
Abstract
Liver enzymes are associated with liver function, but their relationship with body mass index (BMI) remains unclear. This cross-sectional study aimed to identify correlations between serum liver enzyme levels and BMI in the general population. The data were derived from the Dryad Digital Repository. Smooth curve and multiple linear regression analyses were performed to evaluate the associations between BMI and serum liver enzyme levels. A total of 15,464 participants, including 8430 males (54.5%), were included in the study, with a median age of 43.7 years. Smooth curve regression revealed that BMI followed U-shaped curves with respect to serum levels of liver enzymes (AST, ALT, and GGT). For AST serum levels, the turning points were BMI = 19.0 and 23.3 kg/m2; for ALT serum levels, the inflection points were BMI = 19.0 and 23.1 kg/m2; and for GGT serum levels, the inflection point was BMI = 19.5 kg/m2. In addition, stratified analysis revealed that sex, fatty liver, and smoking status as covariates modified the associations between BMI and AST and ALT serum levels in participants with higher BMIs (all interactions P < 0.01). Specifically, in the higher BMI range, the positive associations between BMI and liver enzymes were more robust in men (AST and ALT), participants with fatty liver disease (AST and ALT), and participants with a history of smoking (AST, ALT, and GGT). Interestingly, alcohol consumption modified the association between BMI and GGT serum levels, regardless of BMI. Our study is the first to identify a U-shaped association between BMI and serum levels of liver enzymes in the general population, which suggests a new target for regulating liver enzyme levels.
Similar content being viewed by others


Introduction
According to medical examination reports, liver enzymes, mainly including AST, ALT, and GGT, are standard indices that reflect liver function. Metabolic dysfunction associated steatotic liver disease (MASLD), which is closely related to overweight and obesity, is an important cause of abnormal serum liver enzyme levels in individuals who appear healthy according to physical examinations1,2. The prevalence of MASLD in overweight and obese people has increased significantly, reaching 70.0%3. Previous cross-sectional studies4,5,6 identified obesity as an important factor in the increase in serum liver enzyme levels. Body mass index (BMI) is the most commonly used index to classify obesity in individuals7; however, the relationship between BMI and serum liver enzyme levels remains inconclusive, with a shortage of relevant research.
The current limited studies demonstrated that BMI is positively correlated with serum liver enzyme levels. A study involving 251 Bangladeshi women revealed that participants with higher BMIs had a significantly greater incidence of abnormal elevation of at least one liver enzyme8. Another study that included an American population also revealed that higher BMI was associated with higher levels of AST and ALT, with increased AST and ALT levels in 9.0% of patients in the normal BMI category, 16.4% in the overweight group, and 24.0% in the obese category9. Whereas previous studies have focused on the relationship between high BMI and serum liver enzyme levels, the relationship between BMI and liver enzymes in participants with low BMI remains unclear.
An increasing number of healthy individuals have abnormal serum liver enzyme levels upon physical examination. As liver enzymes are closely related to body weight, an easily controlled physical index, identifying the relationship between BMI and serum liver enzyme levels in the general population might help to better guide lifestyle regulation and provide additional evidence.
Materials and methods
Database source
We obtained the data from the Dryad Digital Repository for secondary analysis, a freely available database (Okamura, Takuro et al. (2019). Data from: Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study [Dataset]. Dryad. https://doi.org/10.5061/dryad.8q0p192). The Japanese participants underwent medical examinations from 2004 to 2015 at Murakami Memorial Hospital (Gifu, Japan).
Study population and covariates
The data were uploaded by Okamura, Takuro, et al. on Dryad, and 15,464 participants were included. To conduct this cross-sectional study, we selected baseline data for analysis. All participants had BMI and liver enzyme serum level data, so addressing missing data was unnecessary. Because we aimed to explore the association between BMI and liver enzymes in the general medical examination population, the selection of covariates was mainly based on lifestyle habits in addition to demographic data, so the following covariates were considered: “age”, “gender”, “fatty liver”, “exercise”, “smoking status” and “alcohol consumption.” In accordance with Okamura, Takuro et al.10, the participants were examined via abdominal ultrasonography by trained technicians and then examined by gastroenterologists to diagnose fatty liver, and the included participants did not include people with viral hepatitis (defined by measurements of hepatitis B antigen and hepatitis C antibodies). Regular exercisers were defined as participants who regularly participated in any exercise more than once a week. The participants were divided into three groups according to their smoking status: nonsmokers (never smoked), ex-smokers (used to smoke but quit before the baseline visit), and current smokers (smoked during the baseline visit). The participants were divided into four groups according to their average weekly alcohol consumption: no or minimal (< 40 g/week), light (40–140 g/week), moderate (140–280 g/week), or heavy (> 280 g/week).
Statistical analysis
In this study, all the statistical analyses were conducted with the use of the statistical packages R (The R Foundation; http://www.r-project.org; version 4.2.0) and EmpowerStats (www.empowerstats.net, X&Y Solutions, Inc. Boston, MA). Normally distributed data are presented as the mean (SD), and categorical data are presented as n (%). First, we performed a smooth curve analysis to estimate BMI and serum liver enzyme levels. Then, according to the results of the smooth curve and log-likelihood ratio tests, multiple linear regression analysis was performed to evaluate the associations between BMI and serum liver enzyme levels with the covariates adjusted (age, sex, fatty liver, alcohol consumption, exercise habits, and smoking status). Finally, subgroup analysis and interaction analysis were performed to identify potential modifiers (sex, fatty liver, alcohol consumption, habit of exercise, and smoking status). P < 0.05 was considered a statistically significant criterion.
Results
Characteristics of the participants
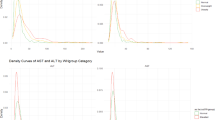
A total of 15,464 participants were enrolled in this study, with a median age of 43.7 years, and 8,430 males (54.5%) were included. The median BMI, AST, ALT, and GGT levels were 22.1 kg/m2, 18.4 IU/L, 20.0 IU/L, and 20.3 IU/L, respectively. More participant information, including blood pressure, other blood biomarkers, and lifestyle indicators, is detailed in Table 1. Importantly, as shown in Fig. 1, smooth curve analysis revealed an approximate U-shaped association between BMI and serum liver enzyme levels (AST, ALT, and GGT) after adjusting for confounding factors. For AST serum levels, the turning points were BMI = 19.0 and 23.3 kg/m2; for ALT serum levels, the inflection points were BMI = 19.0 and 23.1 kg/m2; and for GGT serum levels, the inflection point was BMI = 19.5 kg/m2.

Smooth curve on associations between BMI and serum liver enzyme levels. Adjustment factors included Age, Gender, Hypertension, Fatty liver, Exercise, Alcohol consumption and Smoking status.
Associations of BMI with AST, ALT, and GGT serum levels
As shown in Table 2, after adjusting for confounding factors, the AST serum level decreased with increasing BMI until the first inflection point (β = -0.7, 95% CI -1.0–0.4, P < 0.001). However, beyond the next inflection point, the AST serum level and BMI were positively correlated (β = 0.7, 95% CI 0.6–0.8; P < 0.001). When BMI was between the two inflection points, there was no correlation between the AST serum level and BMI. For the serum ALT level, there was a negative correlation between the serum ALT level and BMI when the BMI was ≤ 19.0 kg/m2 (β = -0.5, 95% CI -1.0–0.1, P = 0.019). ALT serum levels were positively correlated with BMI when BMI > 19.0 kg/m2. Interestingly, the positive correlation between the serum ALT level and BMI was more significant when BMI > 23.1 kg/m2 (β = 1.5, 95% CI 1.3–1.6, P < 0.001) than when BMI was between 19.0 and 23.1 kg/m2 (β = 0.5, 95% CI 0.3–0.7, P < 0.001). For the GGT serum level, there was a negative correlation between the ALT serum level and BMI when the BMI was ≤ 19.5 kg/m2 (β = -0.6, 95% CI -1.0–0.1, P = 0.009), and there was a positive correlation between the ALT serum level and BMI when the BMI was > 19.5 kg/m2 (β = 0.8, 95% CI 0.7–1.0, P < 0.001).
Subgroup analysis and interaction analysis of BMI and AST serum levels
Stratified analyses were performed using sex, fatty liver, exercise, alcohol consumption, and smoking status as stratification variables to assess the associations between BMI and AST serum levels, as shown in Table 3. In participants with a BMI > 23.3 kg/m2, sex (P < 0.0001), fatty liver (P < 0.0001), and smoking status (P = 0.0029) modified the associations between BMI and the serum AST level. Interestingly, in participants with a BMI ≤ 19.0 kg/m2, only alcohol consumption modified the association between BMI and AST serum level (P = 0.0088), which was the opposite of what was observed in people with a high BMI.
Subgroup analysis and interaction analysis of BMI and ALT serum levels
For the stratified BMI and ALT serum level analyses, in participants with a BMI > 19.9 kg/m2, sex and fatty liver affected the association between BMI and ALT serum level. In contrast, in participants with a BMI > 23.1 kg/m2, smoking status modified the association between BMI and AST serum level (P < 0.0001). In participants with a BMI < 19.0 kg/m2, no modification factors affected the association between BMI and the serum ALT level. More details are shown in Table 4.
Subgroup analysis and interaction analysis of BMI and GGT serum level
Interestingly, as shown in Table 5, we found that alcohol consumption could modify the association between BMI and serum GGT levels, regardless of BMI. In participants with a BMI > 19.5 kg/m2, sex (P < 0.0001) and smoking status (P < 0.0001) modified the association between BMI and the serum GGT level. In contrast, fatty liver affected the association between BMI and the serum AST level (P = 0.0138) in participants with a BMI < 19.5 kg/m2.
Discussion
In this study of 15,464 participants, we found U-shaped associations between BMI and serum liver enzyme levels in general patients after adjusting for identified confounders. Sex, fatty liver, alcohol consumption, and smoking are factors that affect the serum levels of liver enzymes. To our knowledge, we are the first to explore the nonlinear associations between BMI and serum liver enzyme levels, identify inflection points, and explore the correlation between low BMI and serum liver enzyme levels.
In this study, the results revealed that in the BMI range that represents normal weight, the AST serum level was not significantly correlated with BMI. In contrast, the ALT serum level was slightly positively correlated with BMI, possibly because ALT is more specific for reflecting liver damage than AST11. When BMI was in the overweight and obese range, both AST and ALT serum levels were significantly positively correlated with BMI. When BMI was greater than 19.5, the GGT serum level was positively correlated with BMI. Previous studies have reported elevated liver enzyme levels in overweight or obese people12,13. For people undergoing medical examinations, a prospective study of 6,846 male workers revealed that weight, rather than alcohol consumption, may be the main factor determining the serum levels of liver enzymes, and slight to moderate increases in weight were associated with increases in serum liver enzymes14. According to the World Health Organization’s recommended standards for Asian populations, a BMI between 18.5 and 22.9 kg/m2 is normal15. Our novel finding was that AST, ALT, and GGT levels were significantly negatively correlated with BMI at lower body weights. However, limited research may explain this phenomenon. A case report revealed that in elderly people with low body weight and/or malnutrition, metabolism in the liver was reduced, and glycogen accumulation was reduced, which can cause acute and significant liver damage16. Therefore, metabolic abnormalities associated with low body weight may also lead to elevated serum levels of liver enzymes. In addition, lower body weight may mean that the participants had poor nutritional levels, with one review suggesting that hypoalimentation was a cause of liver dysfunction and that improving the root cause of low nutrition, rather than subsequent liver disease, can lead to improvements in liver health17. For patients with alcoholic hepatitis, which usually presents with severe protein and calorie malnutrition18,19, nutritional support treatment can improve liver function20,21.
Having identified the correlation between BMI and serum liver enzyme levels, we next performed stratified analyses to explore the modifying factors. The results revealed that sex modified the correlations between AST, ALT, and GGT serum levels and BMI in participants with higher BMIs, and the positive correlations were more significant in male participants. These findings suggest that men are more likely to suffer liver damage due to weight gain. In a prospective study by Meisinger et al., the BMI of male participants was not significantly different from female participants, but the liver enzyme levels of male participants were significantly elevated22. It is difficult to explain why men’s liver enzymes are more strongly influenced by weight gain. Still, this phenomenon must be taken seriously, suggesting that men should carefully control their weight.
Interestingly, we found that in participants with higher BMIs, fatty liver modified the correlation between AST and ALT serum levels and BMI. In contrast, in participants with lower BMIs, fatty liver modified the correlation between serum GGT levels and BMI. In people with a high BMI, the serum levels of AST and ALT in participants with fatty liver have a strong positive correlation with BMI because fatty liver can lead to liver function impairment, and weight gain can exacerbate fatty liver and lead to further liver damage, causing rapid increases in AST and ALT serum levels. Among liver enzymes, only GGT is an independent predictor of fatty liver, whereas AST and ALT are not independent predictors of fatty liver23,24. One study reported that 19.2% of people with fatty liver disease were not overweight, and 40.8% were not obese, indicating that they had a lower BMI and tended to have dietary abnormalities and metabolic disorders25. Our results revealed a strong negative correlation between GGT serum levels and BMI in low-BMI participants with fatty liver, suggesting that this group of people may be able to gain weight through various methods, such as improving diet structure and correcting metabolic disorders, thereby reducing GGT serum levels and improving liver function.
In terms of lifestyle variables, the results showed that alcohol consumption modified the correlation between GGT serum levels and BMI in participants at all BMI levels. Multiple studies have shown that GGT is a widely used indicator of excessive alcohol intake and is the most sensitive liver enzyme to alcohol intake26,27,28,29. Moderate and heavy drinkers are more likely to experience elevated serum GGT levels than non-drinkers30. Interestingly, our results revealed the strongest correlation between serum levels of GGT and BMI in participants who consumed substantial amounts of alcohol, regardless of BMI range. This finding shed further light on the effect of alcohol dose on liver function. Further evidence is needed to elucidate why alcohol consumption modifies the association between AST serum levels and BMI only in participants with a lower BMI. Moreover, concerning smoking, previous epidemiological surveys have shown that smoking is positively correlated with serum liver enzyme levels31,32,33. Our results revealed that smoking status modified the positive correlation between the serum levels of liver enzymes and BMI in participants with a high BMI. Interestingly, the positive correlation between the serum levels of liver enzymes and BMI in non-smokers is weak. In contrast, the positive correlation between the serum levels of liver enzymes (AST, ALT, and GCT) and BMI in former smokers is stronger. The observed phenomenon indicates that the detrimental impact of smoking on liver function may persist for an extended period even after the cessation of smoking.
There are several strengths in this study. First, since the population we included was mainly the general population who underwent general medical examinations, our results were more valuable to the general population; this population should focus on maintaining the right weight to maintain better liver health. Second, our study first identified U-shaped associations between BMI and serum liver enzyme levels, and then elucidated the relevant inflection points, providing evidence for the relationship between weight adjustment and liver enzyme levels, that is, either too high or too low in BMI may lead to liver damage. Overweight people should actively lose weight, and emaciated people should take measures such as active supplementation to increase weight. Our findings help to guide lifestyle adjustments. Finally, interaction and stratification analyses elucidate factors that possibly modify the correlation between BMI and serum liver enzyme levels.
There are also several limitations in this study. First, this was a cross-sectional study, which can only confirm the association between BMI and serum levels of liver enzymes but cannot determine causality. Future prospective studies are needed to elucidate this association further. In addition, although careful adjustments were made for many potential confounding factors, regression analysis could not eliminate unknown or unmeasured variables. Furthermore, since most types of obesity in Asian populations are central obesity, these patients face greater disease risks than other populations with lower BMIs do34. Further studies are needed to determine if our findings are applicable to other ethnic groups.
Conclusions
We identified U-shaped associations between BMI and serum liver enzyme levels. The turning points were BMI = 19.0 and 23.3 kg/m2 for AST serum levels, BMI = 19.0 and 23.1 kg/m2 for ALT serum levels, and BMI = 19.5 kg/m2 for GGT serum levels. Further analysis is needed to elucidate the associations between BMI and serum liver enzyme levels and explore potential biological mechanisms involved.
Data availability
All the original data are available from the corresponding author.
References
Cusi, K. et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the diagnosis and management of nonalcoholic fatty liver Disease in Primary Care and Endocrinology Clinical Settings: co-sponsored by the American Association for the study of Liver diseases (AASLD). Endocr. Pract. 28, 528–562 (2022).
Eslam, M. et al. Ratziu V and George J. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J. Hepatol. 73, 202–209 (2020).
Quek, J. et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 8, 20–30 (2023).
Bizzaro, N. et al. Serum alanine aminotransferase levels among volunteer blood donors: effect of sex, alcohol intake and obesity. Ital. J. Gastroenterol. 24, 237–241 (1992).
Robinson, D. & Whitehead, T. P. Effect of body mass and other factors on serum liver enzyme levels in men attending for well population screening. Ann. Clin. Biochem. 26 (Pt 5), 393–400 (1989).
Hodgson, M. J., Van Thiel, D. H., Lauschus, K. & Karpf, M. Liver injury tests in hazardous waste workers: the role of obesity. J. Occup. Med. 31, 238–242 (1989).
Garrow, J. S. & Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 9, 147–153 (1985).
Noor, F. et al. Prevalence and Associated factors of liver enzyme abnormalities among Bangladeshi women: a cross-sectional study. Cureus 16, e57606 (2024).
Huynh, M. P., Bradshaw, P. T., Tana, M. M., Rachocki, C. & Somsouk, M. Obesity and metabolic outcomes in a safety-net health system. Biodemography Social Biology. 65, 257–267 (2020).
Okamura, T. et al. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Int. J. Obes. 43, 139–148 (2019).
Lee, H. S. et al. Protective effect of morin on dimethylnitrosamine-induced hepatic fibrosis in rats. Dig. Dis. Sci. 54, 782–788 (2009).
Papatheodoridis, G. V. et al. High prevalence of elevated liver enzymes in blood donors: associations with male gender and central adiposity. Eur. J. Gastroenterol. Hepatol. 19, 281–287 (2007).
Villegas, R. et al. Liver enzymes, type 2 diabetes, and metabolic syndrome in middle-aged, urban Chinese men. Metab. Syndr. Relat. Disord. 9, 305–311 (2011).
Lee, D. H., Ha, M. H. & Christiani, D. C. Body weight, alcohol consumption and liver enzyme activity–a 4-year follow-up study. Int. J. Epidemiol. 30, 766–770 (2001).
Consultation, W. H. O. E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet (London England). 363, 157–163 (2004).
Anno, T. et al. Hypoinsulinemic hypoglycemia triggered by liver injury in elderly subjects with low body weight: case reports. Endocrinology, diabetes & metabolism case reports. ;2018. (2018).
McNeice, A., Scott, R., Rafferty, G. P., Cash, W. J. & Turner, G. B. The hepatobiliary complications of malnutrition and nutritional support in adults. Ir. J. Med. Sci. 188, 109–117 (2019).
O’Shea, R. S., Dasarathy, S. & McCullough, A. J. Practice Guideline Committee of the American Association for the Study of Liver D and Practice Parameters Committee of the American College of G. Alcoholic liver disease. Hepatology 51, 307–328 (2010).
Singal, A. K. et al. Nutritional status of patients with alcoholic cirrhosis undergoing liver transplantation: time trends and impact on survival. Transpl. Int. 26, 788–794 (2013).
Arsene, D., Farooq, O. & Bataller, R. New therapeutic targets in alcoholic hepatitis. Hepatol. Int. 10, 538–552 (2016).
Cabre, E. et al. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology 32, 36–42 (2000).
Meisinger, C. et al. Isocaloric Substitution of Dietary Carbohydrate Intake with Fat Intake and MRI-Determined total volumes of visceral, subcutaneous and hepatic Fat Content in Middle-aged adults. Nutrients ;11. (2019).
Bedogni, G. et al. The fatty liver index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 6, 33 (2006).
Ruhl, C. E. & Everhart, J. E. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment. Pharmacol. Ther. 41, 65–76 (2015).
Ye, Q. et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 5, 739–752 (2020).
Rantala, A. O. et al. Gamma-Glutamyl transpeptidase and the metabolic syndrome. J. Intern. Med. 248, 230–238 (2000).
Puukka, K. et al. Age-related changes on serum ggt activity and the assessment of ethanol intake. Alcohol Alcohol. 41, 522–527 (2006).
Hietala, J., Puukka, K., Koivisto, H., Anttila, P. & Niemela, O. Serum gamma-glutamyl transferase in alcoholics, moderate drinkers and abstainers: effect on gt reference intervals at population level. Alcohol Alcohol. 40, 511–514 (2005).
Agarwal, S., Fulgoni, V. L., Lieberman, H. R. & rd and Assessing alcohol intake & its dose-dependent effects on liver enzymes by 24-h recall and questionnaire using NHANES 2001–2010 data. Nutr. J. 15, 62 (2016).
Alatalo, P. et al. Biomarkers of liver status in heavy drinkers, moderate drinkers and abstainers. Alcohol Alcohol. 44, 199–203 (2009).
Wang, C. S., Wang, S. T., Chang, T. T., Yao, W. J. & Chou, P. Smoking and alanine aminotransferase levels in hepatitis C virus infection: implications for prevention of hepatitis C virus progression. Arch. Intern. Med. 162, 811–815 (2002).
Nakanishi, N., Nakamura, K., Suzuki, K. & Tatara, K. Lifestyle and serum gamma-glutamyltransferase: a study of middle-aged Japanese men. Occup. Med. (Lond). 50, 115–120 (2000).
Higashikawa, A. et al. Association of working conditions and lifestyle with increased serum gamma-glutamyltransferase: a follow-up study. Arch. Med. Res. 36, 567–573 (2005).
Bajaj, S. S., Zhong, A., Zhang, A. L. & Stanford, F. C. Body Mass Index thresholds for asians: a race correction in need of correction? Ann. Intern. Med. (2024).
Acknowledgements
The authors sincerely thank Okamura, Takuro et al. for uploading their meaningful data and Dryad for facilitating the flow of high-quality scientific data.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 82360171, 82460056), Jiangxi Provincial Academic and Technical Leaders Training Program in Major Disciplines (No. 20232BCJ23028), Science and Technology Project of Health Commission of Jiangxi Province (No. 202410254), and Science and Technology Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (No.2023A0337).
Author information
Authors and Affiliations
Contributions
Zixi Huang and Zhenyan Xu: contributed to the design of the article, Zixi Huang: data collection and writing, Hualong Liu: obtained the original data and writing, Wen Zhuo and Yuliang Chen: participated in the data analysis, Ying Huang, Xin Chen and Teng Lu: participated in the writing, Zhenyan Xu: responsible for the revision of the full text.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Z., Liu, H., Zhuo, W. et al. U-shaped associations between body mass index and serum liver enzyme levels. Sci Rep 15, 443 (2025). https://doi.org/10.1038/s41598-024-84709-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-84709-1
