
Abstract
Erectile dysfunction (ED) shares common risk factors with cardiovascular (CV) disease, such as a sedentary lifestyle, obesity, and metabolic syndrome. However, the relationship between ED and CV risk in Vietnam remains unknown. To investigate this, we conducted a multi-center observational study, randomly selecting 2,936 men aged 40 to 69 years in Vietnam, with 385 participants included after exclusions. The study evaluated the 10-year CV risk using the Systematic Coronary Risk Evaluation 2-Diabetes (SCORE2-Diabetes) score and assessed ED using the International Index of Erectile Function (IIEF-5) score. Results showed that men with diabetes mellitus and hypertension had significantly lower IIEF-5 scores compared to healthy individuals (18 [15–22] vs. 23 [20–24], p < 0.001). Additionally, the IIEF-5 score proved effective in identifying patients at very high CV risk, with an area under the curve (AUC) of 0.747, a cutoff point of 18.5, sensitivity of 69.6%, and specificity of 69.9%. Furthermore, we found a significant inverse correlation between SCORE2-Diabetes and IIEF-5 (ρ = -0.45 and p < 0.001). These findings establish a significant connection between ED and CV risk in men with diabetes, underscoring the need for integrated screening and management strategies to address both conditions concurrently.
Similar content being viewed by others


Introduction
Sexuality constitutes an indispensable facet of human existence, encompassing both the physiological processes pertinent to procreation and the experiential dimensions associated with pleasure. The multifaceted nature of human sexual function involves an intricate interplay between physiological and psychological factors, rendering it a subject of considerable complexity1. The significance attributed to sexual health and the attainment of gratification within one’s sexual life underscores its pivotal role in overall quality of life2. In males, sexual activity entails a coordinated interplay between cerebral arousal mechanisms and subsequent physiological responses, culminating in the requisite penile erection for successful copulation3. The extant literature has underscored the salutary effects of regular sexual engagement on psychological well-being and the maintenance of both relational and sexual health4. Moreover, satisfactory sexual intercourse correlates with favorable hormonal profiles, such as increased testosterone production, and leads to improvements in physical health, including enhanced cardiovascular (CV) function and muscle tone. Psychologically, it reduces stress, anxiety, and depression, promoting emotional well-being and mental clarity. These combined effects contribute to better overall health, reinforcing the role of sexual activity in maintaining both physical and psychological resilience5.
Findings derived from the National Social Life, Health, and Aging Project revealed a positive correlation between a heightened frequency of sexual activity and a reduced risk of CV events among males in later life stages6. This relationship is further supported by analyses from the National Health and Nutrition Examination Survey in the United States (2005–2016), where 15,629 American adults were studied, showing that those engaging in sexual activity more than 52 times annually had a 21% lower risk of mortality from heart disease and a 49% reduction in all-cause mortality7. Additionally, one specific study highlights the long-term survival benefits of regular sexual activity following myocardial infarction. Maintaining or increasing sexual activity in the months following myocardial infarction was associated with a marked reduction in all-cause mortality and a substantial decrease in non-CV mortality8. These findings suggest that regular sexual activity may offer protective CV benefits, possibly through enhanced physical fitness, mental health, and improved circulatory function.
However, nearly one-third of men within the sexually active age bracket are unable to derive benefits from sexual activity due to experiencing sexual dysfunctions9,10. Various etiological factors contribute to sexual dysfunction in men, each possessing distinct risk profiles and therapeutic modalities11. The Second International Consultation on Erectile and Sexual Dysfunctions has delineated and cataloged male sexual dysfunction, encompassing erectile dysfunction (ED), ejaculation disorders, orgasmic dysfunctions, and disorders of sexual interest/desire12. Among these, ED has emerged as one of the most prevalent male sexual dysfunctions1,13,14.
Given its deleterious impact on men’s quality of life and its heightened prevalence with advancing age (affecting 40% of men aged between 40 and 70 years), ED has garnered considerable attention across diverse disciplinary domains, ranging from urology, andrology, and neuropharmacology to regenerative medicine, vascular surgery, and prosthesis implantation15. However, recent studies have highlighted an increasing interest among internal medicine practitioners regarding ED concerns. Notably, the risk factors associated with ED, such as a sedentary lifestyle, obesity, smoking, hypercholesterolemia, and metabolic syndrome, closely mirror those implicated in cardiovascular disease (CVD)16. Mounting evidence underscores the robust predictive value of ED for CV events, with numerous studies demonstrating that ED can precede major adverse CV events by several years. This early manifestation provides a valuable window for intervention. A meta-analysis has shown that ED is independently associated with an increased risk of all-cause mortality and CV mortality, regardless of traditional risk factors. Early detection of ED could thus facilitate timely management and risk mitigation strategies, potentially reducing the likelihood of subsequent CV events17,18,19.
However, compelling evidence linking ED to CV risk, particularly within the Vietnamese population, remains limited, primarily due to the cultural nuances surrounding sexual intercourse and ED, which often shroud these topics in secrecy. Therefore, we conducted a study to assess the relationship between 10-year CV risk and ED among men with diabetes mellitus (DM) and hypertension (HP) in Vietnam.
Methods
Study population
In this study, given the large and difficult-to-define target population, Cochran’s formula (1977) was applied to estimate the sample size. The formula used was n = (Za)2 × (p × q)/d2, where p represents the prevalence of diabetes (approximately 6% in Vietnam20), q is the complement of the prevalence (1 - p), d is the margin of error, and Za corresponds to a 95% confidence level (1.96). Based on this, n = 1.96 × 1.96 × (0.06 × 0.94)/0.05 × 0.05 = 87, indicating that the minimum sample size required per sampling site was 87 participants.
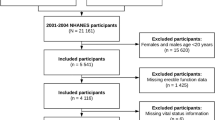
This cross-sectional study was conducted from April 2022 to August 2023, involving 2,936 aged 40 to 69 years who were randomly selected for the study from two healthcare centers: Kien Giang General Hospital in Southern Vietnam and Da Nang General Hospital in Central Vietnam. Following exclusion criteria, the study included 385 participants, comprising 235 male type 2 DM patients and 150 healthy males without a history of disease who attended regular health checkups, serving as the control group. The flowchart illustrating the study’s sample collection and subgroup allocation is shown in Supplementary Fig. S1. Diagnosis of DM was based on the guidelines of the American Diabetes Association and the European Association for the Study of Diabetes or by receiving treatment with glucose-lowering pharmacotherapy21.
The exclusion criteria for this study were as follows: (1) patients in the acute phase of disease, including acute heart failure, acute liver failure, infection, increased intracranial pressure, hypertensive crisis, diabetic ketoacidosis, or the acute phase of chronic obstructive pulmonary disease; (2) patients with chronic diseases such as cirrhosis, hepatitis, stage IV or higher chronic kidney disease, nephrotic syndrome, thyroid disorders, adrenal disorders, cancer, or chronic lung disease were also excluded; (3) patients with any CV conditions that could prevent the accurate assessment of the 10-year CV risk, including coronary artery disease, cerebrovascular disease, aortic aneurysm, peripheral artery disease, or those receiving antithrombotic treatment, were not included; (4) patients with a history of penile trauma, pelvic fracture, urological surgery, or pelvic or sacral trauma; and (5) individuals using medications affecting ED, such as antidepressants (selective serotonin reuptake inhibitors, tricyclic antidepressants), antipsychotics (neuroleptics), androgen suppression agents (GnRH agonists and antagonists, 5-ARIs), antihypertensive medications (beta blockers, thiazide diuretics), or stimulants (heroin, cocaine, marijuana, methadone, synthetic steroids), were excluded. Subsequently, 235 consecutive patients diagnosed with type 2 DM were recruited and categorized into two cohorts—DM without HP (DM-HP) (n = 96) and DM with HP (DM + HP) (n = 139)—based on the presence or absence of concurrent HP. HP was diagnosed through either the use of antihypertensive medication or clinical assessment, with blood pressure measurements meeting the criteria of systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg on at least two separate occasions.
Clinical data
We collected clinical variables, family history, medication use, and other risk factors directly from medical records, while standardized questionnaires were administered to participants through face-to-face interviews. The following data were collected: (1) Age: Calculated by subtracting the participant’s birth year from the survey year. (2) Personal medical history: inquiry regarding any history of internal diseases such as DM, HP, hyperlipidemia, or obesity. (3) Smoking history was recorded as a yes or no regarding their smoking status. Male participants who had abstained from smoking for more than ten years were categorized as nonsmokers22. (4) Alcohol consumption history: patients who responded with either yes or no alcohol consumption. (5) Age at diabetes diagnosis. Other clinical data, such as body mass index (BMI), hip circumference, heart rate, SBP, and DBP, were collected.
Laboratory measurements
Fasting venous blood specimens were analyzed using the Cobas E601 automated biochemical analyzer to measure testosterone, glucose, hemoglobin A1C, total cholesterol (TC), triglycerides, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), non-HDL cholesterol, creatinine, and estimated glomerular filtration rate (eGFR) using CKD-EPI 2021 (eGFR, mL/min per 1.73 m2)23. The albumin and urinary creatinine levels in morning urine samples were quantified to calculate the albumin/creatinine ratio (ACR). Non-HDL-C was derived from total cholesterol and HDL-C values using the equation: non-HDL-C = TC – HDL-C (mmol/L)24.
10-year cardiovascular risk calculator
CV risk was assessed using the SCORE2-Diabetes scale25. The SCORE2-Diabetes tool for individuals aged 40 to 69 years was employed, considering variables such as sex, age, age at diabetes diagnosis, SBP, smoking status, TC, HDL-C, HbA1C, and eGFR, and adjusted for the CV risk region in the population. The surveyed population was classified into four CV risk groups based on the statistical rate of CV mortality per 100,000 people, aligned with ESC 2021 recommendations: low risk (< 100 CV deaths per 100,000 people), moderate risk (100 to < 150 CV deaths per 100,000 people), high risk (150 to < 300 CV deaths per 100,000 people), and very high risk (≥ 300 CV deaths per 100,000 people)26. When selecting the model to assess CV risk using SCORE2-Diabetes, we followed the Vietnam Society of Cardiology recommendations and opted for regions with high CV risk in clinical practice in Vietnam27.
The estimated CV risk (fatal and non-fatal) within ten years was calculated using the SCORE2-Diabetes system, which was used to categorize the risk of CV events into low-moderate, high, and very high risk groups. The interpretation of the results depends on the following cutoff risk levels: low-moderate CVD risk < 10%, high CVD risk 10% to < 20%, and very high CVD risk ≥ 20% 25.
Evaluation and classification of erectile dysfunction
In our study, we utilized a Vietnamese-translated version of the abridged five-item version of the International Index of Erectile Function (IIEF-5) (Supplementary Table S2) to assess ED, intending to enhance objectivity in its evaluation and classification. Patients were provided detailed guidance on utilizing the IIEF-5 scale by an independent urologist, after which they self-evaluated their scores. Subsequently, the severity of ED was determined based on self-assessed IIEF-5 scores, which were categorized into five levels: severe (5–7 points), moderate (8–11 points), mild to moderate (12–16 points), mild (17–21 points), and no (22–25 points)28. In this study, individuals were considered to have ED if their IIEF-5 score ranged from 5 to 21 points.
Statistical analysis
Statistical analyses were conducted using SPSS Version 26 (IBM, New York, United States), MedCalc Software Version 22.019 (MedCalc Software, Ostend, Belgium), and GraphPad Prism Version 10 (GraphPad Software, Boston, United States). Data normality was assessed using the Kolmogorov‒Smirnov tests. Normally distributed continuous variables are presented as the mean ± standard deviation, while nonnormally distributed variables are presented as median values with interquartile ranges. Categorical variables are reported as frequencies and percentages. Fisher’s exact test was utilized to evaluate intergroup differences in categorical variables. In contrast, differences in continuous variables were assessed using either the unpaired T test or the Mann‒Whitney U test, as appropriate. One-way ANOVA with multiple comparisons was used for normally distributed data. The Kruskal‒Wallis test is a nonparametric test that compares three or more unmatched groups. Missing data were excluded from the analyses. Differences in the IIEF5 scores between the DM + HP, DM-HP, and control groups were compared by analysis of covariance after adjusting for age and BMI. Spearman’s correlation coefficient (ρ) and its corresponding p value were calculated to explore correlations between continuous variables. This study employed receiver operating characteristic (ROC) analysis to determine the optimal cutoff value of the IIEF-5 score for detecting ED utilizing the Wilson/Brown method. The determination of the optimal cutoff point was facilitated through Youden’s index. Furthermore, a ROC curve analysis was conducted, adjusting for age and BMI. The areas under the curves (AUCs) were compared using the Hanley and McNeil methods29. Multivariate linear regression was utilized to explore the associations between clinical factors, SCORE2-Diabetes, and IIEF-5. Before conducting the linear regression analysis, Box-Cox transformation transformed non-normally distributed variables into normally distributed ones. Clinical confounders and variables exhibiting significance (p < 0.1) in the univariate analysis were incorporated into the multivariable model. A variance inflation factor of five was applied to address multicollinearity among the univariate variables. All the statistical tests were two-sided, with a significance level of < 0.05.
Ethical approval
The study protocol garnered approval from the Ethics Committee of the Da Nang City Department of Health (Approval number: 869/BVĐN-HĐYĐ) and the Hue University of Medicine and Pharmacy Ethics Council (Approval number: H2022/869). Written consent was obtained from all patients or their legally authorized representatives. The selection of participating centers adhered strictly to our protocol and conformed rigorously to the principles delineated in the Declaration of Helsinki 2013.
Results
Baseline characteristics
Our study included 385 participants divided into three groups: a DM with HP group (DM + HP, N = 139), a DM without HP group (DM-HP, N = 96), and a control group (N = 150). The results showed that the median testosterone (nmol/L) values of the DM + HP, DM-HP, and control groups were 13.2 [10.6–17.1], 14.9 [11.2–19.9], and 17.5 [13.1–22.2], respectively, with p < 0.001. Additionally, the DM + HP group had a lower median IIEF-5 than the DM-HP and control groups, which were 18 [15–22], 22 [17–23], and 23 [20–24], respectively, with p < 0.001. The DM + HP group had a SCORE2-Diabetes of 17.6 [12.5–24.2], which was greater than that of the DM-HP group (13.6 [9.3–20.0]). Further details are presented in Table 1; Fig. 1.

Comparison of IIEF-5, SCORE2-Diabetes, and testosterone values among the three study groups. DM diabetes mellitus, HP hypertension, IIEF-5 International Index of Erectile Function-5, SCORE2-Diabetes systematic coronary risk estimation for type 2 diabetes.

Comparison of the SCORE2-Diabetes and testosterone values among the erectile dysfunction groups. SCORE2-Diabetes systematic coronary risk estimation for type 2 diabetes.

Comparing the values of IIEF-5 and testosterone among the cardiovascular risk groups. IIEF-5 International Index of Erectile Function-5.

Correlation between erectile dysfunction and cardiovascular risk. Panel A: Correlation between SCORE2-Diabetes and IIEF-5. Panel B: Correlation between testosterone and IIEF-5 score. Panel C: Correlation between SCORE2-Diabetes and testosterone. IIEF-5 International Index of Erectile Function-5, SCORE2-Diabetes systematic coronary risk estimation for type 2 diabetes.

ROC curve illustrating the value of the IIEF-5 and testosterone in predicting 10-year cardiovascular risk. IIEF-5 International Index of Erectile Function-5, AUC area under the curve.
The association between erectile dysfunction and cardiovascular risk
The SCORE2-Diabetes values in the groups of patients without ED, with mild ED, with mild-moderate ED, with moderate ED, and with severe ED were 12.3, 17.1, 20.8, 21.5, and 23.8, respectively, with statistically significant differences (p < 0.05). Conversely, testosterone showed a decreasing trend from participants without ED to those with severe ED (see Fig. 2). The IIEF-5 score demonstrated a decreasing trend in patients with low-moderate, high, and very high CV risk (22, 20, and 16, respectively) (Fig. 3a). There was an inverse correlation between SCORE2-Diabetes and IIEF-5, with ρ = -0.45 and p < 0.001 (Fig. 4a). In contrast, a positive correlation was observed between testosterone and IIEF-5 (ρ = 0.43, p < 0.001) (Fig. 4b). Additionally, an inverse relationship was found between SCORE2-Diabetes and testosterone (ρ = -0.21, p = 0.001) (Fig. 4c). Further details are illustrated in Figs. 2, 3 and 4.
The value of the IIEF-5 and testosterone in predicting 10-year cardiovascular risk
The AUC values for the IIEF-5 score and testosterone concentration for predicting very high CV risk were 0.747 and 0.598, respectively. A statistically significant difference was found between their AUCs (p < 0.05) using the Hanley and McNeil methods. More details are provided in Fig. 5.
Univariate and multivariate regression analyses of the IIEF-5 score and SCORE2-Diabetes in men with diabetes
Table 2 summarizes univariate and multivariate analyses of IIEF-5 scores among DM patients. The analysis of factors associated with erectile function, measured by the IIEF-5 score, reveals that age, insulin use, obesity, HP, and high CV risk are significantly linked to reduced erectile function in men with diabetes (p < 0.05). In particular, insulin use and high CV risk remained significant independent predictors of lower IIEF-5 scores even after adjusting for other factors, with p values of < 0.001 and 0.006, respectively.
Additionally, Table 2 also summarizes the results of both univariate and multivariable analyses conducted on SCORE2-Diabetes among individuals with DM. Univariate regression revealed correlations between SCORE2-Diabetes and insulin usage (β = 0.376, p = 0.001) and between SCORE2-Diabetes and ED (β = 0.367, p < 0.001) in DM patients. Furthermore, multivariate analysis revealed that ED was an independent variable significantly associated with SCORE2-Diabetes (β = 0.452, p < 0.001) in individuals with DM. Further details are available in Table 2.
Discussion
Erectile dysfunction and diabetes
Our study found that men with DM had significantly lower IIEF-5 score compared to the control group (Fig. 1a). This finding aligns with the study by Corona et al., which reported that 1 in 5 men with DM experienced severe ED30. Similarly, a recent meta-analysis indicated that more than half of the patients with DM experienced ED31. Another report highlighted that individuals with DM had an approximately 3.5-fold greater incidence of ED than those without DM32.
Additionally, our study demonstrated that testosterone concentrations in the DM group were significantly lower than those in the control group (Fig. 1b), aligning with findings from a comprehensive meta-analysis. A meta-analysis incorporating all prospective and cross-sectional studies comparing testosterone levels in participants with or without DM also indicated that individuals with DM were at greater risk of having low testosterone33. Such findings are particularly important given the well-established role of testosterone in erectile function. Reduced testosterone levels, as seen in many men with DM, contribute significantly to the development of ED. Testosterone plays a crucial role in maintaining the normal physiology of the erectile process34..
Men with DM face a significantly greater risk of ED than those without DM. The etiology of ED in these patients is multifactorial, involving both vascular and neural complications. Chronic hyperglycemia leads to the accumulation of advanced glycation end products (AGEs) and the overproduction of reactive oxygen species (ROS)35, which in turn cause endothelial dysfunction and damage to the vascular system35,36. This vascular impairment reduces nitric oxide (NO) availability, a crucial molecule for smooth muscle relaxation and vasodilation during penile erection37. Additionally, diabetic conditions upregulate the RhoA/Rho-kinase pathway, which promotes smooth muscle contraction and further inhibits the relaxation required for proper erectile function. Furthermore, increased endothelin-1 (ET-1) levels contribute to vasoconstriction, exacerbating the already compromised penile blood flow37. Neuropathy, another complication of diabetes, disrupts the normal neural signaling required for erection by impairing both the autonomic and somatic innervation of penile tissue, reducing the body’s ability to induce and sustain an erection37,38. In addition to these vascular and neurological factors, hypogonadism is prevalent in men with diabetes, further exacerbating ED34. Decreased serum testosterone exacerbates endothelial function by reducing NO synthase activity and increasing the expression of asymmetric dimethylarginine (ADMA), which inhibits NO synthesis. Hypotestosteronemia also impacts insulin sensitivity in skeletal muscle through androgen receptor-mediated mechanisms, resulting in reduced peroxisome proliferator-activated receptor γ activity and impaired glucose metabolism39. Since proper glucose metabolism is essential for cellular energy production and overall vascular health, its impairment leads to further vascular damage and reduced erectile function in men with diabetes.
Erectile dysfunction and hypertension
The diagnosis of HP increases the likelihood of experiencing ED, and conversely, ED can serve as an early indicator of HP40. The prevalence of ED is approximately twice as high in hypertensive patients as in those with normal blood pressure41.
In our study, men with diabetes with HP had a significantly lower IIEF-5 score than those without HP (Fig. 1a). After adjusting for other risk factors, HP was identified as an independent factor affecting the IIEF-5 score in men with diabetes (Table 2). A recent study by Zheng Wang and colleagues indicated a positive causal relationship between HP and the risk of ED. Therefore, greater attention should be given to managing HP to prevent or improve erectile function42.
HP and ED share a significant pathophysiological link primarily rooted in vascular dysfunction. In individuals with HP, there is a heightened release of vasoconstrictive agents such as angiotensin II (AngII), endothelin 1 (ET-1), and aldosterone43. These agents lead to impaired function of the endothelial cells lining the blood vessels, including those responsible for blood flow to the corpus cavernosum, a critical structure for penile erection. This endothelial dysfunction not only limits the ability of blood vessels to relax but also induces a continuous contractile state in vascular and penile smooth muscle tissues. Such an imbalance in vasodilation and vasoconstriction underlies both HP and ED. Elevated AngII levels activate ROS, reducing NO availability, which is essential for vasodilation and smooth muscle relaxation. This cascade promotes a procontractile state in the vascular tissues, further exacerbating the difficulties in achieving an erection. Furthermore, aldosterone and ET-1 contribute to this imbalance by promoting oxidative stress and inflammation, further damaging endothelial cells and hindering NO production. Aldosterone, in particular, increases ROS production, while ET-1 enhances smooth muscle contraction via calcium influx, creating a vicious cycle that worsens both hypertension and ED. In hypertensive conditions, NO deficiency becomes a central issue, as NO is a crucial mediator of erectile function. Reduced NO bioavailability impairs the relaxation of the smooth muscle in the corpus cavernosum, leading to ED40. Recent evidence indicates that the innate immune system, mainly through Toll-like receptor 4 (TLR4), plays a significant role in the pathophysiology of HP and ED by promoting oxidative stress and maintaining a low-grade inflammatory state. Activation of TLR4 by AngII leads to an increase in pro-inflammatory cytokines, contributing to endothelial dysfunction and vascular remodeling, which are critical in both HP and ED. This process is further exacerbated by the upregulation of the RhoA/Rho-kinase pathway and reduced NO availability, impairing vasodilation and smooth muscle relaxation, critical factors in the development of ED44,45.
Furthermore, certain antihypertensive medications can exacerbate ED, complicating treatment adherence for patients with HP. Medications such as beta-blockers and diuretics, commonly prescribed for HP, have been linked to ED due to their negative effects on the vasculature and hormonal balance46,47,48. For instance, beta-blockers may inhibit beta-2 receptors, reducing vasodilation, while diuretics can diminish blood flow to the penile tissues. These medication-induced effects, combined with the already compromised endothelial function in HP, further perpetuate the vascular challenges related to ED. Such a situation creates a challenge where treating HP may worsen ED, reducing medication adherence. Therefore, managing both conditions concurrently is crucial. Tailored therapeutic approaches that preserve erectile function while effectively controlling blood pressure are key to achieving long-term success40.
Erectile dysfunction and cardiovascular risk
Our research indicated that patients with ED have a significantly greater risk of CV than those without ED. The CV risk in the ED group was nearly double that in the non-ED group from moderate levels onward (see Fig. 2a). Additionally, individuals with high and very high CV risk had significantly lower IIEF-5 scores than those with low to moderate CV risk (Fig. 3a). In our study, SCORE2-Diabetes had an inverse correlation with the IIEF-5 score, with ρ = -0.45 and p < 0.001 (Fig. 4a). An analysis of the Olmsted County Study data, a population-based survey involving over 1,400 men aged 40 to 79 years, clearly documented the association between ED and CV risk. Among men aged 40–49 years, those with ED had an almost 50-fold higher incidence of ischemic heart disease compared to their counterparts without ED49. There is widespread consensus that men with ED should be regarded as being at high risk for CVD50,51. Consequently, utilizing available risk assessment tools to stratify coronary risk scores for each patient is recommended50.
In our study, the IIEF-5 demonstrated predictive value for identifying patients at very high CV risk, with an AUC of 0.747. The corresponding cutoff point, sensitivity, and specificity were 18.5, 69.6%, and 69.9%, respectively (Fig. 5). Research on CV risk factors and IIEF-5 score has concluded that patients with ED should be classified as having an extremely high risk for CV events52. Findings from the Multi-Ethnic Study of Atherosclerosis have also highlighted ED as an independent predictor of future CV events53. Additionally, a systematic review and meta-analysis of cohort studies indicated that the presence of ED increases the risk for future CV events, myocardial infarction, cerebrovascular events, and all-cause mortality while also showing a tendency to increase the risk of CV mortality54. Furthermore, meta-analyses have shown that ED is an independent predictor of CV disease and its outcomes. ED and CV disease are two manifestations of the same physiological phenomenon, with ED typically preceding symptomatic CV disease. Such a connection presents an opportunity for healthcare practitioners to screen and identify high risk patients early to prevent avoidable morbidity and mortality55. Recognizing ED as an early harbinger of future CV events is crucial for initiating preventive measures. Screening and diagnosing ED are essential for primary and secondary prevention of CV disease, as ED assessment offers a simple and cost-effective prognostic tool alternative to other investigational CV biomarkers. Moreover, ED significantly contributes to poor adherence to CV therapy or its discontinuation56. Hence, it is imperative to consider ED as an early manifestation of CV disease, warranting careful assessment of CV risk factors in men with ED to prevent future major adverse CV events. Identifying these risk factors can assist in identifying patients with ED who require stricter lifestyle modifications or pharmacological interventions to minimize CV risk. Managing patients with ED provides an opportunity to address modifiable risk factors strictly, potentially reducing CV risk and improving sexual complaints57. Therefore, ED should be recognized as a warning sign of silent or impending CV disease, and CV risk stratification should be integrated into the clinical management of all men with vasculogenic ED.
ED and CVD share common risk factors such as obesity, HP, metabolic syndrome, DM, and smoking. Moreover, they both involve underlying pathological mechanisms, including endothelial dysfunction, inflammation, and atherosclerosis58. The association between ED and CVD may be attributed to the interplay among androgen levels, chronic inflammation, and CV risk factors, which contribute to endothelial dysfunction and atherosclerosis in both the penis and coronary circulation. Due to the smaller size of penile arteries than coronary arteries, the same degree of endothelial dysfunction and atherosclerotic burden can lead to a greater reduction in blood flow in erectile tissues than in coronary circulation. Both ED and endothelial dysfunction are linked to a loss of NO, with the molecular basis of this loss being virtually identical for both conditions. Phosphodiesterase-5 inhibitors, which act by restoring the levels of cyclic guanosine monophosphate downstream, have been shown to effectively improve erectile function in patients with coronary artery disease when taken on demand and are now considered first-line pharmacotherapy for ED treatment59,60.
Our study found that using an ED assessment scale like the IIEF-5 is a simple and practical tool for assessing CV risk in clinical practice. Urologists should refer patients with ED to cardiologists for CV screening, while cardiologists should evaluate the impact of CVD on ED by referring patients to urologists. This integrated approach enhances patient outcomes by enabling early intervention, improving quality of life, and reducing CV risk in men with diabetes. It promotes a collaborative care model that supports holistic management of both ED and CV health through lifestyle modifications, medications, and therapies targeting endothelial function and atherosclerosis.
Strengths
This study has several significant strengths. We utilized well-established and widely available scoring systems, including the IIEF-5 and SCORE2-Diabetes, making it easier for future research to replicate similar studies. Additionally, this is the first study to evaluate the relationship between cardiovascular risk and erectile dysfunction in a Vietnamese population - a country where sexual education has not been strongly emphasized, and sexual health is often overlooked. The study was conducted across two different centers and included a relatively large sample size, further enhancing the reliability of the findings.
Limitations
This study has several limitations. First, this was a cross-sectional study, meaning future CV events could not be tracked. Implementing a prospective longitudinal study design would be essential to evaluate CV events accurately and ED if feasible. Second, due to healthcare conditions in Vietnam, patients with DM and/or HP undergo monthly re-examinations and receive medication from healthcare facilities. However, depending on availability, patients may receive different medications during each visit. Therefore, our study could not evaluate the specific impact of antihypertensive and antidiabetic medications on ED. Third, we have yet to address potential psychological barriers that could affect questionnaire responses related to ED assessment. Fourth, our study was conducted exclusively on a Vietnamese population, which may limit the generalizability of the findings to other populations. Fifth, we did not assess physical activity or diet, both of which are crucial factors that could influence both CVD and ED outcomes. Lastly, as an observational study, the results do not provide conclusive evidence at a high level. Nevertheless, our findings can serve as a valuable foundation for future research exploring the relationship between CVD and ED.
Conclusion
In conclusion, our study shows that men with DM and HP are at significantly higher risk of ED. We found a strong association between ED and CV risk, particularly in these patients. These findings highlight the need for dual screening of ED and CV risk, which can lead to early detection and timely intervention, improving both quality of life and long-term CV outcomes, especially in men with diabetes.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author or first author (Hai Nguyen Ngoc Dang) upon reasonable request. Email: dangnngochai@dtu.edu.vn or ngochai123dc@gmail.com.
References
Anderson, D. et al. Male sexual dysfunction. Health Psychol. Res. 10 https://doi.org/10.52965/001c.37533 (2022).
Flynn, K. E. et al. Sexual satisfaction and the importance of sexual health to quality of life throughout the life course of U.S. adults. J. Sex. Med. 13, 1642–1650. https://doi.org/10.1016/j.jsxm.2016.08.011 (2016).
Vignozzi, L. et al. Testosterone and sexual activity. J. Endocrinol. Invest. 28, 39–44 (2005).
Mollaioli, D. et al. Benefits of sexual activity on psychological, relational, and sexual Health during the COVID-19 breakout. J. Sex. Med. 18, 35–49. https://doi.org/10.1016/j.jsxm.2020.10.008 (2021).
Jannini, E. A., Fisher, W. A., Bitzer, J. & McMahon, C. G. Controversies in sexual medicine: Is sex just Fun? How sexual activity improves Health. J. Sex. Med. 6, 2640–2648. https://doi.org/10.1111/j.1743-6109.2009.01477.x (2009).
Liu, H., Waite, L. J., Shen, S. & Wang, D. H. Is sex good for your health? A national study on partnered sexuality and cardiovascular risk among older men and women. J. Health Soc. Behav. 57, 276–296. https://doi.org/10.1177/0022146516661597 (2016).
Cao, C. et al. Trends in sexual Activity and associations with all-cause and cause-specific mortality among US adults. J. Sex. Med. 17, 1903–1913. https://doi.org/10.1016/j.jsxm.2020.05.028 (2020).
Cohen, G. et al. Resumption of sexual activity after acute myocardial infarction and long-term survival. Eur. J. Prev. Cardiol. 29, 304–311. https://doi.org/10.1093/eurjpc/zwaa011 (2022).
Rosen, R. C. Prevalence and risk factors of sexual dysfunction in men and women. Curr. Psychiatry Rep. 2, 189–195. https://doi.org/10.1007/s11920-996-0006-2 (2000).
Mialon, A., Berchtold, A., Michaud, P. A., Gmel, G. & Suris, J. C. Sexual dysfunctions among Young men: Prevalence and associated factors. J. Adolesc. Health. 51, 25–31. https://doi.org/10.1016/j.jadohealth.2012.01.008 (2012).
Rew, K. T. Men’s health: Male sexual dysfunction. FP Essent. 503, 28–33 (2021).
Lue, T. F. & Khoury, S. Comments on the second international consultation on erectile and sexual dysfunctions. J. Sex. Med. 1, 4–5. https://doi.org/10.1111/j.1743-6109.2004.10103.x (2004).
Lowy, M. & Ramanathan, V. Erectile dysfunction: Causes, assessment and management options. Aust Prescr. 45, 159–161. https://doi.org/10.18773/austprescr.2022.051 (2022).
McMahon, C. G. Current diagnosis and management of erectile dysfunction. Med. J. Aust. 210, 469–476. https://doi.org/10.5694/mja2.50167 (2019).
Argiolas, A., Argiolas, F. M., Argiolas, G. & Melis, M. R. Erectile Dysfunction: treatments, advances and new therapeutic strategies. Brain Sci. 13, 802. https://doi.org/10.3390/brainsci13050802 (2023).
Grant, P., Jackson, G., Baig, I. & Quin, J. Erectile dysfunction in general medicine. Clin. Med. 13, 136–140. https://doi.org/10.7861/clinmedicine.13-2-136 (2013).
Diaconu, C. C. et al. The erectile dysfunction as a marker of cardiovascular disease: A review. Acta Cardiol. 75, 286–292. https://doi.org/10.1080/00015385.2019.1590498 (2020).
Imprialos, K., Koutsampasopoulos, K., Manolis, A. & Doumas, M. Erectile dysfunction as a cardiovascular risk factor: Time to step up? CVP. 19, 301–312. https://doi.org/10.2174/1570161118666200414102556 (2020).
Zhao, B. et al. Erectile dysfunction predicts cardiovascular events as an independent risk factor: A systematic review and meta-analysis. J. Sex. Med. 16, 1005–1017. https://doi.org/10.1016/j.jsxm.2019.04.004 (2019).
Dang, H. N. N., Luong, T. V. & Tran, T. T. Evaluating left atrial function changes by speckle tracking echocardiography in type 2 diabetes patients in Central Vietnam: A cross-sectional comparative study. Egypt. Heart J. 76, 38. https://doi.org/10.1186/s43044-024-00470-w (2024).
Davies, M. J. et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 65, 1925–; (1966). https://doi.org/10.1007/s00125-022-05787-2 (2022).
Centers for Disease Control and Prevention (US), National Center for Chronic Disease Prevention and Health Promotion (US), Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. (2010).
Maynard, R. D., Korpi-Steiner, N. & Cotten, S. W. Concordance of chronic kidney disease stage and metformin management using CKD-EPI 2021 race-free equation vs CKD-EPI 2009 equation to Estimate glomerular filtration rate. Clin. Chem. 69, 202–204. https://doi.org/10.1093/clinchem/hvac195 (2023).
Romaszko, J., Gromadziński, L. & Buciński, A. Friedewald formula may be used to calculate non-HDL-C from LDL-C and TG. Front. Med. 10, 1247126. https://doi.org/10.3389/fmed.2023.1247126 (2023).
SCORE2-Diabetes Working Group and the ESC Cardiovascular Risk Collaboration. SCORE2-Diabetes: 10-year cardiovascular risk estimation in type 2 diabetes in Europe. Eur. Heart J. 44, 2544–2556. https://doi.org/10.1093/eurheartj/ehad260 (2023).
Visseren, F. L. J. et al. ESC Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal 42, 3227–3337; (2021). https://doi.org/10.1093/eurheartj/ehab484 (2021).
Van Minh, H., Van Huy, T., Long, D. P. P. & Tien, H. A. Highlights of the 2022 Vietnamese Society of Hypertension guidelines for the diagnosis and treatment of arterial hypertension: The collaboration of the Vietnamese Society of Hypertension (VSH) task force with the contribution of the Vietnam National Heart Association (VNHA). J. Clin. Hypertens. 24, 1121–1138. https://doi.org/10.1111/jch.14580 (2022).
Rhoden, E. L., Telöken, C., Sogari, P. R. & Souto, V. The use of the simplified International Index of Erectile function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. Int. J. Impot. Res. 14, 245–250. https://doi.org/10.1038/sj.ijir.3900859 (2002).
Hanley, J. A. & McNeil, B. J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 148, 839–843. https://doi.org/10.1148/radiology.148.3.6878708 (1983).
Corona, G., Giorda, C. B., Cucinotta, D., Guida, P. & Nada, E. Sexual dysfunction at the onset of type 2 diabetes: The interplay of Depression, Hormonal and Cardiovascular factors. J. Sex. Med. 11, 2065–2073. https://doi.org/10.1111/jsm.12601 (2014).
Kouidrat, Y. et al. High prevalence of erectile dysfunction in diabetes: A systematic review and meta-analysis of 145 studies. Diabet. Med. 34, 1185–1192. https://doi.org/10.1111/dme.13403 (2017).
Defeudis, G. et al. Erectile dysfunction and diabetes: A melting pot of circumstances and treatments. Diabetes Metabolism Res. 38, e3494. https://doi.org/10.1002/dmrr.3494 (2022).
Corona, G. et al. Type 2 diabetes mellitus and testosterone: A meta-analysis study: type 2 diabetes and testosterone. Int. J. Androl. 34, 528–540. https://doi.org/10.1111/j.1365-2605.2010.01117.x (2011).
Mikhail, N. Does Testosterone have a role in erectile function? Am. J. Med. 119, 373–382. https://doi.org/10.1016/j.amjmed.2005.07.042 (2006).
An, Y. et al. The role of oxidative stress in diabetes mellitus-induced vascular endothelial dysfunction. Cardiovasc. Diabetol. 22, 237. https://doi.org/10.1186/s12933-023-01965-7 (2023).
Yang, D. R., Wang, M. Y., Zhang, C. L. & Wang, Y. Endothelial dysfunction in vascular complications of diabetes: A comprehensive review of mechanisms and implications. Front. Endocrinol. 15, 1359255. https://doi.org/10.3389/fendo.2024.1359255 (2024).
Defeudis, G. et al. Erectile dysfunction and its management in patients with diabetes mellitus. Rev. Endocr. Metab. Disord. 16, 213–231. https://doi.org/10.1007/s11154-015-9321-4 (2015).
Moore, C. R. & Wang, R. Pathophysiology and treatment of diabetic erectile dysfunction. Asian J. Androl. 8, 675–684. https://doi.org/10.1111/j.1745-7262.2006.00223.x (2006).
Cannarella, R. et al. Erectile Dysfunction in Diabetic patients: From etiology to management. Diabetology. 2, 157–164. https://doi.org/10.3390/diabetology2030014 (2021).
De Oliveira, A. A. & Nunes, K. P. Hypertension and Erectile Dysfunction: Breaking down the challenges. Am. J. Hypertens. 34, 134–142. https://doi.org/10.1093/ajh/hpaa143 (2021).
Viigimaa, M. Management of erectile dysfunction in hypertension: Tips and tricks. WJC. 6 (908). https://doi.org/10.4330/wjc.v6.i9.908 (2014).
Wang, Z. et al. Causal effects of hypertension on risk of erectile dysfunction: A two-sample mendelian randomization study. Front. Cardiovasc. Med. 10, 1121340. https://doi.org/10.3389/fcvm.2023.1121340 (2023).
Ma, J. et al. Signaling pathways in vascular function and hypertension: Molecular mechanisms and therapeutic interventions. Sig Transduct. Target. Ther. 8 https://doi.org/10.1038/s41392-023-01430-7 (2023).
Caillon, A., Paradis, P. & Schiffrin, E. L. Role of immune cells in hypertension. Br. J. Pharmacol. 176, 1818–1828. https://doi.org/10.1111/bph.14427 (2019).
Han, J. et al. MD2 mediates angiotensin II-induced cardiac inflammation and remodeling via directly binding to Ang II and activating TLR4/NF-κB signaling pathway. Basic. Res. Cardiol. 112 https://doi.org/10.1007/s00395-016-0599-5 (2017).
Silvestri A. Report of erectile dysfunction after therapy with beta-blockers is related to patient knowledge of side effects and is reversed by placebo. Eur. Heart J. 24, 1928–1932. https://doi.org/10.1016/j.ehj.2003.08.016 (2003).
Botros, S. M., Hussein, M. & Elserafy, A. Effect of different beta blockers on penile vascular velocities in hypertensive males. Egypt. J. Radiol. Nuclear Med. 46, 749–754. https://doi.org/10.1016/j.ejrnm.2015.04.004 (2015).
Handler, J. Managing Erectile Dysfunction in Hypertensive patients: Managing ED in hypertensive patients. J. Clin. Hypertens. 13, 450–454. https://doi.org/10.1111/j.1751-7176.2011.00465.x (2011).
Inman, B. A. et al. A Population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clinic Proceedings 84, 108–113; (2009). https://doi.org/10.4065/84.2.108
Raheem, O. A., Su, J. J., Wilson, J. R. & Hsieh, T. C. The association of erectile dysfunction and cardiovascular disease: A systematic critical review. Am. J. Mens Health. 11, 552–563. https://doi.org/10.1177/1557988316630305 (2017).
Thompson, I. M. Erectile dysfunction and subsequent cardiovascular disease. JAMA 294, ; (2996). https://doi.org/10.1001/jama.294.23.2996 (2005).
Ahmed Memon, S. et al. Association between erectile dysfunction, cardiovascular risk factors, and coronary artery disease: Role of exercise stress testing and International Index of Erectile function (IIEF-5) questionnaire. IJC Heart Vasculature. 40, 101033. https://doi.org/10.1016/j.ijcha.2022.101033 (2022).
Uddin, S. M. I. et al. Erectile dysfunction as an independent predictor of future cardiovascular events: The multi-ethnic study of atherosclerosis. Circulation. 138, 540–542. https://doi.org/10.1161/CIRCULATIONAHA.118.033990 (2018).
Vlachopoulos, C. V., Terentes-Printzios, D. G., Ioakeimidis, N. K., Aznaouridis, K. A. & Stefanadis, C. I. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: A systematic review and Meta-analysis of Cohort studies. Circ: Cardiovasc. Qual. Outcomes. 6, 99–109. https://doi.org/10.1161/CIRCOUTCOMES.112.966903 (2013).
Mostafaei, H. et al. Association of erectile dysfunction and cardiovascular disease: An umbrella review of systematic reviews and meta-analyses. BJU Int. 128, 3–11. https://doi.org/10.1111/bju.15313 (2021).
Terentes-Printzios, D., Ioakeimidis, N., Rokkas, K. & Vlachopoulos, C. Interactions between erectile dysfunction, cardiovascular disease and cardiovascular drugs. Nat. Rev. Cardiol. 19, 59–74. https://doi.org/10.1038/s41569-021-00593-6 (2022).
Yannas, D. et al. Erectile Dysfunction is a Hallmark of Cardiovascular Disease: Unavoidable matter of fact or opportunity to Improve men’s Health? JCM. 10, 2221. https://doi.org/10.3390/jcm10102221 (2021).
Shin, D., Pregenzer, G., Gardin, J. M. & Erectile Dysfunction A disease marker for Cardiovascular Disease. Cardiol. Rev. 19, 5–11. https://doi.org/10.1097/CRD.0b013e3181fb7eb8 (2011).
Ganz, P. Erectile Dysfunction: Pathophysiologic mechanisms pointing to underlying Cardiovascular Disease. Am. J. Cardiol. 96, 8–12. https://doi.org/10.1016/j.amjcard.2005.07.004 (2005).
Sangiorgi, G. et al. Pathophysiology, molecular mechanisms, and clinical management of erectile dysfunction in patients affected by coronary artery disease: A review. Biomedicines. 9, 432. https://doi.org/10.3390/biomedicines9040432 (2021). Anatomy.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Author information
Authors and Affiliations
Contributions
H.N.N.D: Conceptualization, methodology, investigation, data curation, writing – original draft, writing – review & editing; T.V.L: Conceptualization, investigation, data curation, writing – original draft, writing – review & editing; H.M.N, A.K.P, T.T.L, and N.D.L: Investigation, data curation; B.A.H and T.A.H: Supervision, writing – review & editing. The final manuscript has been reviewed and approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol garnered approval from the Ethics Committee of the Da Nang City Department of Health (Approval number: 869/BVĐN-HĐYĐ) and the Hue University of Medicine and Pharmacy Ethics Council (Approval number: H2022/869). Written consent was obtained from all patients or their legally authorized representatives. The selection of participating centers adhered strictly to our protocol and conformed rigorously to the principles delineated in the Declaration of Helsinki 2013.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Copyright permission statement
The figures presented in this article are exclusively crafted by the author and have been thoroughly checked for any necessary copyright permissions, including those sourced from the internet.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nguyen Ngoc Dang, H., Viet Luong, T., Kiem Pham, A. et al. Exploring the bidirectional link between erectile dysfunction and 10-year cardiovascular risk in men with diabetes and hypertension. Sci Rep 14, 28816 (2024). https://doi.org/10.1038/s41598-024-78182-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-78182-z
