
Abstract
Obesity, defined as having a Body Mass Index (BMI) of 30 kg/m² or above, has emerged as a major public health challenge worldwide, and Iran is no exception. This study aimed to examine the socioeconomic and behavioral factors associated with obesity prevalence in Iran by gender from 2006 to 2019, and predict future trends at both national and subnational levels up to 2040. Obesity rates from 31 provinces in Iran between 2006 and 2019 were obtained from the Iran Statistical Yearbook. Spatio-temporal modeling was applied to assess gender-specific factors influencing obesity at the provincial level. Predictions for future obesity trends were generated using spatiotemporal forecasting techniques. Female obesity was significantly associated with divorce (β = 0.239), urbanization (β = 0.035), internet usage (β = 0.040), Log GDP (β = 3.195), and soft drink consumption (β = 0.153). In contrast, male obesity was significantly related to marriage (β = 0.059), divorce (β = 0.124), urbanization (β = 0.012), Log GDP (β = 1.079), soft drink intake (β = 0.002), tobacco usage (β = 0.217), and meat consumption habits (β = 0.030). Spatiotemporal predictions indicate a continued rise in obesity prevalence over the next two decades, with female obesity projected to reach 52.84% by 2040 and male obesity expected to rise to 33.40%. Mazandaran Province is predicted to have the highest obesity rates in 2040, affecting 72.57% of women and 48.21% of men, whereas Sistan and Baluchistan will likely exhibit the lowest obesity prevalence (37.66% in women and 21.43% in men). The findings highlight the urgent need for policy interventions to address the rising prevalence of obesity in Iran. Given the significant socioeconomic and behavioral determinants identified, targeted public health initiatives, lifestyle modifications, and regulatory policies are essential to mitigate the long-term impact of obesity on the healthcare system and overall public health.
Similar content being viewed by others

Introduction
The prevalence of obesity, defined as a body mass index (BMI) of 30 kg/m2 or more, has been increasing globally in recent years, particularly in low- and middle-income countries1,2. In 2016, the worldwide obesity rate among adults was 13%, with higher prevalence rates among women (15.3%) than men (11.1%)3,4. In Iran, the prevalence of obesity among men and women in 2016 was 18.4% and 36.8%, respectively, representing a significant increase from 19905. Obesity is a leading cause of disability and premature mortality, reducing quality of life and increasing the risk of cardiovascular diseases, diabetes, and cancer. It also results in higher healthcare costs for countries6,7,8,9.
Obesity is a complex issue and associated with biological, psychological, behavioral, environmental and socioeconomic status (SES)8,9,10,11,12. Age, sex, urbanization, income13,14, marital status, education level, employment15,16, smoking and alcohol consumption, physical activity17,18,19, and dietary patterns9,20,21 are among the factors related to the prevalence of obesity. However, the influence of SES on the prevalence of obesity is different and is sometimes inconsistent across countries. For instance, while a study in the United States found that obesity chances increased with decreasing levels of education and income20, studies in Turkey and Botswana reported that obesity chances increased with increasing levels of education and income16,22. Gender also plays a significant role in the relationship between SES and obesity, with determinants varying by gender15,23. The impact of SES on obesity has been found to differ between men and women in various studies. For example, a study in rural China reported that women with low education and men with high per capita income had a higher prevalence of obesity23. Another study across 31 countries found that moderate or light smoking in men was inversely associated with obesity, while daily consumption of fruits and vegetables was protective against obesity in men but not in women24. In Mexico, obesity was increased in men with a high level of education and in women with a high wealth index25. So, failing to consider gender differences in the relationship between SES and obesity could lead to inappropriate targeting of populations for reducing obesity prevalence23.
Globalization has led to changes in socioeconomic conditions, including the increase in urbanization rates and disposable income, and has changed lifestyles, which affect the incidence of obesity26. To tackle obesity, we must first fully understand its prevalence and future trends at the global and national levels27. On the other hand, the spatial and temporal dimensions are crucial in epidemiological studies of disease spread or health outcomes, and should be taken into account during analysis28. Bayesian spatio-temporal modeling has recently been used to estimate the relationship between environmental predictors, socioeconomic factors, and obesity in both men and women1,8,29. Given that health policymakers require reliable evidence on the prevalence and distribution of obesity risk factors in both women and men to fulfill global and national obligations in non-communicable disease risk reduction, prevention, and control. However, there is no research that comprehensively analyzes the temporal and spatial trends of obesity in the world and Iran and makes predictions for the future. This study aims to study gender differences in the prevalence of obesity among adults in Iran using the Bayesian spatio-temporal model and predict the prevalence of obesity until 2040 at both national and subnational level of Iran.
Methods
Study design
This study employs a Spatio-temporal bayesian modeling approach to predict the prevalence of obesity (BMI ≥ 30 kg/m²) in individuals aged 20 and older across 31 provinces of Iran from 2020 to 2040. The model integrates historical obesity prevalence data (2006–2019) and socioeconomic and behavioral covariates to estimate future trends.
Data sources and variables
Dependent variable (outcome)
The outcome variable is obesity prevalence, defined as BMI ≥ 30 kg/m² based on the World Health Organization (WHO) criteria30. Data on obesity prevalence by sex and province were obtained from the STEPS national survey (2006–2019)31.
Independent variables (predictors)
The explanatory variables included socioeconomic factors and behavioral determinants, selected based on prior research on obesity risk factors. These variables were collected from the Iran Statistical Yearbook (2006–2019)32.
Definition of variables
Socioeconomic Factors
Provincial income and economic development were indicated by GDP. The urbanization rate was measured by the percentage of people who are inhabitants of urban areas in each province. Unemployment rate was calculated by the proportion of unemployed residents in the total resident population aged 15 years or above. Family changed was shown by divorce rate which was referenced by the number of divorces per 1000 married female residents. The marriage rate in each province was defined as the number of marriages per one thousand people per year. The percentage of households that have access to the internet was a proxy of internet usage.
Behavioral determinants
Average annually household expenditures spent on fruit and vegetables, dairy products, meat, sugar, oil, soft drinks, and tobacco were measured as an indicator of food and tobacco consumption of the households. The information related to these variables was also extracted from the statistical yearbooks of each province from the website of the Statistical Center of Iran32.
Variable selection and data processing
Variables were selected through a literature review, identifying factors significantly associated with obesity prevalence. Missing data were handled using imputation techniques, and if a variable lacked sufficient data coverage, it was excluded.
Statistical modeling
Time-series forecasting of covariates (2020–2040)
To predict the future values of socioeconomic and behavioral variables, we employed Autoregressive Integrated Moving Average (ARIMA) models for each covariate separately across all 31 provinces and two gender groups.
-
The optimal autoregressive (AR) and moving average (MA) components were selected automatically using R programming to enhance predictive accuracy.
-
Forecasts of covariates were generated for 2020 to 2040.
-
Then these predicted covariates were then integrated into the spatio-temporal obesity prediction model.
Spatio-temporal bayesian modeling of obesity prevalence
To analyze long-term provincial trends in obesity, we employed a spatio-temporal bayesian hierarchical model, which is particularly suitable for data with both geographic and temporal structure. This framework enables the simultaneous modeling of variations over space and time and allows for more precise estimates, especially in the presence of spatial correlation and unobserved heterogeneity. Compared to classical regression or MCMC-based Bayesian methods, the Integrated Nested Laplace Approximation (INLA) approach offers faster computation and reliable approximation of posterior distributions, making it appropriate for our large-scale, high-dimensional dataset. We have a Spatio-temporal model which the data are defined with space (i) and time (t) indexed. Allowing interaction between space and time (\(\delta it\)), the model is formulated using the following specification:
Let yit denote the prevalence of obesity in province i at year t which follows a Gaussian distribution. In this model, X is the matrix of covariates, β represents fixed effect coefficients, (ui+vi) are structured and unstructured spatial random effects, (\(\:{{\upgamma\:}}_{t}+{\varphi\:}_{t}\)) are structured and unstructured temporal random effects and \(\:{\delta\:}_{it}\:\)captures space–time interaction.
Bayesian Estimation Framework
-
Priors: A non-informative exchangeable prior was assigned to the accuracy parameters to minimize bias. The prior distribution for random effects was assumed as:
Log Gamma (1, 0.0005).
-
Parameter Estimation: The model was implemented using Integrated Nested Laplace Approximation (INLA) within the INLA package in R (version 3.6.1).
Model validation and sensitivity analysis
-
Cross-validation: The model’s predictive performance was assessed using Root Mean Squared Error (RMSE) and Akaike Information Criterion (AIC).
-
Sensitivity analysis: Conducted to examine the robustness of predictions under varying socioeconomic scenarios.
Prediction of obesity prevalence (2020–2040)
Using the fitted spatio-temporal model, gender-specific obesity prevalence was predicted for all 31 provinces from 2020 to 2040, incorporating:
-
1.
Predicted socioeconomic and behavioral covariates (ARIMA models).
-
2.
Spatio-temporal bayesian modeling (INLA framework).
All analyses and predictions were performed in R software, ensuring robust and reproducible forecasting of obesity trends in Iran.
Results
As illustrated in Fig. 1, obesity prevalence exhibited an increasing trend over the 14-year period for both sexes. However, females consistently showed a higher prevalence of obesity compared to males throughout the study period. Specifically, the obesity prevalence in 2006 was 10.51% for men and 22.62% for women. By 2019, these rates had risen to 20.55% for men and 40.17% for women, reflecting a notable increase in obesity rates for both genders over the study period.

The prevalence rate of obesity by sex in Iran in the period of 2006–2019.
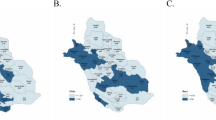
Based on the Fig. 2, in almost all provinces, the prevalence of obesity is higher in women than in men across most regions in 2019. Overall, the lowest and highest rate of obesity prevalence was observed in Sistan & Baluchistan (male obesity: %11.87, female obesity: %26.25) and Mazandaran (Male obesity: %27.45, female obesity: %50.74), respectively.

Mean prevalence of obesity among men and women by province in 2019.
The provided Table 1 enumerates that the marriage rate had a significantly positive effect on male obesity. As a result, per 1 unit increase in the marriage rate, the prevalence of obesity among men increased by %0.05. Moreover, a 1 unit increase in urbanization rate increased significantly male obesity by 0.012%. Additionally, the prevalence of obesity among men increased by % a 1.07 per one unit increase in GDP. Variables such as fruit and vegetable consumption, dairy consumption, and oil consumption have an adverse but not significant correlation with obesity in males. Soft drink consumption illustrated a direct and statistically significant correlation with male obesity, which means that a %0.002 rise in body weight was associated with a 1 unit rise in soft drink consumption. Per unit increase in smoking rate linked to a %0.21 rise in the prevalence of obesity among men. The effect of meat consumption on male obesity was positive and significant (0.03).
Based on the result of Table 2, the divorce rate had a positive and significant relationship with obesity among women. Therefore, the per unit increase in divorce rate increased significantly the rates of obesity by %0.02. Similarly, for a percentage increase in the urbanization rate, a %0.03 increase in the prevalence of female obesity was observed. Regarding the impacts of internet use on female obesity, a per unit increase in the percentage of internet users was significantly associated with a %0.04 increase in obesity prevalence. Likewise, obesity prevalence in women increased by %3.9 as the GDP grew by 1 unit. Variables such as fruit and vegetable consumption, oil consumption, and dairy products have an adverse association with the prevalence of obesity among women, but they were not significant. Furthermore, soft drink consumption had a positive and significant correlation with obesity prevalence among women. For a 1% increase in the consumption of soft drinks, there was a %0.15 increase in the prevalence of female obesity. Moreover, factors including marriage rate, unemployment rate, tobacco intake, and meat consumption have a direct link with female obesity, but they were not significant.
According to Table 3, there is a consistent increase in obesity prevalence (BMI ≥ 30) among Iranian women across all provinces from 2020 to 2040. In 2020, Tehran had the highest obesity prevalence at 55.33%, which is projected to rise to 68.75% by 2040. Similarly, Mazandaran had an initial obesity prevalence of 46.55% in 2020, and this is expected to increase significantly to 72.57% by 2040, indicating a considerable rise over the 20-year period.
Conversely, South Khorasan and Sistan & Baluchistan had the lowest obesity rates among Iranian women, starting at 31.86% and 31.64%, respectively, in 2020. These rates are expected to rise to 48.57% and 37.66%, respectively, by 2040. Nationally, the obesity prevalence in Iranian women is projected to rise from 40.25% in 2020 to 52.84% in 2040, reflecting a substantial increase in the overall burden of obesity across the country. Certain provinces, including Isfahan, Alborz, and Tehran, are expected to see particularly sharp increases in obesity rates. These provinces are predicted to experience more than a 10% increase in obesity prevalence over the next 20 years.
Based on the Table 4, the prevalence of obesity among Iranian men is expected to increase steadily from 21.04% in 2020 to 33.40% in 2040. The growth reflects a compounded increase over the 20-year period, highlighting an urgent need for national-level preventive programs. The province of Mazandaran exhibits the highest predicted obesity rate, rising from 28.30% in 2020 to 48.21% in 2040. In contrast, Sistan and Baluchistan maintain the lowest prevalence, increasing from 12.83 to 21.43% over the same period.
As the data indicate, Ardabil (26.27–43.28%), Yazd (22.37–40.42%), and Mazandaran (28.30–48.21%) show the most significant relative increases. Isfahan, Kermanshah, and Alborz exhibit moderate growth, with projected increases of approximately 13–14% over two decades. Sistan and Baluchistan (12.83–21.43%) and Ilam (17.46–27.69%) demonstrate the slowest growth, albeit with consistent upward trends.
Subsequently, the projected obesity prevalence maps for men and women in different provinces of Iran up to the year 2040 are displayed in Figs. 3 and 4, demonstrating an upward trend in obesity prevalence across all provinces, as indicated by the maps.

The projected obesity prevalence among Iranian women across various provinces of Iran by 2040 (Researcher’s calculations).

The projected obesity prevalence among Iranian men across various provinces of Iran by 2040 (Researcher’s calculations).
Discussion
In the present study, we observed a significant increase in obesity rates across all provinces from 2020 to 2040. Overall, the prevalence of obesity was higher among females compared to males, which is consistent with other research findings33,34. However, some conducted studies suggested that obesity prevalence is more prevalent among men35,36. Gender differences in obesity prevalence can be attributed to hormonal variations between males and females, genetic factors, and eating habits. For instance, women tend to consume more calorie-dense foods37,38.
Regarding socioeconomic determinants, our findings indicate a positive correlation between marriage rate and obesity, which was confirmed by previous studies39,40. Although this relationship was not statistically significant for women.
Some authors suggest that weight gain after marriage or cohabitation may be due to increased opportunities for shared, regular meals with larger portion sizes, decreased physical activity, and reduced focus on weight maintenance for attracting an intimate partner40,41,42.
Moreover, As previously reported42, there was observed a positive association between divorce or marital dissolution and an increased risk of obesity in both females and males. Divorced individuals often exhibit poorer health behaviors such as smoking, alcohol use, and depression which are known predictors of obesity43,44.
Moreover, we found a significant positive association between urbanization rates and obesity prevalence in both genders, consistent with past research36,45,46. The sedentary lifestyle commonly found among city dwellers, combined with the scarcity of physical activity opportunities due to desk jobs, can be identified as the cause45. According to certain research, the occurrence of obesity is increasing at a higher rate in rural regions compared to urban areas22,47.
In terms of behavioral factors, we found a positive association between internet use and obesity prevalence in both sexes, which was align with some previous studies9,21,36,48 however, this association was not significant among men. Despite our result, one study reported a negative association49. The intensive use of the internet contributes to a lack of physical inactivity, increased consumption of snacks, sleep deprivation, and indirectly results in obesity48.
Similar to previous research50,51,52, we observed a significant and positive relationship between GDP (as a proxy of income) and the prevalence of obesity in men and women. As individuals’ incomes rise, they gain the ability to afford an abundance of food beyond basic survival needs, resulting in increased nutrient intake50. Additionally, as a country’s economy becomes more industrialized, the food sector often shifts towards processed and fast foods, which are linked to higher obesity rates53.
However, some studies contradict these findings54,55.
Consumption of sugary beverages, including soft drinks, has been consistently linked to excess weight and an increased risk of obesity in both men and women, supported by previous studies56,57. The presence of liquid carbohydrates in these drinks reduces the feeling of fullness, causing inadequate energy compensation during subsequent meals. The elevated fructose levels found in corn syrup used in soda may have a specific impact on the risk developing of adiposity58,59.
Tobacco use has also been associated with weight gain and an increased risk of obesity in both sexes, although this relationship was not meaningful in women60,61. In contrast, some published studies reported a negative effect of smoking on obesity24,36,46. Heavy smokers tend to have higher body weight, potentially due to a combination of risky behaviors such as low physical activity, poor diet, and smoking62,63,64. Furthermore, a protein-rich diet has been linked to greater weight among both males and females, this association was not significant in females, consistent with previous findings65,66. However, some evidence suggests that meat intake has been beneficial in weight loss67. Mechanistically, meat is a source of saturated fat energy content but a lower percentage of protein, along with elevated levels of obesogenic elements such as nitrosamine and sodium68.
Projected obesity trends and public health implications
The findings of the spatiotemporal prediction models indicate a significant increase in obesity prevalence in Iran over the next two decades, posing substantial implications for public health and the national healthcare system. According to the results, obesity prevalence among Iranian women is projected to rise from 40.25% in 2020 to 52.84% in 2040, highlighting a concerning upward trend at the national level. A similar pattern is observed among men, with obesity rates increasing steadily from 21.04% in 2020 to 33.40% in 2040. This substantial increase in obesity prevalence, particularly among women, underscores the urgent need for targeted preventive interventions and health policies. By 2040, Mazandaran Province is projected to have the highest obesity rates in Iran, with 72.57% of women and 48.21% of men affected. In contrast, Sistan and Baluchistan will experience the lowest obesity rates, with 37.66% of women and 21.43% of men being obese. These projections are in line with global trends, where the prevalence of obesity has been steadily increasing across both developed and developing nations.
In 2010, the obesity prevalence in Brazil was reported at 16% among men and 14% among women. Using statistical modeling and trend analysis, projections indicate that by 2050, these rates will rise significantly, reaching 46% in men and 20% in women69. Similarly, a study conducted in Mexico utilized time-series forecasting methods to estimate future obesity trends. The findings revealed that in 2010, 27% of men and 37% of women were classified as obese, with projections suggesting a rise to 54% in men and 57% in women by 205070.
Furthermore, Keaver and et al. employed demographic and epidemiological projection models to predict obesity trends in Ireland. Their study estimated that the prevalence of overweight and obesity in men, which stood at 74% in 2010, would escalate to 89% by 2030. Likewise, obesity rates among women were predicted to surge from 57% in 2010 to 85% by 203071. In South Korea, Baik and et al. applied dynamic simulation modeling and regression-based forecasting to project obesity prevalence among adults up to 2030. Their analysis estimated that by 2020, obesity rates would be 47% in men and 32% in women, with a further increase to 62% in men and 37% in women by 203072.
Finkelstein and et al., using regression models, predicted that obesity prevalence in the United States would reach 51% by 203073. Similarly, a study conducted in Russia employed longitudinal cohort modeling to estimate future obesity trends. The findings projected that the prevalence of overweight and obesity in men would rise from 21% in 2010 to 76% by 2050, while in women, it would slightly decline from 58% in 2010 to 54% in 205074.
Wang and et al. conducted a study using econometric forecasting models to predict the prevalence of obesity and its associated economic burden in the United States and the United Kingdom. Their projections indicated that in the United States, obesity rates among men would increase from 32% in 2007–2008 to 50–51% by 2030, while in women, the prevalence would rise from 35% to 45–52%. Similarly, projections for the United Kingdom, based on trend analysis and dynamic simulation modeling, estimated that obesity prevalence among men would grow from 26% to 41–48% by 2030, while among women, it would rise from 26% to 35–43%75.
The collective findings of these studies underscore that obesity is a complex and multifactorial public health challenge, influenced by a dynamic interplay of dietary transitions, rapid urbanization, declining physical activity levels, socioeconomic disparities, and gaps in public health policies. The persistent rise in obesity prevalence across diverse populations highlights the urgent necessity for comprehensive, evidence-based interventions that address both individual and structural determinants of obesity69,70,71,72,73,74,75.
Limitations
Spatiotemporal studies serve as valuable analytical tools for examining trends, disparities, and the underlying determinants of obesity; however, they are subject to several methodological limitations. First, spatiotemporal studies typically employ aggregate-level data, such as national, regional, or provincial statistics, which may not accurately reflect individual-level associations, potentially leading to ecological fallacies. Second, spatiotemporal models often depend on underlying statistical and computational assumptions, including stationarity, normality, and independence, which may not always be applicable to complex real-world scenarios. Moreover, due to lack of consistent population data across provinces and years, total provincial GDP was used as a proxy for economic status instead of GDP per capita, which may influence the interpretation of economic disparities.
Conclusion
This study highlights the increasing prevalence of obesity at both national and subnational levels in Iran from 2020 to 2040, with a higher prevalence observed among females. The rise in obesity rate was linked to various factors, including being female, being married, divorce rate, living in urban areas, the economic development of each province, and accordingly behavioral and lifestyle changes (such as using the internet, soft drink intake, tobacco consumption, and meat usage).
To mitigate the escalating obesity epidemic, policymakers and public health authorities must prioritize multi-sectoral strategies, including the implementation of robust nutritional guidelines, the promotion of active lifestyles targeted educational initiatives, and regulatory measures to improve food environments. A concerted global effort is essential to curb this growing health crisis, ensuring sustainable and equitable solutions that enhance population health outcomes worldwide.
Data availability
The data underlying the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- GDP:
-
Gross Domestic Product
- BMI:
-
Body Mass Index
- SES:
-
Socioeconomic Status
- WHO:
-
World Health Organization
- ARIMA:
-
Autoregressive Integrated Moving Average
- AR:
-
Autoregressive
- MA:
-
Moving Average
References
Ikeda, N. et al. Trends and disparities in adult body mass index across the 47 prefectures of Japan, 1975–2018: A Bayesian Spatiotemporal analysis of National household surveys. Front. Public. Health. 10 (2022).
Sun, Y. et al. Spatial patterns of childhood obesity prevalence in relation to socioeconomic factors across England. ISPRS Int. J. Geo-Information. 9 (10), 599 (2020).
World Health Statistics. [ (2019). Available from: https://www.who.int/data/gho/publications/world-health-statistics
Faka, A. et al. Identifying determinants of obesity in Athens, Greece through global and local statistical models. Spat. spatio-temporal Epidemiol. 29, 31–41 (2019).
Djalalinia, S. et al. Levels and trends of BMI, obesity, and overweight at National and sub-national levels in Iran from 1990 to 2016; a comprehensive pooled analysis of half a million individuals. Arch. Iran. Med. 24 (5), 344–353 (2021).
Patil, G. R. & Sharma, G. Overweight/obesity relationship with travel patterns, socioeconomic characteristics, and built environment. J. Transp. Health. 22, 101240 (2021).
Karaketir, Ş. G. et al. Overweight and obesity in preschool children in Turkey: A multilevel analysis. J. Biosoc. Sci. 55 (2), 344–366 (2023).
Amegbor, P. et al. Individual and contextual predictors of overweight or obesity among women in Uganda: a spatio-temporal perspective. GeoJournal 1–21 (2021).
Mohajeri, M. et al. Some behavioral risk factors of obesity in Ardabil–Iran adults. Obes. Med. 18, 100167 (2020).
Spinosa, J. et al. From socioeconomic disadvantage to obesity: the mediating role of psychological distress and emotional eating. Obesity. 27 (4), 559–564 (2019).
Wardle, J. et al. Sex differences in the association of socioeconomic status with obesity. Am. J. Public Health. 92 (8), 1299–1304 (2002).
Sobal, J. & Stunkard, A. J. Socioeconomic status and obesity: a review of the literature. Psychol. Bull. 105 (2), 260 (1989).
Chigbu, C. O. et al. Prevalence and sociodemographic determinants of adult obesity: a large representative household survey in a resource-constrained African setting with double burden of undernutrition and overnutrition. J. Epidemiol. Community Health. 72 (8), 702–707 (2018).
Biswas, T. et al. The prevalence of underweight, overweight and obesity in Bangladeshi adults: data from a National survey. PloS One. 12 (5), e0177395 (2017).
Pou, S. A. et al. Sociodemographic disparities and contextual factors in obesity: updated evidence from a National survey of risk factors for chronic diseases. Public Health. Nutr. 25 (12), 3377–3389 (2022).
Karaoglan, D. & Tansel, A. Determinants of obesity in Turkey: a quantile regression analysis from a developing country. Available SSRN 2900125. (2017).
Haejung, C. Effects of smoking, drinking, and urban environment on obesity in Seoul, Korea. Iran. J. Public. Health. 49 (2), 230 (2020).
Daw, J., Margolis, R. & Wright, L. Emerging adulthood, emergent health lifestyles: sociodemographic determinants of trajectories of smoking, binge drinking, obesity, and sedentary behavior. J. Health Soc. Behav. 58 (2), 181–197 (2017).
Ding, D., Gebel, K., Phongsavan, P., Bauman, A. E. & Merom, D. Driving: a road to unhealthy lifestyles and poor health outcomes. PloS One. 9 (6), e94602 (2014).
Shaikh, R. A., Siahpush, M., Singh, G. K. & Tibbits, M. Socioeconomic status, smoking, alcohol use, physical activity, and dietary behavior as determinants of obesity and body mass index in the united States: findings from the National health interview survey. Int. J. MCH AIDS. 4 (1), 22 (2015).
Cureau, F., Sparrenberger, K., Bloch, K., Ekelund, U. & Schaan, B. Associations of multiple unhealthy lifestyle behaviors with overweight/obesity and abdominal obesity among Brazilian adolescents: a country-wide survey. Nutr. Metabolism Cardiovasc. Dis. 28 (7), 765–774 (2018).
Keetile, M. et al. Socioeconomic and behavioural determinants of overweight/obesity among adults in Botswana: a cross-sectional study. Bmj Open. 9 (12), e029570 (2019).
Pan, M. et al. Associations of socioeconomic status and physical activity with obesity measures in rural Chinese adults. Front. Public. Health. 8, 594874 (2021).
Pengpid, S. & Peltzer, K. Associations between behavioural risk factors and overweight and obesity among adults in population-based samples from 31 countries. Obes. Res. Clin. Pract. 11 (2), 158–166 (2017).
Quezada, A. D. & Lozada-Tequeanes, A. L. Time trends and sex differences in associations between socioeconomic status indicators and overweight-obesity in Mexico (2006–2012). BMC Public. Health. 15, 1–10 (2015).
Fox, A., Feng, W. & Asal, V. What is driving global obesity trends? Globalization or modernization? Globalization Health. 15, 1–16 (2019).
Gao, L. et al. Spatial–temporal trends in global childhood overweight and obesity from 1975 to 2030: a weight mean center and projection analysis of 191 countries. Globalization Health. 19 (1), 53 (2023).
Berger, U. Spatial and Temporal Dimensions of Health: A Statistical-epidemiological Perspective (München, Ludwig-Maximilians-Universität, 2021).
Sartorius, B. et al. Spatial-temporal trends and risk factors for undernutrition and obesity among children (< 5 years) in South Africa, 2008–2017: findings from a nationally representative longitudinal panel survey. BMJ Open. 10 (4), e034476 (2020).
World Health Organization. Obesity and overweight. (2018). https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. 2018.
System, D. V. Available From: https://vizit.report/panel/metabolic/en/main.html#/forestLocation
Statistical Center of Iran (SCI). (2020). Available from: https://www.amar.org.ir/salnameh-amari.
Cooper, A. J., Gupta, S. R., Moustafa, A. F. & Chao, A. M. Sex/gender differences in obesity prevalence, comorbidities, and treatment. Curr. Obes. Rep. :1–9. (2021).
Muhammad, T., Boro, B., Kumar, M. & Srivastava, S. Gender differences in the association of obesity-related measures with multi-morbidity among older adults in India: evidence from LASI, Wave-1. BMC Geriatr. 22 (1), 1–12 (2022).
Kim, K-B. & Shin, Y-A. Males with obesity and overweight. J. Obes. Metabolic Syndrome. 29 (1), 18 (2020).
Shiri, M. S., Emamgholipour, S., Heydari, H., Fekri, N. & Karami, H. The effect of human development index on obesity prevalence at the global level: A Spatial analysis. Iran. J. Public. Health (2023).
Kanter, R. & Caballero, B. Global gender disparities in obesity: a review. Adv. Nutr. 3 (4), 491–498 (2012).
Mauvais-Jarvis, F. et al. Sex and gender: modifiers of health, disease, and medicine. Lancet 396 (10250), 565–582 (2020).
Liu, J. et al. Marriage contributes to higher obesity risk in China: findings from the China health and nutrition survey. Annals Translational Med. ;9(7). (2021).
The, N. S. & Gordon-Larsen, P. Entry into romantic partnership is associated with obesity. Obesity 17 (7), 1441–1447 (2009).
Averett, S. L., Sikora, A. & Argys, L. M. For better or worse: relationship status and body mass index. Econ. Hum. Biology. 6 (3), 330–349 (2008).
Sobal, J., Rauschenbach, B. & Frongillo, E. A. Marital status changes and body weight changes: a US longitudinal analysis. Soc. Sci. Med. 56 (7), 1543–1555 (2003).
Torvik, F. A., Gustavson, K., Røysamb, E. & Tambs, K. Health, health behaviors, and health dissimilarities predict divorce: results from the HUNT study. BMC Psychol. 3, 1–9 (2015).
Umberson, D., Liu, H. & Powers, D. Marital status, marital transitions, and body weight. J. Health Soc. Behav. 50 (3), 327–343 (2009).
Hajian-Tilaki, K. & Heidari, B. Prevalence of obesity, central obesity and the associated factors in urban population aged 20–70 years, in the North of Iran: a population‐based study and regression approach. Obes. Rev. 8 (1), 3–10 (2007).
Tabrizi, J. S., Sadeghi-Bazargani, H., Farahbakhsh, M., Nikniaz, L. & Nikniaz, Z. Prevalence and associated factors of overweight or obesity and abdominal obesity in Iranian population: a population-based study of Northwestern Iran. Iran. J. Public. Health. 47 (10), 1583 (2018).
Rising rural body. -mass index is the main driver of the global obesity epidemic in adults. Nature 569 (7755), 260–264 (2019).
Matusitz, J. & McCormick, J. Sedentarism: the effects of internet use on human obesity in the united States. Social Work Public. Health. 27 (3), 250–269 (2012).
Qiu, Y. et al. Electronic media device usage and its associations with BMI and obesity in a rapidly developing City in South China. Front. Public. Health :950. (2021).
Grecu, A. M. & Rotthoff, K. W. Economic growth and obesity: findings of an obesity Kuznets curve. Appl. Econ. Lett. 22 (7), 539–543 (2015).
Larose, S. L., Kpelitse, K. A., Campbell, M. K., Zaric, G. S. & Sarma, S. Does obesity influence labour market outcomes among working-age adults? Evidence from Canadian longitudinal data. Econ. Hum. Biology. 20, 26–41 (2016).
Talukdar, D., Seenivasan, S., Cameron, A. J. & Sacks, G. The association between National income and adult obesity prevalence: empirical insights into Temporal patterns and moderators of the association using 40 years of data across 147 countries. PloS One. 15 (5), e0232236 (2020).
Canella, D. S. et al. Ultra-processed food products and obesity in Brazilian households (2008–2009). PloS One. 9 (3), e92752 (2014).
Bentley, R. A., Ormerod, P. & Ruck, D. J. Recent origin and evolution of obesity-income correlation across the united States. Palgrave Commun. ;4(1). (2018).
Kim, T. J. & von dem Knesebeck, O. Income and obesity: what is the direction of the relationship? A systematic review and meta-analysis. BMJ Open. 8 (1), e019862 (2018).
González-Morales, R. et al. Soft drink intake is associated with weight gain, regardless of physical activity levels: the health workers cohort study. Int. J. Behav. Nutr. Phys. Activity. 17 (1), 1–10 (2020).
Kim, J-M. & Lee, E. Association between soft-drink intake and obesity, depression, and subjective health status of male and female adults. Int. J. Environ. Res. Public Health. 18 (19), 10415 (2021).
Malik, V. S., Pan, A., Willett, W. C. & Hu, F. B. Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am. J. Clin. Nutr. 98 (4), 1084–1102 (2013).
Teff, K. L. et al. Dietary Fructose reduces Circulating insulin and leptin, attenuates postprandial suppression of Ghrelin, and increases triglycerides in women. J. Clin. Endocrinol. Metabolism. 89 (6), 2963–2972 (2004).
Alkeilani, A. A. et al. Association between waterpipe smoking and obesity: Population-based study in Qatar. Tob. Induc. Dis. ;20. (2022).
Dare, S., Mackay, D. F. & Pell, J. P. Relationship between smoking and obesity: a cross-sectional study of 499,504 middle-aged adults in the UK general population. PloS One. 10 (4), e0123579 (2015).
Chiolero, A., Faeh, D., Paccaud, F. & Cornuz, J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am. J. Clin. Nutr. 87 (4), 801–809 (2008).
Keetile, M., Navaneetham, K. & Letamo, G. Patterns and determinants of hypertension in Botswana. J. Public Health. 23, 311–318 (2015).
Tuovinen, E-L. et al. Smoking status and abdominal obesity among normal-and overweight/obese adults: Population-based FINRISK study. Prev. Med. Rep. 4, 324–330 (2016).
Khodayari, S., Sadeghi, O., Safabakhsh, M. & Mozaffari-Khosravi, H. Meat consumption and the risk of general and central obesity: the Shahedieh study. BMC Res. Notes. 15 (1), 339 (2022).
Yu, S. et al. Prevalence of obesity and associated risk factors and cardiometabolic comorbidities in rural Northeast China. BioMed research international. ;2019. (2019).
Wycherley, T. P., Buckley, J. D., Noakes, M., Clifton, P. M. & Brinkworth, G. D. Comparison of the effects of weight loss from a high-protein versus standard-protein energy-restricted diet on strength and aerobic capacity in overweight and obese men. Eur. J. Nutr. 52, 317–325 (2013).
Micha, R., Wallace, S. K. & Mozaffarian, D. Response to letter regarding article,red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: A systematic review and meta-analysis. Circulation 123 (3), e17–e (2011).
Rtveladze, K. et al. Health and economic burden of obesity in Brazil. PLoS One. 8 (7), e68785–e (2013).
Rtveladze, K. et al. Obesity prevalence in Mexico: impact on health and economic burden. Public Health. Nutr. 17 (1), 233–239 (2013).
Keaver, L. et al. Application of the UK foresight obesity model in Ireland: the health and economic consequences of projected obesity trends in Ireland. PLoS One. 8 (11), e79827–e (2013).
Baik, I. Forecasting obesity prevalence in Korean adults for the years 2020 and 2030 by the analysis of contributing factors. Nutr. Res. Pract. 12 (3), 251–257 (2018).
Finkelstein, E. A. et al. Obesity and severe obesity forecasts through 2030. Am. J. Prev. Med. 42 (6), 563–570 (2012).
Rtveladze, K. et al. Obesity trends in Russia. The impact on health and healthcare costs. (2012).
Wang, Y. C., McPherson, K., Marsh, T., Gortmaker, S. L. & Brown, M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 378 (9793), 815–825 (2011).
Acknowledgements
We sincerely thank all authors who contributed to this work.
Funding
This project was conducted with the financial support of the Tehran University of Medical Sciences (TUMS) (grant No.1400-2-99-53750).
Author information
Authors and Affiliations
Contributions
Conceptualization, Visualization, and Methodology:HK, MSH. Supervision, and Project administration: SE, MSH. Investigation: HK, MSH, AM. Writing, reviewing, and editing: HK, MSH, AM, NB. Data curation, and Software: AGH, MSH. All authors have reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The ethical committee of Tehran University of Medical Sciences approved this study (No.IR.TUMS.SPH.REC.1397.288.). The study was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki and adhered to all applicable national guidelines. Informed consent was obtained from all participants before their inclusion in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shiri, M.S., Karami, H., Ghanbarnezhad, A. et al. National and subnational trends in obesity prevalence in Iran: a Spatiotemporal study with future predictions. Sci Rep 15, 17664 (2025). https://doi.org/10.1038/s41598-025-01531-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01531-z
Keywords
This article is cited by
-
Dietary intakes in relation to nutrition recommendations and dietary quality in an Iranian adult population: the results of the Food and Nutrition Surveillance (FNS)
Journal of Health, Population and Nutrition (2025)
-
Inappropriate GFR equations misrepresent CKD epidemiology and risk interpretation in scientific reports
BMC Nephrology (2025)
-
Prevalence and determinants of general and abdominal obesity and overweight among older Iranian adults using 2016 and 2021 STEPS surveys
Scientific Reports (2025)
-
The national and subnational burden attributable to high body mass index in Iran from 1990 to 2021: a systematic analysis of the global burden of disease study
Journal of Diabetes & Metabolic Disorders (2025)
