
Abstract
Postoperative delirium has the potential to impact individuals of all age groups, with a significant emphasis on the elderly population. Its presence leads to an increase in surgical morbidity and mortality rates, as well as a notable prolongation of hospital stays. However, there is a lack of research regarding the prevalence, risk factors, and implications of postoperative delirium in developing nations like Ethiopia, which affects both patients and healthcare institutions. An observational study was conducted at hospitals in the South Gondar Zone to diagnose postoperative delirium in the Post-Anesthesia Care Unit (PACU) using the Nursing Delirium Screening Scale. Both bivariable and multivariable logistic regression techniques were employed to analyze the association between independent factors and postoperative delirium. The strength of the association was indicated by the odds ratio with a 95% confidence interval (CI). Any p-values below 0.05 were considered statistically significant. The incidence of postoperative delirium was determined to be 41%. In the multivariate logistic regression analysis, several factors were identified as significantly associated with postoperative delirium. These factors include an age of 75 or older (AOR, 11.24; 95% CI, 4.74–26.65), ASA-PS IV (AOR, 3.25; 95% CI, 1.81–5.85), severe functional impairment of activities of daily living (AOR, 3.29; 95% CI, 1.06–10.20), premedication with benzodiazepine (AOR, 4.61; 95% CI, 2.48–8.57), intraoperative estimated blood loss exceeding 1000 ml (AOR, 2.74; 95% CI, 1.50–4.98), and intraoperative ketamine use (AOR, 3.84; 95% CI, 2.21–6.68). Additionally, postoperative delirium was found to significantly prolong the duration of stay in the post-anesthesia care unit (PACU) and the length of hospital stay (p-value < 0.05). Patients aged 75 or older, ASA-PS IV, experiencing severe functional impairment of ADL, patients premedicated with benzodiazepine, patients with intraoperative estimated blood loss exceeding 1000 ml, and intraoperative ketamine use were identified as risk factors for post-operative delirium.
Similar content being viewed by others

Introduction
The current DSM-IV definition of delirium characterizes it as an acute confusional state marked by fluctuating mental status, reduced ability to focus (inattention), disturbances in the level of consciousness, changes in cognition, and perceptual disturbances1. In neo-Latin languages, it is referred to as an acute confusional state2,3.
Postoperative delirium can occur in patients of any age, although it is more commonly observed in older patients. It can lead to longer hospital stays and increased costs due to delayed recovery from anesthesia. The incidence of postoperative delirium varies based on factors such as the type and sensitivity of the delirium assessment used, as well as the type and urgency of the procedure4. Reported rates range from 9 to 87%5. Postoperative delirium is the most frequently reported complication in elderly surgical patients, with incidence rates ranging from 5 to 50% in the postoperative period6,7. In the United States, more than one-third of all surgeries are performed on elderly patients, highlighting the importance for healthcare workers to understand the optimal care for delirium8.
Postoperative delirium may arise from various factors, including neuro-inflammation, neurotransmitter imbalances, pain, infection, metabolic abnormalities, and sleep disturbances9,10,11,12. Key predisposing factors for postoperative delirium include poor preoperative cognitive function, advanced age, and a history of alcohol or substance abuse13. Although most patients eventually recover from postoperative delirium, studies have shown that episodes of delirium are associated with long-term cognitive decline14.
Research findings have shown that approximately 30 to 40% of cases of postoperative delirium are preventable15. Multimodal strategies have been employed to reduce the incidence of postoperative delirium. While pharmacologic interventions for the treatment of active delirium have been extensively studied, most studies have failed to identify effective drugs. A systematic review found that antipsychotic medications did not significantly affect the incidence, duration, severity, or length of hospital stay related to delirium16. A clinical trial by Agar et al. showed that the placebo group had improved survival and reduced delirium severity scores compared to those treated with risperidone and haloperidol17. Furthermore, dexmedetomidine has been associated with a reduction in postoperative delirium18,19.
Non-pharmacologic interventions, such as training on delirium for medical staff, have been shown to reduce the duration of delirium, hospital length of stay, and mortality. These programs also enhance delirium recognition and management and are associated with reductions in point prevalence20,21. A study conducted in Shanghai, China, among elderly patients with lung cancer in the intensive care unit found that the postoperative blood oxygen levels, preoperative cognitive scores, and postoperative sleep quality scores in the delirium group were significantly lower than those in the non-delirium group22.
Postoperative delirium is a common complication, particularly among elderly patients, and can lead to several adverse postoperative outcomes, including prolonged hospital stays, increased healthcare costs, extended ICU stays, and higher morbidity and mortality rates23,24,25,26. However, research on the incidence, duration, and risk factors of postoperative delirium is limited in Ethiopia, especially in the study area. Identifying these risk factors is crucial for implementing strategies to reduce the occurrence, severity, and associated adverse outcomes of delirium. This study aims to provide valuable data on the incidence of postoperative delirium and its associated factors at the time of patient transfer to the ward among elderly patients. The findings may contribute to the existing body of knowledge and serve as baseline data for future research in Ethiopia.
Objectives
Main objective
To determine the prevalence and risk factors for postoperative delirium among elderly surgical patients in south Gondar zone hospitals in 2023.
Specific objectives
To determine the prevalence of postoperative delirium among elderly surgical patients.
To identify variables associated with postoperative delirium in elderly surgical patients.
To evaluate the postoperative impact of delirium on elderly surgical patients.
Methods and materials
Study design, period and setting
A cross-sectional study was conducted at hospitals in the South Gondar Zone, Ethiopia, from January 1st to November 30th, 2023. The South Gondar Zone is one of the ten administrative zones in the Amhara Regional State. According to Ethiopia’s 2021 statistical report, the South Gondar Zone has a total population of 2,631,566, with 1,331,888 males and 1,299,678 females27. The zone is served by eight government hospitals, including seven primary hospitals and one comprehensive specialized hospital. These hospitals are Nefas Mewucha Primary Hospital (NMPH) in Lay Gaynt Woreda, Wogeda Primary Hospital (WPH) in Simada Woreda, Ebinat Primary Hospital (EPH) in Ebinat Woreda, Mekane Eyesus Primary Hospital (MEPH) in Estie Woreda, Andabet Primary Hospital (APH) in Andabet Woreda, Debre Tabor Comprehensive Specialized Hospital (DTCSH) in Debre Tabor, Dr. Ambachew Memorial Hospital (Dr. AMH) in Tach Gaynt Woreda, and Addis Zemen Primary Hospital (AZPH) in Libokemkem Woreda.
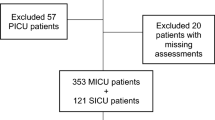
For this study, three institutions (DTCSH, AZPH, and NMPH) were selected, and an average of 57 elderly patients underwent surgery (Fig. 1). After collecting the data, the study was registered with the title on Research Registry, using the unique registration number researchregistry10049.

Schematic presentation for the incidence and risk factors of postoperative delirium in elderly surgical patients in South Gondar Zone hospitals, 2023 (n = 424).
Inclusion/exclusion criteria
Patients above the age of 65 years and who were scheduled for elective surgery9,28 were included in the study. However, elderly patients with severe pulmonary disease or severe cardiac disease, as well as those who were unable to perform cognitive and psychometric tests due to reasons such as sensory impairment, language disorders, or a previous diagnosis of dementia9,28 were excluded from the study.
Sampling size and technique
Since there were no similar studies conducted in Ethiopia, the proportion of postoperative delirium was taken as 50%, with a 95% confidence interval and a margin of error of 0.05. The sample size was determined using the following formula for a single population proportion.
Whereas n represents the sample size, Z represents the confidence interval (1.96), P represents the prevalence (0.5), and d represents the margin of sampling error to be tolerated (0.05), the goal is to determine the sample size with a confidence interval of 95% and a margin of error of 5%.
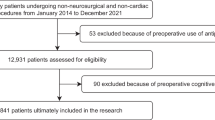
n= (1.96)2 * 0.5(1- 0.5)/ (0.05)2 = 385, and by adding a 10% non-response rate the final sample size was 424. Consecutive sampling technique was used in which every study participant meeting the inclusion criteria was selected until the required sample size was achieved. The daily operation schedule list in each hospital was used as a sampling frame. The situational analysis showed that an average of 40, 10, and 7 elderly patients who meet the inclusion criteria were operated on Debre Tabor Comprehensive Specialized Hospital, Addis Zemen Primary Hospital, and Nefas Mewucha Primary Hospital respectively per month. According to this data, the calculated sample size was proportionally allocated for each hospital (DTCSH = 298, AZPH = 74, NMPH = 52) during the study period.
Dependent variable
Postoperative delirium (Yes/No).
Independent variables
Demographic variables: Age, sex, BMI, history of smoking and alcohol consumption, presence of comorbid disease (medical conditions that are simultaneously present with the surgical condition they already present with in the patient), activities of daily living, presence of preoperative cognitive impairment using Short Portable Mental Status Questionnaire (SPMSQ) score, preoperative anxiety.
Preoperative variables: Premedication (benzodiazepines, hypnotics, narcotic drugs), ASA status, serum electrolytes, creatinine, glycaemia, etc.
Intraoperative and postoperative variables: Surgical specialty, duration of surgery, type of anesthesia, induction agent, use of anticholinergic, IV opioids used, duration of anesthesia, presence of hypotension, intraoperative blood loss, perioperative blood transfusions, postoperative analgesics used, stay duration in PACU, duration of hospital stay, and admission to ICU.
Operational definitions
Elderly: A chronological age of 65 years old or older, while those from 65 to 74 years old are referred to as “early elderly” and those over 75 years old as “late elderly”29.
Activities of Daily Living: The Katz Index of Independence in Activities of Daily Living is the most appropriate instrument to assess the functional status of the elderly. The Index ranks adequacy of performance in functions of bathing, dressing, toileting, transferring, continence, and feeding. Each function is scored as yes/no for independence functions. A score of 6 indicates full function, 4 indicates moderate impairment, and 2 or less indicates severe functional impairment30.
Preoperative dementia: The Short Portable Mental Status Questionnaire (SPMSQ) Scoring of > 2 errors suggests cognitive impairment31. The Short Portable Mental Status Questionnaire (SPMSQ) asks for the following information: date of birth, age in years, and time to the nearest hour, year, name of the hospital or home address, and the ability to recognize two people. What the year before will be: Enter the patient’s grandfather’s name and count backwards from 20 to 1 (no errors or suggestions permitted). On a scale of 1 to 10, a score less than 7 indicates’ cognitive impairment.
Preoperative anxiety: Preoperative anxiety was assessed using the six-item State-Trait Anxiety Inventory measure. The total of all six scores was multiplied by 20/6. Patients with a score of 20 have no anxiety, while those with a score of 80 have a significant level of worry. A score of 44 and above was considered to indicate clinically severe anxiety32.
The State-Trait Anxiety Inventory consists of negative items (I feel tense, I feel upset, I feel worried), and positive items (I feel calm, I feel relaxed, I feel content). Each item was scored as follows: 1 = Not at all, 2 = Somewhat, 3 = Moderately, 4 = Very much32 .
Postoperative delirium: In our research, we utilized the NU-DESC scale to assess delirium in postoperative patients. The NU-DESC scale comprises five parameters: disorientation, inappropriate behavior, inappropriate communication, illusions/hallucinations, and psychomotor retardation. Each parameter is assigned a sub-score ranging from 0 to 2 points, where 0 indicates the absence of symptoms, 1 represents mild symptoms, and 2 corresponds to severe symptoms. A total score of ≥ 2 points is indicative of postoperative delirium33.
Data collection procedure
The questionnaire consists of two sections: Section 1 consists of demographic and patient-related preoperative data, and Section 2 consists of anesthesia and surgery-related intraoperative data. Section 3 consists of post-operative data such as the duration of surgery/anesthesia, stay duration in the PACU, and length of hospital stay.
Patient history was taken to document pertinent patient demographics and health habits. Functional autonomy was assessed using the basic Activities of Daily Living34. Data for Activities of Daily Living were obtained from the patient or from a close relative or caregiver. Cognitive status was measured using the ten-item Short Portable Mental Status Questionnaire (SPMSQ), which is a brief, easy-to-administer tool that does not require specific training for administration and scoring31, It is a reliable and valid tool35. Consecutive patients in the PACU were prospectively evaluated for the presence of delirium. The nursing staff of the PACU will record the Nu-DESC. The presence of delirium was determined using the Nursing Delirium Scale score36. PACU delirium was assessed by obtaining a Nu-DESC score during transfer to the inpatient ward at the end of their PACU stay when deemed ready to be transferred to the surgical inpatient ward. Content validity and reliability have been established33,37,38.
Data quality assurance
A pretest was conducted on 5% of the study participants (21 patients) at Felege Hiwot Comprehensive Specialized Hospital. Nurses working in the Post-Anesthesia Care Unit (PACU) were trained on both the Nu-DESC tool and the clinical significance of delirium before conducting delirium screenings on the patients. Throughout the data collection period, repeated PACU visits were made to provide assistance with any questions related to the delirium assessments.
Data analysis and interpretation
The data was coded and entered into STATA version 17 after being cleaned and checked for completeness. Descriptive statistics, including percentages, frequency distributions, and measures of central tendency, were calculated. Independent variables were initially analyzed using binary logistic regression, with postoperative delirium as the dependent variable. Variables with a p-value of ≤ 0.2 from the bivariate analysis were then included in a multivariable logistic regression model to assess their association with postoperative delirium. Odds ratios with 95% confidence intervals and p-values were computed to identify factors associated with postoperative delirium. A p-value of < 0.05 was considered statistically significant.
Results
Socio demographics and preoperative characteristics of the study participant
A total of 424 surgical patients aged 65 and older participated in this study, with more than half (234, 55.2%) being male. The majority of participants (82.8%) were under the age of 75. In terms of activities of daily living, more than half (231, 54.5%) had full function, 150 (35.4%) exhibited moderate impairment, and 43 (10.1%) had severe impairment. Regarding lifestyle factors, 67 (15.8%) of the participants had a history of smoking, and 69 (16.3%) had a history of alcohol or substance overuse. Preoperative anxiety was observed in 121 patients (28.5%), while 303 (71.5%) did not exhibit preoperative anxiety (Table 1).
Anesthesia and surgery related intraoperative characteristics of the study participants
Preoperative premedication patterns for research participants showed that 218 (51.4%) had premedicated with opioids, and 97 (22.9%) had premedicated with benzodiazepines (Table 2). Out of the 424 participants, 59.4% came for elective surgery, and the other individuals were hospitalized for emergency surgery. Merely 53 (12.5%) out of the participants had a history of preoperative blood transfusion.
The incidence of postoperative delirium and factors associated with it
Of the 424 elderly surgical patients in this study, 41% experienced postoperative delirium. Multivariate analysis revealed that the following factors were significantly associated with the development of delirium: age ≥ 75 years, ASA III status, severe impairment in activities of daily living, preoperative administration of ketamine or benzodiazepines, estimated blood loss exceeding 1000 mL, longer surgery duration, extended PACU stay, and prolonged hospital stay. However, no significant associations were found between postoperative delirium and factors such as opioid use, ASA IV status, anesthesia duration, or moderate impairment in daily living activities.
Post-operative characteristics of study participant
Looking at the postoperative characteristics patient stay duration in PACU and patient hospital stay is significantly associated with the occurrence of postoperative delirium (Table 4).
Discussion
Postoperative delirium is characterized by a sudden disruption in attention and cognition, separate from neurocognitive disorders. It is characterized by difficulty maintaining focus or shift in attention, as well as cognitive disturbances such as memory impairment, disorientation, and hallucinations or illusions39,40,41. According to this study, the prevalence of postoperative delirium among elderly surgical patients is 41%. This is consistent with findings from studies conducted at the Denver Veteran Affairs Medical Center (43–44%) and the University of California, San Francisco (46%)25,42,43. This could be attributed to the use of a similar assessment tool for the primary outcome of the study.
The incidence of postoperative delirium in elderly surgical patients observed in this study is significantly higher than the prevalence reported in a study conducted at Yamaguchi University Graduate School of Medicine in Japan (25%), in Cleveland, USA (11.4%), and at Marmara University Hospital, Istanbul, Turkey (5.32%). This high prevalence of postoperative delirium in this study area could be attributed to a lack of awareness of the issue and the absence of a postoperative delirium management guideline in the study area26,44,45. On the other hand, the prevalence of postoperative delirium in elderly surgical patients found in this study was low compared to a study conducted in the United States of America (71%)46. The lower prevalence observed in our research area may be due to differences in the definition of the problem and the methods used to assess it.
Several studies have revealed many potential factors related to the development of postoperative delirium in elderly surgical patients. According to the findings of this study, age greater than or equal to 75, ASA status of the patient (ASA III), severe impairment in daily living activities, ketamine premedication, benzodiazepine premedication, estimated blood loss greater than 1000 ml, and duration of surgery were associated factors for the development of postoperative delirium among elderly surgical patients. Moreover, according to the results of the student t-test, postoperative delirium was related to a lengthy stay in the PACU and in the hospital overall (Tables 3, 4). Age ≥ 75 was significantly associated with the prevalence of postoperative delirium in this study. It was 11.24 times more likely to cause postoperative delirium when compared to patients with an age of less than 75 (AOR 11.24 with 95% CI (4.74, 26.65)). This finding is supported by a prospective controlled study done in Amsterdam, a study done at Yamaguchi, and a study done at the University of California, San Francisco43,45,47.
The American Society of Anesthesiology (ASA) status of the patient was significantly associated with the prevalence of postoperative delirium. Compared to ASA II patients, ASA III patients were found to have AOR of 3.25 with a 95% CI of (1.81, 5.85). This finding is also supported by a study conducted in the Netherlands, which found that ASA ≥ 3 was associated with the prevalence of postoperative delirium48. The observation that only ASA 3 was related to delirium in our study, while ASA 4 was not, may be due to the small number of participants classified as ASA 4; typically, patients with ASA 4 and above have communication difficulties. Additionally, preoperative functional impairment has been demonstrated to have a substantial correlation with postoperative delirium; patients with severe preoperative impairment in their daily activities are 3.29 times more likely to experience postoperative delirium than patients who are fully functional. Research from California and Indiana supports this finding49.
This study showed that benzodiazepine premedication is significantly associated with the occurrence of postoperative delirium, with an AOR of 4.61 (95% CI 2.48, 8.57). This finding is supported by research done in Addis Ababa, Ethiopia23. This is contradictory to the fact that benzodiazepines were regularly given to reduce perioperative anxiety, which reduces postoperative delirium, as seen in the other research18,19,21. This result could be secondary to the paradoxical effects of BZDs, effects such as irritability, aggressiveness, and confusion that especially result from repeated doses.
Despite there is some previous studies which state ketamine prevent postoperative delirium by reducing pain and opioid consumption this study showed that ketamine premedication is found to be significantly associated with the occurrence of postoperative delirium with AOR (3.84 and CI (2.21, 6.68)). This result is supported by systematic reviews done on the relation of ketamine with postoperative delirium50. This finding is attributed to the deleterious effect of ketamine by increasing the incidence of postoperative nightmares and hallucinations.
Excessive bleeding is significantly associated with the occurrence of postoperative delirium. Patients with an estimated blood loss of 1000 ml or more were found to be 2.7 times more likely to develop postoperative delirium (AOR 2.74, 95% CI: 1.50, 4.98) compared to those with an estimated blood loss of less than 1000 ml. This finding is consistent with research conducted in Addis Ababa, Ethiopia23. While some studies suggest that blood transfusions contribute to postoperative delirium, they do not directly link excessive bleeding to its development23,51,52. This result may be attributed to cerebral hypotension caused by excessive bleeding, which is believed to increase the risk of delirium.
A long duration of surgery was found to be significantly associated with the prevalence of postoperative delirium. This finding is supported by studies conducted in Addis Ababa, Ethiopia; Chongqing, China; Colorado, USA; and at Shanghai Jiao Tong University23,42,51,53. A prolonged duration of surgery may lead to significant blood loss and the exposure to multiple medications, both of which can contribute to the development of postoperative delirium.
The results of this study indicate that the prevalence of postoperative delirium is significantly associated with prolonged stays in both the PACU and the hospital. This finding is consistent with studies conducted at Harvard Medical School in Boston and in Addis Ababa, Ethiopia23,24. This may be attributed to the fact that delirium often causes patients to become resistant to following medical team instructions, leading to increased medication consumption and exposing them to more adverse effects than non-delirious patients. The delay in hospital discharge due to delirium also increases the demand for medical resources, exposes patients to a higher risk of hospital-acquired infections, and exacerbates the financial burden on patients23,24.
Conclusions
The incidence of postoperative delirium was found to be high. Risk factors identified for postoperative delirium include being aged 75 or older, having an ASA classification of III, severe functional impairment of ADL, premedication with benzodiazepines, intraoperative estimated blood loss greater than 1000 ml, and intraoperative ketamine use. The development of postoperative delirium was found to be significantly associated with prolonged stays in the PACU and hospital.
Limitation
The limitations of the study include the small sample size and the lack of a heterogeneous research population.
Data availability
The corresponding author will provide the datasets used in this study upon reasonable request.
Abbreviations
- ADL:
-
Activity of Daily Life
- AOR:
-
Adjusted Odds Ratio
- ASA:
-
American Society of Anesthesiologists
- COR:
-
Crude Odds Ratio
- Nu-DESC:
-
Nursing Delirium Screening Scale
- PACU:
-
Post Anesthesia Care Unit
- SPMSQ:
-
Short Portable Mental Status Questionnaire
References
Alexander, S. K. & Needham, E. Diagnosis of delirium: A practical approach. Pract. Neurol. 23(3), 192–199 (2023).
Whitlock, E. L., Vannucci, A. & Avidan, M. S. Postoperative delirium. Minerva Anestesiol. 77(4), 448 (2011).
Trabold, B. & Metterlein, T. Postoperative delirium: Risk factors, prevention, and treatment. J. Cardiothorac. Vasc. Anesth. 28(5), 1352–1360 (2014).
Rudolph, J. L. & Marcantonio, E. R. Postoperative delirium: Acute change with long-term implications. Anesth. Analg. 112(5), 1202 (2011).
Demeure, M. J. & Fain, M. J. The elderly surgical patient and postoperative delirium. J. Am. Coll. Surg. 203(5), 752–757 (2006).
Dasgupta, M. & Dumbrell, A. C. Preoperative risk assessment for delirium after noncardiac surgery: A systematic review. J. Am. Geriatr. Soc. 54(10), 1578–1589 (2006).
Marcantonio, E. R. Postoperative delirium: A 76-year-old woman with delirium following surgery. Jama 308(1), 73–81 (2012).
DeFrances, C. J., Golosinskiy, A., Hall, M. J., Schwartzman, A. & Williams, S. N. National hospital discharge survey; 2007 summary (2010).
Chaput, A. J. & Bryson, G. L. Postoperative delirium: Risk factors and management: Continuing professional development. Can. J. Anesth. J. Can. d’anesth. 59(3), 304–320 (2012).
Skrobik, Y. Delirium prevention and treatment. Crit. Care Clin. 25(3), 585–591 (2009). x.
Zhang, H. et al. Strategies for prevention of postoperative delirium: A systematic review and meta-analysis of randomized trials. Crit. Care 17(2), 1–21 (2013).
Vlisides, P. & Avidan, M. Recent advances in preventing and managing postoperative delirium. F1000Research 1(8), 1–10 (2019).
Kat, M. G. et al. Long-term cognitive outcome of delirium in elderly hip surgery patients. Dement. Geriatr. Cogn. Disord. 26(1), 1–8 (2008).
Inouye, S. K., Westendorp, R. G. & Saczynski, J. S. Delirium in elderly people. Lancet 383(9920), 911–922 (2014).
Siddiqi, N., House, A. O. & Holmes, J. D. Occurrence and outcome of delirium in medical in-patients: A systematic literature review. Age Ageing 35(4), 350–364 (2006).
Neufeld, K. J., Yue, J., Robinson, T. N., Inouye, S. K. & Needham, D. M. Antipsychotic medication for prevention and treatment of delirium in hospitalized adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 64(4), 705–714 (2016).
Agar, M. R. et al. Efficacy of oral risperidone, haloperidol, or placebo for symptoms of delirium among patients in palliative care: A randomized clinical trial. JAMA Intern. Med. 177(1), 34–42 (2017).
Pasin, L. et al. Dexmedetomidine reduces the risk of delirium, agitation and confusion in critically ill patients: A meta-analysis of randomized controlled trials. J. Cardiothorac. Vasc. Anesth. 28(6), 1459–1466 (2014).
Duan, X. et al. Efficacy of perioperative dexmedetomidine on postoperative delirium: Systematic review and meta-analysis with trial sequential analysis of randomised controlled trials. Br. J. Anaesth. 121(2), 384–397 (2018).
Lundström, M. et al. A multifactorial intervention program reduces the duration of delirium, length of hospitalization, and mortality in delirious patients. J. Am. Geriatr. Soc. 53(4), 622–628 (2005).
Tabet, N. et al. An educational intervention can prevent delirium on acute medical wards. Age Ageing 34(2), 152–156 (2005).
Lu, Y. & Liu, X. Postoperative delirium and its influencing factors in elderly patients with lung cancer in the intensive care unit. J. Thorac. Disease 15(2), 701–710 (2023).
Assefa, S. & Sahile, W. A. Assessment of magnitude and associated factors of emergence delirium in the post anesthesia care unit at Tikur Anbesa Specialized Hospital, Ethiopia. Ethiop. J. Health Sci. 29(5), 597–604 (2019).
Gleason, L. J. et al. Effect of delirium and other major complications on outcomes after elective surgery in older adults. JAMA Surg. 150(12), 1134–1140 (2015).
Robinson, T. N. et al. Postoperative delirium in the elderly: Risk factors and outcomes. Ann. Surg. 249(1), 173–178 (2009).
Yildizeli, B. et al. Factors associated with postoperative delirium after thoracic surgery. Ann. Thorac. Surg. 79(3), 1004–1009 (2005).
service Es. Population Size of Towns by Sex, Region, Zone and Weredas 2021.
Ansaloni, L. et al. Risk factors and incidence of postoperative delirium in elderly patients after elective and emergency surgery. Br. J. Surg. 97(2), 273–280 (2010).
Orimo, H. et al. Reviewing the definition of elderly. Geriatr. Gerontol. Int. 6(3), 149–158 (2006).
Wallace, M. & Shelkey, M. Katz index of independence in activities of daily living (ADL). Urol. Nurs. 27(1), 93–94 (2007).
Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 23(10), 433–441 (1975).
Vergara-Romero, M. et al. Validation of the Spanish version of the Amsterdam preoperative anxiety and information scale (APAIS). Health Qual. Life Outcomes 15(1), 1–10 (2017).
Gaudreau, J-D., Gagnon, P., Harel, F., Tremblay, A. & Roy, M-A. Fast, systematic, and continuous delirium assessment in hospitalized patients: The nursing delirium screening scale. J. Pain Symptom Manag. 29(4), 368–375 (2005).
Katz, S., Downs, T. D., Cash, H. R. & Grotz, R. C. Progress in development of the index of ADL. Gerontologist 10(1_Part_1), 20–30 (1970).
Roccaforte, W. H., Burke, W. J., Bayer, B. L. & Wengel, S. P. Reliability and validity of the short portable mental status questionnaire administered by telephone. J. Geriatr. Psychiatr. Neurol. 7(1), 33–38 (1994).
Inouye, S. K., Director, A. B. C. & Life, H. S. The short confusion Assessment Method (short CAM): Training manual and coding guide. Intern. Med. 113, 941–948 (1990).
Radtke, F. et al. Comparison of three scores to screen for delirium in the recovery room. Br. J. Anaesth. 101(3), 338–343 (2008).
Wang, J. et al. Risk factors contributing to postoperative delirium in geriatric patients postorthopedic surgery. Asia-Pacific Psychiatry. 7(4), 375–382 (2015).
Rengel, K. F., Pandharipande, P. P. & Hughes, C. G. Postoperative delirium. La. Presse Médicale 47(4), e53–e64 (2018).
Sharma, P. T. et al. Recovery room delirium predicts postoperative delirium after hip-fracture repair. Anesth. Analgesia 101(4), 1215–1220 (2005).
Hughes, C. G. et al. Surgery and anesthesia exposure is not a risk factor for cognitive impairment after major noncardiac surgery and critical illness. Ann. Surg. 265(6), 1126 (2017).
Robinson, T. N., Raeburn, C. D., Tran, Z. V., Brenner, L. A. & Moss, M. Motor subtypes of postoperative delirium in older adults. Arch. Surg. (Chicago, Ill : 1960) 146(3), 295–300 (2011).
Vaurio, L. E., Sands, L. P., Wang, Y., Mullen, E. A. & Leung, J. M. Postoperative delirium: The importance of pain and pain management. Anesth. Analg. 102(4), 1267–1273 (2006).
Litaker, D., Locala, J., Franco, K., Bronson, D. L. & Tannous, Z. Preoperative risk factors for postoperative delirium. Gen. Hosp. Psychiatry 23(2), 84–89 (2001).
Morimoto, Y. et al. Prediction of postoperative delirium after abdominal surgery in the elderly. J. Anesth. 23(1), 51–56 (2009).
Marcantonio, E., Ta, T., Duthie, E. & Resnick, N. M. Delirium severity and psychomotor types: Their relationship with outcomes after hip fracture repair. Am. Geriatr. Soc. 50(5), 851–857 (2002).
Kat, M. G. et al. Long-term cognitive outcome of Delirium in elderly hip surgery patients. Dement. Geriatr. Cogn. Disord 26, 1–8 (2008).
Marengoni, A. et al. Risk factors and outcomes for postoperative delirium after major surgery in elderly patients. PLoS ONE 10(8), e0136071 (2015).
Leung, J. M., Tsai, T. L. & Sands, L. P. Brief report: Preoperative frailty in older surgical patients is associated with early postoperative delirium. Anesth. Analg. 112(5), 1199–1201 (2011).
Michael, S. et al. Christine Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: An international, multicentre, double-blind, randomised clinical trial. Lancet 17, 31467–31468 (2017).
Guo, Y. et al. Prevalence and risk factors of postoperative delirium in elderly hip fracture patients. J. Int. Med. Res. 44(2), 317–327 (2016).
van der Sluis, F. J. et al. Risk factors for postoperative delirium after colorectal operation. Surgery 161(3), 704–711 (2017).
Wang, J. et al. Risk factors contributing to postoperative delirium in geriatric patients postorthopedic surgery. Asia Pac. Psychiatry. 7(4), 375–382 (2015).
Acknowledgements
Debre Tabor University, and the study participants.
Funding
Debre Tabor University.
Author information
Authors and Affiliations
Contributions
The data were developed by E.F., D.T., S.K., and K.G., who also contributed to the study’s design, performed the statistical analysis, and drafted the manuscript. Data collection, analysis, and manuscript writing were carried out by A.T., M.H., A.M., B.D., and A.B. All authors have reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethical approval for the study was granted by the Ethical Review Committee of Debre Tabor University. Permission to conduct the study was obtained from the respective hospital administrative bodies. Before participation, informed written consent was obtained from each participant, following a thorough explanation of the study’s objectives. The study ensured the confidentiality and anonymity of all participants throughout the research process.
Methodology statement
All methods, including citations, competing interests, and the data availability statement, were conducted by relevant guidelines and regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fenta, E., Teshome, D., Kibret, S. et al. Incidence and risk factors of postoperative delirium in elderly surgical patients 2023. Sci Rep 15, 1400 (2025). https://doi.org/10.1038/s41598-024-84554-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84554-2
