
Abstract
The gastrointestinal tract is not only an important component of the digestive system but also a crucial part of the body’s immune system. Numerous studies have reported that gastrointestinal immunity plays a critical role in many extraintestinal diseases, including neurodegenerative disorders. However, the relationship between gastric mucosal immunity and neurodegenerative diseases, such as Parkinson’s disease(PD), remains underexplored. The rate of H. pylori infection was assessed using the 13 C-Urea Breath Test (13 C-UBT) in a case-control study involving 315 PD patients and a control group of 22,383 outpatients. Multivariate regression and propensity score matching (PSM) analyses were employed to adjust for confounding factors. A lower H. pylori infection rate was found in PD cases compared to outpatient controls (DOB ≥ 8, 22.5% versus 27.5%, p = 0.049; DOB ≥ 4, 28.6% versus 33.9%, p = 0.046). After adjusting for confounding factors, the H. pylori infection rate remained lower in PD cases compared to controls. The study revealed an inverse correlation between H. pylori infection and PD, suggesting that H. pylori infection could potentially act as a protective factor against the development of PD.
Similar content being viewed by others


Introduction
The gastrointestinal tract serves not merely as a principal organ of digestion but also constitutes a critical immunological interface, orchestrating both local and systemic immune responses1,2. A substantial body of evidence has established that gut-associated lymphoid tissue (GALT)-mediated immunity exerts profound pathophysiological effects on the development and progression of diverse extraintestinal disorders3,4. Nevertheless, the potential mechanistic links between gastric mucosal immune regulation and the pathogenesis of extragastric diseases remain underexplored, with extant literature offering only fragmentary insights into this association.
Helicobacter pylori(H. pylori) is a microaerophilic Gram-negative bacterium and the most prevalent pathogen in the gastrointestinal tract worldwide, infecting approximately half of the global population5,6,7,8. Furthermore, H. pylori can persist long-term in the gastric antrum, triggering corresponding mucosal immune responses and exerting significant effects on human gastric mucosal immunity9,10,11,12. Research indicates its potential influence on various extragastric conditions, acting as a risk factor for some diseases while potentially offering protection against others13,14,15, such as Multiple sclerosis(MS) and inflammatory bowel disease (IBD), where the presence of H. pylori has shown protective effects15,16. However, research on the impact of H. pylori on extraintestinal diseases, particularly central nervous system disorders, is limited, with inconsistent conclusions and unclear mechanisms. Given H. pylori’s protective role against intestinal mucosal inflammation in IBD, there is speculation about its potential inverse correlation with neurodegenerative diseases like Parkinson’s disease(PD).
PD is currently the second most prevalent neurodegenerative disorder worldwide, primarily affecting the elderly, with incidence increasing with age17,18,19,20. In addition to motor symptoms, over 80% of patients may experience a range of gastrointestinal symptoms, including swallowing difficulties, delayed gastric emptying, severe constipation, and anorectal dysfunction, which can occur years before the onset of motor symptoms21,22. The pathological features of PD include progressive apoptosis of dopaminergic neurons in the substantia nigra pars compacta of the midbrain and the formation of Lewy bodies composed of abnormal α-synuclein aggregates within neurons. Post-mortem anatomical and animal experimental studies have shown that Lewy bodies can also be found in the enteric nervous system and vagal nerve axis in PD patients23.
Current evidence regarding the association between gastrointestinal immunity and PD remains limited, characterized by insufficient mechanistic investigations in basic research and clinically heterogeneous studies with inadequate sample sizes and inconsistent findings. To address this critical knowledge gap, particularly concerning the potential link between H. pylori infection and PD pathogenesis, large-scale population-based studies with robust methodological designs are imperative. In this context, we implemented a nationwide population-based cohort study to systematically evaluate the epidemiological and pathophysiological relationship between H. pylori infection and PD risk.
Method
Ethical statement and study design
This was a case-control study with the subjects derived from the outpatients and inpatients in the Sichuan Provincial People’s Hospital, a provincial comprehensive hospital in Chengdu, China. All individuals provided their written, informed permission for the use of their clinical data in this study. Adhering strictly to the Declaration of Helsinki guidelines, this study received full approval from the Institutional Review Board for Clinical Research at the Sichuan Provincial People’s Hospital.
The PD cases were those definitively diagnosed by the Neurology Clinic and who agreed to participate in this study at this hospital from March 2022 to July 2024. During this period, the outpatients who undergopasting the 13 C Urea Breath Test (13 C-UBT) were included in the control group. Additionally, since the PD patients were sourced from outpatient clinics, we collected data on all patients at this hospital who had undergone 13 C-UBT for H. pylori infection detection from 2022 to 2024. Written informed consent was obtained from all participants.
Definition of participants
Parkinson’s disease cases
Inclusion Criteria:
Patients diagnosed with PD were established by neurologists through Movement Disorder Society Clinical Diagnostic Criteria for Parkinson’s disease (PD)24, which was combined with comprehensive neurologic examinations, patient age, family history, and Parkinson’s diseasetous clinical manifestations. Only the initial test result will be recorded if multiple results are available and we did not exclude participants with eradication treatment.
Exclusion Criteria:
Participants with other severe neurodegenerative diseases besides Parkinson’s disease, such as Alzheimer’s disease, multiple system atrophy, progressive supranuclear palsy, etc., were excluded from the study.
Outpatient controls
Inclusion Criteria:
Participants from different outpatient departments in Sichuan provincial people’s hospital after 2022, who underwent 13 C-UBT. Only the initial test result will be recorded if multiple results are available and we did not exclude participants with eradication treatment.
Exclusion Criteria:
Participants with severe neurodegenerative diseases were excluded from the study.
H. pylori Eradicated cases could not be excluded and evaluation between current and past H. pylori infections could not be performed.
Definition of H. pylori infection
H. pylori infection was determined using the 13 C-UBT with the UREA-13 C breath test Heliforce kits (Beijing Richen-Force Science & Technology, Beijing, China). Breath samples were collected before and 30 min after ingestion of 75 mg of 13 C-urea by fasting patients (or those who had fasted for at least two hours). The breath samples were analyzed using an infrared heterodyne radiometer (Guangzhou Huayou Mingkang Optoelectronics Technology Co., Ltd, Guangzhou, China). Subjects who had taken histamine-2 receptor antagonists, proton pump inhibitors, antibiotics, bismuth compounds, or nonsteroidal anti-inflammatory drugs (excluding low doses of aspirin) in the preceding four weeks were excluded to avoid false-negative chances. This test provided a delta over baseline (DOB) value.
The determination of H. pylori infection positivity was conducted the following two criteria:
-
(i)
DOB ≥ 4.0: A DOB value of ≥ 4.0 was considered positive for H. pylori infection. Values below this threshold were considered negative by most of based health check-up population study.
-
(ii)
DOB ≥ 8.0: A DOB value of ≥ 8.0 was considered positive for H. pylori infection. Values below this threshold were considered negative. The magnitude of the DOB value is related to the severity of H. pylori infection, with higher DOB values correlating with greater H. pylori density, as well as histopathological chronicity and activity indices.
In selecting two distinct cutoff values for the 13 C-UBT, we adopted DOB ≥ 4 as the threshold, a standard widely utilized in the majority of epidemiological surveys to facilitate comparisons across studies. However, acknowledging the potential for false positives at the DOB ≥ 4 level, we also employed a DOB ≥ 8 cutoff to enhance the reliability of H. pylori infection detection. The DOB ≥ 8 threshold maintains detection sensitivity while improving specificity for H. pylori infection. This dual-threshold approach offers a more comprehensive assessment of infection status and contributes to the increased reliability of our research findings.
Covariate definitions
Self-designed questionnaire and the electronic medical records are used to collect the sociodemographic and medical characteristics of PD patients and outpatient controls. Participants who PD and non-Parkinson’s diseasetous population are interviewed face to face by the research assistants being trained standard. The covariates include sex, age, area, disease history (e.g. hypertension, diabetes mellitus, coronary artery disease, Peptic ulcer(Gastric and/or duodenal ulcers), Digestive tract cancer(Gastric cancer, colorectal cancer and/or esophageal cancer)), et al.
Statistical analysis
Means ± standard deviations (SD) were calculated for continuous variables, while percentages were used for categorical variables in both the PD and comparison populations. Continuous variables were compared using the independent samples t-test. Categorical variables were compared using the χ² test, where applicable. Multivariate logistic regression and propensity score matching (PSM) analysis were utilized to exclude the selection bias and confounding factors. All variables with P < 0.05 in the univariate analysis were included in the multivariate logistic regression to investigate the associations between risk factors and H. pylori infection. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Data were analyzed using SPSS, version 24.0 (IBM Corp), GraphPad Prism version 9.5.0, and RStudio software, version R-4.2.3 (R Core Team, 2024). P value of less than 0.05 was considered statistically significant (two-tailed tests).
Result
The general situation of PD patients and outpatients population
From 2022 to 2024, 315 PD patients diagnosed by neurologist in the department of neurology of this hospital were included. The average age of PD patients was 64.67 ± 10.21 years, and 50% of them were male.
During the same period, 22,383 outpatients population outpatients (older than 18 years) in the same hospital who had undergone the 13 C-UBT for H. pylori infection were included, comprising the hospital-based controls. The average age was 45.14 ± 10.31 years with 42% of them were male. The age and gender distribution were still different between the PD cases with outpatients’ population (Table 1).
Comparison of H. pylori infection rate between PD patients and outpatients population by univariate and multivariate logistic regression analysis
Due to significant differences in H. pylori infection rates across regions, study periods, and detection methods, we compared whether the baseline infection rate in this study exhibited substantial selection bias. Based on recent studies on H. pylori infection rates across various regions of China, we have compiled data from January 2020 to the present. The subjects in these studies were all aged 18 years or older, and the detection of H. pylori infection was conducted using the 13 C-UBT. These data are consistent with the H. pylori infection prevalence observed in our hospital’s outpatient control group25,26,27,28,29,30,31.
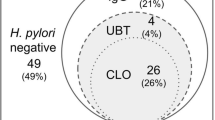
In our statistical results, the univariate analysis showed that the H. pylori infection rate in PD patients was significantly lower than that of the overall outpatient controls (DOB ≥ 8, 22.5% vs. 27.5%, OR 0.77, 95% CI: 0.59-1.00, p = 0.049; DOB ≥ 4, 28.6% vs. 33.9%, OR 0.78, 95% CI: 0.61-1.00, p = 0.046)(Fig. 1A).
Considering the potential influence of other factors, including gender, age, area, hypertension, diabetes, coronary artery disease, Peptic ulcer(Gastric and/or duodenal ulcers) and Digestive tract cancer(Gastric cancer, colorectal cancer and/or esophageal cancer), we conducted a multivariate analysis of H. pylori infection rates between PD patients and the outpatient controls. The results showed that the infection rate in PD patients was still significantly lower than that in the control group (DOB ≥ 8: OR 0.74, 95% CI: 0.56–0.97, p = 0.030; DOB ≥ 4: OR 0.73, 95% CI: 0.56–0.94, p = 0.015) (Fig. 1B). Additionally, regardless of whether the population was urban or rural, the H. pylori infection rate in PD patients was lower with a more pronounced and statistically significant difference observed in the rural population (Supplement Table 1, Supplement Fig. 1).

Comparison of H. pylori infection rates in PD patients with outpatients population for confounding factors by multivariate logistic regression analysis. (A) Comparison of H. pylori infection rates in PD patients with outpatients population. (B) Association of H. pylori infection and PD by a multivariate logistic regression analysis. Odds ratio (ORs) was adjusted for the sex (male = 1, female = 0), age (years), Hypertension (Yes = 1, No = 0), Diabetes Mellitus (Yes = 1, No = 0), Coronary Artery Disease (Yes = 1, No = 0), Peptic ulcer (Yes = 1, No = 0), Digestive tract cancer(Yes = 1, No = 0), H. pylori infection (Positive = 1, Negative = 0). *p < 0.05.
Comparison of H. pylori infection rate between PD patients and outpatient controls after PSM
To further validate the accuracy of these findings, we performed a PSM analysis. After balancing covariates, PSM confirmed lower H. pylori infection rates in PD cases than in outpatient controls(DOB ≥ 8: OR 0.69, 95% CI: 0.52–0.91, p = 0.009; DOB ≥ 4: OR 0.71, 95% CI: 0.55–0.92, p = 0.009) (Table 2; Fig. 2A). Logistic regression post-PSM revealed the same results with the above (DOB ≥ 8: OR 0.68, 95% CI: 0.52–0.90, p = 0.008; DOB ≥ 4: OR 0.70, 95% CI: 0.54–0.91, p = 0.007) (Fig. 2B). In conclusion, the infection rate in PD patients remained significantly lower than that in the control group, with a statistically significant difference.

Comparison of H. pylori infection rates in PD patients with outpatient controls for confounding factors by PSM. (A) Comparison of H. pylori infection rates in PD patients with outpatients population after PSM. (B) Association of H. pylori infection and PD by a Logistic regression post-PSM. Odds ratio (ORs) was adjusted for the sex (male = 1, female = 0), age (years), Hypertension (Yes = 1, No = 0), Diabetes Mellitus (Yes = 1, No = 0), Coronary Artery Disease (Yes = 1, No = 0), Peptic ulcer (Yes = 1, No = 0), Digestive tract cancer(Yes = 1, No = 0), H. pylori infection (Positive = 1, Negative = 0). **p < 0.01.
Discussion
As we know, Parkinson’s disease (PD) is an age-related neurodegenerative disorder. Its onset is associated with multiple factors, including genetics and environmental influences, though the exact pathogenesis remains unclear. In this study, we found that the rate of H. pylori infection in PD patients was consistently lower than that in the outpatient control group across various analytical methods, including univariate analysis, multivariate analysis, and propensity score matching (PSM) analysis. Additionally, we observed that, regardless of whether the population was urban or rural, the H. pylori infection rate in PD patients was lower than that in the control group, with a more pronounced and statistically significant difference observed in the rural population. This may be related to the simpler lifestyle and fewer confounding factors in rural areas(supplement Table 1). Considering that PD is associated with aging, we divided the PD and outpatients population groups using 65 years of age as a cutoff for comparison. In the univariate analysis and multivariate analysis, the infection rate in PD patients under 65 was significantly lower than in outpatients population patients, with statistical significance(supplement Table 2).
Previous studies have reported limited discussion on the relationship between H. pylori and PD, with most findings contrary to our results. Dobbs et al.32 reported a higher infection rate of H. pylori in PD patients (50 out of 105, or 47.6%) compared to non-PD patients (39.5%), with a more pronounced difference in those under 72 years old. The statistical analyses by Nafisah et al., Nielsen et al., and Bu et al.33,34,35 also indicated a higher infection rate in PD patients. Lee et al.36 found that H. pylori infection could reduce levodopa absorption during treatment, exacerbating symptom fluctuations. Mridula et al.18 noted that H. pylori infection affected levodopa absorption, leading to increased medication dosage. Liu et al.19 concluded from a three-group controlled trial that eradicating H. pylori improved clinical symptoms in PD patients, particularly in terms of bradykinesia. Lolekha et al.37 suggested that eliminating H. pylori could reduce symptom fluctuations in PD patients. However, other studies raised doubts. Nafisah et al., Narozanska et al., and Tan et al.6,34,38 argued that there were no significant improvements in clinical manifestations or UPDRS scores after H. pylori eradication in positive PD patients. Nonetheless, these studies have certain limitations: first, current research largely consists of small-sample case-control and cross-sectional studies, with unclear theoretical mechanisms; second, because of the differences of the H. pylori infection rate in rural and urban area, past research has more focused on developed regions while studies in developing countries or rural areas are lacking. This study aims to address these limitations. Based on recent findings in further research on H. pylori and our statistical results, we suspect that the relationship between PD and H. pylori infection differs from earlier research. The clinical research results merit further discussion.
The pathogenesis of PD remains unclear. Brakk’s theory posits that PD may originate outside the CNS, with pathogens crossing the gastrointestinal barrier and entering the CNS via the vagus nerve, with non-motor symptoms like gastrointestinal dysfunction often preceding motor symptoms23. Also, some evidence suggests it may involve immune-related or autoimmune mechanisms39,40,41,42. This study found a negative correlation between PD and H. pylori, indicating a potential protective role of H. pylori, possibly through its modulation of immune responses, such as promoting regulatory T cell (Treg) activity in childhood and reducing inflammation39.The “hygiene hypothesis“43,44, which suggests that early exposure to enteric infections in less hygienic environments may prevent immune-related diseases later in life, further support the idea that early environmental exposures, including H. pylori, may influence PD development by affecting immune regulation and gut-brain interactions, warranting further investigation into H. pylori ‘s role in PD.
This clinical study does have limitations. First, it consists solely of single-center data, which may not fully represent the situation in different countries and regions. Conducting multicenter studies is necessary to confirm these findings. Second, variations in extra-gastric diseases associated with H. pylori may arise from diverse immune responses in hosts, yet we did not assess immune states in participants. Comparing immune responses between H. pylori-positive and -negative individuals among both PD patients and controls is essential.
In conclusion, the prevalence of H. pylori infection in PD patients was significantly lower than that in the outpatient control group, with this difference reaching statistical significance. Given that H. pylori infection is highly prevalent among middle-aged and younger populations, we propose that H. pylori colonization might exert a protective effect against PD development, particularly during the early stages of the disease. However, further experimental and clinical studies are warranted to validate this hypothesis.
Data availability
The datasets generated and/or analysed during the current study are not publicly available. Due to privacy protection and data security concerns, the data cannot be shared. However, upon reasonable request, the data may be made available from the corresponding author.
References
Furness, J. B., Rivera, L. R., Cho, H. J., Bravo, D. M. & Callaghan, B. The gut as a sensory organ. Nat. Reviews Gastroenterol. Hepatol. 10(12), 729–740 (2013).
Guo, N. et al. Immune subset-committed proliferating cells populate the human foetal intestine throughout the second trimester of gestation. Nat. Commun. 14(1). https://doi.org/10.1038/s41467-023-37052-4 (2023).
Rogler, G., Singh, A., Kavanaugh, A. & Rubin, D. T. Extraintestinal manifestations of inflammatory bowel disease: Current concepts, treatment, and implications for disease management. Gastroenterology 161(4), 1118–1132 (2021).
Peng, K. et al. MAdCAM-1 mediates retinal neuron degeneration in experimental colitis through recruiting gut-homing CD4 + T cells. Mucosal Immunol. 14(1), 152–163. https://doi.org/10.1038/s41385-020-0282-x (2021).
Gravina, A. G. et al. Helicobacter pylori and extragastric diseases: A review. World J. Gastroenterol. 24(29), 3204–3221 (2018).
Tan, A. H. et al. Helicobacter pylori infection is associated with worse severity of Parkinson’s disease. Parkinsonism Relat. Disord. 21(3), 221–225 (2015).
Baj, J. et al. Helicobacter pylori infection and extragastric Diseases-A focus on the central nervous system. Cells 10(9), 2191 (2021).
Hunt, R. H. et al. Helicobacter pylori in developing countries. World gastroenterology organisation global guideline. J. Gastrointest. Liver Diseases: JGLD 20(3), 299–304 (2011).
Ito, N., Tsujimoto, H., Ueno, H., Xie, Q. & Shinomiya, N. Helicobacter pylori-Mediated immunity and signaling transduction in gastric Cancer. J. Clin. Med. 9(11), 3699 (2020).
Araújo, G. R. L. et al. Helicobacter pylori infection: How does age influence the inflammatory pattern? World J. Gastroenterol. 28(4), 402–411 (2022).
Harris, P. R. et al. Helicobacter pylori gastritis in children is associated with a regulatory T-cell response. Gastroenterology 134(2), 491–499 (2008).
Yörgüç, E. et al. Comparison of clinical outcomes and FOXP3, IL-17A responses in Helicobacter pylori infection in children versus adults. Helicobacter 26(3), e12795. (2021).
Malfertheiner, P. et al. Helicobacter pylori infection. Nat. Reviews Disease Primers 9(1). https://doi.org/10.1038/s41572-023-00431-8 (2023).
Arjmandi, D. et al. Helicobacter pylori infection and risk of multiple sclerosis: An updated meta-analysis. Helicobacter 27(6), 1–12 (2022).
Lin, K. et al. Effects of Anti–Helicobacter pylori therapy on incidence of autoimmune diseases, including inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 17(10), 1991–1999 (2019).
Jaruvongvanich, V., Sanguankeo, A., Jaruvongvanich, S. & Upala, S. Association between Helicobacter pylori infection and multiple sclerosis: A systematic review and meta-analysis. Multiple Scler. Relat. Disord. 7, 92–97 (2016).
Bu, X. L. et al. The association between infectious burden and Parkinson’s disease: A case-control study. Parkinsonism Relat. Disord. 21(8), 877–881 (2015).
Mridula, K. R., Borgohain, R., Chandrasekhar Reddy, V., Bandaru, V. & Suryaprabha, T. Association of Helicobacter pylori with Parkinson’s disease. J. Clin. Neurol. (Seoul Korea) 13(2), 181–186 (2017).
Liu, H. et al. Eradication of Helicobacter pylori infection might improve clinical status of patients with Parkinson’s disease, especially on bradykinesia. Clin. Neurol. Neurosurg. 160, 101–104 (2017).
Shen, S., Zhang, C., Xu, Y. M. & Shi, C. H. The role of pathogens and Anti-Infective agents in Parkinson’s disease, from etiology to therapeutic implications. J. Parkinson’s Dis. 12(1), 27–44 (2022).
Travagli, R. A., Browning, K. N. & Camilleri, M. Parkinson disease and the Gut: New insights into pathogenesis and clinical relevance. Nat. Rev. Gastroenterol. Hepatol. 17(11), 673–685 (2020).
Ntetsika, T., Papathoma, P. E. & Markaki, I. Novel targeted therapies for Parkinson’s disease. Mol. Med. (Cambridge Mass) 27(1), 17 (2021).
Braak, H., Rüb, U., Gai, W. P. & Del Tredici, K. Idiopathic Parkinson’s disease: Possible routes by which vulnerable neuronal types May be subject to neuroinvasion by an unknown pathogen. J. Neural Transmission (Vienna Austria: 1996). 110(5), 517–536 (2003).
Postuma, R. B. et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disorders: Official J. Mov. Disorder Soc. 30(12), 1591–1601 (2015).
Wang, G., Zhang, Z. Y., Mei, Y. P. & Wang, Y. B. [An analysis of 13 C breath test and immunophenotyping results of Helicobacter Pylori in health examination population in Nanjing area]. Biaoji Mianyi Fenxi Yu Linchuang. 30, 57–60 (2023). 169.
Shi, X. L. [Analysis of Helicobacter Pylori positive rate and health education among healthy people]. Jiankang Zhonggao 16, 1–3 (2022).
Kong, Q. et al. Low compliance to post-screening recommendations in a family-based Helicobacter pylori screening and treatment program: A prospective cohort study. Helicobacter 27, e12912 (2022).
Guan, R. P., Dai, G. K., Jiang, G. L., Li, Y. & Xu, Y. [Analysis of Helicobacter pylori infection and related factors among public officials in Guangzhou]. Guoji Yiyao Weisheng Daobao 28, 284–287 (2022).
Li, C. et al. Prevalence and predictors of Helicobacter pylori infection in asymptomatic individuals: A hospital-based cross-sectional study in Shenzhen, China. Postgrad. Med. 134, 686–692 (2022).
Zhao, H. Z., Chen, Y. Y. & Chang, J. [Analysis about the detection results of Helicobacter Pylori in healthy people]. XinJiang Yixue. 52, 814–815 (2022).
Zhou, X. Z. et al. Large-scale, National, family-based epidemiological study on Helicobacter pylori infection in China: The time to change practice for related disease prevention. Gut 72(5), 855–869 (2023).
Dobbs, R. J., Charlett, A., Dobbs, S. M., Weller, C. & Peterson, D. W. Parkinsonism: differential age-trend in Helicobacter pylori antibody. Aliment. Pharmacol. Ther. 14(9), 1199–1205 (2000).
Bu, X. L. et al. The association between infectious burden and Parkinson’s disease: A case-control study. Parkinsonism Relat. Disord. 21(8), 877–881. https://doi.org/10.1016/j.parkreldis.2015.05.015 (2015).
Nafisah, W.Y., Najman, A.H., Hamizah, R., Azmin, S., Rabani, R., Shah, S.A. and Norlinah, M.I., (2013). High prevalence of Helicobacter pylori infection in Malaysian Parkinson’s disease patients. Journal of Parkinsonism and Restless Legs Syndrome 63.
Nielsen, H. H., Qiu, J., Friis, S., Wermuth, L. & Ritz, B. Treatment for Helicobacter pylori infection and risk of Parkinson’s disease in Denmark. Eur. J. Neurol. 19(6), 864–869 (2012).
Lee, W. Y., Yoon, W. T., Shin, H. Y., Jeon, S. H. & Rhee, P. L. Helicobacter pylori infection and motor fluctuations in patients with Parkinson’s disease. Mov. Disorders: Official J. Mov. Disorder Soc. 23(12), 1696–1700 (2008).
Lolekha, P., Sriphanom, T. & Vilaichone, R. K. Helicobacter pylori eradication improves motor fluctuations in advanced Parkinson’s disease patients: A prospective cohort study (HP-PD trial). PloS One 16(5), e0251042. (2021).
Narożańska, E. et al. Pharmacokinetics of Levodopa in patients with Parkinson disease and motor fluctuations depending on the presence of Helicobacter pylori infection. Clin. Neuropharmacol. 37(4), 96–99 (2014).
Chen, Z., Chen, S. & Liu, J. The role of T cells in the pathogenesis of Parkinson’s disease. Prog. Neurobiol. 169, 1–23 (2018).
Tan, E. K. et al. Parkinson disease and the immune system - associations, mechanisms and therapeutics. Nat. Reviews Neurol. 16(6), 303–318 (2020).
Bonam, S. R. & Muller, S. Parkinson’s disease is an autoimmune disease: A reappraisal. Autoimmun. Rev. 19(12), 102684 (2020).
Campos-Acuña, J., Elgueta, D. & Pacheco, R. T-Cell-Driven inflammation as a mediator of the Gut-Brain Axis involved in Parkinson’s disease. Front. Immunol. 10, 239 (2019).
Kira, J. ichi. Helicobacter pylori infection might prove the hygiene hypothesis in multiple sclerosis. J. Neurol Neurosurg. Psychiatry. 86(6), 603–607 (2015).
Bach, J. F. The hygiene hypothesis in autoimmunity: The role of pathogens and commensals. Nat. Rev. Immunol. 18(2), 105–120 (2018).
Funding
This work was granted by the National Natural Science Foundation of China (82450003, 82370560) and the Sichuan Science and Technology Programgrants (2023YFS0022).
Author information
Authors and Affiliations
Contributions
X.X. and Z.W wrote the main manuscript text. H.Z. prepared figures. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xiao, X., Wang, Z., Zhang, H. et al. Helicobacter pylori infection might be a protective factor against Parkinson’s disease. Sci Rep 15, 16689 (2025). https://doi.org/10.1038/s41598-025-01562-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-01562-6
