
Abstract
We aimed to look at the potential relationship between patterns of protein intake and risk of death in adults with type 2 diabetes. We included 4646 adults with type 2 diabetes participating in NHANES (1999–2018). We estimated intake of proteins from 11 animal- and plant-based food groups and then, used principal component analysis to explore data-driven patterns of protein intake. All-cause mortality was ascertained through linkage to National Death Index until December 31, 2019 (n = 969 deaths). Cox proportional hazard regression models were used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). Four dietary protein patterns were identified: “healthy” (high in proteins from legumes, fruits, nuts, seeds, and fish and low in red meat protein), “red meat and egg” (high in red meat and egg proteins and low in fish and poultry proteins), “vegetables/fish” and “dairy/nuts” patterns. The HRs of all-cause mortality for the highest compared to the lowest quartile of “healthy” and “red meat and egg” protein patterns were, respectively, 0.77 (95%CI: 0.62, 0.97; Ptrend = 0.014) and 1.28 (95%CI: 1.06, 1.54; Ptrend = 0.033). Greater adherence to a healthy protein pattern may be associated with a reduced risk of death in patients with type 2 diabetes, while greater adherence to a dietary pattern rich in red meat and egg proteins and low in fish and poultry proteins may be associated with a higher risk.
Similar content being viewed by others

Introduction
Type 2 diabetes is a leading factor in global mortality and disability1, with around 540 million adults currently affected by the disease worldwide2. Evidence obtained from epidemiologic and intervention studies presents a strong case for the important impacts of dietary modifications in the management of type 2 diabetes, consequently aiding in alleviating the substantial burden of mortality and complications associated with diabetes3,4.
High-protein diets have become popular for their ability to promote healthy aging, control weight, and decrease cardiometabolic risk factors in people with type 2 diabetes5,6,7,8. A meta-analysis of nine randomised trials in patients with type 2 diabetes in 2013 indicated that high-protein diets (25–32% of total energy) improved body weight and glycated hemoglobin (HbA1c) when compared with low-protein diets (15–20% of total energy), but had no significant effects on blood pressure, blood lipids and fasting plasma glucose (FPG)9. The selection of protein-rich food sources is crucial not only in terms of the amount of protein ingested but also due to its potential influence on various dietary components such as macro- and micronutrients, which could affect human health and well-being. Findings from short-term randomized trials indicate that substituting animal proteins with plant proteins could lead to a modest improvement in HbA1c and FPG levels among individuals diagnosed with type 2 diabetes10.
At present, the epidemiological data on the association between dietary protein consumption and health outcomes such as all-cause mortality in individuals with type 2 diabetes is limited and lacks consistency11. Most of this data comes from large-scale population-based cohort studies that reported the findings in the subgroup of patients with diabetes12,13,14. The findings from two large cohort studies conducted on health professionals in the US showed that consuming higher amounts of plant proteins was associated with a decreased risk of overall mortality in the subgroup of individuals with type 2 diabetes14. Conversely, there was a positive link between the consumption of animal proteins and the risk of overall mortality14. Another study found an inverse relationship between the intake of plant proteins and the risk of all-cause mortality among patients with type 2 diabetes who took part in the US National Institutes of Health–AARP Diet and Health Study13. An analysis conducted on 6213 patients with type 2 diabetes involved in the ONTARGET study found an inverse relationship between animal protein consumption and mortality risk and a lack of association for plant protein intake12.
Evidence suggests that the effect of foods on health is determined not solely by specific nutrients, but also by the way in which these nutrients interact with each other15. Nutrition research has transitioned in recent years from a narrow focus on individual nutrients to a greater emphasis on the overall quality of the diet16. In fact, dietary pattern analysis may provide a border image of individual’s diet than that of single foods or food groups. Due to the inconsistency in the data regarding the association between dietary proteins and mortality risk in patients with type 2 diabetes, we aimed to look at the link between patterns of dietary protein intake, identified by principal component analysis, and the risk of death from all-cause in a nationally representative sample of US adults with type 2 diabetes.
Subjects and methods
Study participants
The National Health and Nutrition Examination Survey (NHANES) is a periodic survey that presents population information regarding nutrition and health of a nationally representative sample of the US children and adults17.
For the present study, we used data from continuous NHANES 1999–2018. First, we selected patients with type 2 diabetes at enrollment, resulting in a total of 9516 patients with type 2 diabetes being included. As done in previous research18, we selected patients that had at least one of the following criteria as having type 2 diabetes: self-reported physician-diagnosed type 2 diabetes, use of oral hypoglycemic medications or injection of insulin, FPG ≥ 126 mg/dL (7 mmol/L), 2-hour plasma glucose ≥ 200 mg/dL (11.1 mmol/L) after an oral glucose tolerance test, or HbA1c ≥ 6.5% (48 mmol/mmol). Second, we excluded patients with the following criteria: patients younger than 20 years (n = 192), pregnant females (n = 33), those with a history of cardiovascular disease (n = 1984) and cancer (n = 1308), patients with unreliable dietary recalls (n = 1010), those with implausible energy intake, defined as < 600 and > 3500 kcal in females and < 800 and > 4200 kcal in males (n = 166)19, patients with no information on dietary intake (n = 166), and those with no follow-up information (n = 11). Finally, 4646 patients proved eligible for inclusion (Supplementary Fig. 1).
Assessment of dietary intake
Dietary intake was evaluated via one 24-hour dietary recall in NHANES 1999–2002 and two 24-hour dietary recalls in NHANES 2003–2018. We included patients that had one reliable dietary recall in NHANES 1999–2002. In NHANES 2003–2018, we included patients that had two reliable dietary recalls and then, averaged dietary intakes over the two recalls. We estimated intake of protein from 11 animal- and plant-based dietary protein sources including dairy products, red meat, fish, poultry, egg, grains, fruits, vegetables, nuts, legumes and seeds and then, calculated percentage of energy from individual dietary protein sources for dietary pattern analysis.
Ascertainment of mortality
All-cause mortality was ascertained using Public-use Linked Mortality files until December 31, 2019, by establishing a connection to National Death Index records20. We defined all-cause mortality as all specified and unspecified causes of death.
Assessment of covariates
We used publicly available data to obtain information regarding covariates. Trained interviewers, through personal structured interviews and standardized questionnaires at home, gathered detailed information on sociodemographic characteristics, physical activity, smoking status, history of hypertension, medical history, and diabetes duration and medication. Smoking status was categorized into three groups: never, former, and current smokers. Those who had smoked less than 100 cigarettes in their lifetime were considered as never smokers18. We defined current and former smokers as those who reported smoking > 100 cigarettes in their lifetime and those who reported smoking > 100 cigarettes and had quit smoking, respectively18. We classified study participants based on their level of physical activity as inactive, defined as those with no leisure-time physical activity, insufficiently active, defined as those who reported moderate-intensity leisure-time activity 1–5 times per week or vigorous-intensity leisure-time activity 1–3 times per week, and active group, defined as those who reported moderate-to-vigorous activity more than above21. Alcohol drinking was divided into three groups: non-drinkers, light-to-moderate drinkers (less than 1 drink per day in women and less than 2 drinks per day in men), and heavy drinkers (1 or more drinks per day in women and 2 or more drinks per day in men)22. Measurements of height and weight were taken as part of health examinations conducted at a mobile examination center. Body mass index (BMI) was calculated as weight/height2 (kg/m2). Laboratory analyses including the measurement of serum total cholesterol at recruitment were conducted via specimen analyses in the laboratory23.
Statistical analysis
We performed all analyses by incorporating sample weights, strata, and clustering to generate robust national estimates. Percentages of missing covariates were < 5%, except for family income-poverty ratio (9.1%). We performed multiple imputation to reduce sample size reduction by missing covariates.
We applied principal component analysis to explore data-driven patterns of protein intake. Principal component analysis is a statistical technique used for data reduction, which aids in identifying underlying structures and relationships among different nutrients by reducing the number of variables in a dataset while preserving crucial information24. First, we calculated percentage of energy from 11 different animal-based and plant-based proteins and examined the relationships between individual dietary proteins. Usually, correlation coefficients are computed for the purpose of identifying significant associations. Then, utilizing the chosen correlated variables, a covariance matrix was formulated that presented a comprehensive overview of the associations among every conceivable pair of variables, offering an assessment of the magnitude and direction of these associations. The individual dietary proteins were then transformed to new variables named principal components, presenting uncorrelated linear combinations of individual dietary proteins. Subsequently, varimax rotation was implemented to optimize the variance of the loadings (weights) of the initial variables on every principal component. We identified the nutrients that contribute to each component using the loadings (weights) of dietary proteins on each principal component. Dietary proteins with a factor loading > 0.20 were considered to contribute to each component, with a higher factor loading indicating a stronger contribution to the construction of the principal component. Principal components were retained for additional analyses based on Eigen values obtained in the scree plot. In the present study, principal components with Eigen values of ≥ 1 were kept to determine dietary patterns25. The factorability of the data was validated through the utilization of the Kaiser–Meyer–Olkin test for assessing sample adequacy and Bartlett’s test for examining sphericity, successfully yielding precise statistical estimates for this sample.
We classified dietary pattern scores into quartiles and reported the characteristics of the study participants across quartiles in the form of mean ± SD for continuous variables and number (percentage) for categorical variables. Potential differences among quartiles were analyzed using various statistical tests. The one-way ANOVA was employed for continuous variables and the x2 test was utilized for categorical variables. We used Cox proportional hazards regression models to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) of all-cause mortality across quartiles of dietary pattern scores. The values of person-time were derived by calculating the time interval between the date of the NHANES interview during recruitment and the date of either mortality or the end of the follow-up period, which was determined as December 31, 2019, whichever event occurred earlier.
Two statistical models were applied. In the first model, we controlled for age (continuous, years), sex (male or female), and race/ethnicity (non-Hispanic White, non-Hispanic Black, Mexican American, or other). In model 2, we additionally controlled for BMI (continuous, kg/m2), family income-to-poverty ratio (≤ 1, 1–3, or > 3), education level (< high school, high school or equivalent, or ≥ college), physical activity status (inactive, insufficiently active, or active), smoking status (never, former, or current), alcohol drinking (non-drinker, light-to-moderate drinker, or heavy drinker), self-reported history of hypertension (yes or no), insulin use (yes or no), duration of diabetes (< 3, 3–10, or > 10 years), baseline HbA1c (< 7 or ≥ 7%), serum total cholesterol (in quintiles), dietary supplement use (yes or no), total energy intake (continuous), dietary fiber intake (continuous), and percentage of energy from saturated fats, monounsaturated fats, and polyunsaturated fats (continuous).
We performed several stratified analyses based on age (< 65 or ≥ 65 years), sex (male or female), race/ethnicity (non-Hispanic White or other), BMI (< 30 or ≥ 30 kg/m2), smoking status (never/former or current), leisure-time physical activity (inactive or insufficient active/active), alcohol drinking (non-drinker or drinker), diabetes duration (< 3 or ≥ 3 years), insulin use (yes or no), and baseline HbA1c status (< 7 or ≥ 7%). We also performed three sensitivity analyses. First, we repeated the analyses after exclusion of deaths that occurred within the first two years of follow-up to minimize the potential for reverse causality bias. We also performed a sensitivity analysis after exclusion of participants in NHANES 1999–2002 since they completed only one dietary recall. This helps restrict the analyses to participants with two reliable dietary recalls and minimize measurement error due to recall bias. Finally, after a comment from one of the reviewers, we repeated the analyses considering the method introduced by National Cancer Institute (NCI) to estimate usual dietary intake26,27. This method necessitates the collection of two or more dietary recalls on non-consecutive days from a random sample of the population. This approach is designed to address both between-person and within-person variations in dietary intake and can be utilized to adjust for measurement errors when assessing the usual intake of nutrients27. A two-step methodology was employed to assess the typical consumption of dietary proteins and the total daily caloric intake, utilizing the MIXTRAN and INDIVIT macros provided by the NCI27,28. For this sensitivity analysis, we restricted the analyses to participants with two dietary recalls. SAS 9.4 (SAS Institute; Cary, NC, USA) was used to estimate usual intakes using the NCI macros, and all other analyses were conducted using STATA software, version 17, considering a 2-tailed P value less than 0.05 as statistically significant.
Results
In total, 4646 patients with type 2 diabetes were included in the present study. The mean age of the participants was 58.4 ± 13.6 years, the mean BMI was 32.3 ± 7.4 kg/m2, and the average HbA1c at baseline was 7.4 ± 1.8% (Table 1). Of the study participants, 48% were male, 31% were non-Hispanic White, 41% had a college degree or above, 53% were never smoker and 33% were non-drinker.
Principal component analysis identified four major dietary protein pattern (Table 2). The first pattern was distinguished by a high consumption of proteins derived from fruits, legumes, seeds, nuts, and fish, coupled with a limited consumption of red meat protein. We named this protein pattern as “healthy”. The second pattern identified was the “red meat and egg” protein pattern, distinguished by a high consumption of red meat and egg proteins and a diminished consumption of poultry and fish proteins. The third pattern exhibited high intake of vegetables, fish, and red meat proteins while containing low levels of grains and legumes proteins, hence it was designated as the “vegetable and fish” protein pattern. The fourth protein pattern was “dairy and nut” protein pattern which was accompanied by a high intake of proteins derived from dairy, nuts, and fruits and low intake of proteins from fish and egg.
Characteristics of the study participants across quartiles of dietary protein pattern scores are summarized in Table 3. In brief, patients in the fourth quartile of “healthy” pattern were older, had a higher mean BMI, and were less likely to be female and non-Hispanic White compared to the first quartile. The proportion of patients who were physically inactive and current smoker was also lower in the fourth quartile in comparison to the first quartile. With regards to “red meat and egg” pattern, patients in the top quartile were younger, and were more likely to be male and non-Hispanic White. The proportion of patients who were current smoker and alcohol drinker was higher in the top quartile in comparison to the bottom quartile. The four protein patterns accounted for 41.8% of total variation in dietary proteins.
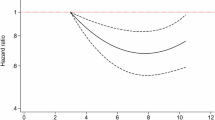
The associations between dietary protein patterns and mortality in patients with type 2 diabetes are summarized in Table 4. Greater adherence to “healthy” protein pattern was associated with a reduced mortality risk, where multivariable-adjusted HRs and 95%CIs for the second, third, and fourth quartiles of “healthy” protein patterns were, respectively, 0.97 (95%CI: 0.81, 1.17), 0.80 (95%CI: 0.67, 0.96), and 0.77 (95%CI: 0.62, 0.97) (Ptrend = 0.014; Table 4). The HRs across quartile of “red meat and egg” protein pattern were, respectively, 1.00 (reference), 1.04 (95%CI: 0.86, 1.25), 1.05 (95%CI: 0.86, 1.29), and 1.28 (95%CI: 1.06, 1.54) (Ptrend = 0.033), suggesting that greatest adherence to “red meat and egg” protein pattern may be associated with a higher risk. No significant association was found between adherence to “vegetable and fish” and “dairy and nuts” dietary protein patterns and overall mortality in patients with type 2 diabetes.
The association of “healthy” and “red meat and egg” protein patterns with mortality risk remained significant and did not change materially when we excluded deaths that occurred during the first two years of follow-up (Supplementary Table 1), as well as when we restricted the analyses to patients with two reliable dietary recalls (Supplementary Table 2). The non-significant associations between “vegetable and fish” and “dairy and nuts” protein patterns and mortality risk persisted in the sensitivity analyses.
We also performed a series of stratified analyses by a few variables. Stratified analyses indicated that there was no significant difference across different subgroups defined based on age, baseline BMI, diabetes duration, baseline HbA1c, smoking status, alcohol drinking, physical activity, and insulin use (Supplementary Table 3). Within stratified analyses, the inverse relationship between a “healthy” dietary protein pattern and the risk of mortality appeared to be significant among individuals aged 65 years and older, females, individuals with a BMI less than 30 kg/m2, individuals who were never or former smokers, individuals who engaged in physical activity, individuals who did not use insulin, and those with a diabetes duration of less than 3 years. For “red meat and egg” dietary protein pattern, the positive association appeared to be significant among individuals aged 65 years and above, males, current smokers, alcohol drinkers, physically active individuals, and those with an HbA1c level below 7% (Supplementary Table 3).
We also performed an additional sensitivity analysis using dietary data obtained by the NCI approach. For this purpose, we limited the analyses to participants with two recalls, applied the NCI method to estimate dietary protein and total energy intakes, performed a factor analysis to generate data-driven dietary patterns, and then investigated the association between dietary patterns and all-cause mortality. This methodology yielded four dietary patterns that closely resembled those found in the primary analysis, albeit with some variations, such as a high factor loading of vegetable proteins within the “healthy” protein pattern and the exclusion of legumes from the “red meat and egg” and “vegetable and fish” dietary patterns (Supplementary Table 4). The relationship between these dietary patterns and all-cause mortality is detailed in Supplementary Table 5, indicating a somewhat more pronounced inverse association for the “healthy” dietary pattern compared to the primary analysis. Other findings remained largely unchanged in this sensitivity analysis.
Discussion
In the present prospective cohort study involving a representative sample of US adults with type 2 diabetes, we found that greater adherence to the “healthy” dietary protein pattern, rich in proteins derived from fruits, legumes, nuts, seeds, and fish, and low in red meat protein, was associated with a graded decrease in the risk of type 2 diabetes. By contrast, greater adherence to the “red meat and egg” protein pattern, rich in red meat and egg proteins and low in poultry and fish proteins, was associated with a higher risk. No association was found between adherence to the “vegetables and fish” and “dairy and nuts” protein patterns and mortality risk.
Research on the link between dietary patterns and mortality among individuals diagnosed with type 2 diabetes is currently lacking and limited to predefined index-based dietary patterns. Previous cohort studies have suggested that greater adherence to healthy dietary patterns such as the Mediterranean dietary pattern29, Alternative Healthy Eating Index30, the Dutch Healthy Nutrient and Food Score31, and Dietary Approaches to Stop Hypertension32 was linked to a reduced all-cause mortality risk. We are not aware of any other cohort study that investigated the association between posteriori-defined data-driven patterns of protein intake and risk of all-cause mortality in patients with type 2 diabetes.
To our knowledge, there is only one cohort study that investigated the association between posterior dietary patterns and mortality risk in individuals with type 2 diabetes29. An examination conducted on a cohort of 1995 individuals diagnosed with type 2 diabetes as part of the MOLI-SANI study in Italy employed principal factor analysis to investigate dietary patterns. The study revealed that a higher level of compliance with the dietary pattern labeled as “olive oil and vegetables”, characterized by a high intake of olive oil, vegetables, fruits, legumes, and fish, exhibited a link with a decreased risk of mortality in the model adjusted for age and sex, although this association was not significant in the fully adjusted model29. The investigation further revealed that a greater adherence to the dietary pattern characterized by consumption of eggs and sweets was linked to a rise in the overall risk of mortality, albeit lacking statistical significance29.
Indeed, there is sparse and inconsistent epidemiological evidence concerning the relationship between dietary protein consumption and the risk of various health consequences, such as overall mortality, in individuals diagnosed with type 2 diabetes11. Two large prospective cohort studies conducted on health professionals in the US indicated that higher consumption of plant proteins was linked with a reduced risk of all-cause mortality in the subgroup of individuals with type 2 diabetes. They also found a positive association between consuming animal proteins and all-cause mortality risk14. Another study indicated an inverse association between the consumption of plant proteins and all-cause mortality risk in the subgroup of patients with type 2 diabetes participating in the US National Institutes of Health–AARP Diet and Health Study13. In contrast, an evaluation among 6,213 patients with type 2 diabetes participating in the Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial (ONTARGET) suggested an inverse association for animal protein intake and no association for plant proteins12.
Our results align with the findings documented in prior studies regarding the relationship between specific foods or food groups and the risk of mortality among individuals diagnosed with type 2 diabetes. Prior meta-analyses conducted on cohort studies revealed a link between increased consumption of fruits, fish, and nuts and a decreased risk of mortality among individuals diagnosed with type 2 diabetes11,33. Our research also aligns with these results, demonstrating an inverse relationship between adherence to a “healthy” dietary protein pattern, characterized by a high intake of proteins derived from fruits, legumes, nuts, seeds, and fish, and the risk of mortality. We also identified a positive relationship between adherence to the “red meat and egg” dietary protein pattern and mortality. This observation aligns with earlier studies that have shown a positive relationship between egg consumption and mortality risk in individuals with type 2 diabetes. Furthermore, there was a non-significant positive relationship between red meat consumption and mortality in individuals with diabetes11.
Within stratified analyses, the inverse relationship between a “healthy” protein pattern and the risk of mortality appeared to be significant among individuals with a BMI less than 30 kg/m2, never or former smokers, individuals who engaged in physical activity, individuals who did not use insulin, and those with a diabetes duration of less than 3 years. This suggests that beneficial effects of a healthy dietary protein pattern could be amplified by additional healthy lifestyle-related behaviors or may be particularly evident among patient with better prognosis. For “red meat and egg” dietary protein pattern, we found that the negative effects of the “red meat and egg” dietary protein pattern may be exacerbated when combined with other unhealthy habits like smoking and alcohol drinking.
Current recommendations for patients with type 2 diabetes available in existing guidelines encourage the choice of plant-based dietary sources of proteins34,35,36; however, their recommendations are mostly based on the data from the general population, or mainly derived from intervention studies that focused on surrogate markers. Although short-term randomised trials have suggested that replacement of animal proteins with plant proteins may slightly improve HbA1c and FPG in patients with type 2 diabetes10, the long-term consequences of dietary protein intake in patients with type 2 diabetes have been inconsistent. Therefore, there is a pressing need to presenting high-quality evidence on the association between dietary proteins and all-cause mortality risk in patients with type 2 diabetes. Our research provides corroborative evidence that aligns with existing guidelines advocating for an increase in the consumption of animal-based proteins while advising a reduction in the intake of proteins derived from red meat, particularly processed meat34,35,36.
Our study is strengthened by the inclusion of a nationally representative sample of patients with type 2 diabetes from the continuous NHANES data from 1999 to 2018. Furthermore, we limited our analyses to patients with reliable dietary recalls, conducted multiple subgroup and sensitivity analyses, and controlled for a wide array of potential confounders including sociodemographic variables, lifestyle factors, glycemic control, blood lipids, diabetes duration, and insulin usage. Certain limitations have the potential to influence the outcomes of our research findings. First, despite utilizing data from a prospective cohort study, the observational design of the study prevented the establishment of causality. Additionally, self-administered dietary evaluation instruments like dietary recalls are prone to measurement errors. Furthermore, dietary evaluations were conducted only once at the beginning of the study, therefore, any possible alterations in dietary habits throughout the duration of the study were not considered. Finally, it is important to consider the potential impacts of unidentified and residual confounding factors while interpreting the findings.
Conclusions
The prospective cohort study we conducted on patients with type 2 diabetes who were part of continuous NHANES from 1999 to 2018 revealed that a higher adherence to a dietary pattern abundant in proteins from fruits, fish, nuts, seeds, and legumes, while being low in red meat protein, may be linked to a reduced risk of mortality in individuals with type 2 diabetes. Greater adherence to “red meat and egg” dietary protein pattern was linked with an increased risk. Further longitudinal studies are required to validate our results and identify beneficial sources of dietary protein for individuals with type 2 diabetes.
Data availability
Data availability statement: Data described in the manuscript, code book, and analytic code generated in this study are available from the corresponding author upon request.
References
Zimmet, P., Alberti, K. G., Magliano, D. J. & Bennett, P. H. Diabetes mellitus statistics on prevalence and mortality: facts and fallacies. Nat. Reviews Endocrinol. 12 (10), 616–622 (2016).
Sun, H. et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 183, 109119 (2022).
Forouhi, N. G., Misra, A., Mohan, V., Taylor, R. & Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. Bmj. 361, 2234. https://doi.org/10.1136/bmj.k2234 (2018).
Zheng, Y., Ley, S. H. & Hu, F. B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Reviews Endocrinol. 14 (2), 88–98 (2018).
Rodriguez, N. R. Introduction to protein Summit 2.0: continued exploration of the impact of high-quality protein on optimal health. Am. J. Clin. Nutr. 101 (6), 1317s–9s (2015).
Solon-Biet, S. M. et al. The ratio of macronutrients, not caloric intake, dictates cardiometabolic health, aging, and longevity in ad libitum-fed mice. Cell Metabol. 19 (3), 418–430 (2014).
Wycherley, T. P., Moran, L. J., Clifton, P. M., Noakes, M. & Brinkworth, G. D. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 96 (6), 1281–1298 (2012).
Santesso, N. et al. Effects of higher-versus lower-protein diets on health outcomes: a systematic review and meta-analysis. Eur. J. Clin. Nutr. 66 (7), 780–788 (2012).
Dong, J. Y., Zhang, Z. L., Wang, P. Y. & Qin, L. Q. Effects of high-protein diets on body weight, glycaemic control, blood lipids and blood pressure in type 2 diabetes: meta-analysis of randomised controlled trials. Br. J. Nutr. 110 (5), 781–789 (2013).
Viguiliouk, E. et al. Effect of replacing animal protein with plant protein on glycemic control in diabetes: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 7 (12), 9804–9824 (2015).
Barbaresko, J. et al. Dietary factors and all-cause mortality in individuals with type 2 diabetes: a systematic review and meta-analysis of prospective observational studies. Diabetes Care. 46 (2), 469–477 (2023).
Dunkler, D. et al. Diet and kidney disease in high-risk individuals with type 2 diabetes mellitus. JAMA Intern. Med. 173 (18), 1682–1692 (2013).
Huang, J. et al. Association between plant and animal protein intake and overall and cause-specific mortality. JAMA Intern. Med. 180 (9), 1173–1184 (2020).
Song, M. et al. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 176 (10), 1453–1463 (2016).
Wang, W. et al. Dietary iron and vitamins in association with mortality. Clin. Nutr. 40 (4), 2401–2409 (2021).
Hu, F. B. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr. Opin. Lipidol. 13 (1), 3–9 (2002).
Centers for Disease Control and Prevention. The National Health and Nutritional Examination Survey (NHANES) Analytic and Reporting Guidelines. Atlanta, CDC, (2006).
Qiu, Z. et al. Associations of serum carotenoids with risk of cardiovascular mortality among individuals with type 2 diabetes: results from NHANES. Diabetes care. 45 (6), 1453–1461 (2022).
Michels, K. B. et al. Prospective study of fruit and vegetable consumption and incidence of colon and rectal cancers. J. Natl Cancer Inst. 92 (21), 1740–1752 (2000).
National Center for Health Statistics. The Linkage of National Center for Health Statistics Survey Data to the National Death Index—2019 Linked Mortality File (LMF): Linkage Methodology and Analytic Considerations. Hyattsville, Maryland (2022)
Beddhu, S., Baird, B. C., Zitterkoph, J., Neilson, J. & Greene, T. Physical activity and mortality in chronic kidney disease (NHANES III). Clin. J. Am. Soc. Nephrol. CJASN. 4 (12), 1901 (2009).
Zhang, W. & Peng, S. F. Association between the oxidative balance score and telomere length from the National Health and Nutrition Examination Survey 1999–2002. 2022:1345071 (2022).
Control CfD Prevention. NHANES laboratory/medical Technologists Procedures Manual (Centers for Disease Control and Prevention (2001).
Jolliffe, I. T. & Cadima, J. Principal component analysis: a review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 374 (2065), 20150202 (2016).
Mazza, E. et al. Association of dietary patterns with Sarcopenia in adults aged 50 years and older. Eur. J. Nutr. 63(5), 1651-1662. https://doi.org/10.1007/s00394-024-03370-6 (2024).
Herrick, K. A., Rossen, L. M., Parsons, R. & Dodd, K. W. Estimating usual dietary intake from National Health and Nutrition Examination Survey data using the National Cancer Institute method. (2018).
Institute, N. C. Usual dietary intakes: the NCI method. Retrieved from the National Cancer Institute website (2018).
National Cancer Institute. Usual Dietary Intakes: Details of the Method [updated December 14, 2021; cited 2022 February 23]. https://epi.grants.cancer.gov/diet/usualintakes/details.html
Bonaccio, M. et al. Adherence to the traditional Mediterranean diet and mortality in subjects with diabetes. Prospective results from the MOLI-SANI study. Eur. J. Prev. Cardiol. 23 (4), 400–407 (2016).
Patel, Y. R., Gadiraju, T. V., Gaziano, J. M. & Djoussé, L. Adherence to healthy lifestyle factors and risk of death in men with diabetes mellitus: the Physicians’ Health Study. Clin. Nutr. (Edinburgh, Scotland) 37 (1), 139–143 (2018).
Sijtsma, F. P. et al. Healthy eating and lower mortality risk in a large cohort of cardiac patients who received state-of-the-art drug treatment. Am. J. Clin. Nutr. 102 (6), 1527–1533 (2015).
Li, L. et al. Associations of healthy dietary patterns with mortality among people with prediabetes. 62(3), 1377–1387. https://doi.org/10.1007/s00394-022-03078-5 (2023).
Jayedi, A., Soltani, S., Abdolshahi, A. & Shab-Bidar, S. Fish consumption and the risk of cardiovascular disease and mortality in patients with type 2 diabetes: a dose-response meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 61 (10), 1640–1650 (2021).
ElSayed, N. A. et al. 5. Facilitating positive health behaviors and well-being to improve health outcomes: standards of care in Diabetes—2023. Diabetes Care. 46 (Supplement_1), S68–S96 (2023).
Evert, A. B. et al. Nutrition therapy for adults with diabetes or prediabetes: a consensus report. Diabetes care. 42 (5), 731 (2019).
Dyson, P. et al. Diabetes UK evidence-based nutrition guidelines for the prevention and management of diabetes. Diabet. Med. 35 (5), 541–547 (2018).
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
Authors Contributions: Conceptualization: Ahmad Jayedi, Methodology: Ahmad Jayedi, Formal analysis and investigation: Ahmad Jayedi, Alireza Emadi, and Mahdieh-sadat Zargar, Writing - original draft preparation: Ahmad Jayedi, Alireza Emadi, and Ali Najafi, Writing - review and editing: Ahmad Jayedi and Ali Najafi, Supervision: Ahmad Jayedi. Ahmad Jayedi had full access to all the data and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors have read and approved the final manuscript. Ahmad Jayedi is the guarantor.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jayedi, A., Zargar, MS., Najafi, A. et al. Patterns of protein intake and mortality in patients with type 2 diabetes: results from NHANES. Sci Rep 14, 26644 (2024). https://doi.org/10.1038/s41598-024-76357-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-76357-2
Keywords
This article is cited by
-
Is Plant Protein-Based Meat the Future? Exploring Recent Advances, Opportunities, and Challenges
Food and Bioprocess Technology (2026)
