
Abstract
This study investigates the asymmetry in heart rate (HRA) during fetal development in the fetus and mother. R-R intervals from noninvasive fetal and maternal ECG signals from 102 pregnant women whose gestational age ranges from 20 to 40 weeks were analyzed. Several HRA indices, which evaluate the accelerations and decelerations in RR interval time-series data, were utilized to examine the variations in HRA in both the fetus and the mother. Results showed that 74.5% of mothers showed asymmetry when measured using index Deceleration Input (DID2A). In fetuses, the asymmetry is driven by acceleration-to-deceleration transitions, while in mothers, asymmetry is influenced by deceleration-to-acceleration. Also, phase rectified signal averaging (PRSA) reveals that acceleration and deceleration capacities (AC and DC) show significant correlations with gestational age (GA), indicating that PRSA is a promising tool for assessing fetal development. This study also showed that Porta Index (PI) is associated with sympathetic activity, and the fetal behavioral state influences maternal HRA. This work provides new insights into fetal heart rate asymmetry, leading to a deeper understanding of fetal health during pregnancy.
Similar content being viewed by others

Introduction
The development of the human Autonomic Nervous System (ANS) in early pregnancy can only be investigated through autopsy; however, in later stages of gestation, the Heart Rate Variability (HRV) analysis offers valuable insights into ANS maturation1. The most important stages of ANS development occur before the 35th week of pregnancy2,3. Later on, fetal behavioral states observed using heart rate spectral analysis4 give information about the maturity of the ANS. The sympathetic nerves begin to form as early as the 8th week of pregnancy, with their most dynamic development occurring during the middle of the fetal period5. The parasympathetic nervous system develops slowly, with its most dynamic maturation occurring between 25 and 32 weeks of gestation6. The phases of ANS growth are reflected in fetal heart rate (HR), which increases by approximately 3.3 bpm per day starting from the 5th week of gestation, peaking at around 175 bpm before the 9th week of gestation. Afterwards, it gradually decreases to about 144 bpm by the end of pregnancy7.
The asymmetry in human heart rate (Heart Rate Asymmetry–HRA) has been a subject of research for nearly 20 years8,9. Initially, the time irreversibility of human HR was used to explain HRA. However, the phenomenon of HRA more specifically refers to the uneven nature of HR acceleration and deceleration.
Heart rate asymmetry (HRA) provides a more detailed understanding of cardiovascular dynamics than traditional heart rate variability (HRV) analysis by distinguishing between accelerations and decelerations, rather than treating variability as a whole. This distinction allows HRA to be more sensitive to physiological changes, such as during orthostatic stress, where conventional HRV metrics may miss critical insights10. HRA also enhances our understanding of autonomic nervous system activity by revealing how decelerations contribute more to short-term HRV, while accelerations dominate long-term HRV, highlighting key regulatory mechanisms11. These advantages position HRA as a promising tool for advancing cardiovascular assessment and developing novel diagnostic approaches.
Past research on fetal HRA has been mainly limited to the analysis using cardiotocograph (CTG) and magnetocardiography (MCG)12. To understand fetal HRA in humans, few studies used HRA metrics13. The study by Karmakar et al.14 showed that fetal HRA undergoes significant changes before and after 35 weeks of gestation. They also found that HRA tends to increase in the late gestation of pregnancy. Other study supports this observation also in earlier stages of pregnancy15. This shows the maturation of the ANS, specifically the shift towards sympathetic dominance as the fetus approaches full term. This finding supports the idea that analyzing fetal HRA can provide valuable insights into the development of fetal ANS14.
HRA studies conducted in different age groups have reported different, sometimes contradictory results of the analysis of the relationship between HRA and age. Long-term HRA correlates with age, significant differences were shown for men between two age groups: the first under 30 and the second over 4010. In such age ranges, HRA was reduced in older subjects. However, in the case of children aged 3–18 years, significant positive correlations of the same HRA parameters with age were observed16. On the other hand, standard HRA measures do not change significantly with age, neither in the range of 25–74 years nor in the case of people under 18 years of age10,16,17. Considering these previous studies, the objective of this study is to analyze fetal HR variations in order to observe the expected changes of asymmetry between accelerations and decelerations in fetal HR at different stages of development, as well as to examine maternal HRA and its changes occurring with the progression of pregnancy to better understand potential relations between fetal and maternal autonomic regulation during pregnancy.
Previous studies on measures differentiating accelerations and decelerations in the fetal heart rate have been limited primarily to the analysis of PRSA18,19,20. A disadvantage of using PRSA is the lack of established standards for the values of the parameters used there (s and T). Part of the studies are based on animal, not human fetuses21,22,23.
Materials & methods
Dataset information and preprocessing
A total of 245 healthy pregnant women, aged between 20 and 41 years, were examined using non-invasive electrocardiography (ECG) signals in a supine position. These data were collected from a multicenter trial involving Tohoku University Hospital, Japan (115 recordings), Children’s National Hospital, USA (64 recordings), and Kanagawa Children’s Medical Center, Japan (66 recordings). All recordings were collected using 12-channel abdominal ECG signals with a sampling frequency of 1000 Hz and 16-bit resolution. The study was approved by the ethics boards of Tohoku University (IRB: 2015-2-80-1). All participants gave written informed consent, and the experiments followed established guidelines and regulations. Specific age details for participants from Children’s National Hospital could not be shared due to Institutional Review Boards restrictions.
The following inclusion criteria were applied in the study:
-
Fetuses with a gestational age ranging from 20 to 40 weeks.
-
ECG recordings that provide a complete and continuous fetal cardiac signal.
-
Recordings with a minimum required duration of 270 s.
-
Only high-quality fetal ECG signals extracted from maternal signals, with less than 10% incorrectly detected intervals or HR artifacts.
Exclusion Criteria:
-
ECG recordings that lack a complete and continuous fetal cardiac signal (59 recordings excluded).
-
Recordings shorter than the minimum required duration of 270 s (27 recordings excluded).
-
Noisy or unreadable fetal ECG signals and recordings with more than 10% incorrectly detected intervals or HR artifacts (57 recordings excluded).
After applying these criteria, 102 high quality ECG recordings were included for further analysis.
The separation of the fetal ECG from the composite abdominal signal (composed from both maternal and fetal signals) was performed in MATLAB24 using a combination of maternal ECG cancellation and blind source separation with a reference25. The ECG signals have been filtered using Pan-Tompkins method26,27. The R peak detection has been performed with HeartPy software28. The detection of artifacts and identification of incorrectly detected intervals involved filtering the RR sequences automatically using the Hampel filter29, followed by a manual review of all ECG recordings and tachograms.
Figure 1 shows the tachogram of the fetus in the upper panel and the mother in the lower panel. The red arrows in the fetal tachogram indicate a drop in fetal HR, followed by a gradual return to the previous HR.

Simultaneously recorded tachograms of fetal (upper panel) and maternal (lower panel) heartbeat intervals recorded in the 20th week of gestation. Red arrows indicate the fetal heart rate variations that may have the biggest impact on the heart rate asymmetry in the recording.
The analysis of these fetal HR variations, particularly accelerations and decelerations, is the focus of this study. Asymmetry between these accelerations and decelerations in fetal HR at different stages of development, as well as in mothers, is studied.
Heart rate variability
HRV features, including mean RR interval (RR), Standard Deviation of the Normal-to-Normal intervals (SDNN) and a Root Mean Square of Successive Differences (RMSSD) of the RR intervals were extracted for all of the maternal and fetal recordings. Also, the power spectral density estimation was performed using the Welch method with a 50% window overlap. The frequency bands analyzed were: Very Low Frequency (VLF) ranges from 0.003 to 0.04 Hz, Low Frequency (LF) ranges from 0.04 to 0.15 Hz, and High Frequency (HF) ranges from 0.15 to 0.4 Hz. The same ranges were used for maternal and fetal recordings30. Additionally, the ratio between LF and HF (LF/HF) was also calculated31.
Fetal gestational age
The study population included fetuses with gestational ages ranging from 20 to 40 weeks. The specific distribution of GA within this cohort is detailed in the histogram presented in Fig. 2.

Distribution of gestational age in study group of 102 fetuses.
One objective of this research is to investigate the potential relationship between fetal GA and HRA and PRSA parameters derived from fetal ECG. Furthermore, we aim to explore potential associations between fetal GA and the corresponding HRA and PRSA metrics calculated from maternal ECG recordings obtained simultaneously. Gestational age serves as a crucial indicator of fetal development, particularly the maturation of the ANS. Given that HRA is an intrinsic characteristic closely related to overall HRV, which reflects ANS activity, it is hypothesized that fetal HRA metrics may exhibit changes correlating with advancing GA. Such changes could mirror the developmental trajectory of fetal autonomic control, providing insights into normative physiological maturation throughout the latter half of pregnancy. Understanding these potential developmental trends is essential for establishing baseline fetal physiology.
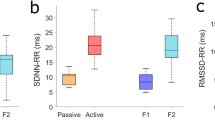
Fetal behavioral states
The behavioral state of a fetus has been assessed by analyzing the HR signal with the unsupervised k-means clustering technique applied using the fetal HRV features32. The classification of the fetal behavioral states into Active (A) and Rest (R) states was based on the criteria provided by Pillai and James33,34. R state was defined as a baseline HR below 160 bpm with no accelerations and an oscillation bandwidth within the range of − 7.5 to 7.5 bpm. The A state was characterized by a baseline HR exceeding 160 bpm and the presence of accelerations greater than 15 bpm. Also, if the oscillation bandwidth is ≥ 7.5 or ≤ − 7.5 bpm, the fetal state is considered as active35.
Heart rate asymmetry
One of the basic methods to understand HRA is the Poincaré plot, which visually compares consecutive heartbeat intervals (Fig. 3). The plot is divided into two areas by the line of identity: HR decelerations (interval elongations) appear above the line, while accelerations below the line. By analyzing the distribution of points on either side of the plot, it is possible to determine whether the HR series is asymmetrical.

Example of a Poincaré plot considering 200 consecutive heart rate intervals (approx. 2 min. 43 s.) from one recording. The perpendicular distance of a given point to the line of identity (used in Guzik Index–GI) and phase angle with respect to the line of identity (used to obtain Slope Index–SI) are pointed out.
The measures based on the Poincaré plot can be obtained for various lags, i.e. shifts between the axes of the plot. In its basic form (lag = 1) the two sets of consecutive RR intervals are {RR1; RRk-1} and {RR2; RRk}, where k is the total number of HR intervals. For lag > 1 the sets of intervals will convert into {RR1; RRk-l} and {RR1+l; RRk}, where l is the lag value. This gives information about the dependence between distant intervals which helps to understand more long-term relationships in pulse regulation.
In this study, the number of points in the plot that are located beyond the line of identity is denoted as n, n– refers to the number of HR accelerations, and n+ represents the number of decelerations. The difference between RR intervals is calculated as ΔRRi = RRi+1 – RRi. The Poincaré plot-based metrics used in this study include the Porta Index (PI), which is the proportion of points below the line of identity (i.e., HR accelerations) out of all the variations in heart rate, calculated as PI = n–/n15. The Guzik Index (GI) represents the contribution of deceleration to short-term variability. GI is calculated using the formula SD1d2/SD12, where SD1d2 = var(ΔRRi/sqrt(2)) which is the distribution (variance) of points across the line of identity, and SD12 is the same variance calculated only for n+ deceleration points9,36. GI can also be interpreted as the contribution of decelerations to short-term HRV, which means the variation of the perpendicular distances of points to the line of identity (Fig. 3)37. Ehlers Index (EI) reflects the skewness of the distribution of ΔRR and is calculated using the formula EI = μ3/σ3, where μ3 is the third central moment of ΔRR, and σ3 is the third power of the ΔRR standard deviation38. EI > 0 indicates a right-skewed ΔRR distribution (extended tail of the ΔRR histogram in the direction of HR decelerations, i.e., positive ΔRR differences). The Slope Index (SI) is the ratio of all the deceleration phase angles of the Poincaré plot points obtained with respect to the line of identity (Fig. 3) to the total sum of the phase angles39. In this work, the origin of the coordinate system was used as a reference point to obtain SI40.
All the above-mentioned Poincaré plot measures are based on the distribution analysis of the points, i.e. pairs (RRi; RRi+1), on the graph. The Deceleration Input (DI) is obtained using triplets (RRi-1;RRi;RRi+1) that form vectors on the Poincaré plot (Fig. 4). Each triplet consists of two pairs of consecutive RR intervals: (RRi-1;RRi) and (RRi;RRi+1) that mark the initial and ending position of the vector. Therefore, the vectors create a “path” made by the consecutive points on the Poincaré plot. DI is defined for vectors that are crossing the line of identity on the plot (black arrows in Fig. 4), which are transitions between HR accelerations and decelerations (RRi-1 > RRi < RRi+1 or RRi-1 < RRi > RRi+1). The consecutive decelerations and accelerations are marked as blue and red arrows respectively (Fig. 4).

Examples of simultaneously recorded 5 min fetal (A) and maternal (B) Poincaré plots (left) in the 38th week of gestation and paths made by consecutive points on Poincaré plot (right). The arrows connecting consecutive points on the plot have blue color for two consecutive decelerations (above the line of identity), red color for subsequent accelerations and black ones are the transitions between the accelerations and decelerations.
The contribution of the deceleration into the i-th HR transition is obtained using DIi = ΔRRi / |ΔRRi-1| +|ΔRRi| for acceleration to deceleration transition and DIi = ΔRRi-1 / |ΔRRi-1| +|ΔRRi| for deceleration to acceleration transitions, with the numerator changing depending on which pair of intervals the deceleration occurs.
The formula for DI is given by the average of DIi components41,42. The DI is the mean input of decelerations into all types of HR transitions and is calculated as
where nT = nDA + nAD is a number of all types of HR transitions, with nT represents the total number, nDA represents deceleration to acceleration transitions and nAD represents acceleration to deceleration transitions number.
The DI can also be calculated for specific transitions. In the case of acceleration-to-deceleration transitions, the formula is:
and for the deceleration to acceleration, the formula is:
Based on the approach of Piskorski and Guzik, the asymmetry in the Poincaré plot is defined using the above-mentioned indices separately as GI > 0.5, PI > 0.5, EI > 0, SI < 0.5, and DI/DID2A/DIA2D < 0.543.
Figure 5 shows the HR transition of DIi < 0.5, where the shortening of two consecutive intervals (HR acceleration) is greater than their elongation (HR deceleration). Therefore, DI < 0.5 indicates that the accelerations in HR transitions are stronger than the decelerations.

A fragment of fetal HR tachogram (GA = 23 weeks) with two types of HR transitions indicated: acceleration to deceleration and an opposite one. Note the difference between HR intervals (ΔRR) is greater in acceleration in both types of transition–therefore DIi < 0.5 in both of them.
All the Poincaré plot HRA measures were calculated within the lag range from 1 to 10. Linear mixed-effects models were applied, incorporating random effects for participant ID. HRA indices obtained for the fetus were the dependent variables, while GA, lag, mother result, and state served as predictors. The analogous analysis was carried out for maternal HRA results. However, only GA, Lag, and State were used as potential fixed effects since the mother-fetus relationship had already been verified in a previous comparison.
Phase rectified signal averaging analysis
The averaging procedure of ten consecutive decelerations surroundings (in order to obtain the deceleration capacity) has been shown in Fig. 6. The window length, L = ± 10 heartbeat intervals, has been used in this study. Phase Rectified Signal Averaging (PRSA) was done as described originally in detail by Bauer et al. in44. In this study, a window length of L = ± 10 heartbeat intervals were used. The procedure for Phase Rectified Signal Averaging (PRSA) was done based on the detailed method explained by Bauer et al.44.

The procedure of Phase Rectified Signal Averaging for 10 deceleration surroundings obtained from a maternal (GA = 20 weeks) heart rate tachogram. The deceleration selection criterion T = 1 so the averaged value X(-1) will always be shorter than X(0). In this case the scale s = 2 and therefore the Deceleration Capacity is obtained by DC = [X(0) + X(1)–X(–1)–X(–2)]/4.
Deceleration Capacity (DC), Acceleration Capacity (AC), and Deceleration Reserve (DR) were calculated for multiple values of s and T parameters: s ∈ [1; 10] and T ∈ [1; 10]. The DR was obtained as a sum of DC and (negative) AC: DR = DC + AC21. Since the window length L influences only the number of decelerations and accelerations captured in the marginal fragments of the recording, this factor was not considered a variable in this work.
The statistical analysis
The occurrence of HRA has been evaluated with a binomial test verifying the hypothesis of whether the probability of asymmetric cases occurrence equals 50%37. All statistical analyses were conducted with a significance level (α) set at 0.05.
In this study, mixed effects models were employed to analyze the HRA results obtained for various Poincaré plot lags. This approach allowed us to account for the inherent dependencies within the data, such as repeated measures from the same individuals, while also capturing the variability between different subjects. By incorporating both fixed and random effects, our analysis effectively delineated the individual-level changes throughout lags while accounting for the overall population trends. The potential predictors for fetal HRA were GA, state, lag, and maternal results (of the same HRA index). In the case of maternal HRA–the tested predictors were GA, lag, and state. To refine the model, the backward effect elimination method was used, systematically excluding non-significant predictors until the most optimal model was achieved. Model fit was assessed using AIC (Akaike Information Criterion). The comparisons were conducted using Spearman’s rank correlation coefficient (ρ).
All the calculations, statistical analyses and plots were done using R statistical software (v. 4.2.2) using appropriate packages45,46,47,48,49.
Results
Poincaré plot-based HRA measures
The occurrence of HRA in maternal and corresponding fetal HR signals are presented in Table 1.
As summarized in Table 1, fetal HRA is markedly more pronounced than maternal, as evidenced by the significant asymmetry observed across multiple fetal indices, including the Guzik Index (GI), Porta Index (PI), Ehlers Index (EI), and Slope Index (SI). In contrast, most maternal indices did not exhibit statistically significant asymmetry, with the exception of Deceleration Input, especially for deceleration-to-acceleration transitions (DID2A) and EI. Notably, fetal GI (92.2%) and PI (98.0%) demonstrated the highest occurrence of asymmetry, underscoring the distinct regulatory mechanisms governing fetal heart rate variability.
Model diagnostics indicated that the robustness and fit to the data were satisfactory only within the lag range of 1 to 4. Including lag ≥ 5 did not improve the model for any of the indices examined. The selection of the mixed-effects model (DI ~ lag) was based on a systematic evaluation of model fit and assumptions. First, when comparing models with different numbers of explanatory variables, the decision was guided by marginal and conditional R2, prioritizing the simpler model in cases where R2 values were similar. When evaluating models with the same set of explanatory variables across different HRA measures, the model having the lower AIC value was chosen. Finally, models that failed to meet key assumptions – most commonly due to violations of linearity – were rejected, even if they initially appeared to offer a better fit. The most reliable outcome was observed when examining the dependence of fetal Deceleration Input (DI) on lag. Table 2 represents the results of the derived formula: DI as a function of lag, with the subject ID considered as a random effect.
The dependence of DI on lag is illustrated in the DI boxplots shown in Fig. 7.

The Deceleration Input (DI) boxplots in different Poincaré plot lags. Lags 1–4 are highlighted in red.
No improvement in analysis performance was observed when considering lags higher than 4. As a result, the results for these calculations (lag: 5–10) are not included in the further part of the study.
The optimal model for fetal HRA did not incorporate GA or maternal results, as they did not significantly enhance the model. However, during model inspection, direct associations between these variables were identified. Table 3 represents the rank-based comparison of the asymmetry measures between the fetus and GA, with results calculated separately for each lag ranges from 1 to 4.
A significant negative correlation was observed for the index across all 4 lags in both GI and EI. Notably, asymmetry increases with GI, PI, and EI, while it decreases with DI and SI. As a result, positive correlation between asymmetry and GA was found only in the DID2A index (lag = 4). Moreover, while examining the relationship between maternal and fetal HRA, significant correlations were observed at lag = 1, including positive correlations (ρ = 0.285 in DI and ρ = 0.283 in DID2A) and a negative correlation (ρ = − 0.203 in SI). At higher lags, only DIA2D showed a negative correlation (ρ = − 0.256) at lag 3. No correlation was found between maternal and fetal average heart rates in this study.
For maternal HRA, the final model revealed significant associations between the maternal PI, lag, and the fetal state. The results for the model based on the formula maternal PI ~ Lag + State (of fetus), with ID treated as a random effect, are represented in Table 4. The calculations were limited to lags ≤ 4, as no linear dependence between the HRA index and lag was observed at higher lags.
GA did not significantly improve any model based on maternal HRA results. However, during model diagnostics, potential direct monotonic relationships between GA and maternal results were identified. The correlations between gestational age and maternal HRA metrics for lag = 1 are presented in Table 5.
No significant correlation between maternal HRA and GA was observed for lag > 1. The strongest association with gestational progress in mothers was found for DID2A (ρ = 0.330, p < 0.001), as shown in Fig. 8.
Figure 8 shows a gradual increase in DI as the pregnancy progresses. Before 30 weeks of gestation, asymmetry is more prevalent, with more cases of DI < 0.5. However, after 30 weeks, cases with DI < 0.5 and DI > 0.5 occur with similar frequency.

Spearman’s Correlation between Deceleration Input calculated for deceleration to acceleration type of transitions only (DID2A) and gestation week (GA) in 102 pregnant women.
PRSA
The mean of AC, DC and DR has been calculated for each s and T value from range 1 to 10. The dependency of mean PRSA measures on s and T parameters is shown in Fig. 9.

The average PRSA measures dependence on s and T parameters in 102 healthy fetuses. Left panel presents mean values of Acceleration Capacity (AC), middle one–Deceleration Capacity (DC) and right one–Deceleration Reserve (DR). The 3D plots are located in the upper row and the 2D projection of each plot is presented respectively under a corresponding graph.
The relationships of PRSA indices with s and T are clearly nonlinear; hence, a linear model was not constructed. Instead, the tabulated results of individual comparisons for each variable are shown below (Table 6). The correlation of PRSA measures (acceleration and deceleration capacities) and GA is represented in Fig. 10.

Results of Spearman’s correlation between the fetal PRSA Acceleration Capacity (left) and Deceleration Capacity (right) and gestational age (GA) of 102 healthy fetuses. All p-values < 0.001
A significant (p < 0.001) negative correlation was observed between AC and GA, along with a positive correlation between DC and GA, for all s and T values (Fig. 10). The DR, however, has been significantly correlated with GA only within s = T = 1. Hence, the values of Spearman’s ρ within s = 1 separately are shown in Table 6.
A significant positive correlation of DR asymmetry index with GA (p = 0.034) was obtained only within s = 1 and T = 1.
Figure 11 represents the dependency between maternal PRSA and GA. The correlations of maternal PRSA with GA were weaker than fetal ones – the strongest dependencies were observed in DC (s = 9, T = 1): ρ = 0.38; p < 0.001; DR (s = 4, T = 1): ρ = 0.334; p < 0.001 and AC (s = 10, T = 4): ρ = − 0.242; p = 0.014. The correlations of PRSA metrics (AC and DC) between maternal and fetal signals are presented in Table 7 for all the studied s and T values.

The rank correlation between maternal PRSA and GA. The Spearman’s ρ not significantly different from 0 has been converted into 0 for better readability of the plot.
The only significant (p = 0.013) Spearman’s correlation for DR has been obtained for s = 1 and T = 1 with Spearman’s ρ = 0.247.
Heart rate variability
The spectral analysis results of HRV of mother and fetus have been summarized in Table 8. The mean RR for fetuses was significantly smaller compared to maternal recordings, reflecting the faster HR in fetuses. SDNN was higher in maternal recordings compared to fetal recordings, indicating greater HRV in mothers. RMSSD followed a similar pattern, with fetuses showing lower variability compared to mothers. Power spectral density analysis revealed that maternal recordings had higher values in all frequency bands, particularly in VLF) and HF ranges. The LF/HF ratio was higher in fetuses than in mothers, indicating a difference in the balance between sympathetic and parasympathetic activity in fetal HR regulation. These findings highlight the physiological differences in HR regulation between fetuses and mothers.
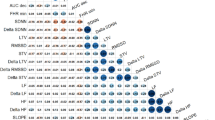
The Spearman’s correlation between all the HRV and HRA measures has been tested within the basic metric parameters, i.e., lag = 1 in the case of HRA indices and s = T = 1 in PRSA. The correlation matrix of all the metrics studied in this paper is presented in Table 9.
However, some relations presented in Table 9 do not manifest linear dependencies–e.g., the strong dependency between DR and PI in maternal recordings exhibits logistic properties rather than linear ones. The examples of the relation between DR and DI, GI and PI in maternal recordings are presented in Fig. 12.

The correlations (Spearman’s ρ–here marked as R) between chosen Poincaré plot–based measures (DI–left, GI–middle and PI–right panel) and PRSA-based asymmetry measure: Deceleration Reserve (DR). Poincaré plot lag and PRSA s and T parameters set to 1.
Discussion
The prevalence of HRA occurrence in healthy fetuses (Table 1) is clearly notable, especially using indices PI (98.0% of asymmetric cases), GI (92.2%), and EI (91.2%). The studies of Piskorski and Guzik carried out on young, healthy adults generally report GI and PI asymmetry presence in 62–84% of the population50,51,52. Also, the asymmetry tends to decrease with age. However, the phenomenon of time irreversibility in HR is still not fully understood, and various studies report different outcomes depending on the measurement method, group size, and possibly even the data curation process8,10,17. Considering all these factors, HRA may be a phenomenon present clearly in fetal life and declining with age in adulthood. Physiologically, the reduction in fetal HRA reflects the gradual maturation of the autonomic nervous system (ANS). At the start of fetal development, the sympathetic nervous system develops, leading to more pronounced fluctuations in heart rate and greater asymmetry in heart rate. As the fetus matures, the parasympathetic system develops, leading to reduced variability in heart rate, and decline in HRA. Regarding system complexity, a decrease in HRA does not indicate a less complex system. In early gestational age, greater variability and asymmetry reflects an immature autonomic nervous system. The later stage of gestation shows more stable cardiac regulation and symmetry, indicating the development of ANS. The sympathetic and parasympathetic branches of the human ANS are responsible for HR regulation change and their control level throughout human life. Therefore, it affects HR descriptors like HRA indices53,54.
The part of analysis employing mixed-effects models indicated that gestational age was not a significant predictor for the examined fetal HRA indices. One potential explanation for this finding could relate to the non-uniform distribution of GA within our study sample, as depicted in the histogram (Fig. 2). This distribution exhibited rather a bimodal than uniform pattern, characterized by a relative scarcity of cases around the 30-week gestation mark. Such sampling across the gestational range might affect the ability of the mixed-effects models to robustly capture the influence of GA, especially if the relationship is non-linear or subtle. To circumvent potential limitations associated with the GA distribution, bivariate relationships were also explored using Spearman’s rank correlation to assess monotonic associations between GA and the calculated HRA and PRSA measures.
Cases of HR slowdown to less than 110 bpm (RR intervals over 550 ms) are generally understood as fetal bradycardia; however, spontaneous HR drops followed by an instant return to a normal state are commonly observed during fetus examinations and do not indicate irregularities55. This kind of variation (visible in Fig. 1) may appear due to the movement of the mother or fetal breathing activity56,57. In this study, it is observed that there is a decrease in their frequency and intensity with fetus development. This explains the significant decrease of GI and EI in fetuses with gestation age (Table 3). However, the dependence of HRA and GA should not be extrapolated – the results of Porta et al., including GA < 20 weeks, stay in contradiction with our results reporting the increase of asymmetry measures between the groups of fetuses in GA 16–24 and 25–32 weeks15.
The underlying mechanisms of HRA differ between fetuses and mothers (Table 1), with fetal asymmetry driven by both acceleration (PI > 0.5, SI < 0.5) and deceleration-dominant measures (GI > 0.5, DI < 0.5). Conversely, maternal asymmetry is predominantly influenced by acceleration-dominant measures (DID2A < 0.5), indicating a heightened sensitivity to heart rate accelerations. Additionally, the positive and significant EI (p = 0.004) indicates a subtle but notable skew toward deceleration-driven asymmetry in maternal heart rate. However, other maternal indices, including GI, PI, SI, and DIA2D, did not reach statistical significance, suggesting a weaker or less consistent presence of asymmetry in maternal heart rate dynamics compared to the fetus. These findings highlight fundamental differences in fetal and maternal autonomic regulation, with fetal HRA reflecting more pronounced and structured asymmetry patterns, likely due to the ongoing maturation of the autonomic nervous system during gestation.
74.5% of studied women were in asymmetry by DID2A, and the deceleration to acceleration type of HR transitions has a stronger contribution to overall DI asymmetry rather than acceleration to deceleration transitions (Table 1). Especially in earlier stages of pregnancy, the average input of decelerations (described by DID2A) is smaller than 0.5, which indicates that this area of heart functioning may be affected by the pregnancy progression (Fig. 8). Since HR accelerations are generally caused by sympathetic activation and vagal withdrawals, it is presumed that one of these behaviors is regulated by factors related to pregnancy development. Moreover, the contribution of different types of transitions to the overall DI asymmetry is different in fetal and maternal HR recordings: acceleration to deceleration transitions generate the asymmetry in fetuses, while in pregnant females, the deceleration to acceleration type of transitions plays a key role in DI level.
The fetal ANS undergoes a sequential development, with the sympathetic nervous system start first, followed by the parasympathetic system, and finally a subsequent dominance of sympathetic activity near to the term. This developmental progression is seen in the observed HRV parameters. The significantly shorter mean RR intervals in fetuses, compared to maternal signals, reflects faster HR, which indicates sympathetic dominance. Over time, as the parasympathetic system develops, greater modulation of HR occurs, contributing to an increase in variability. The differences in LF/HF ratios between mothers and fetuses suggest variations in sympathovagal balance. It is speculated that these changes align with the known developmental progression of the ANS, eventually leading to a more sympathetic regulation closer to the term. The dependence between HRA index and lag can be interpreted through the sympatho-vagal balance. The sympathetic branch of ANS is responsible for slower HR oscillations (2–3 s) but of higher amplitude58. The average length of 4 consecutive RR intervals oscillates around 1,67 ms (Table 8), and therefore, relatively stable values of DI for lag ≥ 4 (Fig. 7) may be evidence of its link to the vagal regulation. The lag values in other studies used to evaluate HR behavior in adults reached up to 10059. Our study shows that in the case of fetal HR, the crucial interactions between the neighboring RR intervals occur within 5 heartbeats (4 intervals), which may be caused due to the nature of fetal HR–it is much faster and more consistent in time. The scheme presented in Fig. 13 shows the process of dividing the HR series into lagged sequences (lag = 3 in this example). This approach helps to observe how DI reflects the long-term behavior of HR, with an increasing lag. The prevalence of accelerations over decelerations (DI < 0) is a short-term phenomenon observed in HR transitions only when DI is obtained by lag = 1 (Fig. 7). By increasing the lag, DI starts to describe the same process that PI does—more frequent occurrence of HR accelerations (and thus DI > 0). The more points (accelerations) there are on the tachogram, the smaller the time difference is, and therefore, the deceleration input (DI) increases. Since higher lag makes DI more similar to PI, PI may be an index related to the sympathetic nervous system by indicating the long-term tendency in human HR.

The tachogram from Fig. 5 split into lagged (lag = 3) intervals graphs. Note DIi > 0 from the bottom panel–the deceleration prevails the acceleration in the highlighted transition, contributing to higher values of DI with the increase of lag.
We observed a similar tendency of HRA index ~ lag dependence in mothers; however, in the case of PI, the interpretation of this tendency might be different than in DI. The asymmetry observed in the majority of healthy populations is obtained by PI > 0.5 and, on the contrary, DI < 0.541,42,50. Therefore, DI changed its properties with increasing lag, while PI strengthened its properties with lag increase. Additionally, the maternal model showed significant dependence of HRA index (PI) on the state of the fetus indicating that active state decreases maternal PI (Table 4). This shows that fetal behavioral state influences the maternal HRA index.
The results of PRSA measures (AC, DC, and DR) dependency on GA (Fig. 10 and Table 6) show that the optimal values of s and T parameters to study those relations in fetal HR are s = T = 1. PRSA values obtained when s = 1 can be interpreted as mean ΔRR for accelerations (AC) and decelerations (DC). The correlation results show a clear dependence between PRSA values and gestational age in fetuses. On the other hand, the same comparison conducted for maternal HR reveals weaker yet still significant dependencies (Fig. 11). It is harder to establish optimal s and T parameters in this case since significant dependencies were obtained for higher values of both of those variables.
Our results indicate that DR shows a stronger correlation between maternal and fetal values and better reflects heart rate asymmetry than AC and DC. Furthermore, DR correlates more strongly (than DC or AC) with asymmetry indices such as GI, PI and EI (Table 9). This is consistent with previous studies, in which DR was effective in distinguishing FHR between preterm and term fetuses20. Another study demonstrated that DR displayed higher discriminatory power than AAC and ADC in distinguishing acidemic fetuses during labor21. This suggests that DR can provide insights into the autonomic nervous system’s regulation of fetal heart rate, potentially surpassing the discriminatory power of AC and DC in certain contexts. We suggest that the greater effectiveness of DR is due to its ability to account for non-stationarity and asymmetry in autonomic regulation, which may be crucial in the context of studies on fetal heart dynamics.
DR was originally introduced in order to emphasize the asymmetric growths and decay in HR arising during uterine contractions in labor21. Therefore, this parameter can be considered as one of the HRA measures. In the context of our study, DR performed similar to Poincaré-plot-based methods while comparing maternal results with GA (ρ = 0.330 in DID2A and ρ = 0.334 in DR) and maternal versus fetal results (ρ = 0.285 in DI and ρ = 0.247 in DR) and worse than Poincaré-plot-based indices in fetal results versus GA (ρ = 0.513 in EI and ρ = 0.210 in DR). However, the AC and DC performance in comparing fetal results versus GA (Fig. 10 and Table 6) makes PRSA a promising tool in terms of assessing fetal age based on the analysis of its heart rhythm. The non-linear nature of PRSA (Fig. 9) makes it hard to describe it with the use of the analogous methods as with HRA indices. Lopez–Justo et al. reports optimal DR results obtained within 40 ≤ T ≤ 5020. Stampalija et al. used T parameter up to 45 in order to evaluate its influence on AC and DC in fetuses19. The relation with age evaluated by the same group was postulated as quadratic18. In assessing the relationship between PRSA and GA, no evidence was found to suggest that the relationship is non-linear (the use of nonparametric methods, in this case, arose due to the outliers occurrence that would complicate a proper linear evaluation).
Since women over 30 years of age comprised a large part of our database, the potential influence of maternal age on the obtained results should be taken into account. Autonomic nervous system changes with age what may influence fetal development and, consequently, fetal HRV. Older mothers often exhibit distinct autonomic functions and stress responses compared to younger women, which can indirectly affect fetal HRV60. Advanced maternal age is also associated with specific hormonal and metabolic profiles that may impact fetal development and contribute to variations in HRV. For instance, alterations in insulin sensitivity or cortisol levels can influence fetal stress responses and subsequently affect HRV. Furthermore, women over 30 face an increased risk of pregnancy complications, which can modify the intrauterine environment and lead to changes in fetal HRV parameters. There are studies indicating that these complications, often linked to fetal growth restrictions, have been correlated with variations in specific HRV metrics, highlighting the potential impact of maternal age on fetal autonomic regulation61.
The findings from our study open promising paths for future research. Most importantly, the HRV patterns we have established in healthy fetuses could serve as reference points against which abnormal patterns might be detected. Future studies could investigate whether our methodological approach could be adapted for earlier detection of fetal distress, potentially identifying subtle changes in autonomic regulation before conventional monitoring methods detect problems.
Future research should focus on longitudinal measurements of fetal heart rate at multiple time points throughout gestation. By collecting HRV data at several gestational ages for the same fetuses, more precise analysis may be conducted of how these metrics change during pregnancy development. This longitudinal approach would allow for tracking individual developmental trajectories and potentially identify critical windows during which HRV parameters undergo significant changes.
The clinical utility of our approach could be enhanced by developing algorithms specifically designed to identify deviations from normal HRV patterns that might indicate emerging pathologies. This could be particularly valuable in high-risk pregnancies where early intervention is critical. These algorithms should include measures such as PRSA and DI (in the lag 1–4 range). Furthermore, longitudinal studies examining how prenatal HRV patterns correlate with postnatal development and long-term outcomes would provide valuable insights into the predictive value of fetal HRV analysis.
Limitations
While this study provides valuable insights into fetal HRA, it is important to acknowledge certain limitations. Firstly, this study is limited by the lack of consideration for fetal sex, which could potentially influence HRV. Additionally maternal age and BMI are factors associated with fetal development and cardiovascular health. Also, our study did not explicitly investigate ethnic, cultural, or demographic influences. These factors may play a role in heart rate asymmetry. Future research should address them to provide a more holistic view of fetal and maternal HR dynamics.
Conclusions
In this study, for the first time, a thorough analysis of fetal HRA based on ECG recordings was performed in such a large group and over such a wide range of gestational age. The asymmetry in HR is clearly noticeable during fetal development and diminishes as one progresses into adulthood. The PI might be an indicator associated with the sympathetic nervous system. A comprehensive analysis of the parameters of HRA measures was also performed to help future researchers choose their optimal values and assess the impact of their modification on the results. The optimal lag value for the most reliable interpretation of the fetal HRA results based on Poincaré plots falls within the [1, 4] range. The optimal values of PRSA parameters to use in the analysis of relations with gestational age are s = T = 1.
Data availability
The datasets presented in this article will be made available on request after adequate justification. Requests to access the datasets should be directed to A.K.
References
Cerritelli, F. et al. A review on the vagus nerve and autonomic nervous system during fetal development: Searching for critical windows. Front. Neurosci. 15, 721605 (2021).
Chatow, U., Davidson, S., Reichman, B. L. & Akselrod, S. Development and maturation of the autonomic nervous system in premature and full-term infants using spectral analysis of heart rate fluctuations. Pediatr. Res. 37, 294–302 (1995).
Ohta, T. et al. Alteration in the low-frequency domain in power spectral analysisof fetal heart beat fluctuations. FDT 14, 92–97 (1999).
Schneider, U. et al. Developmental milestones of the autonomic nervous system revealed via longitudinal monitoring of fetal heart rate variability. PLoS ONE 13, e0200799 (2018).
Krivova, Y. S., Proshchina, A. E., Otlyga, D. A., Leonova, O. G. & Saveliev, S. V. Prenatal development of sympathetic innervation of the human pancreas. Ann. Anat. Anatomischer Anzeiger 240, 151880 (2022).
Mulkey, S. B. & Plessis, A. D. The critical role of the central autonomic nervous system in fetal-neonatal transition. Semin. Pediatr. Neurol. 28, 29–37 (2018).
DuBose, T. J., Cunyus, J. A. & Johnson, L. F. Embryonic heart rate and age. J. Diagnos. Med. Sonogr. 6, 151–157 (1990).
Costa, M., Goldberger, A. L. & Peng, C.-K. Broken asymmetry of the human heartbeat: Loss of time irreversibility in aging and disease. Phys. Rev. Lett. 95, 198102 (2005).
Guzik, P., Piskorski, J., Krauze, T., Wykretowicz, A. & Wysocki, H. Heart rate asymmetry by Poincaré plots of RR intervals. Biomedizinische Technik/Biomed. Eng. 51, 272–275 (2006).
Pawłowski, R., Buszko, K., Newton, J. L., Kujawski, S. & Zalewski, P. Heart rate asymmetry analysis during head-up tilt test in healthy men. Front. Physiol. https://doi.org/10.3389/fphys.2021.657902 (2021).
Sibrecht, G., Piskorski, J., Krauze, T. & Guzik, P. Heart rate asymmetry, its compensation, and heart rate variability in healthy adults during 48-h Holter ECG recordings. J. Clin. Med. 12, 1219 (2023).
Fanelli, A., Magenes, G., Campanile, M. & Signorini, M. G. Quantitative assessment of fetal well-being through CTG recordings: A new parameter based on phase-rectified signal average. IEEE J. Biomed. Health Inform. 17, 959–966 (2013).
Hoyer, D. et al. Heart rate variability categories of fluctuation amplitude and complexity: diagnostic markers of fetal development and its disturbances. Physiol. Meas. 40, 064002 (2019).
Karmakar, C., Kimura, Y., Palaniswami, M. & Khandoker, A. Analysis of fetal heart rate asymmetry before and after 35 weeks of gestation. Biomed. Signal Process. Control 21, 43–48 (2015).
Porta, A. et al. Temporal asymmetries of short-term heart period variability are linked to autonomic regulation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 295, R550–R557 (2008).
Zalas, D., Bobkowski, W., Piskorski, J. & Guzik, P. Heart rate asymmetry in healthy children. JCM 12, 1194 (2023).
Voss, A., Schroeder, R., Heitmann, A., Peters, A. & Perz, S. Short-term heart rate variability—influence of gender and age in healthy subjects. PLoS ONE 10, e0118308 (2015).
Stampalija, T. et al. Brain sparing effect in growth-restricted fetuses is associated with decreased cardiac acceleration and deceleration capacities: A case–control study. BJOG Int. J. Obstetr. Gynaecol. 123, 1947–1954 (2016).
Stampalija, T. et al. Parameters influence on acceleration and deceleration capacity based on trans-abdominal ECG in early fetal growth restriction at different gestational age epochs. Eur. J. Obstetr. Gynecol. Reprod. Biol. 188, 104–112 (2015).
López-Justo, C. et al. Differences in the asymmetry of beat-to-beat fetal heart rate accelerations and decelerations at preterm and term active labor. Sensors 21, 8249 (2021).
Rivolta, M. W., Stampalija, T., Frasch, M. G. & Sassi, R. Theoretical value of deceleration capacity points to deceleration reserve of fetal heart rate. IEEE Trans. Biomed. Eng. 67, 1176–1185 (2020).
Rivolta, M. W., Barbieri, M., Stampalija, T., Sassi, R. & Frasch, M. G. Relationship between deceleration morphology and phase rectified signal averaging-based parameters during labor. Front. Med. 8, 626450 (2021).
Rivolta, M. W. et al. Acceleration and deceleration capacity of fetal heart rate in an in-vivo sheep model. PLoS ONE 9, e104193 (2014).
MATLAB version: 9.13.0 (R2022b). The MathWorks Inc. (2022).
Sato, M. et al. A novel extraction method of fetal electrocardiogram from the composite abdominal signal. IEEE Trans. Biomed. Eng. 54, 49–58 (2007).
Pan, J. & Tompkins, W. J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. BME-32, 230–236 (1985).
Sedghamiz, H. Matlab Implementation of Pan Tompkins ECG QRS Detector.
van Gent, P., Farah, H., van Nes, N. & van Arem, B. HeartPy: A novel heart rate algorithm for the analysis of noisy signals. Transp. Res. F Traffic Psychol. Behav. 66, 368–378 (2019).
Pearson, R. K. Data cleaning for dynamic modeling and control. in 1999 European Control Conference (ECC) 2584–2589 (IEEE, Karlsruhe, 1999). https://doi.org/10.23919/ECC.1999.7099714.
Van Laar, J. O. E. H., Porath, M. M., Peters, C. H. L. & Oei, S. G. Spectral analysis of fetal heart rate variability for fetal surveillance: Review of the literature. Acta Obstet. Gynecol. Scand. 87, 300–306 (2008).
Akselrod, S. et al. Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science 213, 220–222 (1981).
Samjeed, A., Wahbah, M., Khandoker, A. H. & Hadjileontiadis, L. Unsupervised Fetal Behavioral State Classification Using Non-Invasive Electrocardiographic Recordings. in 2021 Computing in Cardiology (CinC) 1–5 (IEEE, Brno, Czech Republic, 2021). https://doi.org/10.23919/CinC53138.2021.9662900.
Pillai, M. & James, D. The development of fetal heart rate patterns during normal pregnancy. Obstet. Gynecol. 76, 812 (1990).
Pillai, M. & James, D. Behavioural states in normal mature human fetuses. Arch. Dis. Child. 65, 39–43 (1990).
Brändle, J. et al. Heart rate variability parameters and fetal movement complement fetal behavioral states detection via magnetography to monitor neurovegetative development. Front. Hum. Neurosci. https://doi.org/10.3389/fnhum.2015.00147 (2015).
Brennan, M., Palaniswami, M. & Kamen, P. Do existing measures of Poincare plot geometry reflect nonlinear features of heart rate variability?. IEEE Trans. Biomed. Eng. 48, 1342–1347 (2001).
Piskorski, J. & Guzik, P. Asymmetric properties of long-term and total heart rate variability. Med. Biol. Eng. Comput. 49, 1289–1297 (2011).
Ehlers, C. L., Havstad, J., Prichard, D. & Theiler, J. Low doses of ethanol reduce evidence for nonlinear structure in brain activity. J. Neurosci. 18, 7474–7486 (1998).
Karmakar, C. K., Khandoker, A. & Palaniswami, M. Phase asymmetry of heart rate variability signal. Physiol. Meas. 36, 303–314 (2015).
Yan, C., Li, P., Yao, L., Karmakar, C. & Liu, C. Impacts of reference points and reference lines on the slope- and area-based heart rate asymmetry analysis. Measurement 137, 515–526 (2019).
Pawłowski, R., Buszko, K. & Zalewski, P. The Asymmetric Nature of Transitions in Heart Rate Variations (Tampere, 2022).
Pawłowski, R. & Buszko, K. The Analysis of Transitions in Heart Rate Variability Obtained from Photo Plethysmograph–A Novel Insight into Asymmetry. in (IEEE, Strbske Pleso, Vysoké Tatry, Slovakia, 2022). https://doi.org/10.1109/ESGCO55423.2022.9931361.
Piskorski, J. & Guzik, P. Asymmetric properties of long-term and total heart rate variability. Se2.4: The directionality of HRA. Med. Biol. Eng. Comput. 49, 1289–1297 (2011).
Bauer, A. et al. Deceleration capacity of heart rate as a predictor of mortality after myocardial infarction: Cohort study. Lancet 367, 1674–1681 (2006).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing (2022).
Bates, D., Maechler, M., Bolker, B. & Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 67, 1–48 (2015).
Nychka, D., Furrer, R., Paige, J. & Sain, S. fields: Tools for spatial data. (2021).
Soetaert, K. plot3D: Plotting Multi-Dimensional Data. (2021).
Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Springer-Verlag, 2016).
Guzik, P. et al. Asymmetric features of short-term blood pressure variability. Hypertens. Res. 33, 1199–1205 (2010).
Piskorski, J. & Guzik, P. Compensatory properties of heart rate asymmetry. J. Electrocardiol. 45, 220–224 (2012).
Piskorski, J. et al. Testing heart rate asymmetry in long, nonstationary 24 hour RR-interval time series. Physiol. Meas. 40, 105001 (2019).
Harteveld, L. M. et al. Maturation of the cardiac autonomic nervous system activity in children and adolescents. J. Am. Heart Assoc. 10, e017405 (2021).
Zeytinoglu, S., Calkins, S. D. & Leerkes, E. M. Autonomic nervous system functioning in early childhood: Responses to cognitive and negatively-valenced emotional challenges. Dev. Psychobiol. 62, 657–673 (2020).
Hornberger, L. K. & Sahn, D. J. Rhythm abnormalities of the fetus. Heart 93, 1294–1300 (2007).
Artal, R., Paul, R. H., Romem, Y. & Wiswell, R. Fetal bradycardia induced by maternal exercise. Lancet 324, 258–260 (1984).
Monga, M. Fetal heart rate response to maternal exercise. Clin. Obstet. Gynecol. 59, 568 (2016).
Zygmunt, A. & Stanczyk, J. Methods of evaluation of autonomic nervous system function. Arch. Med. Sci. 6, 11–18 (2010).
Karmakar, C. K., Khandoker, A. H., Gubbi, J. & Palaniswami, M. Complex correlation measure: A novel descriptor for poincaré plot. BioMed. Eng. OnLine 8, 17 (2009).
Braeken, M. A. K. A. et al. Pregnant mothers with resolved anxiety disorders and their offspring have reduced heart rate variability: Implications for the health of children. PLoS ONE 8, e83186 (2013).
Sharifi-Heris, Z., Rahmani, A. M., Axelin, A., Rasouli, M. & Bender, M. Heart rate variability and pregnancy complications: Systematic review. Interact. J. Med. Res. 12, e44430 (2023).
Author information
Authors and Affiliations
Contributions
Conceptualization, R.P. and A.K.; methodology, R.P., A.K. and K.B.; software, R.P. and F.A.A.; validation, R.P., A.K. and K.B.; formal analysis, R.P.; investigation, R.P. and A.K.; resources, A.K.; data curation, R.P., F.A.A. and A.S; writing–original draft preparation, R.P.; writing–review and editing, A.K. and K.B.; visualization, R.P.; supervision, A.K.; project administration, A.K.; funding acquisition, A.K. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pawłowski, R., Al-Ani, F., Samjeed, A. et al. Investigating asymmetry in fetal and maternal heart rate accelerations and decelerations. Sci Rep 15, 18887 (2025). https://doi.org/10.1038/s41598-025-00962-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-00962-y
