
Abstract
To explore the association between anxiety symptoms, BIS/BAS and the relationship between both and physical activity in college students. A cross-sectional research design was used to recruit 4962 current college students to fill out three scales: generalised anxiety, behavioural inhibition/activation system, and physical activity level, which were analysed using statistical methods such as independent samples t-tests, Pearson correlation coefficient analyses, canonical correlation analyses, and one-way analyses of variance (ANOVAs). Female students had a higher detection rate of anxiety symptoms (41.58%), higher reward responsiveness scores for female students and higher behavioural inhibition scores for male students. Behavioural inhibition and reward responsiveness were found to be canonical correlations of anxiety symptoms in college students. Among male students, behavioural inhibition was associated with nervousness and irritability, while reward responsiveness was associated with nervousness and worry too much. In female students, behavioural inhibition was associated with uncontrollable worrying, feeling afraid, while reward responsiveness was associated with nervousness, restlessness. The lower the level of physical activity, the higher the score of anxiety symptoms in male/female (p < 0.05). The higher the level of physical activity, the higher the score of reward responsiveness in the behavioural activation system of male/female students (P < 0.05); and the effect of the level of physical activity on the behavioural inhibition score of college students was non-linear. Intensity, duration and frequency of physical activity were negatively correlated with anxiety symptoms and positively correlated with reward responsiveness, but not with behavioural inhibition. For females, vigorous/high-intensity exercise with a duration greater than 30 min once a day was most effective in alleviating anxiety symptoms. For males, vigorous exercise lasting > 30 min, 3–5 times per week, was most effective in reducing anxiety symptoms. To improve reward responsiveness, females benefited most from vigorous exercise lasting > 30 min once a day, while males benefited most from vigorous exercise lasting > 60 min once a day. Behavioural inhibition and reward responsiveness were canonically correlated with anxiety symptoms in college students, with differences in canonical correlations between male and female college students. But both could improve behavioural inhibition and reward responsiveness, mitigate specific symptoms of anxiety by modulating physical activity levels.
Similar content being viewed by others
Introduction
Anxiety is an emotional state characterized by excessive and persistent worry1, often without a clear focus or direction2. Common symptoms include irritability, somatic tension, and insomnia3. Anxiety is among the most prevalent psychological issues in college students, with the detection rate rising from 16.6 to 34.8% over the past decade4, and continuing to increase in recent years5. This growing prevalence underscores the urgent need to identify effective strategies for alleviating anxiety and enhancing students’ well-being, academic performance, and personal development. The behavioral inhibition/activation system consists of the Behavioral Activation System (BAS) and the Behavioral Inhibition System (BIS)6. BIS/BAS is a theoretical model developed by psychologist Jeffrey Gray to describe how individuals respond to motivationally driven behaviour7. They are the two main motivational systems in the brain, which are associated with emotion regulation, behavioural responses, and an individual’s adaptive behaviour, respectively8. The BAS is sensitive to rewarding, non-punishing, and punishment-avoidant stimuli, leading to a tendency to approach incentive signals and contributing to positive emotional experiences. In contrast, the BIS is responsive to punishment, non-reward, and novelty stimuli, manifesting as withdrawal or avoidance in response to error signals, which inhibits behavioral responses and is associated with negative emotional experiences8,9. Therefore, abnormalities in the sensitivity of the BIS and BAS can result in behavioral and psychopathological issues, with anxiety being a prominent example10,11. Previous studies have shown that personality traits (BIS and BAS) account for all genetic variation in depressive and anxiety symptoms12. Neuroanatomically, BIS sensitivity is associated with gray matter volume (rGMV) in the parahippocampal region, while BAS sensitivity is linked to rGMV in the ventromedial prefrontal and inferior parietal regions. These findings suggest that brain regions associated with processing negative emotions and reward-related information may be linked to rGMV related to BIS and BAS13.
Evidence suggests that physical activity effectively promotes mental health, offering benefits such as high adherence, minimal side effects, and lasting results14,15. Cross-sectional studies have reported a negative association between physical activity and anxiety symptoms in college students 16,17, while longitudinal studies have confirmed significant reductions in anxiety scores after 6 weeks of regular exercise18. Research also indicates that moderate to high-intensity physical activity is positively associated with BAS19, while low-intensity activity is linked to BIS20. Furthermore, individuals with high BAS exhibit greater motivation to engage in physical activity and experience more positive emotional responses to exercise21. Neurobiological studies have shown that exercise increases cerebral blood flow22, upregulates neurotrophic factors23, enhances hypothalamic–pituitary–adrenal axis function24, and inhibits pro-inflammatory cytokine secretion25. These effects stimulate the central nervous system26, enhancing the behavioral activation system and helping alleviate negative emotions such as anxiety27.
A review of the existing literature indicates that physical activity can effectively alleviate anxiety symptoms28 and modulate the behavioral inhibition/activation system (BIS/BAS) in college students29. Previous studies have not examined whether the synchronization of behavioral inhibition and activation systems with anxiety symptoms exists in college students, nor clarified the relationship between physical exercise components and anxiety symptoms or BIS/BAS. The primary objective of this study was to investigate the synchrony between anxiety symptoms and the BIS/BAS systems; thus, canonical correlation analysis (CCA) was selected. Canonical correlation analysis is particularly suited for examining concurrent changes and associations between multidimensional variables, rather than establishing causal relationships. This approach contrasts with methods such as path analysis or structural equation modeling (SEM). Based on existing research and identified gaps, this study proposes three hypotheses: (a) Anxiety symptoms are synchronized with BIS/BAS. (b) Higher levels of physical activity are associated with lower anxiety symptom scores in college students. (c) Higher physical activity levels are associated with higher behavioral activation scores and lower behavioral inhibition scores. Although physical activity was a key aspect of this study, its potential to introduce complexity into the model led us to exclude it from the combined causal model of BIS/BAS and psychological symptoms. Instead, a one-way analysis of variance (ANOVA) was employed to compare groups with varying levels of physical activity. This decision aligns with the primary objective of the study, which was to elucidate the synchrony between BIS/BAS and anxiety symptoms. This study aims to test these hypotheses using a cross-sectional design, providing guidance for clinical identification and targeted interventions for anxiety and depression symptoms in college students, as well as offering insights for researchers and university administrators.
Research subjects and methods
Recruitment of subjects
The test had run from February to August 2024. College students were recruited from seven colleges and universities in Songjiang University City, Shanghai, according to a cross-sectional study design with randomised cluster sampling. The sample size was calculated using the formula: “n ≥ µα/2 * p * (1 − p)/δ2 * deff”30, where the significance level (α) was set at 0.05, the sampling tolerance (δ) at 0.03, and the design effect (deff) for cluster sampling at 3. Previous data indicated that the anxiety symptom detection rate was 24.215% for male college students and 25.146% for female students31. Based on these rates, the required sample size was calculated to be 2350 for male students and 2411 for female students, yielding a total sample size of 4761. Considering a balanced gender ratio at Songjiang University City and assuming a 5% attrition rate, a total of 5011 students were planned for recruitment. Sampling was performed on a class basis, with 125 classes selected to participate. Ultimately, 5125 college students volunteered, recruited through outreach by teachers and researchers who distributed the questionnaires.
Subjects in this study were current university students, and all subjects volunteered to take the test and signed an informed consent form. The informed consent was obtained from all subjects and/or their legal guardians. The study was approved by the university ethics committee. Name of ethics committee: Ethics Review From for Studies at School of Education, SISU. Ethics number: SISUGJ2024015. The research have been performed in accordance with the Declaration of Helsinki. We confirm that all research was performed in accordance with relevant guidelines/regulations.
Questionnaire survey process and quality control:
-
(1)
Pre-test procedures Researchers underwent centralized training to ensure familiarity with the inclusion and exclusion criteria for participant selection. Only individuals meeting the inclusion criteria and not the exclusion criteria were included in the study, with participants assigned numbers based on their order of inclusion. Researchers were trained on standardized procedures for administering each screening scale, ensuring accurate real-time data recording. Before completing the survey, participants were provided with instructions, the study’s purpose was explained, and any questions were addressed. Participants were informed that the data would be used solely for scientific research and that their responses should be honest, independent, and voluntary. They were also informed of their right to withdraw from the study at any time.
-
(2)
During the test: Researchers prompted participants to respond according to the provided instructions.
-
(3)
Post-test procedures Researchers reviewed the completed questionnaires for missing items or responses inconsistent with common sense. Missing or incorrect responses were addressed to ensure the completeness, accuracy, and truthfulness of the data. Questionnaires with completion times under 3 min, patterned responses, or those failing to meet the inclusion/exclusion criteria were excluded to maintain a high effective response rate.
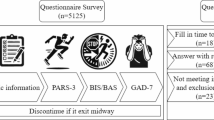
The specific process is outlined in Fig. 1.

Flowchart of the test process with the inclusion and exclusion process.
Inclusion Criteria (1) Aged 18–24 years; (2) Right-handed; (3) No history of mental illness and no current use of psychotropic drugs; (4) No chronic physical conditions, no history of brain injury, and no visual impairments.
Exclusion Criteria (1) Age outside the inclusion range; (2) Left-handedness; (3) Long-term or recent use of psychotropic drugs, drugs affecting physical mobility, cholinergics, or similar substances; (4) Severe cardiovascular disease, major organic disorders, or impaired vision or hearing that would prevent completion of the test.
Test instruments
General information questionnaire
This questionnaire collects basic demographic and lifestyle information from the study subjects, including age, gender, height, weight, smoking and drinking habits, one child, and single parents.
Physical activity rating scale-3 (PARS-3)
The PARS-3, developed by Kimio Hashimoto and revised by Deqing Liang32, demonstrates good reliability and validity33. This scale primarily assesses physical activity over the past month, focusing on intensity, duration, frequency, and overall volume. Physical activity is rated across three dimensions: intensity, duration, and frequency. The scoring system includes a 5-point scale for intensity and frequency (ranging from 1 to 5), and a 5-point scale for duration (ranging from 0 to 4). The total score is calculated as: Activity = Intensity * Duration * Frequency. The score range is 0–100, with low-intensity activity defined as 19 or below, moderate-intensity activity ranging from 20 to 42, and high-intensity activity defined as 43 or above. In this study, the Cronbach’s α coefficient for the questionnaire was 0.651.
Behavioral inhibition/activation system scale (BIS/ BAS)
The Behavioral Inhibition/Activation System (BIS/BAS) scale was originally developed by Carver and White in 199434 and later revised by Li Yanzhang et al. in China7. The revised scale consists of four dimensions: behavioral inhibition and three behavioral activation dimensions—reward responsiveness, drive, and fun seeking—comprising 18 items in total. The scale uses a four-point Likert scoring system, with responses ranging from 1 (strongly disagree) to 4 (strongly agree). The total score for reward responsiveness and drive ranges from 4 to 16, while the total score for fun seeking and behavioral inhibition ranges from 5 to 20. Higher scores indicate a stronger tendency in the corresponding dimension. In this study, the Cronbach’s α coefficient for the BIS/BAS scale was 0.908, with 0.902 for the BAS subscale and 0.796 for the BIS subscale.
Generalized anxiety disorder 7-item scale (GAD-7)
Anxiety symptoms were assessed using the Generalized Anxiety Disorder 7-item scale (GAD-7), developed by Spitzer et al. based on the diagnostic criteria from the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), and later revised by Yu Wang et al. The GAD-7 is one of the most widely used tools for anxiety measurement in clinical practice and research35,36. Studies both domestically and internationally have demonstrated the high reliability and validity of the GAD-7 in anxiety screening37,38,39,40. The GAD-7 requires respondents to report the frequency of seven core symptoms of generalized anxiety disorder over the past two weeks, with response options ranging from "not at all" to "nearly every day" (scored 0 to 3). The seven core symptoms are: nervousness (GAD1), uncontrollable worrying (GAD2), worry too much (GAD3), trouble relaxing (GAD4), restlessness (GAD5), irritability (GAD6), and feeling afraid (GAD7). The total score is the primary statistic, with higher scores indicating more severe anxiety. Scores range from 0 to 21, with the following categories: 0–4 indicating no anxiety or subclinical anxiety, 5–9 indicating mild anxiety, 10–14 indicating moderate anxiety, and 15–21 indicating severe anxiety. In this study, the Cronbach’s α coefficient for the GAD-7 was 0.939.
Mathematical and statistical methods
All statistical analyses were performed using SPSS 29.0 software. A two-tailed test was used with a significance level of α = 0.05. Continuous data are presented as mean ± standard deviation, and categorical data are expressed as percentages, with results rounded to two decimal places. Independent sample t-tests were used to compare the age, BMI, BIS/BAS, anxiety symptoms, and physical activity levels between male and female college students (significant differences). Chi-square tests were used to compare drinking habits (significant), smoking habits (significant), only-child status (not significant), and single-parent status (not significant) between male and female students. Pearson correlation coefficients were used to analyze the relationship between BIS/BAS and anxiety symptoms. The primary objective of this study was to investigate the synchrony between anxiety symptoms and the BIS/BAS systems. To this end, canonical correlation analysis (CCA) was employed, as it is well-suited for examining concurrent relationships and associations among multidimensional variables, rather than establishing causal links. Canonical correlation analysis was employed to extract statistically significant variable pairs, using their correlation coefficients to assess the degree of relationship between canonical variables, followed by examining their loadings to test their contributions to the respective canonical variables. Canonical redundancy analysis was used to evaluate the explanatory power of the canonical variables. Descriptive statistics were used to describe anxiety and BIS/BAS scores. To avoid the complexity of causal modeling, physical activity variables were excluded from the combined causal model for BIS/BAS and psychological symptoms. Instead, a one-way analysis of variance (ANOVA) was conducted to compare BIS/BAS and anxiety symptoms across different levels of physical activity (exercise intensity, frequency, and duration). Descriptive statistics were used to summarize the anxiety and BIS/BAS scores for different physical activity dimensions.
Results
Basic characteristics of the subjects
Anxiety symptoms were observed in 35.17% of male participants and 41.58% of female participants. As shown in Table 1, males scored significantly lower than females on most dimensions of the Generalized Anxiety Disorder scale (all P < 0.001). However, males scored higher than females on drive and fun seeking (P < 0.05), but lower on reward responsiveness (both P < 0.001). Additionally, male students reported significantly higher levels of physical activity, including greater exercise intensity, duration, and frequency (all P < 0.001). To minimize potential bias, data were analyzed separately for male and female college students.
Relationship between BIS/BAS, anxiety symptoms in college students
Pearson correlation analyses were conducted to examine the relationships between the BIS/BAS dimensions and anxiety symptoms among college students, as shown in Table 2. Significant negative correlations were observed between the BIS/BAS dimensions and the anxiety scale dimensions for both male and female college students (all P < 0.001). In female students, a significant positive correlation was found between the behavioral inhibition dimension and anxiety scale dimensions (P < 0.001). Among male students, no significant correlations were observed between behavioral inhibition and the anxiety symptoms of uncontrollable worrying (r = − 0.023, P = 0.272), worry too much (r = − 0.035, P = 0.095), irritability (r = − 0.028, P = 0.174), and feeling afraid (r = − 0.030, P = 0.141). However, all other anxiety symptoms were significantly positively correlated with behavioral inhibition (all P < 0.001). Strong negative correlations were found between the drive and anxiety symptoms in both male and female students (r < − 0.210, P < 0.001), representing the strongest association in the study. Significant correlations were also observed between most other BIS/BAS dimensions and anxiety symptoms, laying the groundwork for subsequent canonical correlation analyses.
Canonical correlation analysis was performed to explore the relationship between the BIS/BAS and anxiety symptom dimensions, as shown in Table 3. Four pairs of canonical variables were extracted for each group. In female students, the first three pairs were significant (all P < 0.001), with canonical correlation coefficients of 0.431, 0.157, and 0.138, respectively. In male students, the first three pairs were significant (all P < 0.05), with canonical correlation coefficients of 0.418, 0.130, and 0.079, respectively. Due to the lower coefficient of the third pair in both groups, only the first two pairs were further analyzed.
As shown in Fig. 2, among male college students, the canonical variables u1 and u2 exhibited higher loading coefficients for behavioural inhibition (0.736) and reward responsiveness (1.553), respectively. The canonical variable v1 had higher loading coefficients for nervousness (0.233) and irritability (0.213), while v2 showed higher loading coefficients for nervousness (1.057) and worry too much (0.866). These findings suggest that dysfunction in behavioural inhibition in male students may be more strongly associated with the symptoms of nervousness and irritability, while dysfunction in reward responsiveness may be more closely linked to nervousness and worry too much. In males, the BIS/BAS is more strongly correlated with the anxiety symptoms of nervousness, irritability, and worry too much. Furthermore, within these anxiety symptoms, the three symptoms demonstrated a more synchronous manifestation.

Canonical correlation analysis load coefficient.
Among female college students, the canonical variables u1 and u2 exhibited higher loading coefficients for behavioural inhibition (0.874) and reward responsiveness (1.283), respectively. The canonical variable v1 had higher loading coefficients for uncontrollable worrying (0.298) and feeling afraid (0.237), while v2 showed higher loading coefficients for nervousness (0.760) and restlessness (0.757). These findings suggest that dysfunction in behavioural inhibition in female students may be more strongly associated with the symptoms of uncontrollable worrying and feeling afraid, whereas dysfunction in reward responsiveness may be more closely linked to the symptoms of nervousness and restlessness. The BIS/BAS system exhibited a stronger association with uncontrollable worrying, feeling afraid, nervousness, and restlessness among anxiety symptoms in female students. Furthermore, within these anxiety symptoms, the four symptoms demonstrated a more synchronous manifestation.
The above results validate hypothesis (a).
The loading coefficients for both behavioural inhibition and reward responsiveness functions were higher in both genders, indicating that these two functions are more strongly associated with anxiety symptoms within the behavioural inhibition and activation system.
As shown in Table 4, the first canonical redundancy for male BIS/BAS was 50.90%, and for male anxiety symptoms, it was 80.10%. The second canonical redundancy for male BIS/BAS was 13.20%, while for male anxiety symptoms, it was 7.30%. For female BIS/BAS and anxiety symptoms, the first canonical redundancy was 33.40% and 79.00%, respectively, while the second canonical redundancy was 13.20% for female BIS/BAS and 4.60% for female anxiety symptoms.
Relationship between BIS/BAS, anxiety symptoms, and physical activity in college students
One-way ANOVA and descriptive statistics were used to compare and describe the scores on the anxiety scale, Behavioral Inhibition and Activation scales, and their subdimensions among college students with different levels of physical activity. The results are presented in Table 5 and Fig. 3.

Comparison of anxiety symptoms and BIS/BAS scores between male and female college students with varying physical activity levels. G1 Nervousness, G2 Uncontrollable Worrying, G3 Worry too much, G5 Restlessness, G6 Irritability, G7 Feeling Afraid. A1 Reward Responsiveness, I1 Behavioral Inhibition System.
As male students’ physical activity levels decrease, their GAD-7 scores increase. Specifically, the low activity group exhibited higher scores for nervousness, worry too much, and irritability compared to the medium and high activity groups. Among male students in the low activity group, excessive worry had the highest score, while nervousness was most prominent in the medium activity group. These findings suggest that worry too much may be the primary manifestation of anxiety symptoms in male students with low physical activity levels, while nervousness is more prevalent in those with moderate activity levels.
For female students, as physical activity levels decrease, GAD-7 scores increase, with a significant difference in anxiety scores between the low and medium activity groups (P < 0.05). Specifically, the low activity group scored significantly higher on nervousness, uncontrollable worrying, restlessness, and feeling afraid compared to the medium activity group. Within each group, nervousness was the most prominent symptom across all physical activity levels. These findings suggest that nervousness may be the primary manifestation of anxiety in female students.
Between groups, higher levels of physical activity were associated with increased reward responsiveness in the BIS/BAS system for both male and female students. Additionally, the relationship between physical activity levels and behavioral inhibition scores was non-linear. Females consistently exhibited higher mean scores for reward responsiveness than males across all activity levels, while males had higher mean scores for behavioral inhibition. These findings suggest that enhanced reward responsiveness may be the primary benefit of physical activity on the BIS/BAS in females, whereas reduced behavioral inhibition may be the key benefit of moderate physical activity levels in males.
The above results verify hypotheses (b) and (c).
As shown in Table 6, the intensity, duration, and frequency of physical activity were positively correlated with reward responsiveness, negatively correlated with anxiety symptoms, and showed no significant correlation with behavioral inhibition in both male and female college students. Specifically, in female students, nervousness was negatively correlated with intensity and duration, but not with frequency. Similarly, uncontrollable worrying in female students was negatively correlated with duration, but showed no significant correlation with intensity or frequency.
The potential non-linear relationship between physical activity, anxiety, and reward responsiveness in college students was further examined using line graphs. As shown in Fig. 4, reward responsiveness was highest in females engaging in high-intensity exercise (> 30 min, 1 time/day). In contrast, vigorous exercise combined with > 60 min of activity resulted in the lowest G1 scores in females. G2 scores were lowest in females with > 60 min of physical activity, while the lowest G5 scores were observed with vigorous exercise (31–59 min, 1 time/day). Finally, the lowest G7 scores were recorded in females engaging in high-intensity exercise for > 60 min, 1–7 times/week.

Relationship between physical activity and anxiety symptoms and BIS/BAS among college students. G1 Nervousness, G2 Uncontrollable worrying, G3 Worry too much, G5 Restlessness, G6 Irritability, G7 Feeling afraid, A1 Reward responsiveness.
For males, high exercise intensity (> 60 min, 1 time/day) was associated with the highest reward responsiveness. Vigorous or higher intensity exercise, > 60 min, 3–5 times/week, resulted in the lowest G1 scores. Vigorous exercise intensity (31–59 min, 1 time/day) was linked to the lowest G3 scores, while the lowest G6 scores were observed in males with vigorous exercise intensity (31–59 min, 1–5 times/week).
In conclusion, high exercise intensity (> 30 min, 1 time/day) had the most beneficial effect on female reward responsiveness, while high exercise intensity (> 60 min, 1 time/day) was most beneficial for male reward responsiveness. Vigorous or high exercise intensity (> 30 min, 1 time/day) was most effective for anxiety intervention in females, while vigorous exercise intensity (> 30 min, 3–5 times/week) was most effective for anxiety intervention in males.
Discussion
The present study found a high prevalence of anxiety symptoms among college students, with a higher prevalence in female students compared to males. A previous study on the mental health of 7,143 Chinese college students reported anxiety symptom detection rates of 25.146% for females and 24.215% for males31, partially supporting the findings of the current study41.
The association between anxiety symptoms and the BIS/BAS system in college students is a key area of research. The present study confirmed a significant relationship between anxiety symptoms and the BIS/BAS through canonical correlation analysis, aligning with findings from previous studies42,43,44. Hypothesis (a) was validated, with similar conclusions drawn in prior cross-sectional studies. Previous research has identified strong associations between behavioral inhibition45,46 and behavioral activation—particularly reward responsiveness—and anxiety symptoms through large-scale studies47,48. For instance, David et al. found that females exhibited higher BIS sensitivity and lower BAS tendencies on the BAS/BIS scale in a sample of 2208 subjects, suggesting that females may be more predisposed to anxiety symptoms49. Shaunt’s study also revealed a link between BAS-reward responsiveness and anxiety in a cross-sectional analysis of 459 college students50. More detailed conclusions are provided in previous review studies. Additionally, Charles found that BIS dysfunction was associated with nervousness symptoms based on a literature review51. Building on these findings, the current study contributes novel insights by highlighting gender differences in the manifestation of these associations. Specifically, in males, behavioral inhibition dysfunction might be more closely linked to nervousness and irritability, while reward responsiveness dysfunction could be associated with nervousness and worry too much. In females, behavioral inhibition dysfunction may be more strongly correlated with uncontrollable worry and fear, while reward responsiveness dysfunction might be linked to nervousness and restlessness. These findings provide an important addition to the existing literature, offering valuable insights for the diagnosis and treatment of anxiety symptoms and suggesting that specific dysfunctions may require tailored intervention strategies.
This study shows that higher levels of physical activity are associated with lower anxiety symptom scores in college students52, consistent with previous cross-sectional studies, thus validating hypothesis (b)16,53. This study further revealed that the manifestations of anxiety symptoms varied by gender and physical activity levels in college students. Specifically, worry too much was the predominant anxiety symptom in male students with low physical activity, while nervousness was the primary symptom in those with medium activity levels. In female students, nervousness consistently emerged as the main anxiety symptom, regardless of physical activity level. These findings offer new directions for exercise interventions targeting emotional well-being in college students. Additionally, the study found that the intensity, duration, and frequency of physical activity were negatively correlated with anxiety symptoms, supporting results from previous research. Similar conclusions have been mentioned in previous review and experimental studies. Singh et al. conducted a systematic review of 77 studies and concluded that higher intensity physical activity was more effective in alleviating anxiety15. Similarly, Xin et al. found that engaging in low-to-high-intensity physical activity twice a week improved anxiety symptoms, based on an analysis of 26 different prescribed therapies54. Building on these findings, The present study suggests that vigorous or high-intensity exercise (≥ 30 min, once a day) could be the most effective intervention for anxiety in female students, while vigorous exercise (≥ 30 min, 3–5 times per week) may be the most effective intervention for male students. Numerous studies have explored the biological mechanisms underlying these effects55, revealing that exercise can prevent and alleviate anxiety symptoms by increasing serum BDNF levels56, modulating the autonomic nervous system (ANS) 46, decreasing heart rate variability (HRV) 57, and reducing parasympathetic nervous system activity26,27,58. Furthermore, the psychological mechanisms may include improvements in self-efficacy43, self-esteem59, and reductions in anxiety sensitivity, all of which contribute to the alleviation of negative emotions60,61.
The present study demonstrated that higher levels of physical activity were associated with higher scores in behavioural activation-reward responsiveness among college students29, while the relationship between physical activity and behavioural inhibition scores was found to be non-linear62, consistent with prior research. This finding partially validates hypothesis (c). The present study suggests that there may be gender- and activity level-specific benefits for the BIS/BAS. Specifically, increased reward responsiveness could be the primary benefit of physical activity for female students’ BIS/BAS, while decreased behavioral inhibition might be the main benefit of moderate physical activity for male students. Additionally, the study found that the intensity, duration, and frequency of physical activity were positively correlated with reward responsiveness but showed no significant correlation with behavioral inhibition63, partially corroborating previous findings19. Similar conclusions have been reported in previous cross-sectional and experimental studies. The study suggests that high-intensity physical activity (> 30 min, once a day) may have the greatest impact on reward responsiveness in female students, while the same duration of physical activity (> 60 min) could be most effective for male students. Previous studies have highlighted brain regions involved in behavioral inhibition and activation, such as the ventral striatum, hippocampus, hypothalamus, and insula64. Physical exercise has been shown to enhance behavioral activation by increasing left frontal cortical activity65 and to reduce behavioral inhibition by decreasing right frontal cortical activation66. These findings provide further insight into the neurobiological mechanisms underlying the effects of physical activity on the BIS/BAS system.
This study suggests that physical activity might enhance sensitivity to reward responsiveness in behavioral activation while possibly reducing sensitivity to behavioral inhibition. Additionally, it emphasizes the importance of considering gender-specific differences in physical activity dosage to effectively alleviate anxiety symptoms and related negative emotions in college students. The results provide scientific evidence for anxiety interventions in college students and suggest that detailed exercise plans can facilitate personalized interventions and optimize the design of university sports curricula.
Limitations
-
(1)
The measurement tools used in this study were all self-report questionnaires, which may introduce subjective bias. Future research could benefit from incorporating objective assessment tools, such as accelerometers and heart rate monitors, to evaluate physical activity, along with psychologist interviews and EEG-magnetoencephalography for a more accurate assessment of anxiety symptoms.
-
(2)
Anxiety symptoms in this study were assessed using the Generalized Anxiety Disorder Scale. However, as anxiety can be divided into state and trait anxiety, the findings may not apply to all anxiety-related groups. Future studies could categorize anxiety symptoms more specifically based on their nature and source to enhance the specificity and applicability of the results.
-
(3)
The advantage of cross-sectional studies lies in their ability to analyze large numbers of individuals or groups simultaneously, making them useful for describing group characteristics. However, they have certain limitations: since data are collected at a single time point, causal relationships between variables cannot be established, and only correlations can be identified. Additionally, cross-sectional studies reflect data from a specific time point and cannot capture temporal changes or long-term effects. Future research should integrate multiple methods (applied research, review studies, theoretical research) based on the field’s characteristics to further explore physical activity, anxiety symptoms, and BIS/BAS in college students.
Conclusion or recommendation
College students’ BIS/BAS functions are significantly correlated with anxiety symptoms, and physical activity has been shown to improve both BIS/BAS functioning and anxiety symptoms. The effects of physical activity on these variables vary by intensity, duration, and frequency, with notable gender differences. It is recommended that universities encourage students experiencing anxiety to increase physical activity, while also considering gender-specific exercise intensity and dosage to enhance reward responsiveness in behavioral activation and reduce behavioral inhibition, thereby alleviating anxiety symptoms.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Abi-Dargham, A. et al. Candidate biomarkers in psychiatric disorders: State of the field. World Psychiatry 22(2), 236–262 (2023).
Crocq, M.-A. The history of generalized anxiety disorder as a diagnostic category. Dialogues Clin. Neurosci. 19(2), 107–115 (2017).
Norbury, R. & Evans, S. Time to think: Subjective sleep quality, trait anxiety and university start time. Psychiatry Res. 271, 214–219 (2019).
Lipson, S. K. et al. Trends in college student mental health and help-seeking by race/ethnicity: Findings from the national healthy minds study, 2013–2021. J. Affect. Disord. 306, 138–147 (2022).
Zeng, W. et al. Prevalence of mental health problems among medical students in China. A meta-analysis. Medicine 98(18), e15337 (2019).
Carver, C. S. & White, T. L. Behavioral-inhibition, behavioral activation, and affective responses to impending reward and punishment: The bis bas scales. J. Pers. Soc. Psychol. 67(2), 319–333 (1994).
Li, Y. Z. et al. Reliability analysis of the Chinese version of the behavioural inhibition/activation system scale (BIS/BAS). Chin. Ment. Health J. 08, 613–616 (2008).
Scholten, M. R. M. et al. Behavioral inhibition system (BIS), behavioral activation system (BAS) and schizophrenia: Relationship with psychopathology and physiology. J. Psychiatr. Res. 40(7), 638–645 (2006).
Johnson, S. L., Turner, R. J. & Iwata, N. BIS/BAS levels and psychiatric disorder: An epidemiological study. J. Psychopathol. Behav. Assess. 25(1), 25–36 (2003).
Xie, J. L. et al. Behavioral inhibition/activation systems and depression among females with substance use disorder: The mediating role of intolerance of uncertainty and anhedonia. Front. Psychiatry 12, 644882 (2021).
Liu, Y. et al. The relationship between physical activity and internet addiction among adolescents in western China: A chain mediating model of anxiety and inhibitory control. Psychol. Health Med. 29(9), 1602–1618 (2024).
Takahashi, Y. et al. Etiological pathways of depressive and anxiety symptoms linked to personality traits: A genetically-informative longitudinal study. J. Affect. Disord. 291, 261–269 (2021).
Li, Y. et al. Gender-specific neuroanatomical basis of behavioral inhibition/approach systems (BIS/BAS) in a large sample of young adults: A voxel-based morphometric investigation. Behav. Brain Res. 274, 400–408 (2014).
Hallgren, M. et al. Treatment guidelines for depression: Greater emphasis on physical activity is needed. Eur. Psychiatry 40, 1–3 (2017).
Singh, B. et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. Br. J. Sports Med. 57(18), 1203–1208 (2023).
Xiang, M. Q. et al. Relationship of physical activity with anxiety and depression symptoms in Chinese college students during the COVID-19 outbreak. Front. Psychol. 11, 582436 (2020).
Liu, Y. et al. Physical activity moderated the mediating effect of self-control between bullying victimization and mobile phone addiction among college students. Sci. Rep. 14(1), 71494 (2024).
Ji, C. et al. Physical exercise ameliorates anxiety, depression and sleep quality in college students: experimental evidence from exercise intensity and frequency. Behav. Sci. 12(3), 61 (2022).
Malik, A. A. et al. Influence of personality and self-efficacy on perceptual responses during high-intensity interval exercise in adolescents. J. Appl. Sport Psychol. 33(6), 590–608 (2021).
Voigt, D. C. et al. Carver and White’s (1994) BIS/BAS scales and their relationship to risky health behaviours. Pers. Individ. Differ. 47(2), 89–93 (2009).
Motl, R. W., Mcauley, E. & Distefano, C. Is social desirability associated with self-reported physical activity?. Prev. Med. 40(6), 735–739 (2005).
Klein, T. et al. Cerebral blood flow during interval and continuous exercise in young and old men. Med. Sci. Sports Exerc. 51(7), 1523–1531 (2019).
Kruk, J., Kotarska, K. & Aboul-Enein, B. H. Physical exercise and catecholamines response: Benefits and health risk: possible mechanisms. Free Radic. Res. 54(2–3), 105–125 (2020).
Cherian, K., Schatzberg, A. F. & Keller, J. HPA axis in psychotic major depression and schizophrenia spectrum disorders: Cortisol, clinical symptomatology, and cognition. Schizophr. Res. 213, 72–79 (2019).
Paolucci, E. M. et al. Exercise reduces depression and inflammation but intensity matters. Biol. Psychol. 133, 79–84 (2018).
Ma, K. et al. Progress in the study of the intervention effect and mechanism of exercise on depression. China Sport Sci. Technol. 56(11), 13–24 (2020).
Chen, M. et al. Progress in the study of neurobiological mechanisms related to the improvement of depression by sports exercise. China Sport Sci. Technol. 57(04), 89–97 (2021).
Ashdown-Franks, G. et al. Exercise as medicine for mental and substance use disorders: A meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med. 50(1), 151–170 (2020).
Schneider, M. L. & Graham, D. J. Personality, physical fitness, and affective response to exercise among adolescents. Med. Sci. Sports Exerc. 41(4), 947–955 (2009).
Zheng, W. J. & He, F. Sample size calculations for fact-finding missions. Prev. Med. 32(06), 647–648 (2020).
Cao, W. et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 287, 112934 (2020).
Liang, D. Q. Stress levels and their relationship with physical activity among university students. Chin. Ment. Health J. 01, 5–6 (1994).
Ren, Y. & Li, M. Influence of physical exercise on social anxiety of left-behind children in rural areas in China: The mediator and moderator role of perceived social support. J. Affect. Disord. 266, 223–229 (2020).
Heubeck, B. G., Wilkinson, R. B. & Cologon, J. A second look at Carver and White’s (1994) BIS/BAS scales. Pers. Individ. Differ. 25(4), 785–800 (1998).
Dear, B. F. et al. Psychometric comparison of the generalized anxiety disorder scale-7 and the Penn State Worry Questionnaire for measuring response during treatment of generalised anxiety disorder. Cogn. Behav. Ther. 40(3), 216–227 (2011).
Toussaint, A. et al. Sensitivity to change and minimal clinically important difference of the 7-item generalized anxiety disorder questionnaire (GAD-7). J. Affect. Disord. 265, 395–401 (2020).
Spitzer, R. L. et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166(10), 1092–1097 (2006).
Plummer, F. et al. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 39, 24–31 (2016).
Sousa, T. V. et al. Reliability and validity of the Portuguese version of the generalized anxiety disorder (GAD-7) scale. Health Qual. Life Outcomes 13, 244 (2015).
Wang, Y., Chen, R. & Zhang, L. A reliability study of the Generalised Anxiety Scale-7 in Chinese general hospital inpatients. J. Clin. Psychiatry 28(03), 168–171 (2018).
Li, L. et al. Canonical correlation analysis of depression and anxiety symptoms among college students and their relationship with physical activity. Sci. Rep. 13(1), 38682 (2023).
Ito, R. et al. Interaction effects of behavioral inhibition system/behavioral activation system and cost/probability biases on social anxiety. Front. Psychol. 10, 2536 (2019).
Xu, Z. & Du, J. A mental health informatics study on the mediating effect of the regulatory emotional self-efficacy. Math. Biosci. Eng. MBE 18(3), 2775–2788 (2021).
Jung, W. H. et al. Sex differences in the behavioral inhibition system and ventromedial prefrontal cortex connectivity. Soc. Cogn. Affect. Neurosci. 17(6), 571–578 (2022).
Heym, N. & Lawrence, C. The role of Gray’s revised RST in the P-psychopathy continuum: The relationships of Psychoticism with a lack of fear and anxiety, and increased impulsivity. Pers. Individ. Differ. 49(8), 874–879 (2010).
Wilborn, D. D. et al. Should I stay or should I go? Approach/avoidance conflict and emotional functioning. Personal. Ment. Health 12(4), 298–308 (2018).
Dong, Z. et al. The relationship between physical activity and trait anxiety in college students: The mediating role of executive function. Front. Hum. Neurosci. 16, 9540 (2022).
Arfaie, A. et al. Assessment of behavioral approach and behavioral inhibition systems in mood disorders. Basic Clin. Neurosci. 9(4), 261–268 (2018).
Pagliaccio, D. et al. Revising the BIS/BAS scale to study development: Measurement invariance and normative effects of age and sex from childhood through adulthood. Psychol. Assess. 28(4), 429–442 (2016).
Arkarian, S. A. et al. A model of BIS/SAS sensitivity, emotion regulation difficulties, and depression, anxiety, and stress symptoms in relation to sleep quality. Psychiatry Res. 210(1), 281–286 (2013).
Carver, C. S. Negative affects deriving from the behavioral approach system. Emotion 4(1), 3–22 (2004).
Liu, Y. et al. The chain mediating effect of anxiety and inhibitory control between bullying victimization and internet addiction in adolescents. Sci. Rep. 14(1), 74132 (2024).
Wang, P. et al. Relationship between physical activity levels and depressive symptoms in college students: aa pathway of action analysis based on resting EEGs. J. Shanghai Univ. Sport 47(04), 51–60 (2023).
Luan, X. et al. Exercise as a prescription for patients with various diseases. J. Sport Health Sci. 8(5), 422–441 (2019).
Bettariga, F. et al. Exercise training mode effects on myokine expression in healthy adults: A systematic review with meta-analysis. J. Sport Health Sci. 13(6), 764–779 (2024).
Stroehle, A. et al. Acute exercise ameliorates reduced brain-derived neurotrophic factor in patients with panic disorder. Psychoneuroendocrinology 35(3), 364–368 (2010).
Stubbs, B. et al. An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis. Psychiatry Res. 249, 102–108 (2017).
Xia, J. et al. PGC-1α-mediated ‘myoencephalic crosstalk’ and the antidepressant mechanism of exercise: Reflections and perspectives based on integrative biology. J. Shanghai Univ. Sport 41(04), 57–64 (2017).
Sabo, A. et al. The validity and reliability of the Malay version of the social support for exercise and physical environment for physical activity scales. PLoS ONE 15(9), e0239725 (2020).
Radak, Z. et al. The complex role of physical exercise and reactive oxygen species on brain. J. Sport Health Sci. 2(2), 87–93 (2013).
Wang, W. L. & Liu, H. R. The mediating role of behavioral systems in linking physical activity and anxiety symptoms in college students. Sci. Rep. 15(1), 91924 (2025).
Firoozjah, M. H. et al. Behavioral activation/inhibition systems and lifestyle as predictors of mental disorders in adolescent athletes during Covid19 pandemic. BMC Public Health 22(1), 13816 (2022).
Liu, Y. et al. The chain mediating effect of anxiety and inhibitory control and the moderating effect of physical activity between bullying victimization and internet addiction in Chinese adolescents. J. Genet. Psychol. 1, 1–16 (2025).
Guyer, A. E. et al. Probing the neural correlates of anticipated peer evaluation in adolescence. Child Dev. 80(4), 1000–1015 (2009).
Broelz, E. K. et al. The neurobiology of placebo effects in sports: EEG frontal alpha asymmetry increases in response to a placebo ergogenic aid. Sci. Rep. 9, 38898 (2019).
Liu, G. X. et al. The effect of convergence/avoidance motivation on the choice of time-motion perspective. Chin. J. Clin. Psychol. 31(01), 63–68 (2023).
Author information
Authors and Affiliations
Contributions
Wenli Wang: Methodology; Investigation; Data Collection; Data Analysis; Literature Review; Discussion Writing; Writing Original Draft. Hairong Liu: Conceptualization; Technical Support; Language Editing; Project Administration; Final Proofreading.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, W., Liu, H. Canonical correlation analysis of anxiety symptom and behavioral inhibition/activation system among college students and their relationship with physical activity. Sci Rep 15, 17547 (2025). https://doi.org/10.1038/s41598-025-01499-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01499-w
