
Abstract
Biallelic pathogenic variants at TK2 lead to a severe and progressive myopathy (TK2d). For a disease with unspecific clinical findings, and the possibility of a supplementation therapy that changes the natural history of the disease, highlighting clinical features that increase suspicion and accelerate diagnosis is essential. Clinical and genetic findings of 36 Brazilian patients with TK2d were identified and presented in this work. Genotype-phenotype correlation was performed for recurrent and novel variants. Motor and respiratory assessments were systematically performed in 13 patients, three of them were receiving the nucleosides replacement therapy. Natural history data was gathered from the follow up of five adult patients. Eight patients with the infantile form, 19 with childhood-onset and five with late-onset form were described. Extramuscular features were present in 30% of the cohort. Neuropathy and encephalopathy were the clinically predominant features for some patients. Four variants were recurrent (p.Thr108M, p.His121Asn, p.Arg183Trp and c.536_538 + 8del) allowing genotype-phenotype correlations, and one was novel (G91D). P.Thr108Met patients presented a milder presentation when compared to the p.His121Asn group. P.Arg183Trp was associated with peripheral nerve involvement and c.536_538 + 8del with encephalomyopathy. Long-term follow-up of 5 patients harbouring p.Thr108Met showed decreased motor, bulbar, and respiratory function, compared to a dramatic improvement in the treated patients. TK2d is a very debilitating and progressive disease among all forms including the childhood-onset as we demonstrated. Early diagnosis is essential since a potential treatment can change the natural history of the disease. Extramuscular involvement plays an important role for diagnostic strategies.
Similar content being viewed by others

Introduction
Thymidine kinase 2 (TK2) is the enzyme responsible for the phosphorylation of deoxyribonucleosides deoxythymidine and deoxycytidine to deoxythymidine and deoxycytidine monophosphates, respectively. Both are phosphorylated to generate the deoxynucleosides triphosphates needed for the replication of mtDNA1. Biallelic pathogenic variants within the TK2gene result in TK2 deficiency (TK2d) and lead to mtDNA maintenance defects and depletion of mtDNA. This condition typically presents with pure myopathy, although extramuscular involvement may occur2,3.
The initial description by Saada et al. outlined four children with severe myopathy, elevated serum creatine kinase, multiple defects of mitochondrial respiratory chain activity and a low mtDNA copy number in muscle tissue1. Since then, up to 150 additional cases have been described as isolated cases or as part of a case series, revealing clinical and molecular heterogenicity4,5.
Clinical manifestations and severity may vary and often correlate with the age of onset3,4,6,7. From a clinical perspective, three clinical forms are recognized based on the age of symptom onset: infantile-onset (< 1 year), childhood-onset (1–12 years) and late-onset form (> 12 years). In all presentations, patients manifest with progressive proximal and axial weakness, and disproportional respiratory insufficiency with early diaphragm involvement8. Ophthalmoparesis is present often in the late-onset presentation, and encephalopathy was described in severe infantile-onset patients. Despite all similarities, the infantile-onset group presents a very high mortality rate with a post onset survivor of one year, as demonstrated in a previous retrospective natural history study3.
Based on mouse-model data, a supplementation therapy using monophosphate nucleosides to bypass the biochemical defect was developed and showed pronounced clinical benefits at open-label trials, enhancing the importance of an early diagnosis and early treatment to change the lethal natural history of the disease9,10.
In the current study, we aimed to present a comprehensive analysis of the clinical and genetic profile of a large Brazilian cohort of TK2d. Genotype-phenotype correlations were performed among four recurrent variants, and one novel variant was described. A two-year follow-up of three and one-year follow up of two adult patients are presented to gather insights about the natural history of the disease. Furthermore, the data of three patients receiving nucleosides replacement therapy are shown.
Methods
Patients
This is a retrospective and observational study. Thirty-six patients from 27 unrelated families with molecularly confirmed TK2d were included. Patients were recruited from six different tertiary neuromuscular clinics in Brazil. The identified patients were contacted by the attending physician and consented to participate in the study. Four patients were participants of a clinical trial and their clinical information was not available for this study.
Clinical and molecular data were collected from clinical notes using a questionnaire designed for the study. Gastrointestinal involvement (recurrent vomits, recurrent diarrhea, bloating, failure to thrive and early satiety), presence of pain, cardiac involvement, high blood pressure, and CNS involvement were also evaluated according to the chart review and actively asking patients when possible. Results from ancillary exams, such as MRI, EMG, audiometry, serum creatine kinase (CK), serum lactate, echocardiogram, and renal and liver function tests, were collected and included in the analysis. Central involvement was considered for patients presenting with seizures, impairment of consciousness or neurologic regression.
Patients were stratified based on motor function, need for respiratory support (invasive ventilatory support [IVS] or noninvasive ventilatory support [NIVS]) and swallow function according to the age of symptom onset.
Fifteen patients were prospectively followed at the Department of Neurology of FMUSP from 2019 to 2023, five of them had more than one evaluation in the period of 12 or 24 months. Their assessment included a standardized clinical protocol with a detailed clinical questionnaire, physical and neurological exam. Motor assessment scales were performed for 13 patients chosen according to the age of the patient and motor status: Chop Intend for < 2-year-old patients, Motor Function Measure 20 (MFM20) for patients 2–6 years old and MFM32 for patients > 6 years old. Chop Intend was also used for patients > 2 years old who were not able to sit independently. The muscle strength of the four limbs and neck was measured with Medical Research Council grading (MRC). The presence of ptosis, facial involvement, extraocular weakness, a high-arched palate, scoliosis, a rigid spine, and articular retraction were evaluated. Spirometry was performed for all patients aged > 6 years.
Genetic test and variant interpretation
Molecular studies were performed through commercial genetic panels whole exome sequencing (WES), and Sanger sequencing.The selection of the test was according to the availability for each center. Variants were annotated for the transcript TK2:ENST00000299697 using Ensembl Variant Effect Predictor (VEP)11and then filtered using custom R-scripts. Filtered variants were rare or absent in control population databases (gnomAD) and absent in homozygous individuals in controls. To detect if the variant was previously reported, literature and ClinVar were used. In silico predictors used were Polyphen and CADD for missense and Splice AI for splice-site variants12,13. Variants were classified according to the ACMG guidelines14.
Nucleosides replacement therapy
The supplementation therapy with deoxynucleosides (DThd and dCtd) is not available yet, however three patients were approved for a compassionate program by the sponsor and offered orally at a total dosage of 800 mg/kg/day10. They were evaluated through a clinical protocol to access motor and respiratory function, including a pre-dosing visit followed by one-, three-, six-, nine-, twelve-, and eighteen-month visits when applied. Blood tests for liver function and liver enzymes were performed at pre-dosing and three-month visits, then every six months.
Statistical analysis
R-packages were used for the statistical calculations. Continuous variables were presented as mean and standard deviation (SD) or median and interquartile range and discrete and categorical variables as counts and percentages. Univariate analyses were performed to calculate the prevalence and describe the characteristics of the patients. Odds ratio was calculated as a measure of association between the independent and dependent variables using contingency tables and the Mantel-Haenszel chi-square test. Additionally, 95% Confidence Interval (CI) and p value were calculated. All tests were 2-sided, and a p-value of 0.05 was considered as the threshold for significance. Missing data were handled individually. The denominator for each variable subtracted subjects for whom data were not available.
Results
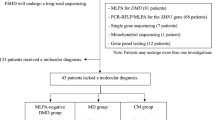
We identified 38 patients from 30 families presenting myopathy caused by biallelic pathogenic variants in the TK2 gene. Thirty-two patients agreed to participate in the clinical data collection. After consented, clinical and genetic information were obtained through chart review. Genetic information from four additional patients, which were part of a running clinical trial, were included after patient consent.
Clinical findings
Clinical findings (N = 32) were described in Table 1. There were 17 females and 15 males, with a mean age at evaluation of 17 (± 14) years old. Two patients indicated the disease was triggered by infection, and 18 patients (70%) indicated they became significantly worse during infection episodes. According to the age of onset, there were eight patients in the infantile-onset group, 19 patients in the childhood-onset group and five patients in the late-onset group.
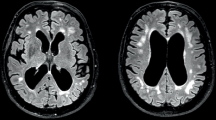
In the infantile-onset group, 6 patients presented motor delay, half of them were able to acquire gait, but one of those lost it at 2 months of disease duration (F7). All patients presented an aggressive disease. At a disease duration of 3.1 [± 6] years, 75% were bed-restricted, 90% needed ventilatory support, 90% were dysphagic, and 60% were feed by a gastrostomy tube (GT). Mortality rate was high in this group. 62% died with median disease duration of one year. The cause of death was ventilatory failure in all cases Extramuscular findings were found at 50% of patients. Hearing impairment was evaluated only at two patients, and both presented a normal study; two patients had neurogenic findings at EMG (SMA phenotype), two patients presented CNS involvement reported as encephalopathy and one patient presented with recurrent episodes with vomits and diarrhea nonrelated to infection. In the childhood-onset group (disease duration of 16 [± 13] years), 70% of patients were able to walk, but 35% of the patients lost gait 11 (+−9) years old. Thirteen patients (70%) needed NIVS, and one additional patient (5%) required IVS. Fourteen patients (80%) were dysphagic, and two of them had a feeding device. In addition, 70% were dysphonic and 85% referred exercise intolerance and 20% presented ophthalmoparesis. Three of them died of respiratory complications at ages of 4, 20, and 21 years old (median of 20 [± 12] years old). They presented an age of onset of 2.5, 4 and 5 years old respectively. Extramuscular involvement was also observed in the childhood-onset group. Hearing impairment was detected in four out of 10 patients that were investigated. Two siblings (P22.1 and P22.2) showed findings on EMG. Sensory and motor nerve conduction studies were within normal limits in both siblings, performed at ages 7 and 8, respectively. Electromyography revealed motor unit action potentials (MUAPs) with prolonged duration, increased amplitude, and a diffusely reduced interference pattern. Patient F22.2 showed signs of muscle membrane instability, including fibrillation potentials (FIBs) and positive sharp waves (PWs) in the lower limbs. Both patients presented with distal weakness as well as respiratory involvement. Additional two patients presented neurogenic findings. P17 had an SMA phenotype, EMG described on chart review as neurogenic, but no other details were provided and P18 had a muscle biopsy described as neurogenic, but no EMG was performed. One patient presented epilepsy, pain was reported by five (30%), and GI symptoms by 8 (50%) patients.
In the late-onset group (disease duration of 12 [± 11] years), four patients (80%) were able to walk, and one lost gait. This patient had an age of onset of 14 years old, developed with an aggressive disease, lost gait within 2 years of disease duration, and died at 18 years old due to respiratory insufficiency. One patient (20%) needed non-invasive ventilatory support. Three patients (60%) were dysphagic, and three (60%) were dysphonic. Two patients (40%) had ophthalmoparesis, they presented an age of onset of 35 and 31 years.
Motor assessment and natural history of the disease
Motor scales and spirometry were performed in 13 patients (Table 2). Eleven were evaluated with MFM32. They were 25 (± 14) years old and had a mean disease duration of 21 (± 15) years. The mean percentage of MFM32 was 60% (± 22) of the total score, 38% (± 18) at the first domain, 80% (± 12) at the second domain and 98% (± 2) at the third domain. Spirometry performed on the same day showed a mean FVC of 34% (± 11). Three patients had two visits at with a 24-month interval and two patients had two visits with a 12-month interval. All of them presented a decline in MFM32 and in the FVC Table 2.
Muscle histology and genetic analysis
The diagnosis was confirmed through genetic test for all patients. However, six patients underwent muscle biopsy prior to the genetic investigation. Five of them presented COX-negative, SDH-positive and ragged red fibers suggesting the mitochondrial dysfunction in addition to mild increased of connective tissue. However, there was not necrosis and increased of regenerating fibers. Depletion or multiple deletions in mtDNA were not evaluated. The histology was normal at one patient and neurogenic in another one, showing fiber-type grouping, increased fiber type variability and fibrosis.
Genetic information was available for all the 32 patients in the study and additional 4 patients from 2 families that were part of a clinical trial. Molecular studies were performed through an expanded neuromuscular panel (26 patients), WES (four patients), and Sanger sequencing (six patients). Of the four patients tested with WES, 2 of them were tested first with a neuropathy panel. Of the patients tested with commercial panels, two of them were tested first for SMA.
Twelve variants were found in the 36 patients (Table 3). Twenty-five patients had homozygous (HZ) variants, of those, six patients reported non-consanguineous parents, three of them referred they did not come from the same region, but no bioinformatic relatedness-inference was performed to gather more information about that. Eleven of the twelve presented variants that were previously reported in the literature or ClinVar and one was novel.
Four variants were recurrent, three of them were previously known in the literature (p.His121Asn, T108M, and p.Arg183Trp )1,2,15,16. p.His121Asn was detected in fifteen patients (13 families), ten were HZ and five were CH. P.Thr108Met was present in thirteen patients (nine families), ten were HZ and two were CH. Variant c.536_538 + 8del was found as CH with a pathogenic variant in four patients. This variant is predicted to delete a cryptic splice site, it is absent in population databases, it was not previously reported in literature, but it was reported in ClinVar (single submitter). No functional study was performed to confirm the effect of this variant. Three of the patients harboring c.536_538 + 8del patients had a severe infantile-onset presentation in addition to seizures. The fourth patient harbored c.536_538 + 8del in CH with p.Lys202del and had a late-onset phenotype. P.Arg183Trp was present in seven patients from four families. Of those families, neurogenic involvement was present in the two families on which we had data (P22.1, P22.2, P17). Patient P13 had an SMA-like phenotype, but no electrophysiology was performed. The remaining three patients had no EMG.
The novel variant (G91D) was in trans with a pathogenic variant in one patient. It is absent in population databases and located in a conserved residue. Different amino acid change at the same residue is reported as pathogenic. Therefore, it was classified as likely pathogenic.
Clinical findings from 10 HZ patients for p.His121Asn and 10 HZ for p.Thr108Met were compared (Table 4). Median age was 29 years old (± 10) for p.Thr108Met and 12 years old (± 10) for p.His121Asn. Age of onset was 7 (± 9) years old for p.Thr108Met and 4 (± 5) years old for p.His121Asn. Disease duration was 24 (± 13) years for p.Thr108Met and seven (± 9) years for p.His121Asn. Age that patients lost gait was 20 (± 10) years for p.Thr108Met and 8 (± 7) years for p.His121Asn. Age that patients started to use ventilatory support was 22 years for p.Thr108Met and 15 years for p.His121Asn. Dysphonia was reported in 90% of patients for p.Thr108Met and 30% of the patients for p.His121Asn. Ophthalmoparesis was reported only in p.Thr108Met -group.
Nucleosides replacement therapy
Three patients (F6, F8.1 and F9) were receiving nucleosides replacement therapy through a compassionate care program (Table 5). F6 and F8 started with weakness below the age of two. F6 started with difficulty to raise up from the floor. Patient progressed with gait lost, pronounced neck weakness, restrictive pulmonary dysfunction, dysphagia, weight lost and intestinal constipation at nine months after first symptoms. At pre-dosing visit, a pronounced hypotonia was noticed added to inability to sit unsupported, roll over and lift upper limbs. Patient was on continuous NIVS and being feed by G-tube exclusively. Data for one-year-follow up is presented in Table 5. At 12-month visit, Chop Intend increased from 20 to 60 points, patient was able to sit unsupported, lift upper limbs at elbows level and eat smooth food by mouth. Ventilation time decreased from 24 h/day to 15 h/day, in his last evaluation he was able to perform for the first time an spirometry showing 53% of FVC, and weight increased 6.5 kg in 18 months (30% of his total mass).
Patient F8.1 started with difficulty to stand from floor followed by neck weakness and gait lost. At the pre-dosing visit, a pronounced hypotonia was noticed added to inability to sit unsupported and roll over. Patient was presenting weight loss and NIVS was indicated due to night-time hypoventilation and recurrent pulmonary infections. Six-month follow up demonstrated an increase of MFM20 of 6 points, going from 31 (51.6%) to 33 (55%) at 3 months evaluation and 37 (61%) at 6-months evaluation, weight gain, and absence of pulmonary infection in the period.
Patient F9 noticed first symptoms after the age of five presenting knee pain and leg weakness. The disease progressed to difficulty to walk, stand from the floor, and jump. Pre-dosing revealed pronounced proximal and axial weakness, independent gait only for short distances, inability to climb steps, jump and lift arms above elbows. Night-time NIVS was initiated due to restrictive respiratory disturb. At six-months visit patient demonstrated more energy for daily activities and she had a six points-increase on MFM32 going from 68 (69%) to 71 (74%) at 3 months evaluation and 74 (77%) at 6-months evaluation. FVC increased from 40 to 55% at the 6-months visit.
Discussion
Biallelic variants in TK2 manifest primarily as progressive myopathy with mtDNA depletion. The non-specificity of symptoms in addition to a rapid progression and high mortality rates mainly among the infantile-onset presentations, makes this diagnosis particularly challenging. However, due to a potential treatment capable of changing the natural history of the disease4, the early recognition of this condition is urgent.
In this study, we described 32 patients in the largest non-Spanish cohort reported to date, focusing on extramuscular symptoms, genotype-phenotype correlation, and natural history of the disease. We also presented the description of three patients receiving nucleosides supplementation, highlighting the dramatic effect of the therapy in childhood-onset patients.
In this cohort, eight patients (30%) had infantile-onset (≤ 1year), 19 (53%) had childhood-onset (> 1 and < 12 years) and five (17%) presented late-onset (> 12 years)3,4. Like in the literature, the not-treated infantile-onset patients had a severe presentation and a very high mortality-rate (62% in the first year of the disease)3. Interestingly, patients with symptoms beginning between 1 and 2 years also had a severe and fast progressive disease, as we observed with F6, F8.1, and F25. They presented a disease pattern more similar to the infantile-onset than childhood-onset.
It’s important to emphasize that the childhood-onset group also had a debilitating and progressive disease. At the evaluation, when patients were 20 (± 13) years old, 70% used NIVS (starting at 21(± 7) years old) and 75% were dysphagic. Loss of ability to walk was reported by 30% of them and three patients died of ventilatory insufficiency during an infection episode at four, 20 and 21 years old (mortality rate of 15%). Eleven patients were evaluated using MFM32 which demonstrated a decreased performance mainly at domain 1 (60% of total performance and 37% of domain 1 performance) illustrating the severity of axial involvement of TK2d.
Extramuscular manifestations were described as rare. Brain, eyes, ears, heart, liver, and peripheral nerve can be affected, but there is no systematic study to evaluate the prevalence of these symptoms in this population3,7,17. In this cohort, 30% of patients presented at least one extramuscular symptom. Neurogenic involvement was pronounced in four patients leading the investigation towards this direction. A similar scenario was found with epilepsy. Three patients in the cohort had seizures and presented a very aggressive disease leading the investigation towards encephalopathies. TK2d should be investigated at all patients presenting a progressive myopathy. But we raise the importance of including TK2d in the differential diagnosis of inherited neuropathies, SMA, encephalopathies and epilepsy since these symptoms may overlap with the myopathic features and mislead the clinical investigation causing diagnostic delay as we demonstrated. Neurosensorial hearing loss is also described in TK2d18, however the prevalence of this symptom is not clear. In this cohort, two patients complained of hearing issues, and both had bilateral neurosensorial loss. Additional ten patients underwent a routine audiogram. Of those, four presented neurosensorial loss. Despite the lower sample size, we believe that hearing loss may be underestimated. In this sense, we recommend routinely investigation even at asymptomatic patients. Exercise intolerance, which is one of the most common symptoms in mitochondrial myopathy19,20, was reported by 85% of the patients, and worsening of symptoms during infection episodes was reported by 18 patients (70%).
Genotype-phenotype correlations reinforced some of the literature data and showed novel findings. We identified 12 variants among the 36 patients, ten of those were previously reported. Like the literature, the variant p.Arg130Trp was associated to a severe phenotype4,21and p.Lys202del, a common variant at the Spanish cohort was also associated to a milder late-onset presentation, at the only patient presenting this variant in this cohort. Interestingly, four variants were recurrent: p.Thr108Met (12 patients), p.His121Asn (14 patients), p.Arg183Trp (7 patients), and c.536_538 + 8del (4 patients). Clinical findings of HZ patients harboring p.Thr108Met were compared to HZ patients with p.His121Asn revealing a higher disease duration and milder presentation at p.Thr108Met group which goes in the same direction as the slower progression patients presented in a long-term follow up. Dysphonia and ophthalmoparesis were also more frequent in p.Thr108Met group. Both variants are also frequent in Spain5, but are present in other populations. Variant c.536_538 + 8del was reported only by one submitter in ClinVar with no clinical data, and it was found at homozygous state in one patient and in trans with a pathogenic variant in additional three patients. Therefore, it was classified as likely pathogenic according to ACMG criteria, however a functional study would be ideal to clarify the impact at protein level. Of those patients, three of them had a severe phenotype including seizures suggesting it might be associated with central involvement. Seven patients (4 families) harbored the variant p.Arg183Trp. Three of them had neurogenic findings at neuroconduction studies. We speculated that this variant might be associated with peripheral nerve involvement adding novel insights into genotype-phenotype correlations.
Despite being more aggressive in the infantile-onset group, the disease is clearly progressive at all groups. Five patients were evaluated more than once at 24-month interval and their follow-up showed a discrete worsening at motor and respiratory function, in addition to the patient perception.
In the opposite direction, the improvement of the three patients receiving the nucleoside reposition was evident, as already suggested in the literature4,10,22. At 9 months therapy follow-up all of them presented a significant improvement at motor, respiratory and bulbar function in addition to weight gain (Table 5). Patients also referred that they were more active, happier, and felt more energy.
In conclusion, we presented one of the largest cohorts of novel patients presenting TK2d and the historical Iberic inheritance might not be a clear explanation behind the high number os patients detected. In this population most of the patients presented infantile- and childhood-onset disease, in contrast to the late-onset predominance in Spanish cohort. Also, variant p.Lys202del, which is frequent in Spain, appeared in only one individual in this cohort. Despite the fact that some of the most recurrent variants we found, were also find in other populations, some of them seemed to be more common in Brazil such as p.Arg183Trp and c.536_538 + 8del adding valuable genotypic information regarding this population.
This study had several limitations. Retrospective cohorts relying on chart review are usually challenging and the analysis needed to take in account all the missing data we had. However, it made it possible to show data of a large cohort of a super rare disease. A long and structured natural history would be important for gathering data regarding the progression of the disease, but this is disrupted by the fact of a known treatment that might be available and benefit the patients when they are progressing. The possible access to a disease modifier treatment makes an early diagnosis of TK2d urgent, which could be facilitated with a phenotype awareness for a progressive myopathy with high CK, and also with the inclusion of the TK2 gene in the differential diagnosis guidelines for neuropathy, epilepsy, and encephalopathy attempting to increase the clinical suspicion for TK2d and then, accelerate the diagnostic rates for this condition.
Data availability
Data is provided within the manuscript or supplementary information files. The submission number for each variant is placed in the deposit data as a supplementary data.
References
Saada, A. et al. Mutant mitochondrial thymidine kinase in mitochondrial DNA depletion myopathy. Nat. Genet. 29 (3), 342–344 (2001).
Mancuso, M. et al. Mitochondrial DNA depletion: mutations in thymidine kinase gene with myopathy and SMA. Neurology 59 (8), 1197–1202 (2002).
Garone, C. et al. Retrospective natural history of thymidine kinase 2 deficiency. J. Med. Genet. 55 (8), 515–521 (2018).
Berardo, A. et al. Advances in thymidine kinase 2 Deficiency: clinical aspects, translational progress, and emerging therapies. J. Neuromuscul. Dis. 9 (2), 225–235 (2022).
Ceballos, F. et al. Clinical and genetic analysis of patients with TK2 Deficiency. Neurol. Genet. 10 (2), e200138 (2024).
Domínguez-González, C. et al. Late-onset thymidine kinase 2 deficiency: a review of 18 cases. Orphanet J. Rare Dis. 14 (1), 100 (2019).
Wang, J. et al. Clinical and molecular spectrum of thymidine kinase 2-related mtDNA maintenance defect. Mol. Genet. Metab. 124 (2), 124–130 (2018).
Laine-Menéndez, S. et al. Preferent diaphragmatic involvement in TK2 Deficiency: an autopsy case study. Int. J. Mol. Sci., 22(11):5598 (2021).
Garone, C. et al. Deoxypyrimidine monophosphate bypass therapy for thymidine kinase 2 deficiency. EMBO Mol. Med. 6 (8), 1016–1027 (2014).
Domínguez-González, C. et al. Deoxynucleoside therapy for thymidine kinase 2-Deficient myopathy. Ann. Neurol. 86 (2), 293–303 (2019).
McLaren, W. et al. The Ensembl variant effect predictor. Genome Biol. 17 (1), 122 (2016).
Rentzsch, P. et al. CADD: predicting the deleteriousness of variants throughout the human genome. Nucleic Acids Res. 47 (D1), D886–D894 (2019).
Jaganathan, K. et al. Predicting Splicing from primary sequence with deep learning. Cell 176 (3), 535–548e24 (2019).
Richards, S. et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 17 (5), 405–424 (2015).
Tulinius, M. et al. Novel mutations in the thymidine kinase 2 gene (TK2) associated with fatal mitochondrial myopathy and mitochondrial DNA depletion. Neuromuscul. Disord. 15 (6), 412–415 (2005).
Hu, C. et al. Clinical Profile and Outcome of Pediatric mitochondrial myopathy in China. Front. Neurol. 11, 1000 (2020).
Knierim, E. et al. Clinical application of whole exome sequencing reveals a novel compound heterozygous TK2-mutation in two brothers with rapidly progressive combined muscle-brain atrophy, axonal neuropathy, and status epilepticus. Mitochondrion 20, 1–6 (2015).
Martí, R. et al. Hearing loss in a patient with the myopathic form of mitochondrial DNA depletion syndrome and a novel mutation in the TK2 gene. Pediatr. Res. 68 (2), 151–154 (2010).
Ahuja, A. S. Understanding mitochondrial myopathies: a review. PeerJ 6, e4790 (2018).
de Hoz, F. F. Recurrent rhabdomyolysis and exercise intolerance: a new phenotype of late-onset thymidine kinase 2 deficiency. Mol. Genet. Metab. Rep. 26, 100701 (2021).
Lesko, N. et al. Two novel mutations in thymidine kinase-2 cause early onset fatal encephalomyopathy and severe mtDNA depletion. Neuromuscul. Disord. 20 (3), 198–203 (2010).
Dombi, E. et al. Nucleoside supplements as treatments for mitochondrial DNA depletion syndrome. Front. Cell. Dev. Biol. 12, 1260496 (2024).
Acknowledgements
PJT was supported by an MRC strategic award to establish an International Centre for Genomic Medicine in Neuromuscular Diseases (ICGNMD MR/S005021/1.
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Contributions
C.A.M.M., A.T.Q.S.M.F., A.M.S.S., M.A.P., F.T.P., A.L.S.P., V.L.L.B, T.C.M., E.P.E., M.P.M., A.P.P.C.M., V.V.L., P.J.T., R.S., J.G.G., L.M.F.S., T.M.O., R.H.M., E.L.S., M.M.C., C.W.P.J., W.M.J., C.F.R.S., A.S.B.O., F.K., M.H., A.N. contributed with data collection. C.A.M.M., C.G.C, D.S., E.Z. wrote the main manuscript text, designed the study. and prepared figure and tables. M.C.A., T.R.F. contributed with data collection and motor assessments. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics Declarations
The authors disclose that the study have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
The authors declare that informed consent was obtained from all subjects and/or their legal guardian(s). The authors declare that this work has not been published before.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Moreno, C.A.M., Artilheiro, M.C., Fonseca, A.T.Q.S.M. et al. Clinical and molecular spectrum of TK2-deficiency: a large Brazilian cohort. Sci Rep 15, 9013 (2025). https://doi.org/10.1038/s41598-024-84373-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84373-5
