
Abstract
Research on QOL of patients with chronic diseases has attracted extensive attention and the QLICD-GM (general module of Quality of Life Instruments for Chronic Diseases) has been used worldwide. To compare QOL in patients with 10 kinds of different chronic diseases, and to explore its socio-demographic influencing factors, so as to provide reference for improving QOL of chronic disease patients. A Multicenter Large Sample Cross-sectional Study with nine hospitals. 1953 patients with 10 kinds of chronic diseases were investigated by a general situation questionnaire, and the QLICD-GM including three domains of physical function (PHD), psychological function (PSD) and social function (SOD). The influencing factors of PHD, PSD, SOD and the overall scale were analyzed by univariate analysis such as t-test or one-way analysis of variance, and multiple linear regressions. The total mean score of QLICD-GM in all chronic diseases was 65.24 ± 13.50;Among three domains, the highest mean score was found in SOD 72.54 ± 15.55, the second highest mean score in PHD was 62.45 ± 15.37, and the lowest mean score in PSD was 62.23 ± 17.79. Marriage, occupation, education, family economic, medical format were main influencing factors of QOL for patients with chronic diseases. QOL of patients with chronic diseases is low. Effective corresponding strategies and targeted management or intervention measures should be taken to improve QOL, and it is important to give personalized treatment and nursing to patients based on various factors.
Similar content being viewed by others


Introduction
Along with the continuous changes of Chinese people’s lifestyles, living environments, and healthcare, chronic non-communicable diseases such as cardiovascular and cerebrovascular diseases, chronic obstructive pulmonary diseases, diabetes mellitus, malignant tumors, and other chronic non-communicable diseases have become the primary public health problem of the disease burden of China’s residents, occupying about 70% or more of the proportion of disease burden among all types of diseases in China1. Data show that the incidence of cardiovascular and cerebrovascular diseases in China is as high as 25.10%, ranking first in the prevalence of various chronic diseases. The fastest growing prevalence rate is 5.10% for diabetes2. The prevalence of chronic bronchitis and chronic obstructive pulmonary disease is also as high as 2.61%3. Chronic diseases have become a major threat to people’s lives and health due to their long duration, slow recovery and complications, greatly affecting quality of life (QOL) of patients with chronic diseases.
Given the far-reaching impact of chronic diseases on QOL, research on the QOL of patients with chronic diseases has attracted extensive attention from all sectors of society. Scholars, medical practitioners, policy makers, and patient organizations have devoted themselves to the development of QOL scales for chronic disease patients and to exploring effective ways to improve the QOL of chronic disease patients. However, in the process of practice, the scales developed and introduced by foreign countries have large differences in cultural backgrounds with China, and are less generalizable, and some of the domestic QOL measurement scales for patients with chronic diseases can be used to study fewer types of chronic diseases, and cannot comprehensively study the changes in the QOL of patients. It is urgent to develop scientific, effective and easy-to-operate QOL measurement instruments.
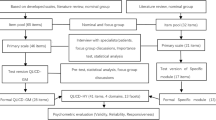
In this background, our QOL team developed a system entitled Quality of Life Instruments for Chronic Diseases (QLICD) through a modular approach. The system includes a general module (QLICD-GM) which can be used for all types of chronic diseases, as well as specific modules only for related diseases4. The latest version of the system QLICD (V2.0) contained 34 chronic disease-specific scales, including QLICD-HY for hypertension5, QLICD-CHD for Coronary Heart Disease6, QLICD-OS for osteoporosis7 etc. Among them, QLICD-GM is a basic and core instrument which can be used for all chronic diseases, and has been tested to have high reliability and validity, has a wide range of applications, and is an important tool for evaluating the effectiveness of prevention and treatment of chronic diseases4,5.
This study is aimed to understand the quality of life of patients with different chronic diseases in Dongguan, Zhanjiang and Kunming in China. The quality of life of patients with a variety of chronic diseases in the region was evaluated and compared, in order to understand the impact of different influencing factors on the quality of life of patients so as to carry out interventions to improve the quality of life of patients.
Methods
Sample and setting
This current study is a cross-sectional study, which was approved by the Ethics Committees at all participating hospitals.
Study subjects were conducted at nine hospitals in Dongguan City, Zhanjiang City, Guangdong Province and Kunming City in Yunnan province. The diseases suffered by the chronic disease patients investigated in the study mainly include hypertension, coronary heart disease, chronic gastritis, peptic ulcer, chronic obstructive pulmonary disease, diabetes mellitus, stroke, osteoporosis, and other chronic non-communicable diseases.
The inclusion criteria of the studied subjects were: (1) All the participating subjects were diagnosed as suffering from one or more chronic diseases through the outpatient or inpatient department of the hospital; (2) All the subjects were over 16 years of age, with stable conditions and no life-threatening relapses or complications; (3) The research subjects have no history of dementia or psychiatric diseases, have normal cognitive function, thinking ability and expression ability, and can answer questions clearly and completely; (4) The research subjects voluntarily participate in this study.
The exclusion criteria were: (1) the subjects were physically weak and unable to communicate verbally; (2) they had serious mental disorders; (3) they were unable to complete the questionnaire survey independently; (4) they refused the survey and did not cooperate.
According to the literature, the sample size required for multiple linear regression should be at least 10 times the number of independent variables; therefore, this study screened a maximum of 20 independent variables prior to the multiple linear regression analysis, and the sample size was pre-determined to be 200 (20 × 10).
Measure instruments
This investigation includes the general situation questionnaire and the general module of the QLICD (QLICD-GM (V2.0)). The general situation questionnaire is a self-designed questionnaire, mainly including gender, age, education level, marital status, etc.
The QLICD-GM (V2.0) is a general scale for chronic disease patients, and it can be used to compare the quality of life of patients with various chronic diseases.
The QLICP-GM (V2.0) has the three domains: physical function (PHD), psychological function (PSD) and social function (SOD), with the total 28 items. Among them, PHD contains nine items, PSD contains eleven items, SOD contains eight items. Each item of the QLICP-GM (V2.0) was rated on the 5-point Likert scale, each item was scored as 1, 2, 3, 4 and 5 points, and reverse items were scored in reverse. Each domain score was obtained as the total of the corresponding item responses. The overall scale score was also obtained as the sum of the three domain scores. To facilitate comparison, we used the hundred-mark system for calculation. The method is to subtract the score from its minimum and then divide the difference by the range. Higher scores on the scale indicate a better quality of life.
The QLICD-GM(V2.0) has good validity, reliability and better responsiveness to better evaluate the quality of life of patients with chronic diseases4. Retest reliability coefficients above 0.70(ranging from 0.71 to 0.92) for all domains and facets, the internal consistency alphas for most domains and facets were higher than 0.65 (ranging from 0.52 to 0.89), the theoretical construct was confirmed by the data analyses, which demonstrated good construct validity.
Survey methods
The trained investigators carried out an on-site survey. After the investigators explained the above two questionnaires, the patients with pre-determined chronic diseases such as hypertension, coronary heart disease etc. filled out the above two questionnaires by themselves. In this survey, 1953 valid questionnaires were collected, with an effective recovery rate of 97.65%. At the same time, some patients were selected for qualitative interview survey in order to further understand their survival conditions and influencing factors.
Statistical analysis
The statistical analysis of the data in this study was conducted using SPSS25.0 software. Descriptive statistics were used to summarize the socio-demographic variables. Mean and standard deviations (SD) were calculated for continuous variables. Frequencies and percentages were calculated for categorical variables. The influencing factors of each domain of PHD, PSD, SOD, TOT were analyzed by univariate analysis such as t-test or one-way analysis of variance (ANOVA). The statistically significant variables from univariate analysis were used to fit a multiple linear regression model. A multiple linear regression was performed with the total score and the scores of each domain of the QLICD-GM (V2.0) scale as the dependent variables respectively, and the possible influencing factors of gender, age, occupation, and marriage etc. as the independent variables. The rationale behind this approach is to understand the specific factors influencing each dimension of QoL separately, as well as their combined effect on overall QoL. The categorical variables were recoded as quantification method before analysis (see Table 1 in detail). The variables were selected by stepwise procedure with P-value in = 0.05 and P-value out = 0.10.
Results
Sample characteristics
A total of 1953 participants were recruited. Details of the social-demographic characteristics for the 1953 participants are shown in Table 2. The mean age of the subjects was 52.29 years old, SD = 17.50. Female were 1,052 (53.87%), Han Chinese were 1916 (98.11%);farmers were 642 (32.87%), married 1602 (82.03%), secondary school education were 1110 (56.84%); the moderate family economic status was 1,224 (62.67%), participants covered by other medical insurance were 1022(52.33%); using a single drug treatment were 877 (44.91%).
Scores of QLICD-GM(V2.0) in 10 different kinds of patients
The scores of QLICD-GM(V2.0) in 10 different kinds of patients and their comparisons were presented in Table 3; Fig. 1 in details. Among the scores of QLICD-GM(V2.0) in patients with 10 different chronic diseases, from the perspective of the total score of the general module, the score of hypertension patients was the highest (70.95 ± 13.83), and the score of gout patients was the lowest (58.82 ± 9.00). In terms of domain score, hypertensive patients had the highest score in the domain of physical function (69.07 ± 14.75), COPD patients had the lowest score in the domain of physical function (51.76 ± 14.51). The patients with peptic ulcer had the highest score of psychological function (69.52 ± 15.80), Gout patients had the lowest score in the domain of psychological function (48.67 ± 14.19). The score of social function of hypertension patients was the highest (76.15 ± 16.17), while the score of social function of COPD patients was the lowest (68.45 ± 14.37). There were significant differences in the scores of each domain among different diseases (P < 0.05).

Comparison of the scores of QLICD-GM in 10 kinds of chronic diseases.
Scores of QLICD-GM (V2.0) in all patients with chronic diseases
The scores of QLICD-GM(V2.0) in all patients were presented in Table 4; Fig. 2 in details. It can be seen that scores on each domain in the QLICD-GM (V2. 0) scale were statistically significant (P < 0.05), with the total score of the QLICD-GM (V2. 0) scale being 65.24 ± 13.5 (95%CI 61.77–63.13). Among all domains, the social function domain had the highest score with a mean of 72.54 ± 15.55 (95%CI 61.44–63.02). The mean score in the domain of physical function was 62.45 ± 15.37 (95% CI 71.85–73.23), while the mean score of psychological function was 62.23 ± 17.79 (95%CI: 64.64–65.85).

Comparison of the scores of QLICD-GM in all patients.
Multiple linear regression analysis
To explore the factors influencing quality of life in patients with chronic diseases, in this study, the total score of the QLICD-GM (V2.0) and the score of each domain were used as the dependent variables, respectively; the multiple linear regressions were conducted to analyze the socio-demographic influences as independent variables. Before analyzing, the correlations between independent variables were computed and the inspection on no-multicollinearity has been diagnosed. The VIF values for all domain-specific models were close to 1 and remained below the threshold of 10, implying that multicollinearity was not a concern in these analyses.
The influencing factors on QOL for both total score and scores in each domain in patient with chronic diseases were presented detailed in Table 5. The regression results showed that the regression equation was significant for physical functions domain in general (F = 44.392, P < 0.001), and 6 statistically significant variables were finally entered into the regression equation, with age(B=−7.957, t=−14.422, P < 0.001), family economy(B = 2.603, t = 4.164, P < 0.001), medical Format (B = 1.429, t = 3.584, P < 0.001) P < 0.001), the Marriage (B = 3.154, t = 3.604, P < 0.001), occupation (B = 1.848, t = 2.460, P = 0.014), treatment (B = 0.657, t = 1.999, P = 0.046). The coefficient of determination (R2) of the model was 0.120, and the adjusted R2 was 0.118, indicating that these variables could explain 11.80% of the variance in physical function scores of patients with chronic diseases.
The results of regression equation for psychological function domain as the dependent variable showed that the regression equation was significant in general (F = 30.462, P < 0.001), and 5 statistically significant variables were finally entered into the regression equation. Family economy (B = 5.554, t = 7.872, P < 0.001), medical format (B = 3.287, t = 6.994, P < 0.001), age (B = 2.863, t = 4.454, P < 0.001), marriage (B = 3.097, t = 2.990, P = 0.003), and gender (B=−2.253, t=−2.827, P = 0.005) were the influence factors of psychological domain. The coefficient of determination (R2) of the model was 0.073, and the adjusted R2 was 0.070, indicating that these variables could explain 7.00% of the variation in physiological function scores of patients with chronic diseases.
The results of regression equation with social function domain as the dependent variable showed that the regression equation was significant in general (F = 55.553, P < 0.001), and four statistically significant variables were finally entered into the regression equation. Family economy (B = 7.708, t = 12.124, P < 0.001), age (B=−2.770, t=−5.155, P < 0.001), occupation (B=−2.969, t=−3.328, P = 0.001), marriage (B = 2.033, t = 2.680, P = 0.07) were the main influences on social functioning scores. The coefficient of determination (R2) of the model was 0.102, and the adjusted R2 was 0.101, indicating that these variables could explain 10.10% of the variance in social function scores.
The results of the regression equation with the total score of QLICD-GM as the dependent variable showed that the regression equation was generally significant (F = 57.072, P < 0.001), and four statistically significant variables were finally entered into the regression equation. Family economy (B = 5.577, t = 10.546, P < 0.001), age (B=−4.723, t=−9.857, P < 0.001), medical format (B = 2.019, t = 5.752, P < 0.001), marriage (B=−3.026, t=−3.923, P < 0.001) were the main influences on the overall quality of life scores of patients with chronic diseases. The coefficient of determination (R2) of the model was 0.105, and the adjusted R2 was 0.103, indicating that these variables could explain 10.30% of the variation in total scores of patients with chronic diseases.
Discussions
As we all know, with the economic development and the change of people’s living habits, the prevalence of chronic diseases in residents is gradually increasing. Studies have shown that the prevalence of individual chronic diseases among cardiovascular and metabolic diseases, bone and joint diseases, digestive diseases, respiratory diseases, neurological diseases, urological diseases, and oncological diseases has increased over the years in older adults aged 60 years and over. The degree of aging in many country is gradually increasing, and the burden of aging has become an important public health problem. This requires multi-party efforts to improve it. As a comprehensive index, quality of life can well evaluate the physical, psychological and social functions of patients. This study adopts the QLICD-GM (V2.0) scale for evaluation, which is generalizable to all chronic diseases and is culturally adapted for Chinese residents with good reliability, validity and responsiveness.
On the scores of QLICD-GM (V2.0)
This study found that the mean score of the QLICD-GM (V2.0) scale of patients with chronic diseases was 65.24 ± 13.58, suggesting that the health status of patients with chronic diseases is still relatively poor. The results of the scores for each domains showed that people with chronic diseases had the highest scores in the social functioning domain. This is similar to the findings of Rao8 and other scholars, which may be due to the fact that most of the patients receive more family love and care than they used to receive after their illness. In addition, they have the support of friends and community, which can help them cope with the stress caused by the disease, play their social roles better, and enhance the patients’ self-worth, thus improving the quality of life9. The physical function domain had the second highest score and the psychological function domain had the lowest score, which similar to those of An et al.10. As people age, they are more likely to suffer from chronic diseases such as cardiovascular disease and diabetes, resulting in physical function decline to reduce or even unable to participate in social activities, such a change will cause chronic disease patients’ psychological gap, further affects their psychological well-being and leads to lower scores in the domain of psychological functioning.
On influencing factors of physical function
The results of this study found that age would affect the physical function of patients, and the physical function score of older people was lower than that of younger people, which was similar to the research results of Vanleerberghe11, Hjelmeland12, CHEN13. Previous studies have also shown that age is negatively correlated with mobility, self-care ability, and daily activities in elderly patients. It is possible that with the growth of age, the human body’s cardiovascular system, respiratory system, nervous system, etc. will undergo a series of physiological and pathological changes. The decline in physical function can lead to various diseases in the elderly, which in turn results in lower physical function scores.
This study has revealed that an increased number of medications can have a detrimental impact on the physical function of patients. As the number of medications rises, patients’ physical function scores tend to decrease. Ghita Zahlan and other scholars also demonstrated that excessive polypharmacy may contribute to a higher prevalence of chronic pain among patients14. The growing number of medications used can exacerbate the metabolic burden on patients. Potential side effects and drug interactions directly influence patients’ physiological function, leading to liver and kidney damage, digestive system symptoms, and other discomforts which subsequently affect their quality of life. Furthermore, the complexity associated with multi-drug therapy may compromise patient compliance, resulting in medication non-adherence and discontinuation, ultimately undermining therapeutic efficacy and reducing overall physiological function. Therefore, regular medication assessments should be conducted to streamline medication regimens and minimize adverse drug reactions; additionally, comprehensive drug treatment management is essential for enhancing the QOLfor patients15.
This study has shown that marital status is one of the influencing factors of physical function. A study of Japanese residents using collaborative cohort study found that being single was associated with a higher risk of death than being married, and marriage had a protective effect on the health of older adults16. There are multiple explanations for this phenomenon. For elderly individuals who are married, their spouses can provide accompaniment during illness, take care of their diet and daily activities, and offer emotional support and spiritual comfort. These factors can contribute to the improvement of both physical and mental well-being in patients. Furthermore, the spouses of married patients may encourage positive health-related behaviors and facilitate early detection of diseases for timely treatment. Additionally, spousal companionship and support can help alleviate pain and psychological burden associated with chronic illnesses, reduce anxiety and depression symptoms, as well as enhance the QOL and physiological function scores in patients17.
On influencing factors of psychological function
The results of the current study found that family economy, medical format were positive influencing factors of patients’ psychological function. Age, marriage and Gender were negative factors of patients’ psychological function scores.
The type of medical insurance is one of the important factors affecting the mental health domain of QoL, and the results of the study found that the greater the proportion of reimbursement, the higher the mental health score of the patients. The results show that participation in the basic health insurance for urban workers contributes to the mental health of the elderly, and that the level of mental health of the elderly who participate in this insurance is significantly higher than that of the elderly who pay for their own health care. This is similar to the results of Chen S18, Chiu SYR19 and other scholars. One of the reasons for this may be that for the elderly, the decline in physical function with age leads to an increase in the demand for medical security for the elderly. The elderly can enjoy a better level of medical services after choosing to participate in medical insurance, and the improvement of physical health will indirectly improve the mental health20.
On influencing factors of social function
In the domain of social function, family economic status is an important influencing factor. Compared to patients with poor family financial status, patients with moderate and good family economic level scored higher on the social functioning domain. The results of this study are consistent with those of Chen21. The reason for this may be that differences in family economic conditions will lead to the patient’s family environment, which will lead to the patient’s initiative and enthusiasm in seeking medical treatment. Due to economic reasons, patients will choose to tolerate pain and other behaviors, which will lead to delay of treatment, aggravation of the disease, and then lead to the decline of the quality of life. Family economic level also may affect the patient’s social status, which affects the patient’s quality of life.
The study findings indicate that occupation is a positive influence factor on social function, which is similar to the research findings of Takamitsu Shimada22, Qi Y23, Lope B24. This may be due to the fact that farmers have a relatively low level of income, which may result in their scores in the area of social functioning being affected. In addition, compared to workers and employees of enterprises and institutions, farmers have relatively weak social security in the areas of old age and health care, and may not be able to receive adequate protection and support. In contrast, practitioners in other occupations often enjoy better social security, which is beneficial to improve their scores in the social functioning domain.
On influencing factors of the total QLICD-GM (V2.0)
This study also found that age is a significant factor of the total score of QLICD-GM (V2.0). As individuals age, there is a progressive decline in organ and system function, leading to decreased immune function and heightened susceptibility to pathogens, epidemics, and immune system disorders25. The accumulation of age-related ailments can also give rise to somatic symptoms that may trigger adverse emotional states such as anxiety, irritability, and depression among the elderly population, further impacting their quality of life. Moreover, entering old age often coincides with retirement and potential negative life events such as bereavement, illness, and loneliness which can result in diminished social support networks and exacerbate both mental and physical health issues among the elderly26,27.
The results of the study found that unmarried patients with chronic diseases had lower overall QOL scores than those with other marital status. Similar findings have been reported by Tigirigi28, Jang29, Zhang30, and Zhao31. Research has shown that marriage or partnership is an important source of social support, that social support is an important buffer against stressful life events, and that having the presence of family and spouse positively impacts an individual’s physical and mental health, performance, creativity and ability, as well as providing resilience to patients in the face of stressful situations32.
Similar to the results of Chen33 and Mei34, family economic status is also one of the key factors affecting the total score of QOL in patients with chronic diseases. First of all, the family economic status directly affects the patient’s choice of treatment; patients with good family economic conditions will go to the hospital for examination and treatment in a timely manner after they fall ill, while patients with poorer economic conditions will consider their illnesses according to their economic status, which delays the treatment of their illnesses and affects the effect of treatment. Financial pressure may also lead to negative emotions such as anxiety and depression, which can exacerbate the symptoms of chronic diseases and thus reduce the quality of life. In addition, patients with good economic conditions may have better health management behaviors and pay more attention to their health, such as regular physical examination, healthy diet, appropriate exercise, etc., which will also make their overall QOL score higher.
Medical insurance is a positive factor affecting the total score of quality of life. With the greater proportion of medical insurance reimbursement, the total score of QOL of patients is higher. Wang35 and Babiarz36 have similar research results. The results of the study showed that after having rural medical insurance, the QOL score of the residents was significantly higher than before. This may be due to the fact that the higher the reimbursement rate of health insurance, the less pressure the patient has to bear on the medical expenses, the more timely the patient can seek medical treatment to avoid delays in treatment due to financial reasons, and in the treatment of the disease, the patient is able to choose a better treatment plan and medical services, which in turn produces a better therapeutic effect. In addition, compared with those without medical insurance, the larger the proportion of medical insurance reimbursement, the less psychological pressure patients have when facing the treatment of diseases, and the better they can pay attention to their own health status, so as to improve their QOL.
The relatively low R2 values (ranging from 7.3 to 12%) across all domains (physical function, psychological function, social function, and overall QoL) indicate that the current models explain only a small proportion of the variance in quality of life outcomes. This may be attributed to several factors. First, chronic diseases are inherently complex, and their impact on QoL of patients with chronic diseases is influenced by a multitude of variables beyond those included in this study, such as genetic predispositions, environmental factors, lifestyle habits, and social determinants of health. Second, the QLICD-GM scale, while comprehensive, may not fully capture all aspects of QoL relevant to the study population. Third, the cross-sectional design of this study limits our ability to capture temporal relationships and dynamic changes in QoL over time. Future research should consider incorporating additional predictors, adopting longitudinal designs, and utilizing mixed-methods approaches that combine quantitative data with qualitative insights from interviews or focus groups to provide a more comprehensive understanding of the factors influencing QoL.
Advantages and limitations
A Multicenter Large Sample Cross-sectional Study 1953 individuals diagnosed with chronic illnesses were recruited from Dongguan, Zhanjiang and Kunming city in China. The extensive sample size coupled with a multi-center approach enhances result generalizability while providing deeper insights into current trends regarding patient QOL experiences across various regions within China. Utilizing QLICD-GM (V2.0), a standardized tool for assessing quality-of-life metrics encompassing physiological, psychological, and social dimensions enables comprehensive evaluation among individuals coping with chronic conditions.
One limitation lies in its reliance on cross-sectional methodology; thus establishing correlation rather than causation between variables impacting QOL outcomes. Future investigations might benefit from adopting longitudinal designs to track temporal changes influencing QOL in chronic disease populations. Moreover, relatively low R2 values may be caused by unobserved cofounder variables such as lifestyle habits, and environmental and social determinants of health. In addition, although the participants demonstrated diverse geographic representation, the sample selection was limited to hospitalized patients, which may introduce selection bias. Consequently, the overall representativeness of the sample may still be somewhat constrained. It is recommended that future studies expand regional diversity, include a broader range of populations, and broaden the spectrum of diseases to enhance the generalizability of the findings. Future inquiries could incorporate interventional trials aimed at evaluating intervention efficacy and feasibility.
Conclusions
In conclusion, the quality of life of patients with chronic diseases is low, and the influencing factors of the overall quality of life mainly include occupation, marital status, medical insurance type, family economy, and age. Effective corresponding strategies and targeted management or intervention measures should be taken to improve quality of life, and it is important to give personalized treatment and nursing to patients based on various factors.
Data availability
The datasets generated and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Abbreviations
- QoL :
-
Quality of life
- QLICD-GM (V2.0):
-
General module of quality of life instruments for chronic diseases
- PSD:
-
Physical functioning domain
- PHD:
-
Psychological functioning domain
- SOD:
-
Social functioning domain
- TOT:
-
Total scale score
- COPD:
-
Chronic obstructive pulmonary disease
References
World Health Organization. World Health Statistics 2022:Monitoring Health for the SDGs, Sustainable Development Goals. Accessed August 10. (2024). https://www.who.int/publications/i/item/9789240051157
Ma, R. C. W. Epidemiology of diabetes and diabetic complications in China. Diabetologia 61 (6), 1249–1260. https://doi.org/10.1007/s00125-018-4557-7 (2018).
Zhou, M. et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet 394 (10204), 1145–1158. https://doi.org/10.1016/S0140-6736(19)30427-1 (2019).
Wan, C. et al. Development and validation of the general module of the system of quality of life instruments for chronic diseases and its comparison with SF-36. J. Pain Symptom Manage. 42 (1), 93–104. https://doi.org/10.1016/j.jpainsymman.2010.09.024 (2011).
Liu, Y. et al. Development and validation of a disease-specific quality of life measure QLICD-HY (V2.0) for patients with hypertension. Sci. Rep. 13, 12935. https://doi.org/10.1038/s41598-023-39802-2 (2023).
Qiao, L. et al. Development and validation of the coronary heart disease scale among the system of quality of life instruments for chronic diseases QLICD-CHD (V2.0) based on classical test theory and generalizability theory. Int. J. Gen. Med. 17, 1975–1989. https://doi.org/10.2147/IJGM.S447752 (2024).
Liu, Q. et al. Development and validation of the osteoporosis scale among the system of quality of life instruments for chronic diseases QLICD-OS (V2.0). BMC Geriatr. 24, 407. https://doi.org/10.1186/s12877-024-05019-9 (2024).
Rao, S. et al. Health-Related quality of life and influencing factors in coronary heart disease based on the scale QLICD-CHD (V2.0): A Cross-Sectional study. IJGM 16, 5119–5129. https://doi.org/10.2147/IJGM.S430169 (2023).
Pineda, C. N. et al. Resilience, social support, loneliness and quality of life during COVID-19 pandemic: A structural equation model. Nurse Educ. Pract. 64, 103419. https://doi.org/10.1016/j.nepr.2022.103419 (2022).
An, J. et al. Relationship of psychological factors with daily activities and quality of life in patients with chronic obstructive pulmonary disease in a Chinese rural population. Annals Palliat. Med. 10 (2), 1675684–1671684. https://doi.org/10.21037/apm-20-1151 (2021).
Vanleerberghe, P., De Witte, N., Claes, C. & Verté, D. The association between frailty and quality of life when aging in place. Arch. Gerontol. Geriatr. 85, 103915. https://doi.org/10.1016/j.archger.2019.103915 (2019).
Hjelmeland, I. H. H., Drageset, J., Nordvik, Ø. & Beisland, E. G. Quality of life in home-dwelling cancer patients aged 80 years and older: a systematic review. Health Qual. Life Outcomes. 20, 154. https://doi.org/10.1186/s12955-022-02070-1 (2022).
Chen, C. et al. Health-Related quality of life and associated factors among Oldest-Old in China. J. Nutr. Health Aging. 24 (3), 330–338. https://doi.org/10.1007/s12603-020-1327-2 (2020).
Zahlan, G. et al. Polypharmacy and excessive polypharmacy among persons living with chronic pain: A Cross-Sectional study on the prevalence and associated factors. J. Pain Res. 16, 3085–3100. https://doi.org/10.2147/JPR.S411451 (2023).
George, J., Elliott, R. A. & Stewart, D. C. A systematic review of interventions to improve medication taking in elderly patients prescribed multiple medications. Drugs Aging. 25 (4), 307–324. https://doi.org/10.2165/00002512-200825040-00004 (2008).
Ikeda, A. et al. Marital status and mortality among Japanese men and women: the Japan collaborative cohort study. BMC Public. Health. 7, 73. https://doi.org/10.1186/1471-2458-7-73 (2007).
Chen, Z. H. et al. Assessment of modifiable factors for the association of marital status with Cancer-Specific survival. JAMA Netw. Open. 4 (5), e2111813. https://doi.org/10.1001/jamanetworkopen.2021.11813 (2021).
Chen, S. et al. Health-related quality of life and its influencing factors in patients with breast cancer based on the scale QLICP-BR. Sci. Rep. 13, 15176. https://doi.org/10.1038/s41598-023-41809-8 (2023).
Chiu, S. Y. R. & Yang, Z. Influence of family income and medical insurance coverage on health-related quality of life and optimism in cancer patients at a Hong Kong private hospital: A cross-sectional study. Psychooncology 28 (10), 1971–1977. https://doi.org/10.1002/pon.5175 (2019).
Kong, L. & Zhang, H. Latent profile analysis of depression in non-hospitalized elderly patients with hypertension and its influencing factors. J. Affect. Disord. 341, 67–76. https://doi.org/10.1016/j.jad.2023.08.114 (2023).
Chen, H. et al. Quality of life and its related-influencing factors in patients with cervical cancer based on the scale QLICP-CE(V2.0). BMC Womens Health. 24, 277. https://doi.org/10.1186/s12905-024-03068-1 (2024).
Shimada, T. et al. A retrospective study on the relationship between cognitive function and social function in patients with schizophrenia. J. Clin. Med. Res. 14 (9), 348–356. https://doi.org/10.14740/jocmr4798 (2022).
Qi, Y., Liang, T. & Ye, H. Occupational status, working conditions, and health: evidence from the 2012 China labor force dynamics survey. J. Chin. Sociol. 7 (1), 14. https://doi.org/10.1186/s40711-020-00128-5 (2020).
Lopes, B., Kamau, C. & Jaspal, R. The roles of socioeconomic status, occupational health and job rank on the epidemiology of different psychiatric symptoms in a sample of UK workers. Community Ment Health J. 55 (2), 336–349. https://doi.org/10.1007/s10597-018-0259-3 (2019).
Pera, A. et al. Immunosenescence: implications for response to infection and vaccination in older people. Maturitas 82 (1), 50–55. https://doi.org/10.1016/j.maturitas.2015.05.004 (2015).
Falsarella, G. R. et al. Impact of rheumatic diseases and chronic joint symptoms on quality of life in the elderly. Arch. Gerontol. Geriatr. 54 (2), e77–82. https://doi.org/10.1016/j.archger.2011.06.038 (2012).
Giebel, C. et al. A UK survey of COVID-19 related social support closures and their effects on older people, people with dementia, and carers. Int. J. Geriatr. Psychiatry. 36 (3), 393–402. https://doi.org/10.1002/gps.5434 (2021).
Tigirigi, T. O. et al. Evaluation of the health-related quality of life and associated factors in Zimbabwean adults living with HIV: a cross-sectional study. BMC Res. Notes. 16 (1), 251. https://doi.org/10.1186/s13104-023-06536-3 (2023).
Jang, M. et al. Health-Related quality of life of Post-Stroke patients in a public hospital. Brain Neurorehabil. 17 (1), e1. https://doi.org/10.12786/bn.2024.17.e1 (2024).
Zhang, C. et al. Exploring the influencing factors of quality of life among the empty nesters in shanxi, china: a structural equation model. Health Qual. Life Outcomes. 19, 156. https://doi.org/10.1186/s12955-021-01793-x (2021).
Zhao, M., Luo, L. & zhang, C. Healthy-related quality of life in patients with cervical cancer in Southwest china: a cross-sectional study. BMC Health Serv. Res. 21, 841. https://doi.org/10.1186/s12913-021-06723-7 (2021).
Khademi, N., Saeidi, S., Zangeneh, A., Saeidi, F. & Choobtashani, M. The relationship between life satisfaction and quality of life among people living with HIV/AIDS in Kermanshah-West of Iran. Health Soc. Care Community. 28 (6), 2218–2224. https://doi.org/10.1111/hsc.13034 (2020).
Chen, P. et al. Health-Related quality of life and its influencing factors in patients with hepatitis B: A Cross-Sectional assessment in southeastern China. Can. J. Gastroenterol. Hepatol. 2021, 9937591. https://doi.org/10.1155/2021/9937591 (2021).
Mei, Y. X. et al. Health-related quality of life and its related factors in coronary heart disease patients: results from the Henan rural cohort study. Sci. Rep. 11 (1), 5011. https://doi.org/10.1038/s41598-021-84554-6 (2021).
Wang, Y. et al. Health-related quality of life in patients with esophageal cancer or precancerous lesions assessed by EQ‐5D: A multicenter cross‐sectional study. Thorac. Cancer. 11 (4), 1076–1089. https://doi.org/10.1111/1759-7714.13368 (2020).
Babiarz, K. S., Miller, G., Yi, H., Zhang, L. & Rozelle, S. New evidence on the impact of china’s new rural cooperative medical scheme and its implications for rural primary healthcare: multivariate difference-in-difference analysis. BMJ 341, c5617. https://doi.org/10.1136/bmj.c5617 (2010).
Acknowledgements
We sincerely appreciate the help of all the instructors, the contributions of all the researchers, and the time and evaluation of all the participants.
Funding
This research was funded by the National Natural Science Foundation of China (Grant No. 72164024, 71373058, 81460519).
Author information
Authors and Affiliations
Contributions
C.L. was responsible for the data analysis and the writing of the paper. W.L., Q.L. and H.D. were responsible for the data collection. C.X. and C.W. and Y.C. were responsible for the study design and methods. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study involving human subjects were reviewed and approved by the IRB (Institutional Review Board) of affiliated Hospital Guangdong Medical University (PJ2013037), and performed in accordance with the Declaration of Helsinki for ethical principles for medical research involving human subjects. Subjects participated voluntarily and provided written informed consent. All subjects gave written consent before they participated in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, C., Chen, Y., Li, W. et al. A multicenter cross-sectional study on quality of life and influencing factors in patients with 10 kinds of chronic diseases. Sci Rep 15, 21246 (2025). https://doi.org/10.1038/s41598-025-05353-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05353-x
