
Abstract
Disinfection is a critical process to ensure the safety of drinking water. To curb the spread of various bacteria and viruses, disinfectants are extensively employed in communities, hospitals, sewage treatment plants, and other settings. However, disinfectants can produce disinfection by-products (DBPs) that threaten human health. Despite their importance, research and systematic analyses of these risks remain limited. This study monitored DBPs in drinking water across 13 districts and counties in Hangzhou, conducting a risk assessment based on the health risk assessment model recommended by the United States Environmental Protection Agency. Concentrations of 12 DBPs ranged from 0.01 µg/L to 120 µg/L, with levels in 2020–2022 generally exceeding those in 2018–2019. Notably, median concentrations of trichloromethane peaked at 18.00 µg/L in 2021. Most DBPs are detected at higher concentrations in the central and northern parts. However, the spatial distribution of DBPs in drinking water was determined to be random. The health risks associated with most DBPs were higher in 2021 compared to other years. Cancer risks of DBPs ranged between 10− 6 and 10− 4 and noncarcinogenic risks were below 1. This study demonstrates that increased disinfectant use during water treatment may elevates DBPs concentrations.
Similar content being viewed by others


Introduction
Disinfection is a crucial component of the drinking water treatment process and a vital measure to ensure the safety of public water supply systems. It prevents microbial infections and diseases, thereby enhancing drinking water quality and safeguarding public health1. However, disinfectants such as chlorine, ozone, chlorine dioxide, and chloramine are strong oxidants. When natural organic matter (NOM) is present in water, these disinfectants react with NOM to form disinfection by-products (DBPs)2,3. Since their discovery in 1974, over 800 DBPs have been identified in drinking water4,5, including carbonaceous DBPs like trihalomethanes (THMs) and haloacetic acids (HAAs), and nitrogenous DBPs such as nitrosodimethylamine, haloacetonitriles (HANs), and haloacetamides6.7. The formation of these DBPs depends on the type of NOM, inorganic constituents, and other physicochemical factors such as pH and temperature, leading to the creation of various DBP classes like THMs, HAAs, HANs, haloketones, and trihalophenols. Most DBPs are potential human carcinogens and mutagens, often linked to rectal and colon cancers, as well as developmental and reproductive disorders8. Research on drinking water DBPs in China indicates that THMs and HAAs are the most prevalent DBPs formed during chlorination and other disinfection processes9,10. The United States Environmental Protection Agency (US EPA) regulates THMs and HAAs in drinking water, with maximum contaminant levels (MCLs) of 80 µg/L and 60 µg/L, respectively11.
The adverse biological responses to DBPs include cytotoxicity, genotoxicity, mutagenicity, teratogenicity, induction of reactive oxygen species, and enhancement of antibiotic-resistant pathogens12,13. Over the past 40 years, numerous studies have investigated the potential health risks posed by these compounds. Epidemiological evidence links exposure to DBPs with an increased risk of bladder cancer and reproductive effects14,15. Some DBPs are potential or known human carcinogens that can cause bladder and colon cancer16.
Most scientific studies since the outbreak of SARS-CoV-2 have focused on the efficiency of virus elimination or deactivation17,18. Disinfection has been considered the most effective measure to eliminate or deactivate viruses, including SARS-CoV-2, and prevent transmission. Consequently, the dose of disinfectants in domestic wastewater and drinking water was elevated to curb the spread of SARS-CoV-219. However, only a few studies have evaluated the changes in the occurrence, distribution, and potential risks of DBPs resulting from the increased use of disinfectants18,20. This study analyzed the contamination of DBPs in Hangzhou’s drinking water sources and conducted a risk assessment to better understand the impact of disinfection on drinking water, providing data support for ensuring the safety of drinking water in Hangzhou.
Materials and methods
Study area
Hangzhou, the capital city of Zhejiang Province in East China, comprises 10 municipal districts and 3 counties which is illustrated in Fig. 1. Covering a total area of 16,850 square kilometers, Hangzhou had a resident population of 12,376,000 as of the end of 2022.

Geographical location of Hangzhou, China.
Sample collection
From 2018 to 2022, a total of 490 water plants in Hangzhou were sampled. Among these, 176 plants had a processing capacity of over 1,000 cubic meters /Day, including 65 urban and 111 rural plants. Small water plant was defined as the processing capacity of below cubic meters/Day. And there were 314 plants with the capacity below 1,000 cubic meters /Day, comprising 7 urban and 307 rural plants. Almost 470 water plants are treated with hypochlorite chemicals, and the other water plants are treated with chlorine dioxide. A total of 4,403 drinking water samples were collected from 13 districts and counties in Hangzhou, Zhejiang Province, China. These samples were collected from each water plant twice a year. The number of water samples each year were 775, 717, 886, 905 and 1120 respectively.
Treated water refers to the water treated by centralized water supply units. Treated water was collected before entering the delivery pipeline and a total of 1397 treated water were collected. Secondary water supply systems (SWSSs) refer to the in-building infrastructures (e.g., water tanks, pumps, pipes) that are used to store, pressurize and transport water from the distribution main to taps. SWSSs are commonly constructed in multi-floor and high-rise buildings in metropolitan cities, and they provide adequate hydraulic pressure for higher floors and equalize water demands. SWSSs with a total of 387 samples were collected at the user’s faucet. Tap water refers to the water that was transported from the factory through the water supply network to the terminal without SWSSs. Tap water with a total of 2619 samples were collected at the user’s faucet.
Sample analysis
Two regular parameters of 4403 water samples were analyzed, which included trichloromethane (TCM) and carbon tetrachloride (CT). 47 out of 4403 water samples were tested for 10 non-regular parameters: dibromochloromethane (DBCM), bromodichloromethane (BDCM), methylene chloride (DCM), trihalomethanes (THMs), 1,2-dichloroethane (1,2-DCA), 1,1,1-trichloroethane (1,1,1-TCA), bromoform (TBM), dichloroacetic acid (DCAA), trichloroacetic acid (TCAA) and trichloroethanal (CH). All 47 water samples were collection from 8 urban plants with the capacity of over 1,000 cubic meters/Day and were treated water. According to the state standard, THMs includes TCM, DBCM, BDCM and TBM. The THMs used was the sum of the individual species.
The collection, preservation, and analysis of DBPs followed the Chinese Standard Examination Methods for Drinking Water (GB/T 5750 − 2006)21. Samples were filled in brown glass bottles to protect from sunlight until they overflowed. Hydrochloric acid was used to adjust the pH to below 2. Water temperature and residual chlorine concentration were measured on the spot. Water samples were stored and transported at 4 °C. Results were evaluated according to the Health Standard for Drinking Water (GB 5749 − 2006)22 and the limits of DBPs were listed in Table 2.
The elution-trapping/gas chromatography-mass spectrometry (GC-MS) method was employed followed the Chinese Standard Examination Methods for Drinking Water (GB/T 5750 − 2006)21. Reagents and materials included methanol (Purity99.99%, Fisher), purified water (LC/MS Grade, Fisher), and standard stock solutions. The GC-MS underwent performance testing and was calibrated using the external standard method. TCM (99.92%), CT (99.92%), DBCM (98.1%), BDCM (97.3%), and TBM (99.73%) were prepared. The samples were injected with an injection port temperature of 150 °C and in split mode with a split ratio of 5:1. Helium gas (purity 99.999%) was used as carrier gas at a constant flow rate of 30 mL/min, and the injection volume was 30 µL. The GC oven temperature was programmed from 60 °C (held for 3 min) to 150 °C at 30 mL/min, hold for 10 min. The GC-MS was adjusted to meet the analysis conditions. The temperatures of the transfer line, quadrupole, and ion source were 150 °C, 85 °C, and 180 °C, respectively. It was followed by purging, trapping, desorbing, and automatic injection into the GC-MS for qualitative and quantitative analyses at room temperature. The method limit of detection (LOD) was also listed in Table 2. Values reported below LOD were substituted with values equal to half of LOD.
Health risk assessment
This study conducted a health risk assessment of DBPs in Hangzhou City’s drinking water using the health risk assessment model recommended by the US EPA11.
Cancer risk assessment
Cancer risk is often expressed as a risk value (R). Generally, a risk greater than 10− 6 indicates a certain cancer risk, while a risk greater than 10− 4 indicates an unacceptable cancer risk. When there are multiple pollutants, the total of cancer risk (RT) is the sum of the risks of each pollutant. The variables and parameters are illustrated in Tables 1 and 2.
The formulas are as follows:
Noncarcinogenic risk assessment
Noncarcinogenic risks are described using the hazard quotient (HQ). Generally, an HQ less than 1 indicates a low noncarcinogenic risk, whereas an HQ of 1 or greater indicates a high noncarcinogenic risk. The HQ of each component was calculated by dividing the average daily dose (ADD) by the reference dose (RfD) as follows:
Statistical analysis
Statistical analyses were performed using version 26.0. Data in accordance with non-normal distribution were expressed as median, p25 and p75. Comparisons among different years were performed using non-parametric test (the Kruskal Wallis test). The test statistic used in this test was called the H statistic. Differences were considered statistically significant at P < 0.05.
The geographical distributions of DBPs concentrations of were mapped by ArcGIS software version 10.4 using the spatial statistical analysis module. The Moran’s I value for global spatial autocorrelations was computed. Moran’s I is a way to measure spacial autocorrelation. It’s a way to quantify how closely values are clustered together in a 2-D space. Spatial autocorrelation assesses the patterns of spatial aggregation of DBPs across Hangzhou, expressed through Moran’s I index, which ranges from − 1 to 1.
Results
Occurrence of DBPs in drinking water
A total of 4,403 drinking water samples were collected and analyzed for TCM and CT from 2018 to 2022. Only 7 water samples of TCM were higher than the limit set by the Standard for Drinking Water Quality of China (GB 5749 − 2006; 60 µg/L)22, which ranged from 67 µg/L to 120 µg/L. All 7 water samples were collected from rural plants with the capacity below 1,000 cubic meters/Day. The median concentration of TCM was 18 µg/L in 2021, which was the highest in 5 years, and that was 2.5 µg/L in 2019. The concentration of CT in all samples were below 2 µg/L, which conformed with the state standard. As shown in Fig. 2, there was a statistically significant difference in the median concentrations of TCM over the past five years. The same significant difference was also observed in CT. Notably, median concentrations of TCM peaked at 18.00 µg/L in 2021.

The annual median concentrations of TCM and CT in 4403 water samples in the past 5 years (µg/L).
Forty-seven treated water samples were collected and analyzed for 10 DBPs from 2018 to 2022, including DBCM, BDCM, DCAA, DCM, TCAA, CH, THMs, 1,2-DCA, 1,1,1-TCA, and TBM. Figure 3 presents the concentrations of non-regular parameters in treated water. The results for these DBPs were below the limits of the Standard for Drinking Water Quality of China22. 8 indicators of DBCM, BDCM, DCAA, DCM, TCAA, CH, THMs and TBM had significant differences from 2018 to 2022. However, the medians of 1,2-DCA and 1,1,1-TCA showed no significant trends over the five-year period.

The annual concentration of 10 DBPs in 47 water samples in the past 5 years (µg/L).
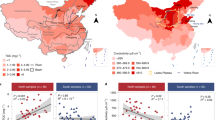
The spatial grade distribution of DBPs in drinking water is illustrated in Fig. 4, where darker colors represent higher concentrations in the relevant district or county. Higher concentrations of TCM, DBCM, 1,2-DCA, and 1,1,1-TCA are primarily found in the central regions. Higher concentrations of CT are mainly located in the northeastern regions. Elevated levels of BDCM, THMs, and CH are mainly found in the southern areas. Higher concentrations of DCAA and DCM are primarily in the southeastern regions. TCAA concentrations are predominantly higher in the northern areas, while TBM concentrations are higher in the central areas. Overall, most DBPs are detected at higher concentrations in the central and northern parts.


(a). The spatial grade distribution of DBPs in Hangzhou. (b). The spatial grade distribution of DBPs in Hangzhou.
Spatial autocorrelation analysis
The global Moran’s I results indicated that the Moran’s I values for TCM, BDCM, DCAA, CH, and THMs in Hangzhou’s drinking water from 2018 to 2022 were all greater than 0, with values of 0.058, 0.082, 0.032, 0.029, and 0.006, respectively. Conversely, the Moran’s I value for CT, DBCM, DCM, TCAA, 1,2-DCA, 1,1,1-TCA, and TBM were all less than 0, with values of − 0.044, − 0.252, − 0.282, − 0.077, − 0.163, − 0.095, and − 0.098, respectively. However, since all P-values were more than 0.05, the spatial distribution of DBPs in drinking water was determined to be random. Details are provided in Table 3.
Comparison of the concentrations of DBPs in drinking water
Table 4 shows that the median concentrations of TCM and CT in treated water, tap water and SWSSs. All three types of water showed higher TCM and CT values in 2020–2022 compared to those in 2018–2019.
Table 5 presents a comparison of non-regular parameters between different years in treated water. The median concentrations of BDCM, DCAA, DCM, CH and 1,1,1-TCA showed statistical differences between 2018 and 2022. However, these differences were not observed in other 5 indicators. BDCM and CH were significantly higher in 2018 than in other years. And DCM reached its highest point in 2019, while DCAA reached its highest point in 2021.
Cancer risk of DBPs
As shown in Table 6, the cancer risk values of TCM and CT in treated water, tap water, and SWSSs were higher in 2020, 2021, and 2022 compared to other years. Females had the highest cancer risk for TCM in SWSSs in 2021 (6.86 × 10− 6) and for CT in treated water in 2022 (2.26 × 10− 6). Overall, the cancer risks for the regular parameters of DBPs were all lower than 10⁻⁴, indicating that the cancer risk posed by TCM and CT is low.
As shown in Table 7, the cancer risk values of DBCM and BDCM in 2018 were higher than in other years, with females having the highest cancer risk (9.40 × 10− 6 and 7.74 × 10− 6, respectively). The cancer risk value of DCAA in 2021 was higher than in other years, with females having the highest cancer risk (11.46 × 10− 6). The cancer risk value of DCM in 2019 was higher than in other years, with females having the highest cancer risk (0.42 × 10− 6). The cancer risk value of TCAA in 2021 was higher than in other years, with females having the highest cancer risk (16.22 × 10− 6). The cancer risk value of TBM in 2018 was higher than in other years, with females having the highest cancer risk (5.95 × 10− 6). All results ranged between 10− 6 and 10− 4, indicating they were within the acceptable range.
Noncarcinogenic risk of DBPs
The noncarcinogenic risks of the regular parameters for DBPs are shown in Table 8. The noncarcinogenic risks of TCM and CT in treated water, tap water, and SWSSs in 2020, 2021, and 2022 were higher than in other years. SWSSs had the highest effect on females in 2021 (9.80 × 10− 2). CT had the highest noncarcinogenic risk in treated water for females in 2022 (4.62 × 10− 2). Overall, the noncarcinogenic risk of DBPs in drinking water was lower than 1, which is acceptable in China.
As shown in Table 9, the noncarcinogenic risk values of DBCM, BDCM, CH, and TBM in 2018 were higher than in other years, with females having the highest noncarcinogenic risks (1.60 × 10− 2, 1.78 × 10− 2, 0.36 × 10− 2, and 1.08 × 10− 2, respectively). The noncarcinogenic risk values of DCAA and TCAA in 2021 were higher than in other years, with females having the highest noncarcinogenic risks (16.38 × 10− 2 and 3.31 × 10− 2, respectively). The noncarcinogenic risk value of DCM in 2019 was higher than in other years, with females having the highest noncarcinogenic risk (9.94 × 10− 2). All results were lower than 1, indicating they were within the acceptable range.
Discussion
In recent decades, water pollution has become a global concern due to the substantial increase in the demand for safe water driven by overpopulation23,24. This study analyzed the distribution of DBPs from 2018 to 2022 and estimated their health risks in drinking water, which is crucial for understanding the water quality during infectious disease epidemics. The concentrations of TCM and CT in drinking water from 2020 to 2022 were higher than those in previous years. The total carcinogenic risk of exposure was lower than 10−4, and the total HQT of DBP exposure in drinking water was lower than 1, indicating acceptable levels based on the results from 490 drinking water treatment plants in Hangzhou.
Both World Health Organization (WHO) and China have set limits on the concentration of DBPs25. The US EPA26 and Health Canada27 specified the MCL of THMs as 80 µg/L. In this study, the maximum concentrations of CT, DBCM, BDCM, DCAA, DCM, TCAA, CH, THMs, 1,2-DCA, 1,1,1-TCA, and TBM were below the standard limits, except for TCM with the highest concentrations of 120 µg/L. The median concentrations of TCM, CT, and DCAA in 2021 were greater than those in other years. Increased formation of individual DBPs is generally attributed to increased disinfectant doses and residual chlorine28,29. The increase in the use of chlorine disinfectants during the COVID-19 may lead to an increase in the residual concentration of disinfectants in the source water and the environment. Therefore, the concentration of DBPs in drinking water has also increased. This finding contrasts with previously published results showing that increased disinfectant use within the guideline range did not result in significant increases in DBP concentrations30. This difference may be attributed to varied monitoring times and locations.
This study utilized both regular and non-regular parameters for monitoring DBPs. The regular parameters for TCM were significantly higher than those for CT, and the non-regular parameters for THMs were higher than haloacetic acids (HAAs) and halogenated acetaldehyde (HA). This finding aligns with a study showing THMs in parts of China (3.26–69.28 µg/L) ranked highest among DBPs but remained below the US EPA’s maximum contamination limits31. In Croatian drinking water, DBP values ranged from 0.40 µg/L to 30.90 µg/L for TCM, which were lower than those in this study; however, TBM values ranged from the limit of quantification (LOQ) to 16.6 µg/L, higher than the results of this study. BDCM concentrations in Croatian drinking water were lower than those in 2018 and 2021 in this study but higher than those in 2019, 2020, and 2022. TBM concentrations in Croatian drinking water were higher than those observed in 2018–2022 in this study, while DCAA and TCAA concentrations were lower than those in 2021 but higher than those in other years32. Lower results for HAAs (DCAA, TCAA) compared to THMs may be due to the increased potential for HAA formation in the first 3 h of chlorination; as contact time increases, residual chlorine levels decrease, reducing HAA formation33,34. The findings are consistent with other studies indicating that chlorinated disinfected water yields higher concentrations of THMs than HAAs35,36. Regular parameters were divided among three different water bodies for monitoring, with higher DBP concentrations found in treated water than in tap water and SWSSs. Additionally, TCM’s relatively low boiling point may contribute to its reduction during pipe network transportation31.
The results showed that the total cancer risk values for regular and non-regular parameters were between 10− 6 and 10− 4, and the total noncarcinogenic risk value was less than 1, which is considered acceptable. Among regular parameters, the TCM concentration in treated water posed a greater health risk than other DBPs. A study by the National Cancer Institute confirmed the carcinogenic effect of TCM in experimental animals, and a subsequent Salmonella mutagenicity test confirmed the mutagenic effect of organic extracts of drinking water37,38. Compared to other non-regular parameters, TCAA and DCAA in treated water had the highest cancer and noncarcinogenic risks, respectively. Most CDBPs are potentially carcinogenic, teratogenic, and mutagenic, with HAAs, bromate, and THMs being more carcinogenic, while halogenated acetonitriles, halogenated cyanides, and halogenated nitromethanes are more teratogenic and mutagenic39,40. A study determined the annual average THM levels in municipal drinking water in 28 European countries from routine surveillance records for 2005–2018 and estimated that 4.90% of bladder cancer cases in the EU population were attributable to THM exposure in drinking water41. Therefore, the presence of DBPs in drinking water remains a significant risk factor for human health.
This study has several limitations. Estimating DBPs concentrations as half of LOD may lead to overestimations. Additionally, the Chinese population’s habit of drinking boiled water rather than direct tap water may result in overestimated health risks when using treated water concentrations for assessment. Moreover, health effects on the skin, respiratory system, and other physiological systems from airborne volatile disinfectants and DBPs were not considered, as this study focused solely on oral exposure routes. Further studies are necessary to accurately assess the health risks of DBPs in drinking water.
Conclusion
This study compared the distribution and health risks of different DBPs in 490 water plants from 2018 to 2022. All three types of water showed higher TCM and CT values in 2020–2022 compared to those in 2018–2019. Most DBPs are detected at higher concentrations in the central and northern parts. However, the spatial distribution of DBPs in drinking water was determined to be random. The cancer risk is within the acceptable range and the noncarcinogenic risk of DBPs in Hangzhou’s drinking water was lower than 1, suggesting that long-term consumption is unlikely to cause chronic somatic toxic effects. Developing healthier drinking water disinfection technologies, such as the advanced oxidation processes, nanotechnology and solar radiation, is essential to reduce the health risks associated with DBPs. Studying the health effects of drinking water DBPs is crucial to ensure safe drinking water and protect the health of the Chinese population.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article. Raw data supporting the findings of this study are available from the corresponding author upon reasonable request.
References
Lanrewaju, A. A., Enitan-Folami, A. M., Sabiu, S. & Swalaha, F. M. A review on disinfection methods for inactivation of waterborne viruses. Front. Microbiol. 13, 991856. https://doi.org/10.3389/fmicb.2022.991856 (2022).
Ding, S. et al. Formation and estimated toxicity of trihalomethanes, haloacetonitriles and haloacetamides from the chlor(am)ination of acetaminophen. J. Hazard. Mater. 341, 112–119. https://doi.org/10.1016/j.jhazmat.2017.07.049 (2018).
Ghanadi, M., Kah, M., Kookana, R. S. & Padhye, L. P. Formation of disinfection by-products from microplastics, tire wear particles, and other polymer-based materials. Water Res. 230, 119528. https://doi.org/10.1016/j.watres.2022.119528 (2023).
Culin, J. & Mustac, B. Environmental risks associated with ballast water management systems that create disinfection by-products (DBPs). Ocean. Coastal. Manage. 105, 100–105. https://doi.org/10.1016/j.ocecoaman.2015.01.004 (2015).
Chen, H. et al. Database and review of disinfection by-products since 1974: Constituent elements, molecular weights, and structures. J. Hazard. Mater. 462, 132792. https://doi.org/10.1016/j.jhazmat.2023.132792 (2024).
An, D. et al. Lower molecular weight fractions of PolyDADMAC coagulants disproportionately contribute to N-nitrosodimethylamine formation during water treatment. Water Res. 150, 466–472. https://doi.org/10.1016/j.watres.2018.12.002 (2019).
Vu, T. N., Kimura, S. Y., Plewa, M. J., Richardson, S. D. & Mariñas, B. J. Predominant N-Haloacetamide and haloacetonitrile formation in drinking water via the aldehyde reaction pathway. Environ. Sci. Technol. 53 (2), 850–859. https://doi.org/10.1021/acs.est.8b02862 (2019).
Benmarhnia, T., Delpla, I., Schwarz, L., Rodriguez, M. J. & Levallois, P. Heterogeneity in the relationship between disinfection by-products in drinking water and cancer: A systematic review. Int. J. Environ. Res. Public. Health. 15 (5), 979. https://doi.org/10.3390/ijerph15050979 (2018).
Liu, X., Chen, L., Yang, M., Tan, C. & Chu, W. The occurrence, characteristics, transformation and control of aromatic disinfection by-products: A review. Water Res. 184, 116076. https://doi.org/10.1016/j.watres.2020.116076 (2020).
Mishra, B. K., Gupta, S. K. & Sinha, A. Human health risk analysis from disinfection by-products (DBPs) in drinking and bathing water of some Indian cities. J. Environ. Health Sci. Eng. 12 (73). https://doi.org/10.1186/2052-336x-12-73 (2014).
United States Environmental Protection Agency. National Primary Drinking Water Regulations: Stage 2 Disinfectants and Disinfection Byproducts Rule. In: Final Rule. Washington, DC. pp. 387–493. (2006).
Benson, N. U., Akintokun, O. A. & Adedapo, A. E. Disinfection byproducts in drinking water and evaluation of potential health risks of long-term exposure in Nigeria. J. Environ. Public. Health. 7535797. https://doi.org/10.1155/2017/7535797 (2017).
Parveen, N., Chowdhury, S. & Goel, S. Environmental impacts of the widespread use of chlorine-based disinfectants during the COVID-19 pandemic. Environ. Sci. Pollut. Res. Int. 29 (57), 85742–85760. https://doi.org/10.1007/s11356-021-18316-2 (2022).
Grellier, J., Rushton, L., Briggs, D. J. & Nieuwenhuijsen, M. J. Assessing the human health impacts of exposure to disinfection by-products–a critical review of concepts and methods. Environ. Int. 78, 61–81. https://doi.org/10.1016/j.envint.2015.02.003 (2015).
Shi, J. et al. Exposure to disinfection by-products and risk of cancer: A systematic review and dose-response meta-analysis. Ecotoxicol. Environ. Saf. 270, 115925. https://doi.org/10.1016/j.ecoenv.2023.115925 (2024).
Helte, E., Säve-Söderbergh, M., Larsson, S. C., Martling, A. & Åkesson, A. Disinfection by-products in drinking water and risk of colorectal cancer: A population-based cohort study. J. Natl Cancer Inst. 115 (12), 1597–1604. https://doi.org/10.1093/jnci/djad145 (2023).
Wang, J. et al. Disinfection technology of hospital wastes and wastewater: Suggestions for disinfection strategy during coronavirus disease 2019 (COVID-19) pandemic in China. Environ. Pollut. 262, 114665. https://doi.org/10.1016/j.envpol.2020.114665 (2020).
Zhang, D. et al. Potential spreading risks and disinfection challenges of medical wastewater by the presence of severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) viral RNA in septic tanks of Fangcang Hospital. Sci. Total Environ. 741, 140445. https://doi.org/10.1016/j.scitotenv.2020.140445 (2020).
Rimoldi, S. G. et al. Presence and infectivity of SARS-CoV-2 virus in wastewaters and rivers. Sci. Total Environ. 744, 140911. https://doi.org/10.1016/j.scitotenv.2020.140911 (2020).
Xue, B. et al. The occurrence, ecological risk, and control of disinfection by-products from intensified wastewater disinfection during the COVID-19 pandemic. The Science of the total environment. 900, 165602. (2023). https://doi.org/10.1016/j.scitotenv.2023.165602
Ministry of Health of China. Standards Examination Methods for Drinking Water-Organic Parameters (GB 5750.8–2006). National Health Commission of the People’s Republic of China. (2006b). http://www.nhc.gov.cn/wjw/pgw/201805/31cdfe4324c8458cb6c7d93f1b270133.shtml (in Chinese) (2006).
Ministry of Health of China China. Standards for Drinking Water Quality (GB 5749 – 2006). National Health Commission of the People’s Republic of China. (2006a). http://www.nhc.gov.cn/wjw/pgw/200701/33644.shtml (in Chinese) (2006).
Ranjan, M., Singh, P. K. & Srivastav, A. L. A review of bismuth-based sorptive materials for the removal of major contaminants from drinking water. Environ. Sci. Pollut Res. Int. 27 (15), 17492–17504. https://doi.org/10.1007/s11356-019-05359-9 (2020).
Wu, T. et al. Traditional methods and biosensors for detecting disinfection by-products in water: A review. Environ. Res. 237, 116935. https://doi.org/10.1016/j.envres.2023.116935 (2023).
World Health Organization. Guidelines for drinking-water quality, 4th ed. Geneva. https://www.who.int/publications/i/item/9789241549950 (2011).
United States Environmental Protection Agency. National Primary Drinking Water Regulations.https://www.epa.gov/ground-water-and-drinking-water/national-primary-drinking-water-regulations#Byproducts (2020).
Canada, H. & The Guidelines for Canadian Drinking Water Quality. https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/waterquality/guidelines-canadian-drinking-water-quality-summary-table.html (2020).
Zhang, Y., Chu, W., Yao, D. & Yin, D. Control of aliphatic halogenated DBP precursors with multiple drinking water treatment processes: Formation potential and integrated toxicity. J. Environ. Sci. 58, 322–330. https://doi.org/10.1016/j.jes.2017.03.028 (2017).
Li, X. et al. A review of traditional and emerging residual chlorine quenchers on Disinfection By-Products: Impact and mechanisms. Toxics 11 (5), 410. https://doi.org/10.3390/toxics11050410 (2023).
Li, Z. et al. Occurrence and distribution of disinfection byproducts in domestic wastewater effluent, tap water, and surface water during the SARS-CoV-2 pandemic in China. Environ. Sci. Technol. 55 (7), 4103–4114. https://doi.org/10.1021/acs.est.0c06856 (2021).
Yu, Y. et al. The occurrence and transformation behaviors of disinfection byproducts in drinking water distribution systems in rural areas of eastern China. Chemosphere 228, 101–109. https://doi.org/10.1016/j.chemosphere.2019.04.095 (2019).
Kurajica, L. et al. Disinfection by-products in Croatian drinking water supplies with special emphasis on the water supply network in the city of Zagreb. J. Environ. Manage. 276, 111360. https://doi.org/10.1016/j.jenvman.2020.111360 (2020).
Wei, X., Han, B., Gu, R., Geng, W. & Gao, N. Formation of typical disinfection by-products (DBPs) during chlorination and chloramination of polymyxin B sulfate. RSC Adv. 13 (31), 21537–21544. https://doi.org/10.1039/d3ra01981k (2023).
Liu, T. et al. Temporal and spatial variations of disinfection by-products in South Taihu’s drinking water, Zhejiang Province, China. J. Water Health. 21 (10), 1503–1517. https://doi.org/10.2166/wh.2023.149 (2023).
Padhi, R. K., Subramanian, S. & Satpathy, K. K. Formation, distribution, and speciation of DBPs (THMs, HAAs, ClO(2)(-),andClO(3)(-)) during treatment of different source water with chlorine and chlorine dioxide. Chemosphere 218, 540–550. https://doi.org/10.1016/j.chemosphere.2018.11.100 (2019).
Wang, L. et al. A one-year long survey of temporal disinfection byproducts variations in a consumer’s tap and their removals by a point-of-use facility. Water Res. 159, 203–213. https://doi.org/10.1016/j.watres.2019.04.062 (2019).
Cortés, C. & Marcos, R. Genotoxicity of disinfection byproducts and disinfected waters: A review of recent literature. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 831, 1–12. https://doi.org/10.1016/j.mrgentox.2018.04.005 (2018).
Chen, X. et al. Novel insights into impacts of the 7.20 extreme rainstorm event on water supply security of Henan Province, China: Levels and health risks of tap water disinfection by-products. J. Hazard. Mater. 452, 131323. https://doi.org/10.1016/j.jhazmat (2023).
Richardson, S. D., Plewa, M. J., Wagner, E. D., Schoeny, R. & Demarini, D. M. Occurrence, genotoxicity, and carcinogenicity of regulated and emerging disinfection by-products in drinking water: A review and roadmap for research. Mutat. Res. 636 (1–3), 178–242. https://doi.org/10.1016/j.mrrev.2007.09.001 (2007).
Kali, S. et al. Occurrence, influencing factors, toxicity, regulations, and abatement approaches for disinfection by-products in chlorinated drinking water: A comprehensive review. Environ. Pollution (Barking Essex: 1987). 281, 116950. https://doi.org/10.1016/j.envpol.2021.116950 (2021).
Evlampidou, I. et al. Trihalomethanes in drinking water and bladder cancer burden in the European Union. Environ. Health Perspect. 128 (1), 17001. https://doi.org/10.1289/ehp4495 (2020).
Acknowledgements
The authors thank all participants for their long-term commitment to the study.
Funding
This research was supported by the Health Science and Technology Program Key Projects of Hangzhou (ZD20210026) and the Health Science and Technology Program for Young Innovative Talent Project of Zhejiang (2022RC063).
Author information
Authors and Affiliations
Contributions
L.W. and Z.S.F. wrote the manuscript and analysed data. X.C.Z., K.Y.C. and Y.J.R. helped with statistical analysis and graphing. C.K.L. processes samples, B.G., Y.L. and S.S.X. collected samples, proofread and modifed the format. H.X. provided funding acquisition, supervised the form of the paper. All authors have read and agreed to the submitted version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Funding
This research was supported by the Health Science and Technology Program Key Projects of Hangzhou (ZD20210026) and the Health Science and Technology Program for Young Innovative Talent Project of Zhejiang (2022RC063).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, L., Fang, Z., Zhou, X. et al. Health risk assessment via ingestion of disinfection by-products in drinking water. Sci Rep 15, 1793 (2025). https://doi.org/10.1038/s41598-024-84094-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84094-9
