
Abstract
In the intensive care unit (ICU), acute kidney injury (AKI) is the most common cause of morbidity and mortality. Hospital-acquired acute kidney injury (HAAKI) is AKI developing after 48 h. We aimed to study the development of AKI and its associated risk factors. We conducted a longitudinal observational study. Inclusion criteria were patients > 18 years of age admitted to ICU. The primary outcome was the development of AKI as defined by Kidney Disease Improving Global Outcomes (KDIGO) criteria. A total of 273 patients were included in the study. Out of 273, 44(16.11%) patients developed AKI. The mean age was 45.80(17.39) years, and 60.81% were males. The median acute physiology and chronic health evaluation (APACHE II) and sequential organ failure assessment (SOFA) scores were 12(8–18) and 5(3–7), respectively. Diabetes mellitus (23.44%) and hypertension (23.81%) were predominant comorbidities. The risk factors associated with AKI were serum chloride level, colistin, invasive ventilation, positive end-expiratory pressure (PEEP), and fluid balance. The hospital mortality was significantly higher in patients with AKI (43.18%) as compared with no AKI (14.41%). Among the secondary outcomes, 7 (15.90%) patients required renal replacement therapy (RRT) during hospitalisation. The length of ICU stay was higher in patients with AKI 8(5–13) compared to no AKI 5(3–8). A total of 16.11% developed HAAKI, and mortality was 43.18%. Post 6 months follow-up of AKI patients, mortality was 23%. Among survivors none of the patients were on RRT.Patients admitted with normal kidney function can develop AKI. Hence, careful monitoring of ICU patients is necessary.
Similar content being viewed by others

Introduction
In the ICU, AKI develops due to a renal cause or as an organ failure secondary to nonrenal insult1,2,3. The most common etiology for the development of AKI is sepsis, and it is observed in 50% of the patients with AKI3. AKI is associated with prolonged hospitalisation, need for renal replacement therapy, and has huge cost implications. AKI can progress to acute kidney disease or chronic kidney disease in some patients4.
The incidence of AKI ranges from 20 to 57%1,5,6. In the multinational AKI-EPI study of 1032 ICU patients, > 50% of the patients who developed AKI had higher mortality1. The types of AKI are community-acquired AKI and hospital-acquired AKI (HAAKI)7. Wonnacott A, et al. showed although the incidence of community-acquired AKI was higher (4.3%) and was severe in nature it had a better survival (45% mortality) than HAAKI (62.9% mortality)7.
Meta-analysis by Huang, et al., showed mortality and other outcomes were better in community acquired AKI than in hospital acquired AKI8. HAAKI is seen in older patients and carries higher mortality. The risk factors associated with HAAKI are nephrotoxic medications and sepsis9. Limited studies describe characteristics, risk factors associated with the HAAKI, follow up and outcome of these patients8,9,10.
We aimed to evaluate the proportion of ICU patients developing AKI, risk factors associated with it, and survival rates of AKI patients after hospital discharge over six months in a longitudinal study.
Methodology- A prospective observational study was conducted in a tertiary care hospital from 5th September 2018 to 16th October 2023. Institutional ethics committee approval was obtained (IEC205/2018 dated 28th August 2018, CTRI/2018/09/015615, 5th Sept2018). All the procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975. Strengthening the reporting of observational studies in epidemiology (STROBE) guidelines were followed (Strobe checklist). The written informed consent was obtained from the legally acceptable representative (LAR). The sample size 246 was adequate, with 20% incidence of AKI, 95% confidence interval, and 5% relative precision. With 10% missing data, the total sample size required was 271. The inclusion criteria were patient’s ≥ 18 yrs. of age, admitted in the ICU. Patients were enrolled within 24–48 h. of hospitalization. Patients presenting with AKI or had chronic kidney disease were excluded. Pregnant patients and terminally ill patients were excluded. Diagnosis of HAAKI was made based on the admission creatinine and using KDIGO guidelines. Baseline and demographic characteristics were collected. Acute physiology and chronic health evaluation (APACHE II) and sequential organ failure assessment (SOFA) scores were calculated. Laboratory parameters, serum creatinine, blood urea, electrolytes, fluid balance, need for renal replacement therapy, vasopressors, and ventilator parameters (noninvasive or invasive) were collected for the first seven days of ICU admission. Post ICU transfer, patients were followed up till the hospital discharge. At 6 months from discharge telephonic follow up was done. Survival outcome in the AKI patients was collected.
Statistics
Continuous variables presented as mean (standard deviation SD) or median (interquartile range IQR) as applicable. Categorical data presented as percentages (%). Clinical characteristics compared between AKI and no AKI using independent ‘t test’ or ‘Mann Whitney U’ test as applicable. A generalized linear mixed model analysis was performed to assess the clinical factors associated with the development of AKI over 7 days. Age, gender, history of diabetes mellitus, APACHE II score were considered in the regression model for adjusted analysis. Risk factors associated with the hospital mortality were analysed. Estimation of survival probabilities was done using Kaplan-Meier and log-rank test. The p-value < 0.05 was considered statistically significant. Statistical analysis was done using STATA 15.0.
Results
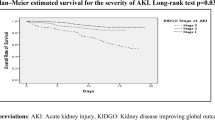
A total of 273 patients were included in the analysis. The mean age was 45.80(standard deviation SD 17.39) yrs., and predominantly were males (60.81%). Out of 273, 44 (16.11%) patients developed AKI. Among 44 patients, 28(63.64%), 11(25%) and 5(11.36%) patients developed stage 1, 2 and 3 AKI respectively. Total 7 patients (15.90%) required renal replacement therapy.
Comparison of baseline characteristics of the patients with AKI and no AKI is presented in Table 1. Mean age of the AKI patients was significantly higher than no AKI group (p < 0.01). Presence of any comorbidities was significantly associated with the development of AKI (p = 0.027). Diabetes mellitus and ischemic heart disease (IHD) were significantly associated with the development of AKI. Patients of AKI had significantly higher median APACHE II 16 (12–23) score, higher requirement of vasopressors on day1, and invasive ventilation. Postoperative status and sepsis were not significantly associated with the development of AKI. Readmissions were significantly associated with the development of AKI.
Primary and secondary outcomes
Total 44(16.11%) patients developed AKI. Overall, the mortality rate was 19.05%. The mortality was significantly higher in AKI (43.18%) as compared to no AKI group (14.41%). The length of ICU stay was significantly higher in AKI group (8 Vs. 5 median days, p = 0.001). Factors associated with the development of AKI are presented in Table 2. Patient with increased serum chloride [1.06 (1.03, 1.08)], requiring invasive ventilation [2.583(1.708, 3.905)], PEEP [1.126 (1.02, 1.24)], received colistin [1.98 (1.22, 3.19)], requiring fentanyl [1.78, (1.28, 2.48)], dexmedetomidine [1.92 (1.02, 3.61)], increased fluid balance [1.05 (1.02, 1.08)] had higher odds for AKI. Low molecular weight heparin (LMWH), furosemide, midazlam and pantoprazole were found to be protective.
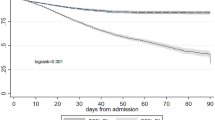
The risk factors associated with hospital mortality were elderly patients, higher APACHE II score, and AKI. Presence of AKI had higher odds [1.626(1.164–2.272)] for hospital mortality (Table 3). Figure 1 shows a comparison of survival plots between AKI and no AKI using Kaplan-Meier survival curve. Significant difference in the survival probability was noted between AKI and no AKI groups showing patients with AKI had significantly lower survival (p = 0.01) (Fig. 1).

Kaplan-Meier graph showing comparison of survival probabilities between patients with AKI and no AKI.
Among 44 patients of AKI, 25 discharged from the hospital. On follow-up of AKI patients, after 6 months of discharge, data of 22 patients was available. We observed a mortality of (5/22) 23%. Among the patients who were alive none was requiring renal replacement therapy.
Discussion
Among 273 ICU patients, 44 developed acute kidney injury. The mean age was [50.61(SD17.53) yrs] significantly higher in patients who developed AKI in our study. This was similar to the study published by Biradar, et al9. Our study had predominantly younger population as against older population seen in sepsis associated AKI11.
We observed 43.18% mortality among AKI patients. Singh, et al., described clinical profile of the patients of HAAKI who were admitted in the medical, surgical ward or intensive care unit showed higher mortality in ICU (73.5%) patients due to multiorgan involvement10. Multinational, multicentre observational study of AKI also showed mortality of 60.3%12. Long term follow up of RENAL trial observed 62–63% mortality and 5.1–5.8% patients were on RRT13. In our study mortality at the end of six months was 23%. We observed lower mortality in follow up patients possibly due to less severe AKI and none of the patients were requiring RRT.
Presence of one or more comorbidities had higher odds for AKI [2.07(1.07–3.99)]. Among the comorbidities we observed diabetes mellitus and ischemic heart disease were significantly associated with AKI. The study by Hoste, et al. showed higher proportions of patients with diabetes and hypertension developed AKI1.
We observed administration of intravenous contrast was not associated with HAAKI. The clinical decision about administration of intravenous contrast needs to be individualized after carefully evaluating risk and benefits. Although, antiedema therapy with mannitol and 3% saline was not associated with the development of AKI in our study, higher serum chloride level was associated with AKI. Chloride excess causes vasoconstriction of the afferent glomerulus and decreases glomerular filtration rate14. This indicates careful monitoring of electrolytes especially chloride in ICU patients. However, the available evidence about hyperchloremia and development of AKI is mixed15,16,17,18. The meta-analysis of 8 studies showed no difference in development of AKI and type of fluid used18. Surprisingly studies done in pediatric population showed chloride levels associated with the development of AKI19.
Colistin was associated with higher risk of AKI with the adjusted odds ratio of 1.980(1.226, 3.195). However, study by Rocco et al., did not find association between colistin methane sulphonate (CMS) and development of AKI. The patients included in this study were elderly with median age of 61(43–78) years20. The preparation used in our study was CMS, 1 million equals 80 mg and we used loading dose of 9 million international units (MIU) followed by 4.5 MIU 12 h. Lower dose was used in study by Rocco et al.as compared to our study. Hence while comparing the results emphasis should be given to colistin preparation, concentration per 1 MIU and dose used. The meta-analysis including 34 studies showed colistin is being used as a last therapeutic strategy for multidrug resistant gram-negative bacteria. Hence the development of AKI should not be the limiting factor for its use21. Higher dose is necessary to achieve the serum concentration above minimum inhibitory concentration in critically ill patients22.
We did not find any protective effect of steroids in preventing AKI. The study by Rubin et al., in patients of COVID-19 showed patients who received dexamethasone had lesser risk of AKI23. This observation needs to be studied in future trials. Multicentre study from Belgium in COVID-19 patients found older age, obesity, higher APACHE II and requirement of invasive ventilation were the risk factors associated with AKI24. These were similar to our study.
Interesting observation was patients who were requiring invasive ventilation or positive end expiratory pressure (PEEP) either during invasive or noninvasive ventilation had significantly higher risk of AKI. Similar observation was seen in covid patients and PEEP had shown fivefold increase in the risk of AKI25. The systematic review and meta-analysis of 31 studies showed invasive mechanical ventilation as a risk factor for AKI26. This indicates although PEEP is beneficial in improving oxygenation one need to check its effects on kidney.
Among the sedatives, fentanyl and dexmedetomidine had higher odds for AKI. The post hoc analysis of the randomized controlled trial showed lesser renal impairment was seen with no sedation strategy27. We could not find any evidence showing fentanyl or dexmedetomidine as a possible risk factor for AKI. We observed patients who were on invasive ventilator support were on sedatives. Hence invasive ventilation was a possible risk factor for AKI. Among patients who were on midazolam we observed lesser renal impairment (p = 0.031). The patients who received midazolam were predominantly neurological patients who presented with neurotrauma or had presented with seizures. Antiepileptic effect of midazolam was possibly renal protective. We did not find any association with use of paralytics like vecuronium and AKI.
Positive fluid balance has been shown to be associated with AKI and mortality in various studies28,29. The fluid overload leads to distension of renal capsule, congestion and causes decrease in glomerular filtration rate. We observed positive fluid balance as a risk factor for AKI and administration of diuretics had a protective effect. Possible reason being diuretics would have helped in managing fluid balance and thereby reducing the development of AKI. The findings of our study are similar to FACTT study, where use of diuretics was not associated with new onset non-pulmonary organ failure30,31.
We observed lesser risk of AKI with pantoprazole. As per the available literature it is one of the drugs causing interstitial nephritis32. However, there are animal studies reporting protective effect of pantoprazole33. This needs to be studied in future trials.
Also, LMWH was associated with lesser risk of AKI. We could not find any evidence supporting this finding and possible reason could be formation of microthrombi causing AKI. Similar etiology was found in AKI seen in COVID-19 patients34. This needs to be studied in future trials.
The strengths of our study are this is one of the study that showed the longitudinal data of patients who developed HAAKI and also included follow up of these patients. We observed several risk factors associated with HAAKI. We studied various medications which are routinely used in ICU patients. The findings of this study will help the clinicians in identifying patients at risk of developing HAAKI.
There are certain limitations. AKI was diagnosed based on the serum creatinine only. The measurement of hourly urine output requires intensive monitoring of the patient and is associated with errors. Hence, we used change in the serum creatinine to diagnose AKI. We did not study the effect of antifungals (Amphotericin B) as only 5(1.83%) patients received this drug. The future studies should focus on early diagnosis of AKI using a specific biomarker.
The results of the study showed possible modifiable risk factors like monitoring of serum chloride levels, fluid balance and early weaning thereby reducing the effect of PEEP and sedation. Findings of this study need to be validated in a larger cohort.
Conclusion
The proportion of patients developing AKI was 16.11%. Risk factors associated with AKI were high serum chloride level, colistin, invasive ventilation, PEEP, and fluid balance. Mortality was higher (43.18%) in AKI patients. Among patients of AKI, 7 (15.90%) required RRT. At the end of six-month, mortality was 23%. As AKI is associated with the higher mortality vigilant monitoring for risk factors is necessary in ICU patients.
Data availability
Data will be available on reasonable request from the principal investigator, Dr Amarja Ashok Havaldar.
References
Hoste, E. A. et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 41, 1411–1423 (2015).
Abebe, A. et al. Mortality and predictors of acute kidney injury in adults: a hospital-based prospective observational study. Sci. Rep. 11 (1), 15672 (2021).
Kuwabara, S., Goggins, E. & Okusa, M. D. The pathophysiology of sepsis-associated AKI. Clin. J. Am. Soc. Nephrol. 17 (7), 1050–1069 (2022).
Levey, A. S. & Defining, A. K. D. The spectrum of AKI, AKD, and CKD. Nephron. 146 (3), 302–305 (2022).
Bouchard, J. et al. A prospective international multicenter study of AKI in the intensive care unit. Clin. J. Am. Soc. Nephrol. 10 (8), 1324–1331 (2015).
Schwager, E. et al. Accurate and interpretable prediction of ICU-acquired AKI. J. Crit. Care. 75, 154278 (2023).
Wonnacott, A. et al. Epidemiology and outcomes in community-acquired versus hospital-acquired AKI. Clin. J. Am. Soc. Nephrology: CJASN. 9 (6), 1007 (2014).
Huang, L. et al. Clinical characteristics and outcomes of community-acquired versus hospital-acquired acute kidney injury: a meta-analysis. Kidney Blood Press. Res. 44 (5), 879–896 (2019).
Biradar, V. et al. Clinical spectrum of hospital acquired renal failure: a study from tertiary care hospital. Indian J. Nephrol. 14 (3), 93–96 (2004).
Singh, T. B. et al. Hospital-acquired acute kidney injury in medical, surgical, and intensive care unit: a comparative study. Indian J. Nephrol. 23 (1), 24 (2013).
White, K. C. et al. Sepsis-associated acute kidney injury in the intensive care unit: incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes. A multicenter, observational study. Intensive Care Med. 49 (9), 1079–1089 (2023).
Uchino, S. et al. Acute renal failure in critically ill patients: a multinational, multicenter study. Jama. 294 (7), 813–818 (2005).
Gallagher, M. et al. Long-term survival and dialysis dependency following acute kidney injury in intensive care: extended follow-up of a randomized controlled trial. PLoS Med. 11 (2), e1001601 (2014).
Pfortmueller, C. A. et al. Serum chloride levels in critical illness—the hidden story. Intensive care Med. Experimental. 6, 1–4 (2018).
Yessayan, L. et al. Acute kidney Injury in critical illness Study Group. Effect of hyperchloremia on acute kidney injury in critically ill septic patients: a retrospective cohort study. BMC Nephrol. 18, 1–9 (2017).
Commereuc, M. et al. Hyperchloremia is not associated with AKI or death in septic shock patients: results of a post hoc analysis of the HYPER2S trial. Ann. Intensiv. Care. 9, 1–9 (2019).
Semler, M. W. et al. Balanced crystalloids versus saline in critically ill adults. N. Engl. J. Med. 378 (9), 829–839 (2018).
Xue, M. et al. Effects of chloride content of intravenous crystalloid solutions in critically ill adult patients: a meta-analysis with trial sequential analysis of randomized trials. Ann. Intensiv. Care. 9, 1–6 (2019).
Mhanna, A. et al. Balanced crystalloids versus isotonic saline in pediatric sepsis: a comprehensive systematic review and meta-analysis. Proc. (Bayl Univ. Med. Cent). 37 (2), 295–302. https://doi.org/10.1080/08998280.2024.2301904 (2024).
Rocco, M. et al. Risk factors for acute kidney injury in critically ill patients receiving high intravenous doses of colistin methanesulfonate and/or other nephrotoxic antibiotics: a retrospective cohort study. Crit. Care. 17, 1–1 (2013).
Chien, H. T. et al. Is colistin-associated acute kidney injury clinically important in adults? A systematic review and meta-analysis. Int. J. Antimicrob. Agents. 55 (3), 105889 (2020).
Karaiskos, I. et al. Colistin population pharmacokinetics after application of a loading dose of 9 MU colistin methanesulfonate in critically ill patients. Antimicrob. Agents Chemother. 59 (12), 7240–7248 (2015).
Rubin, S. et al. Impact of dexamethasone in severe COVID-19-induced acute kidney injury: a multicenter cohort study. Ann. Intensiv. Care. 14 (1), 26 (2024).
Schaubroeck, H. et al. Acute kidney injury in critical COVID-19: a multicenter cohort analysis in seven large hospitals in Belgium. Crit. Care. 26 (1), 225 (2022).
Ottolina, D. et al. Acute kidney injury (AKI) in patients with Covid-19 infection is associated with ventilatory management with elevated positive end-expiratory pressure (PEEP). J. Nephrol. 35 (1), 99–111 (2022).
van den Akker, J. P., Egal, M. & Groeneveld, A. J. Invasive mechanical ventilation as a risk factor for acute kidney injury in the critically ill: a systematic review and meta-analysis. Crit. Care. 17, 1–9 (2013).
Strøm, T. et al. Sedation and renal impairment in critically ill patients: a post hoc analysis of a randomized trial. Crit. Care. 15, 1–6 (2011).
Salahuddin, N. et al. Fluid overload is an independent risk factor for acute kidney injury in critically ill patients: results of a cohort study. BMC Nephrol. 18, 1–8 (2017).
Zhang, J. et al. Cumulative fluid accumulation is associated with the development of acute kidney injury and non-recovery of renal function: a retrospective analysis. Crit. Care. 23, 1–0 (2019).
Grams, M. E. et al. Fluid balance, diuretic use, and mortality in acute kidney injury. Clin. J. Am. Soc. Nephrol. 6 (5), 966–973 (2011).
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 354 (24), 2564–2575 (2006).
Ra, A. & Tobe, S. W. Acute interstitial nephritis due to pantoprazole. Ann. Pharmacother. 38 (1), 41–45 (2004).
Yan, X. X. et al. Protective effect of pantoprazole against sepsis-induced acute lung and kidney injury in rats. Am. J. Translational Res. 11 (8), 5197 (2019).
Rapkiewicz, A. V. et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: a case series. EClinicalMedicine. 24, 100434 (2020).
Acknowledgements
We would like to thank all staffs who helped in completing this project.
Author information
Authors and Affiliations
Contributions
AAH-Concept, design, data collection, conduct, writing of the final draft, EAC, SBS, MHS, MN - conduct and data collection. SS -Helped in statistical analysis and writing the manuscript. All the authors have approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
IEC approval was obtained from the respective hospitals. Consent was obtained from the legally acceptable representative (LAR).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Havaldar, A.A., Sushmitha, E.C., Shrouf, S.B. et al. Epidemiological study of hospital acquired acute kidney injury in critically ill and its effect on the survival. Sci Rep 14, 28129 (2024). https://doi.org/10.1038/s41598-024-79533-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-79533-6
