
Abstract
The fragile X premutation is a public health concern worldwide. Implementing a comprehensive screening program for FMR1 premutation alleles could empower individuals and families with information, supporting informed health decisions and potentially reducing the incidence of fragile X syndrome (FXS). This study aimed to determine the prevalence of FMR1 premutations in the Thai population. We screened 369 female blood donors and 449 males with tremor and/or ataxia who tested negative for spinocerebellar ataxia (SCA) types 1, 2, and 3 for FMR1 CGG repeat expansions. Among the female blood donors, 0.27% (1/369) had a premutation allele, and 1.08% (4/369) had intermediate alleles. One female with a premutation carrier had 89 CGG repeats with one AGG interruption. In the male cohort, no premutations or full mutations were found; however, intermediate alleles were identified in 0.67% (3/449) of the males. This study provides the evidence of fragile X premutation screening in the Thai population. These findings contribute to the understanding of FMR1 premutation prevalence in Thailand and should encourage wider discussions on the feasibility for a national fragile X carrier screening program in Thailand to reduce the burden of fragile X-associated disorders.
Similar content being viewed by others


Introduction
Fragile X syndrome (FXS, OMIM 300624) is the most common inherited cause of intellectual disability, affecting approximately 1 in 4000–6000 males and 1 in 6000–8000 females1,2. FXS is caused by cysteine-guanine-guanine (CGG) repeat expansions in the 5′-untranslated region (UTR) of the FMR1 gene on the X chromosome. CGG repeat expansion mutations lead to gene methylation and subsequent silencing of FMR1 expression. There are four allelic forms of the FMR1 gene that are categorized based on the CGG repeat length: normal alleles with fewer than 45 repeats, intermediate alleles with 45–54 repeats, premutation alleles with 55–200 repeats, and full mutation alleles with more than 200 repeats. Full mutation expansions generally become methylated in the promoter and CGG-repeat regions, resulting in FMR1 gene silencing and the absence of the FMRP protein, which leads to FXS. Individuals carrying premutations are not affected by FXS, but premutation alleles can expand to full mutations in their offspring, which almost always occur through maternal transmission. Premutation carrier status often goes unnoticed by individuals, leaving them unaware of their risk for having an affected FXS child. All sizes of premutation alleles can expand into a full mutation in a single female meiosis, but larger premutation alleles expand more frequently to full mutations than smaller ones. Moreover, the presence of AGG interruptions decreases the intergenerational repeat instability of CGG repeats, thus reducing the risk of expansion to a full mutation allele during parental transmission3,4. Although males with a premutation pass on the premutation allele to all of their daughters without the repeat expanding to the full mutation range, in the next generation all daughters of males carrying a fragile X premutation will inherit the premutation allele and will be at risk of having sons with FXS and fragile X heterozygous daughters5. In general practice, females heterozygous for full mutation alleles are also diagnosed with FXS. However, females with full mutations have variable clinical presentations, ranging from no detectable deficits to clinical symptoms as severe as those seen in affected male5.
Initial investigations into FXS centered on the notion that a carrier’s primary concern was the risk of passing the gene to their offspring. However, the current understanding is that fragile X premutation carriers face health concerns beyond genetic transmission to their children. Individuals carrying a premutation allele do not have FXS but are at increased risk for fragile X premutation associated conditions (FXPAC), including fragile X-associated primary ovarian insufficiency (FXPOI) in females, and fragile X-associated tremor/ataxia syndrome (FXTAS) and fragile X-associated neuropsychiatric disorders (FXAND) in both male and female carriers of a premutation allele6. These conditions significantly impact both quality of life and parenting. Identifying the FMR1 premutation is crucial for accurate diagnosis, genetic counseling, and appropriate management for affected individuals and their families. For FXTAS, early identification enables the implementation of management strategies such as physical therapy and medications to control symptoms. In the case of FXPOI, screening provides critical information for fertility planning and hormonal management. Women identified with a premutation can make informed decisions about family planning and seek appropriate hormonal treatments to manage symptoms associated with premature ovarian insufficiency. This can lead to better reproductive outcomes and improved overall health. For FXAND, knowing one’s premutation status provides access to psychiatric support and behavioral therapies6,7. Therefore, identifying premutations facilitates personalized genetic counseling, helping individuals understand their risks, manage symptoms proactively, and make informed decisions about their health and family planning.
Fragile X premutation screening is now recommended to determine whether patients suspected of having fragile X-associated conditions have an FMR1 premutation allele. The core presenting features of FXTAS include intention tremors and cerebellar ataxia. FXTAS possibly remains underdiagnosed due to its rarity, lack of recognition, and overlap with many neurodegenerative disorders manifesting with cerebellar ataxia as the major clinical presentation, including spinocerebellar ataxia (SCA). Several previous studies have screened for FMR1 premutations in male patients who tested negative for SCA, reporting prevalence rates of FMR1 premutation alleles in patients with movement disorders ranging from 0 to 4%8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24.
Premutation carrier testing is also recommended for any preconception or pregnant woman who expresses interest in or requests Fragile X carrier testing25,26. Population carrier screening and newborn screening for FXS are currently considered controversial and are not currently recommended; however, there is growing interest in screening programs in general populations and advocacy for universal screening due to the high prevalence of premutations27. Previous studies have explored wider screening for FXS in populations beyond those recommended by guidelines28,29,30. The results from these studies were encouraging, although they faced practical difficulties such as ethical considerations and the cost-effectiveness of expanded screening. Screening for fragile X expanded carriers is essential for providing accurate genetic counseling, family planning, and early intervention, especially for individuals who are unaware that they have the condition6. The prevalence of premutations in the general population is estimated to be between 1 in 250 to 1 in 850 in males and 1 in 110 to 1 in 300 in females2,31,32. The variability in prevalence rates across studies may be explained by sample selection, sample size, founder effects, ethnic differences, the use of different detection methods, imprecision in laboratory measurements of repeat numbers, and nonidentical definitions of premutation alleles33.
Despite the importance of fragile X premutation screening, limited data are available on its prevalence and impact in many countries, especially Southeast Asian countries including Thailand. The premutation frequency might differ across populations; however, in Thailand, there has been only one recent study that screened for FMR1 premutation carriers in reproductive women34. Understanding the prevalence of fragile X premutations is important, particularly in the context of reproductive health and genetic counseling. This research aimed to investigate the prevalence of fragile X premutations among two distinct groups in Thailand: females who were blood donors representing the general female population and males presenting with tremor and/or ataxia who tested negative for SCA types 1, 2, and 3. These groups represent unique cohorts within which identifying fragile X premutations could have significant clinical implications.
Materials and methods
Participants
This retrospective study was conducted at Songklanagarind Hospital, a main laboratory for FXS diagnosis in Thailand. Two groups of participants were recruited for the study, who represented two groups of the Thai population: 369 female blood donors and 449 males with tremor and/or ataxia who tested negative for SCA 1, 2, and 3 (Fig. S1). The study was approved by the Ethics Committee, Faculty of Medicine, Prince of Songkla University (REC.62-018-5-2) and the Ethics Committee, Faculty of Medicine Siriraj Hospital, Mahidol University (190/2562 (EC3)). All methods were performed in accordance with the relevant guidelines and regulations.
To screen for fragile X premutation carriers in the general Thai population, the sample size was calculated using the single population proportion formula based on the prevalence of premutations in the general female population, reported in a previous study as approximately 0.9%35, 1% marginal error (d) and Zα/2 Standard variant (1.96) which corresponded to a 95% confidence interval. This yielded a total sample size of 343 individuals. However, our study included a total of 369 available DNA samples. Female participants were recruited voluntarily from blood donor populations at the Blood Bank Units of Thammasat University Hospital (Central Thailand) and Songklanagarind Hospital (Southern Thailand), with informed consent. All participants were screened via questionnaires to ensure that they had no current or past psychiatric or neurological disorders, developmental delays, learning disabilities, medical disorders affecting the central nervous system, were not taking any regular medications, and had no family history of psychiatric or neurological disorders across three generations. The mean age of the participants was 30.4 years (standard deviation (SD) 8.8) at the time of recruitment.
To screen for a fragile X premutation in males with tremor and/or ataxia exhibiting some clinical features suspicious for FXTAS, 449 Thai males referred for SCA testing and found negative for repeat expansions in the ATXN1 for SCA1, ATXN2 for SCA2, and ATXN3 for SCA3 were included in this study. We excluded males with obvious physical characteristics or symptoms related to other genetic disorders. Males who were diagnosed with other disorders, such as a brain tumor, were also excluded. The average age of this cohort was 48.6 years (SD 15.2).
In order to compare the frequency and distribution of FMR1 CGG repeats, a total of 212 normal Thai males collected from a previous study were used as the control group36. The control group was recruited voluntarily from blood donor populations consisting of individuals who did not take regular medications and had no known psychiatric or neurological disorders, developmental delays, or learning disabilities, thus representing a healthy population. Among the normal males, the mean age at their examinations was 31.2 years (SD 9.35).
FXS DNA analysis
Genomic DNA was extracted from peripheral blood using the standardized phenol-chloroform method or a FlexiGene DNA Kit (Qiagen, Germany). For FXS testing, the DNA quality required an A260/280 ratio of 1.7–2.0 and an A260/230 ratio of > 1.8. All individuals were screened using standard molecular methods and FMR1 CGG repeats were classified according to the American College of Medical Genetics and Genomics (ACMG) Standards and Guidelines for Fragile X Testing5. All samples were first analyzed using fluorescent PCR to screen for CGG repeats of the FMR1 gene following the method used in previous studies37,38 with slight modifications. The PCR reactions were performed in 10 µl mixtures containing 50 ng DNA, 1X ImmoBuffer (Bioline), 1.5 mM MgCl2, 200 µM dNTPs (dGTP replaced with 7-deaza dGTP), 2.2 M betaine, 0.2 µM each of the primers FRAXA-PSU-F (5′-6FAM-CAGCGTTGATCACGTGACGTGGTTTCAGTG-3′)36 and Primer3-R (5′-GTGGGCTGCGGGCGCTCGAGG-3′)39, and 0.5 units of Taq DNA Polymerase (Immolase, Bioline). The thermal cycling was as follows: denaturation at 95 °C for 15 min, 10 cycles of 95 °C for 30 s, 64 °C for 35 s, and 72 °C for 2 min, followed by 25 cycles of 95 °C for 35 s, 64 °C for 35 s, and 72 °C for 2 min with a 10 s increment per cycle, and a final extension at 72 °C for 10 min. One microliter of PCR product was then mixed with 10.7 µl of HiDi formamide and 0.3 µl of LIZ600, then denatured at 95 °C for 2 min and 4 °C for 5 min. The PCR mixture was loaded on an ABI3500 Genetic Analyzer (Applied Biosystems) and analyzed using GeneMapper v5 software. The sizes of the CGG repeats of the normal, intermediate, premutation, and full mutation alleles were defined as < 45, 45–54, 55–200, and > 200 CGG repeats, respectively. Fluorescent PCR using primers that flank the CGG repeat was employed to amplify FMR1 alleles containing CGG repeats usually up to the lower premutation range. Triplet repeat-primed PCR and methylation-specific PCR were then used to determine the expanded alleles in females and males, respectively.
Methylation-specific PCR (MS-PCR) was subsequently performed to determine the methylation status in the male samples carrying a premutation allele or suspected full mutation allele, as detected by fluorescent PCR following the method used in a previous study40. Briefly, the DNA samples were treated with sodium bisulfite using a commercial kit (EZ DNA Methylation-Gold Kit, Zymo Research, USA), following the manufacturer’s protocol. PCR amplification was performed using the four sets of primers from the previous study40. A single multiplex PCR was set up in a 15 µl reaction volume, comprising 0.24 µM of a pair of PUF and PUR primers, 0.24 µM of a pair of PMF and PMR primers, 0.24 µM of a pair of XUF and XUR primers, 0.1 µM of a pair of XMF and XMR primers, 1X PCR buffer (Qiagen, containing 1.5 mM MgCl2), 1.0 mM MgCl2, 0.2 mM dNTPs, 1 unit of Taq DNA polymerase (Hot Start, Qiagen), and 200–300 ng of bisulfite-treated DNA. Thermal cycling was as follows: initial denaturation at 95ºC for 10 min, followed by 40 cycles of 95 °C for 1 min, 61 °C for 45 s, and 72 °C for 45 s, with a final extension at 72 °C for 10 min. The PCR products were separated on 2.5% agarose gel, stained with ethidium bromide, and visualized under a UV transilluminator. This MS-PCR assay can distinguish between full mutation males and normal males. However, this method does not identify the number of CGG repeats because the PCR does not amplify across this region; therefore, it cannot distinguish normal males from premutation males. Moreover, MS-PCR cannot be used for females due to random X-inactivation, which prevents the method from distinguishing premutation or full mutation females from normal females who have the same pattern. Consequently, in female samples, triplet repeat-primed PCR (TP-PCR) was performed instead of MS-PCR. TP-PCR41 of the FMR1 gene was used to detect the presence of premutations and/or full mutations in samples where the fluorescent PCR results suggested repeat expansions. TP-PCR was also used to determine the AGG interruption patterns within the CGG repeats in individuals with intermediate, premutation, and full mutation statuses.
Southern blot analysis was used to confirm large expanded alleles and methylation status for CGG repeats in the suspected premutation and full mutation ranges observed in the PCR results. Briefly, 8–10 µg of genomic DNA from blood was digested with EcoR I/Eag I, and hybridized with an FMR1-specific genomic probe (StB12.3) as described elsewhere38. Sanger DNA sequencing was applied to confirm the accuracy of the numbers of FMR1 CGG repeats and AGG interruptions, as well as the positions of the AGG within the CGG-repeat loci in individuals with premutation alleles using the primers reported in a previous study42.
Statistical analysis
Fisher’s exact test was used to determine the differences in frequencies between the male cohort and the normal male controls. Pairwise comparisons were adjusted for multiple comparisons using the Bonferroni method to evaluate differences in frequencies between the current study and previous studies. Values of p < 0.05 were considered to indicate statistical significance. The exact binomial test was performed using the R program to calculate the 95% confidence intervals (CIs) for the prevalence of the premutation and intermediate alleles.
Results
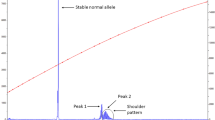
Of the 369 female random blood donors screened, 364 (98.64%) carried normal repeat alleles. The screening identified 4 subjects with intermediate alleles (1.08%, 95% CI 0.30–2.75%) and one carrier with a premutation allele (0.27%, 95% CI 0.01–1.50%) (Fig. S2). The prevalence of FMR1 premutations in the random Thai female blood donors of our study was therefore 1 in 369. No full mutations were detected in this cohort. Among the 449 males with tremor and/or ataxia who tested negative for SCA 1, 2, and 3, and were screened to identify potential cases of FXTAS due to the overlap in clinical features with other neurodegenerative disorders, three cases (3/449, 0.67%, 95% CI 0.14–1.95%) were found to have CGG repeats falling into the intermediate category. The remaining 446 males (99.33%) had normal CGG repeats. No premutations or full mutations were identified in the screened males. No significant differences were observed when comparing the frequencies of FMR1 intermediate alleles between the SCA-negative Thai males and the normal Thai males (3/449 versus 0/202 cases, p-value = 0.5550). The results of the FMR1 CGG repeat analysis are summarized in Table 1. The most frequent number of FMR1 CGG repeats in the cohorts was 29, followed by 30 and 36. The distributions of allele frequencies for FMR1 CGG repeats in the two studied cohorts of the Thai population with normal CGG repeat numbers are shown in Fig. 1.

Distribution of the sizes of the normal CGG repeat alleles (< 45 CGG) analyzed in this study. The most frequent FMR1 allele sizes in the population were 29 repeats, 30 repeats, and minor peaks at 36 repeats.
TP-PCR analysis was performed to determine the AGG interruption patterns in individuals with intermediate and premutation alleles. Most of the expanded alleles exhibited at least one AGG interruption. However, a notable exception was observed in one female participant who carried a normal allele with 30 CGG repeats (10A9A9) and an intermediate allele with 46 CGG repeats without any AGG interruptions (Table 2).
Discussion
This study examines the prevalence of fragile X premutation screening in the Thai population, providing important insights into the prevalence of FMR1 premutations and intermediate alleles in Thailand. It represents a significant report on the prevalence of fragile X premutation in a Southeast Asian population. The most common number of CGG repeats in the two Thai cohorts was 29, followed by 30 and 36, which is consistent with allele distributions reported in a previous study of Thai patients with autism spectrum disorder36 and other Asian populations43. Among the 369 female random blood donors screened, we identified a single carrier of a premutation allele, representing a prevalence of 1/369 (0.27%, 95% CI 0.01–1.50%) of the FXS carriers in the general Thai population. While this finding provides an initial insight into the presence of fragile X premutation carriers in the Thai population, the sample size was not sufficient to allow the drawing of definitive conclusions about the actual population frequency. Further studies with larger cohorts are necessary to establish a more accurate prevalence rate. The absence of full mutation alleles in the female cohort aligns with the expected lower prevalence of full mutations in the general population. Additionally, in the female cohort, four out of 369 individuals (1.08%, 95% CI 0.30–2.75%) were detected as carriers of an intermediate allele. Both expansion and contraction of the CGG repeat size can occur when intermediate alleles are passed on, but there is no measurable risk of a child with FXS in the next generation5,44. The involvement of intermediate alleles in clinical, behavioral, and cognitive phenotypes remains controversial and needs to be further studied in larger cohorts across different populations with diverse genetic backgrounds. The detection of premutation carriers among potential mothers is significant for the potential transmission of these alleles to their own offspring, where expansions to full mutations could occur. Our study showing the frequency of fragile X premutations adds important information to the current discussion concerning implementation of an FXS carrier screening program in Thailand. We believe that the screening procedure used in our study can be adapted for a national fragile X carrier screening program in Thailand in the future. The screening methods employed in our study included fluorescent PCR for CGG repeat screening for all participants, TP-PCR for female participants, and MS-PCR for male participants. The cost per screening for FXS in this study was approximately 650 Thai Baht (~ 19 USD), with the cost for fluorescent PCR being 300 Thai Baht (~ 9 USD) per individual, while TP-PCR and MS-PCR each cost approximately 350 Thai Baht (~ 10 USD) per individual. This cost may vary between different institutes, as it is based solely on reagent costs (2024) and does not include other expenses such as laboratory management and equipment. The cost of FXS screening may be reduced if a larger number of samples are tested. Although there is ongoing debate regarding the screening for FXS and the appropriate model to use, particularly in a population-based screening program, some experts advocate for universal prenatal screening. They argue that it is more effective in identifying premutation carriers compared to case finding followed by cascade screening30,45. A previous literature review and modelling study indicated that the maximal rate of female premutation carriers detected by population screening (60%) was much greater than that detected by active cascade screening (6%)46. Although the population and prenatal screening programs were more effective than active cascade screening, they would cost much more46. Because family sizes tend to be small in many developed countries, the effectiveness of cascade screening has become significantly limited. A recent cost-effectiveness analysis model examining East Asian populations found that population-based screening was more cost-effective than targeted screening in providing families with information that can help reduce the incidence of FXS, thereby supporting informed reproductive choices. According to this model, targeted screening would miss approximately 69% of carriers47. Other studies have found that healthcare professionals and families of patients with FXS were in favor of prenatal screening for pregnant women or preconception women of reproductive age48,49,50. Although the benefits of prenatal screening for the early identification and intervention of FXS are widely recognized, population-based carrier screening is still not endorsed by professional guidelines due to the main concerns about a lack of disease education, insufficient cost-benefit evidence, the complexity of genetic counseling, and the potential for psychosocial harm. However, several national population-based screening programs, including FXS carrier screening, have already been implemented and have yielded positive outcomes in countries with high prevalences of FXS and fragile X premutations27,51,52.
The detection of fragile X premutation carriers also provides information about the women’s own health, as they are at increased risk of FXPAC. These factors may affect a woman’s fertility planning and allow informed choices not only in the current pregnancy but also in subsequent pregnancies. Individuals carrying premutation alleles are mostly concerned about the risk of having a child with CGG repeat expansions5,6,7. The majority of existing tests detect only the number of CGG repeats. Although higher CGG repeat numbers indicate a higher risk of expansion, AGG interspersion patterns are also an important factor in predicting CGG repeat instability3,4,53,54,55. The stability of the CGG repeats increases with increasing numbers of AGG interruptions, making them less likely to expand. The detection of AGG interruptions within FMR1 intermediate and premutation alleles is important in genetic counseling to better predict the risk of expansion during transmission. A previous study revealed that mothers with 2 AGG interruptions and an FMR1 repeat size of ~ 75 repeats had more than a 60% decreased risk of having a full mutation child compared to mothers with an allele with 0 AGG interruptions3. However, this and another study reported that nearly all premutation alleles with 90 repeats or more expanded to the full mutation upon transmission, and the presence of 1 or 2 AGG interruptions did not decrease the risk of having an offspring with a full mutation3,54. Therefore, the characterization of AGG interruptions is more important for premutation alleles with a smaller number of CGG repeats. Indeed, our analysis suggests that a Thai female with an FMR1 premutation carrying 89 CGG repeats and one AGG interruption (9A79) has an approximately 80–95% increased risk of expansion to a full mutation in her offspring when considering the number of CGG repeats along with AGG interruptions based on data from previous studies3,4.
The results of our study should be considered as an initial step for fragile X premutation screening and serve as a foundational basis due to the limitation of a small sample size. We also recommend that carrier screening to identify female carriers be conducted on a large scale in our population and extended to other Southeast Asian populations. The frequency of fragile X premutation carriers varies among different populations worldwide based on different subject groups and large sample sizes. The rates of female premutation carriers in the European and American populations are high28,32,35,52,56,57,58,59,60,61,62. Most studies have been conducted on East Asian populations34,47,63,64,65,66,67,68,69,70,71,72,73,74, and it has been observed that the population studied from Asian countries, including Japan, Taiwan, Korea, Hong Kong, and China, generally exhibited a lower prevalence of premutation alleles than other ethnic groups, especially those from Western countries1,58,59. During the review process of the manuscript, we recently found a coincidence in FXS screening among another cohort of Thai women. This recent study reported a prevalence of 2/1250 or 1 in 625 (0.16%, 95% CI 0.02–0.58%) for premutations and 3/1250 or 1 in 417 (0.24%, 95% CI 0.05–0.70%) for intermediate alleles34. Notably, this study specifically focused on reproductive women in the central region of Thailand, which differs from our study that involved the general female population in both the southern and central regions of Thailand. However, the prevalence of premutations in both studies of the Thai population showed similar trends and was consistent with those observed in other Asian populations. If we combine the populations of both studies, the prevalence of FMR1 premutations in the Thai female population is found to be 3/1,619 or 1 in 540 (0.19%, 95% CI 0.04−0.54%). Earlier studies have reported that the prevalence of fragile X premutation carriers in the general population in China ranged from 16/10,145 or 1 in 634 (0.16%, 95% CI 0.09−0.26%) to 29/11,891 or 1 in 410 (0.24%, 95% CI 0.16−0.35%)72,73,74. A large sample of 10,145 Chinese women of childbearing age was screened for fragile X carrier status, and 78 intermediate alleles were identified, resulting in a prevalence of 78/10,145 or 1 in 130 (0.77%, 95% CI 0.61−0.96%). The frequencies of premutation and full mutation carriers among these women were 16/10,145 (0.16%, 95% CI 0.09−0.26%) and 2/10,145 (0.02%, 95% CI 0−0.07%), respectively, giving an overall carrier frequency of 0.18% (18/10,145 or 1 in 564)74. The prevalence of FXS carriers in the population of Taiwan was estimated to be between 0/1,002 (0%, 95% CI 0−0.37%) and 68/39,458 (0.17%, 95% CI 0.13−0.22%)47,65,66,67,68. The overall prevalence of premutation and full mutation alleles among pregnant women in Hong Kong was 0.11% (3/2650). The frequency of fragile X premutation carriers was 2/2650 or 1 in 1,325 (0.08%, 95% CI 0.01−0.27%), while 30/2650 or 1 in 88 (1.13%, 95% CI 0.77−1.61%) of women were found to have intermediate alleles71. A large-scale fragile X carrier screening study in the United States found that the frequency of premutation carriers among women who self-identified as Asian was 19 out of 7961 or 1 in 419 (0.24%, 95% CI 0.14−0.37%) within a large and ethnically diverse population referred for carrier testing32. Tassone et al. (2012) observed a higher frequency in their Asian group compared to the overall population (1/123 versus 1/209)59. This discrepancy may be explained by the inclusion of individuals who identified as Indian within the Asian group, whereas individuals of Indian mixed ethnicity were categorized as other/mixed/unknown in another study32. It should be noted that some previous studies used different criteria for intermediate and premutation allele categories61,62,65. Thus, the prevalences of both alleles may be higher than in other studies that used the current ACMG categories of FMR1 alleles, leading to difficulty in comparing prevalences. For fragile X premutation carriers in the general population, the differences between our study and previous studies were not statistically significant (Table S1). A review of the literature on the prevalence of FMR1 expanded alleles in the general population of various countries is shown in Fig. 2 and Table S1.

Prevalence data of FMR1 intermediate (45–54 CGG) (A) and premutation (55–200 CGG) (B) alleles among various general populations. The data represent the prevalence among the general female population, except for the studies from Taiwan, which were conducted in newborn males as reported by Chow et al.66, and Tzeng et al.67.
The presence of an FMR1 premutation has been linked to patients with intention tremor and cerebellar ataxia, which is a core presenting feature of FXTAS. FXTAS is often mistaken for other movement disorders, including SCA. Therefore, this study also focused on the prevalence of FXTAS in Thai patients with tremor and/or ataxia who were negative for repeat expansions in SCA1, 2, and 3. Our screening of 449 SCA-negative males revealed no premutations; only three individuals (0.67%, 95% CI 0.14–1.95%) were found to carry alleles in the intermediate range, suggesting that FXTAS may be less common in this specific population. The low prevalence of premutation and intermediate alleles in our male cohort may support the belief that FXTAS is underdiagnosed due to its rarity and the overlap with other conditions. It also suggests that other genetic or environmental factors may contribute to the tremor and ataxia observed in these patients. This finding underscores the importance of comprehensive genetic screening and clinical evaluation in patients with tremor and ataxia to ensure accurate diagnosis and management. Several previous studies have been conducted to screen for FMR1 premutation expansions in males who tested negative for SCA. Among male patients with tremor and/or ataxia, the frequencies of FMR1 premutations in previous studies ranged from 0% (0/269) to 4% (5/122)8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24; however, few studies have been conducted in Asian populations. The frequency of premutations in males negative for SCA in our study was lower than that in other studies in European and American populations. The results of this study were similar to those of a study from Singapore12 but were lower than those of another study from India, where the frequency of premutation alleles in males was reported to be 3/80 or 1 in 27 (3.75%, 95% CI 0.78–10.46%)11, and Japan, where the prevalences of FMR1 premutation alleles were estimated to be 2/540 or 1 in 270 (0.37%, 95% CI 0.05–1.34%)10 and 2/100 or 1 in 50 (2%, 95% CI 0.24–7.01%)15 among patients with cerebellar ataxia who also tested negative for SCA. These discrepancies may be related to differences in the ethnic backgrounds of the populations as well as sample sizes and different criteria of patient selection. The selection of patient criteria is an important factor for any study examining fragile X premutation alleles in patients with suspected FXTAS. Our study only considered participants based on tremor and ataxia features, whereas other studies included additional criteria such as neurological features, age of onset, and/or age of recruitment. This approach could lead to the recruitment of participants who more closely resemble patients with FXTAS, thereby increasing the likelihood of detecting FMR1 premutations compared to our study. Moreover, the exclusion of individuals with obvious physical characteristics or symptoms related to other genetic disorders in our study was intended to focus on those most likely to have FXTAS. However, this approach may have inadvertently excluded individuals with atypical presentations of FXTAS or other related conditions. Because we did not have access to demographic or clinical information for our patient cohort, it is possible that some participants did not meet the criteria for fragile X premutation testing for FXTAS. A previous study in India, which found a high premutation frequency, recruited patients with SCA type 12-like phenotypes presenting with cerebellar ataxia or tremor along with other neurological features, such as upper limb incoordination, hand tremor, hyperreflexia, nystagmus, and Parkinsonian signs11. These clinical features are highly similar to the clinical symptoms of FXTAS. Therefore, to address these limitations, future studies should include a broader range of participants, including those with atypical FXTAS presentations. More consistent inclusion criteria will be required to accurately assess the frequency of FXTAS in the Thai population.
Our study did not find evidence of fragile X premutations in SCA 1, 2, and 3 negative Thai males with tremor and/or ataxia. However, the presence of intermediate alleles underscores the importance of FMR1 screening in this group and may aid in providing appropriate genetic counseling for patients harboring these alleles. Although intermediate alleles show a very low risk of expansion, they may still change during transmission and could be associated with FXS in future generations or distant relatives. Intermediate carriers are at a higher risk of CGG repeat expansion, which can result in premutation offspring or full mutation patients in subsequent generations. Previous studies reported a higher degree of instability in paternal than maternal transmissions of intermediate alleles53,75. An intermediate allele with 52 repeats was reported to expand to a premutation allele of 56 repeats in one generation, which subsequently expanded to a full mutation allele in the next generation76. Thus, testing at-risk relatives of individuals with an intermediate allele may determine the stability of the allele in the family. In our study, we observed a male patient with a high-repeat intermediate allele of 53 CGG repeats, which included one AGG interruption (10A42). Previous research indicated that the change in size for unstable paternal transmission of CGG repeats varies with the number of AGG interruptions. The risk of unstable transmission is approximately 100% in paternal alleles with a CGG size range of 50–54 repeats that lack AGG interruptions. In contrast, for these alleles with one AGG interruption, the size change was approximately 75%4. This suggests that the presence of AGG interruptions in a patient may reduce the risk of the allele expanding due to unstable transmission, supporting the idea that AGG interruptions can play a significant role in mitigating the risk of transmitting an FMR1 full mutation to future generations. The results of the present study also indicate avenues for further research into the genetic underpinnings of ataxia-like symptoms in populations in which SCA has been ruled out. Some studies have reported that intermediate alleles may be associated with a range of clinical features that overlap with those observed in FXTAS77,78,79. Previous studies have found that individuals with FMR1 repeat expansions in the intermediate range exhibited increased levels of FMR1 mRNA transcription and transcriptional activity, similar to the changes observed in premutation carriers with FXTAS77,80,81. The occurrence of FXTAS in individuals with intermediate alleles may be influenced by the presence of relatively high numbers of CGG repeats, which are associated with increased levels of FMR1 mRNA, combined with a family history of FXTAS that could provide a predisposing genetic background78. Despite this association being observed in previous studies, our research could not establish a correlation between clinical manifestations and the presence of FMR1 intermediate alleles in our patient cohort due to the limitation of clinical information available for this cohort. Although no significant difference was observed in the frequencies of intermediate alleles between SCA-negative males and normal Thai males, the number of intermediate alleles in the male cases (3/449) was higher than in the male controls (0/202). This result may serve as a basis for future studies investigating the stability and clinical implications of these alleles across diverse ethnicities and regions. Further research into the clinical implications of intermediate alleles is recommended to elucidate the role of FMR1 intermediate alleles in the broader spectrum of neurodevelopmental and neurodegenerative disorders including FXTAS.
One limitation of this study is that our cohorts mainly consisted of individuals from the southern and central regions of Thailand, which may not reflect the genetic diversity of the entire Thai population. Additionally, our female samples were obtained from random blood donors which might not accurately represent the overall population of women of reproductive age or pregnant women. The exclusion of individuals with personal or familial psychiatric disorders may have led to an underrepresentation of premutation carriers in our cohort. Future studies should consider broader inclusion criteria to capture a more representative sample of the general population, including those with psychiatric symptoms, to better understand the prevalence of fragile X premutation carriers. This study was also limited by its retrospective design, which involved the use of pre-existing anonymous blood samples from females. Consequently, we are unable at this time to provide genetic counseling and FMR1 DNA testing for at-risk family members of individuals with FMR1 expanded alleles, particularly fragile X premutation carriers. Despite these limitations, our study underscores the importance of understanding the prevalence of FMR1 premutations in the general Thai female population, representing a low-risk group, which is a critical first step in considering the implementation of a national screening program. The findings of our study provide a basis for further large-scale national studies that will enhance our understanding of carrier frequencies across different regions of Thailand and among other Asian populations. The results of this study also support further screening of the FMR1 gene, particularly in preconceptional or pregnant women and newborns, to enable early intervention and family planning, thus reducing the burden of FXS-associated disorders. Further studies are required to evaluate different models of fragile X screening programs and their cost-effectiveness in our region to determine the most suitable screening strategy for the Thai population and to engage stakeholders in developing screening guidelines. These efforts aim to establish a comprehensive national screening strategy, ensuring future accessibility for appropriate groups in Thailand.
Conclusion
This study investigates the prevalence of FMR1 premutations in the Thai population across unique cohorts, in which identifying fragile X premutations could have significant clinical implications. We found a premutation prevalence of 1 in 369 (0.27%, 95% CI 0.01−1.50%) among female blood donors. In males presenting with tremor and/or ataxia who tested negative for SCA types 1, 2, and 3, no premutations or full mutations were identified, but intermediate alleles were found in 3 out of 449 (0.67%, 95% CI 0.14−1.95%) of the male cohort. These findings underscore the importance of FMR1 carrier screening in Thailand as a means of providing individuals and families with critical information that can help prevent the transmission of FXS and FMR1-related disorders, thereby enhancing public health outcomes. Further large-scale studies on the prevalence of the fragile X premutation in Thailand and different areas of Asia may be beneficial for developing future screening strategies.
Data availability
The datasets generated and/or analysed during the current study are available in the corresponding author repository.
References
Hill, M. K., Archibald, A. D., Cohen, J. & Metcalfe, S. A. A systematic review of population screening for fragile X syndrome. Genet. Med. 12, 396–410 (2010).
Hunter, J. et al. Epidemiology of fragile X syndrome: A systematic review and meta-analysis. Am. J. Med. Genet. A 164A, 1648–1658 (2014).
Yrigollen, C. M. et al. AGG interruptions and maternal age affect FMR1 CGG repeat allele stability during transmission. J. Neurodev. Disord. 6, 24 (2014).
Nolin, S. L. et al. Fragile X full mutation expansions are inhibited by one or more AGG interruptions in premutation carriers. Genet. Med. 17, 358–364 (2015).
Spector, E. et al. Laboratory testing for fragile X, 2021 revision: A technical standard of the American College of Medical Genetics and Genomics (ACMG). Genet Med 23, 799–812 (2021).
Tassone, F. et al. Insight and recommendations for fragile X-premutation-associated conditions from the fifth international conference on FMR1 premutation. Cells 12, 2330 (2023).
Johnson, K. et al. A holistic approach to fragile X syndrome integrated guidance for person-centred care. J. Appl. Res. Intellect. Disabil. 37, e13214 (2024).
Reis, A. H. O. et al. Frequency of FMR1 premutation in individuals with ataxia and/or tremor and/or parkinsonism. Genet. Mol. Res. 7, 74–84 (2008).
Seixas, A. I. et al. FXTAS is rare among Portuguese patients with movement disorders: FMR1 premutations may be associated with a wider spectrum of phenotypes. Behav. Brain Funct. 7, 19 (2011).
Higuchi, Y. et al. Prevalence of fragile X-associated tremor/ataxia syndrome in patients with cerebellar Ataxia in Japan. Cerebellum 21, 851–860 (2022).
Faruq, M. et al. Identification of FXTAS presenting with SCA 12 like phenotype in India. Parkinsonism Relat. Disord. 20, 1089–1093 (2014).
Tan, E. K. et al. Fragile X premutation alleles in SCA, ET, and parkinsonism in an Asian cohort. Neurology 63, 362–363 (2004).
Van Esch, H. et al. Screening for FMR-1 premutations in 122 older Flemish males presenting with ataxia. Eur. J. Hum. Genet. 13, 121–123 (2005).
Macpherson, J., Waghorn, A., Hammans, S. & Jacobs, P. Observation of an excess of fragile-X premutations in a population of males referred with spinocerebellar ataxia. Hum. Genet. 112, 619–620 (2003).
Almansour, A. et al. Frequency of FMR1 premutation alleles in patients with undiagnosed cerebellar ataxia and multiple system atrophy in the japanese population. Cerebellum 21, 954–962 (2022).
Pešić, M. et al. Premutations in the FMR1 gene in Serbian patients with undetermined tremor, ataxia and parkinsonism. Neurol. Res. 43, 321–326 (2021).
Seixas, A. I. et al. FXTAS, SCA10, and SCA17 in American patients with movement disorders. Am. J. Med. Genet. A 136, 87–89 (2005).
Rajkiewicz, M. et al. Screening for premutation in the FMR1 gene in male patients suspected of spinocerebellar ataxia. Neurol. Neurochir. Pol. 42, 497–504 (2008).
Adams, S. A., Steenblock, K. J., Thibodeau, S. N. & Lindor, N. M. Premutations in the FMR1 gene are uncommon in men undergoing genetic testing for spinocerebellar ataxia. J. Neurogenet. 22, 77–92 (2008).
Milunsky, J. M. & Maher, T. A. Fragile X carrier screening and spinocerebellar ataxia in older males. Am. J. Med. Genet. A 125A, 320 (2004).
Rodriguez-Revenga, L. et al. FXTAS in Spanish patients with ataxia: Support for female FMR1 premutation screening. Mol. Neurobiol. 35, 324–328 (2007).
Cellini, E. et al. Fragile X premutation with atypical symptoms at onset. Arch. Neurol. 63, 1135–1138 (2006).
Brussino, A. et al. FMR1 gene premutation is a frequent genetic cause of late-onset sporadic cerebellar ataxia. Neurology 64, 145–147 (2005).
Zühlke, C. et al. FMR1 premutation as a rare cause of late onset ataxia–evidence for FXTAS in female carriers. J. Neurol. 251, 1418–1419 (2004).
Sherman, S., Pletcher, B. A. & Driscoll, D. A. Fragile X syndrome: Diagnostic and carrier testing. Genet. Med. 7, 584–587 (2005).
American College of Obstetricians and Gynecologists Committee on Genetics. ACOG committee opinion No. 469: Carrier screening for fragile X syndrome. Obstet. Gynecol. 116, 1008–1010 (2010).
Archibald, A. D. et al. Reproductive genetic carrier screening for cystic fibrosis, fragile X syndrome, and spinal muscular atrophy in Australia: Outcomes of 12,000 tests. Genet Med 20, 513–523 (2018).
Berkenstadt, M., Ries-Levavi, L., Cuckle, H., Peleg, L. & Barkai, G. Preconceptional and prenatal screening for fragile X syndrome: Experience with 40,000 tests. Prenat. Diagn 27, 991–994 (2007).
Alfaro Arenas, R., Rosell Andreo, J., Heine Suñer, D., Group for the study of FXS in the Balearic Islands. A pilot study of fragile X syndrome screening in pregnant women and women planning pregnancy: Implementation, acceptance, awareness, and geographic factors. J. Genet. Couns. 26, 501–510 (2017).
Johansen Taber, K., Lim-Harashima, J., Naemi, H. & Goldberg, J. Fragile X syndrome carrier screening accompanied by genetic consultation has clinical utility in populations beyond those recommended by guidelines. Mol. Genet. Genomic Med. 7, e1024 (2019).
Hagerman, R. J. et al. Fragile X syndrome. Nat. Rev. Dis. Primers 3, 17065 (2017).
Owens, K. M. et al. FMR1 premutation frequency in a large, ethnically diverse population referred for carrier testing. Am. J. Med. Genet. A 176, 1304–1308 (2018).
Ciobanu, C.-G. et al. Narrative review: Update on the molecular diagnosis of fragile X syndrome. Int J Mol Sci. 24, 9206 (2023).
Ain, Q. et al. Population-based FMR1 carrier screening among reproductive women. J. Assist. Reprod. Genet. https://doi.org/10.1007/s10815-024-03242-2 (2024).
Toledano-Alhadef, H. et al. Fragile-X carrier screening and the prevalence of premutation and full-mutation carriers in Israel. Am. J. Hum. Genet. 69, 351–360 (2001).
Hnoonual, A., Jankittunpaiboon, C. & Limprasert, P. Screening for FMR1 CGG repeat expansion in Thai patients with autism spectrum disorder. Biomed. Res. Int. 2021, 4359308 (2021).
Jankittunpaiboon, C. Mutation Screening and Association Study of the FMR1 Gene in Thai Patient with Autism (Prince of Songkla University, 2008).
Hnoonual, A., Plong-On, O., Worachotekamjorn, J., Charalsawadi, C. & Limprasert, P. Clinical and molecular characteristics of FMR1 microdeletion in patient with fragile X syndrome and review of the literature. Clin. Chim. Acta 553, 117728 (2024).
Brown, W. T. et al. Rapid fragile X carrier screening and prenatal diagnosis using a nonradioactive PCR test. JAMA 270, 1569–1575 (1993).
Charalsawadi, C., Sripo, T. & Limprasert, P. Multiplex methylation specific PCR analysis of fragile X syndrome: Experience in Songklanagarind Hospital. J. Med. Assoc. Thai. 88, 1057–1061 (2005).
Tassone, F., Pan, R., Amiri, K., Taylor, A. K. & Hagerman, P. J. A rapid polymerase chain reaction-based screening method for identification of all expanded alleles of the fragile X (FMR1) gene in newborn and high-risk populations. J. Mol. Diagn. 10, 43–49 (2008).
Zhou, Y. et al. Robust fragile X (CGG)n genotype classification using a methylation specific triple PCR assay. J. Med. Genet. 41, e45 (2004).
Peprah, E. Fragile X syndrome: The FMR1 CGG repeat distribution among world populations. Ann. Hum. Genet. 76, 178–191 (2012).
Nolin, S. L. et al. Familial transmission of the FMR1 CGG repeat. Am. J. Hum. Genet. 59, 1252–1261 (1996).
Musci, T. J. & Moyer, K. Prenatal carrier testing for fragile X: Counseling issues and challenges. Obstet. Gynecol. Clin. North Am. 37, 61–70 (2010).
Song, F. J., Barton, P., Sleightholme, V., Yao, G. L. & Fry-Smith, A. Screening for fragile X syndrome: A literature review and modelling study. Health Technol. Assess 7, 1–106 (2003).
Guo, Q. et al. Population-based carrier screening and prenatal diagnosis of fragile X syndrome in East Asian populations. J. Genet. Genom. 48, 1104–1110 (2021).
Skinner, D., Sparkman, K. L. & Bailey, D. B. Screening for Fragile X Syndrome: Parent attitudes and perspectives. Genet. Med. 5, 378–384 (2003).
Acharya, K. & Ross, L. F. Fragile X screening: Attitudes of genetic health professionals. Am. J. Med. Genet. A 149A, 626–632 (2009).
Zhu, Y. et al. Attitudes of medical professionals toward fragile X carrier screening and genetic counseling in China. J. Commun. Genet. 15, 177–185 (2024).
Zlotogora, J., Grotto, I., Kaliner, E. & Gamzu, R. The Israeli national population program of genetic carrier screening for reproductive purposes. Genet. Med. 18, 203–206 (2016).
Westemeyer, M. et al. Clinical experience with carrier screening in a general population: Support for a comprehensive pan-ethnic approach. Genet. Med. 22, 1320–1328 (2020).
Nolin, S. L. et al. Expansion of the fragile X CGG repeat in females with premutation or intermediate alleles. Am. J. Hum. Genet. 72, 454–464 (2003).
Nolin, S. L. et al. Fragile X analysis of 1112 prenatal samples from 1991 to 2010. Prenat. Diagn. 31, 925–931 (2011).
Nolin, S. L. et al. Expansions and contractions of the FMR1 CGG repeat in 5,508 transmissions of normal, intermediate, and premutation alleles. Am. J. Med. Genet. A 179, 1148–1156 (2019).
Rousseau, F., Rouillard, P., Morel, M. L., Khandjian, E. W. & Morgan, K. Prevalence of carriers of premutation-size alleles of the FMRI gene–and implications for the population genetics of the fragile X syndrome. Am. J. Hum. Genet. 57, 1006–1018 (1995).
Lévesque, S. et al. Screening and instability of FMR1 alleles in a prospective sample of 24,449 mother-newborn pairs from the general population. Clin. Genet. 76, 511–523 (2009).
Hantash, F. M. et al. FMR1 premutation carrier frequency in patients undergoing routine population-based carrier screening: Insights into the prevalence of fragile X syndrome, fragile X-associated tremor/ataxia syndrome, and fragile X-associated primary ovarian insufficiency in the United States. Genet. Med. 13, 39–45 (2011).
Tassone, F. et al. FMR1 CGG allele size and prevalence ascertained through newborn screening in the United States. Genome Med. 4, 100 (2012).
Pesso, R. et al. Screening for fragile X syndrome in women of reproductive age. Prenat. Diagn. 20, 611–614 (2000).
Drasinover, V. et al. Increased transmission of intermediate alleles of the FMR1 gene compared with normal alleles among female heterozygotes. Am. J. Med. Genet. 93, 155–157 (2000).
Geva, E. et al. The risk of fragile X premutation expansion is lower in carriers detected by general prenatal screening than in carriers from known fragile X families. Genet. Test 4, 289–292 (2000).
Arinami, T., Asano, M., Kobayashi, K., Yanagi, H. & Hamaguchi, H. Data on the CGG repeat at the fragile X site in the non-retarded Japanese population and family suggest the presence of a subgroup of normal alleles predisposing to mutate. Hum. Genet. 92, 431–436 (1993).
Otsuka, S. et al. Fragile X carrier screening and FMR1 allele distribution in the Japanese population. Brain Dev. 32, 110–114 (2010).
Huang, K.-F. et al. Original article pilot screening for fragile X carrier in pregnant women of southern Taiwan. J. Chin. Med. Assoc. 66, 204–209 (2003).
Chow, J. C. et al. Feasibility of blood spot PCR in large-scale screening of fragile X syndrome in southern Taiwan. J. Formos. Med. Assoc. 102, 12–16 (2003).
Tzeng, C.-C. et al. Prevalence of the FMR1 mutation in Taiwan assessed by large-scale screening of newborn boys and analysis of DXS548-FRAXAC1 haplotype. Am. J. Med. Genet. A 133A, 37–43 (2005).
Hung, C.-C. et al. Fragile X syndrome carrier screening in pregnant women in Chinese Han population. Sci. Rep. 9, 15456 (2019).
Kim, M. J. et al. Fragile X carrier screening in Korean women of reproductive age. J. Med. Screen 20, 15–20 (2013).
Jang, J.-H. et al. Frequency of FMR1 premutation carriers and rate of expansion to full mutation in a retrospective diagnostic FMR1 Korean sample. Clin. Genet. 85, 441–445 (2014).
Cheng, Y. K. et al. Identification of fragile X pre-mutation carriers in the Chinese obstetric population using a robust FMR1 polymerase chain reaction assay: Implications for screening and prenatal diagnosis. Hong Kong Med. J. 23, 110–116 (2017).
Huang, W. et al. Distribution of fragile X mental retardation 1 CGG repeat and flanking haplotypes in a large Chinese population. Mol. Genet. Genomic Med. 3, 172–181 (2015).
Ma, Y. et al. The prevalence of CGG repeat expansion mutation in FMR1 gene in the northern Chinese women of reproductive age. BMC Med. Genet. 20, 81 (2019).
Gao, F. et al. Development of Chinese genetic reference panel for Fragile X Syndrome and its application to the screen of 10,000 Chinese pregnant women and women planning pregnancy. Mol. Genet. Genomic Med. 8, e1236 (2020).
Sullivan, A. K. et al. Association of FMR1 repeat size with ovarian dysfunction. Hum. Reprod. 20, 402–412 (2005).
Fernandez-Carvajal, I. et al. Expansion of an FMR1 grey-zone allele to a full mutation in two generations. J. Mol. Diagn. 11, 306–310 (2009).
Hall, D., Tassone, F., Klepitskaya, O. & Leehey, M. Fragile X-associated tremor ataxia syndrome in FMR1 gray zone allele carriers. Mov. Disord. 27, 296–300 (2012).
Liu, Y., Winarni, T. I., Zhang, L., Tassone, F. & Hagerman, R. J. Fragile X-associated tremor/ataxia syndrome (FXTAS) in grey zone carriers. Clin. Genet. 84, 74–77 (2013).
Aydin, G. et al. Frequency of SCA8, SCA10, SCA12, SCA36, FXTAS and C9orf72 repeat expansions in SCA patients negative for the most common SCA subtypes. BMC Neurol. 18, 3 (2018).
Kenneson, A., Zhang, F., Hagedorn, C. H. & Warren, S. T. Reduced FMRP and increased FMR1 transcription is proportionally associated with CGG repeat number in intermediate-length and premutation carriers. Hum. Mol. Genet. 10, 1449–1454 (2001).
Loesch, D. Z. et al. Transcript levels of the intermediate size or grey zone fragile X mental retardation 1 alleles are raised, and correlate with the number of CGG repeats. J. Med. Genet. 44, 200–204 (2007).
Acknowledgements
We would like to thank Ms. Oradawan Plong-On and Ms. Pornsiri Sangmanee from Department of Pathology, Faculty of Medicine, Prince of Songkla University for their technical assistance, and Dr. Theeraphong Pho-iam and Ms. Benjarat Yimming from Siriraj Genomics, Faculty of Medicine Siriraj Hospital, Mahidol University for their help with the sample preparation process. We also extend our gratitude to Ms. Jirawan Jayuphan from the Department of Epidemiology and Mr. Kittisakdi Choomalee from the Department of Family and Preventive Medicine, Faculty of Medicine, Prince of Songkla University, for their assistance with statistical analysis. Additionally, we thank Dr. Chariyawan Charalsawadi for her valuable suggestions regarding this work, and Mr. David Patterson from the International Affairs Office, Faculty of Medicine, Prince of Songkla University, for his English language editing. This study was funded by the Faculty of Medicine, Prince of Songkla University (356/63-00646) and the Education & Public Welfare Foundation, Thailand.
Author information
Authors and Affiliations
Contributions
A.H.: Conceptualization, Data curation, Funding acquisition, Formal analysis, Investigation, Methodology, Validation, Project administration, Writing – original draft, Review & editing. S.K.: Investigation, Methodology, Validation, Data curation. C.L.: Data curation, Investigation. P.L.: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Writing – review & editing. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hnoonual, A., Kaewfai, S., Limwongse, C. et al. Prevalence and implications of fragile X premutation screening in Thailand. Sci Rep 14, 26257 (2024). https://doi.org/10.1038/s41598-024-77762-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-77762-3
