable learning tool in medical training, playing a positive role in trainees’ subjective learning experiences24. The interactive learning experience with tactile and visual feedback from 3D-printed models may contribute to residents’ appreciation of these models in fracture learning. Furthermore, the 3D-printed model, as a novel instrument and advanced technology representing real fractures, is likely more appealing to residents compared to on-screen digital imaging. Overall, the subjective assessment results reinforce the growing body of evidence indicating the improved value of 3D printing in orthopedic residents’ training of tibial plateau fractures.
It is important to highlight that the cost of 3D printed models illustrating complex tibial plateau fractures varies, ranging from hundreds to thousands of dollars, depending on the printing and software utilized. In this study, the cost of a tibial plateau print was approximately $150, covering materials and processing expenses, making it an affordable option for educational training. Furthermore, with ongoing advancements in technology and software used for 3D printing, prices are expected to decrease over time, making them more accessible for residents’ training. Moreover, virtual reality is a valuable tool in teaching, including in orthopaedic contexts. Its application in studying fracture patterns could bridge the gap between the high cost of 3D models and the limited usability of CT images25.
While our results show promise, it’s important to acknowledge several limitations in the current study. Firstly, the small sample size is a constraint, as the study was restricted to orthopedic residents from a single institution. Secondly, the study design involved an unblinded survey, introducing an inevitable bias due to the disclosure of randomization assignments to all residents for written informed consent. Thirdly, the 3D-printed models exclusively depicted the bone without considering the soft tissues around the tibial plateau. This limitation could lead some residents to overlook soft tissue damage and focus solely on bone injuries. Therefore, future research with larger sample sizes and a focus on both bone and soft tissue injury is essential to further establish the positive contribution of 3D printed models to tibial plateau fracture learning outcomes. In addition, future studies could also focus on the transferring these skills to the operating theatre, which could help in predicting the precision of reduction and the duration of surgeries.
Conclusion
In the present study, the utilization of 3D-printed models in orthopedic resident training yielded positive outcomes. This included a comprehensive understanding of tibial plateau fracture classification, improved proficiency in inferring to traumatic mechanisms, and enhanced decision-making regarding preoperative plan. Furthermore, residents’ subjective responses indicated a favorable attitude toward the use of 3D-printed models in the learning of tibial plateau fractures. Given their affordability, these 3D printed models accurately depicting real fractures are an effective educational tool for residents training in tibial plateau fractures.
Data availability
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- 3D:
-
Three-dimensional
- CT:
-
Computed tomography
- 2D:
-
Two-dimensional
- PGY:
-
Postgraduate year
References
Yao, P. et al. Tibial plateau fractures: three dimensional fracture mapping and morphologic measurements. Int. Orthop. 46, 2153–2163 (2022).
Elsoe, R. et al. Population-based epidemiology of Tibial Plateau fractures. Orthopedics 38, e780–786 (2015).
Hua, K. et al. Retrospective analysis of 514 cases of tibial plateau fractures based on morphology and injury mechanism. J. Orthop. Surg. Res. 14, 267 (2019).
Rudran, B., Little, C., Wiik, A. & Logishetty, K. Tibial Plateau fracture: anatomy, diagnosis and management. Br. J. Hosp. Med. (Lond.) 81, 1–9 (2020).
Li, K. et al. Optimal surgical timing and approach for tibial plateau fracture. Technol. Health Care 30, 545–551 (2022).
Gahr, P. et al. Functional assessment and outcome following surgical treatment of displaced tibial plateau fractures: a retrospective analysis. Eur. J. Trauma. Emerg. Surg. 49, 2373–2379 (2023).
Schatzker, J. & Kfuri, M. Revisiting the management of tibial plateau fractures. Injury 53, 2207–2218 (2022).
Lou, Y. et al. Comparison of traditional surgery and surgery assisted by three dimensional printing technology in the treatment of tibial plateau fractures. Int. Orthop. 41, 1875–1880 (2017).
Rossmann, M. et al. Tibial plateau fracture: does fracture classification influence the choice of surgical approach? A retrospective multicenter analysis. Eur. J. Trauma. Emerg. Surg. 48, 3635–3641 (2022).
Meng, M. et al. 3D printing metal implants in orthopedic surgery: methods, applications and future prospects. J. Orthop. Transl. 42, 94–112 (2023).
Ejnisman, L., Gobbato, B., de Franca Camargo, A. F. & Zancul, E. Three-dimensional printing in orthopedics: from the basics to surgical applications. Curr. Rev. Musculoskelet. Med. 14, 1–8 (2021).
Xie, L. et al. Three-dimensional printing assisted ORIF versus conventional ORIF for tibial plateau fractures: a systematic review and meta-analysis. Int. J. Surg. 57, 35–44 (2018).
Awan, O. A. et al. Efficacy of 3D printed models on resident learning and understanding of common acetabular fracturers. Acad. Radiol. 26, 130–135 (2019).
Montgomery, S. J., Kooner, S. S., Ludwig, T. E. & Schneider, P. S. Impact of 3D printed calcaneal models on fracture understanding and confidence in orthopedic surgery residents. J. Surg. Educ. 77, 472–478 (2020).
Yan, M. et al. Three-Dimensional Printing Model enhances correct identification and understanding of pelvic fracture in medical students. J. Surg. Educ. 80, 331–337 (2023).
Kfuri, M. & Schatzker, J. Revisiting the Schatzker classification of tibial plateau fractures. Injury 49, 2252–2263 (2018).
Wang, Y. et al. Updated three-Column Concept in surgical treatment for tibial plateau fractures—a prospective cohort study of 287 patients. Injury 47, 1488–1496 (2016).
Goyal, S., Chua, C., Chen, Y. S. & Murphy, D. Utility of 3D printed models as adjunct in acetabular fracture teaching for orthopaedic trainees. BMC Med. Educ. 22, 595 (2022).
Huitema, J. M. et al. Are 3D-printed models of Tibial Plateau fractures a useful addition to understanding fractures for Junior surgeons? Clin. Orthop. Relat. Res. 480, 1170–1177 (2022).
Huang, Z. et al. Three-dimensional printing model improves morphological understanding in acetabular fracture learning: a multicenter, randomized, controlled study. PLoS ONE 13, e0191328 (2018).
Xie, X. et al. Comparative analysis of mechanism—Associated 3-dimensional tibial plateau fracture patterns. J. Bone Jt. Surg. Am. 102, 410–418 (2020).
Masada, K. M., Cristino, D. M., Dear, K. A., Hast, M. W. & Mehta, S. 3-D printed fracture models improve resident performance and clinical outcomes in operative fracture management. J. Surg. Educ. 80, 1020–1027 (2023).
Li, Z. et al. Three-dimensional printing models improve understanding of spinal fracture–A randomized controlled study in China. Sci. Rep. 5, 11570 (2015).
Lim, P. K. et al. Use of 3D printed models in resident education for the classification of acetabulum fractures. J. Surg. Educ. 75, 1679–1684 (2018).
Capitani, P. et al. The role of virtual reality in knee arthroscopic simulation: a systematic review. Musculoskelet. Surg. 107, 85–95 (2023).
Acknowledgements
This study was funded by the Higher Education Teaching Reform Project of Central South University (2023jy091), Higher Education Teaching Reform Project of Hunan Province (HNJG-20230108), Scientific Research Project of Health Commision of Hunan Province, China (B202304077065), and Hunan Provincial Natural Science Foundation Joint Fund for the Medical and Health Industry Project (2024JJ9202).
Author information
Authors and Affiliations
Contributions
MMY and JJW wrote the initial draft of the manuscript. MLD and JH collected and analyzed the data. DYS supervised the project from initiation and revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yan, M., Huang, J., Ding, M. et al. 3D-printed model is a useful addition in orthopedic resident education for the understanding of tibial plateau fractures. Sci Rep 14, 24880 (2024). https://doi.org/10.1038/s41598-024-76217-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76217-z
Keywords
This article is cited by
-
Evaluating the educational impact of tomography-based high-resolution 3D-printed distal radius fracture models
BMC Medical Education (2025)
