
Abstract
Proton pump inhibitors (PPIs) are commonly prescribed medications, but their relationship to mortality in colorectal cancer (CRC) remains poorly understood. This study aims to evaluate the association between PPI use and all-cause mortality IN newly diagnosed CRC. This retrospective cohort study utilized electronic medical records from a network comprising over 80 million patients across 57 healthcare organizations in the USA. We identified adult patients with a first-time CRC diagnosis between January 1, 2010, and December 31, 2022, ensuring at least one year of follow-up. Patients were classified as new users or non-users of PPIs at the time of CRC diagnosis. A lag time of 6 months was adopted to minimize protopathic bias. The primary outcome was all-cause mortality. Patients in the study group were matched with patients controls by using 1:1 propensity matching. The analysis included 252,022 patients (126,011 PPI users and 126,011 non-users) matched on propensity scores. PPI users had a higher mortality risk at 1 year (HR = 1.42), 2 years (HR = 1.44), and over the entire follow-up period (HR = 1.40). Sensitivity analyses, which excluded early outcomes, and ancillary analyses, which compared to those on histamine-2 receptor antagonists, confirmed the robustness of these results. Even for former PPI users, the all-cause mortality HR was 1.39. PPI use was associated with an increased risk of all-cause mortality in CRC patients. These findings highlight the need for further research to explore the underlying mechanisms and clinical implications of PPI use in this population. The study indicates that PPIs are associated with increased all-cause mortality in CRC. This highlights the need for careful consideration when prescribing PPIs to this population.
Similar content being viewed by others

Introduction
The incidence of colorectal cancer (CRC) has been rising worldwide and now accounts for approximately 10% of all cancer cases. In addition, CRC is the third most often diagnosed cancer and the third most common cause of cancer-related death in both men and women in the United States1. The prognosis is not solely due to the characteristics of the cancer itself; it also depends on host and microenvironment factors2. Alterations in the microenvironment can influence the behavior of cancer and patient outcomes, encompassing elements like diet, medication, and microbiota3.
Several plausible biological mechanisms suggest that several medications, like aspirin4,5, metformin4,5, and statins6, may reduce the risk of CRC and/or improve its prognosis. On the other hand, epidemiological studies in noncancer populations suggest an association between proton pump inhibitors (PPI) use and higher CRC risk. Some observational studies found a greater risk of CRC with PPI use7,8. However, others disagree9,10,11,12,13. Therefore, the clinical relationship between PPI usage and the incidence of CRC needs to be determined, and additional investigations are important7,11,13. Furthermore, there is a notable lack of literature on the relationship of PPIs to survival in CRC.
A few studies have identified a negative association between PPI and cancer prognosis14,15. In two recent epidemiological studies, an association between PPI use and higher CRC-specific mortality was observed16,17. However, a Canadian study revealed a 34% greater all-cause mortality with PPI use18. Conversely, in another tumor site in untreated head and neck squamous cell cancer, in a cohort of 596 patients with the use of either PPIs or Histamine 2 receptor antagonists (H2RAs) was linked to longer overall survival19. Although PPIs are most often prescribed for upper gastrointestinal symptoms, PPIs might affect cancer outcomes by modifying the acidic tumor microenvironment or enhancing cancer cells chemosensitivity20. Consequently, the relationship of PPIs with CRC survival remains inconclusive, necessitating further investigation.
Prior population-based studies evaluating the association between PPI and CRC survival have had conflicting results. This discrepancy can be attributed to their limitations, including time-related biases, such as immortal time bias and protopathic bias. In addition, a recent study revealed that over a quarter of patients undergoing anticancer treatment were concurrently on PPIs21. This highlights their widespread utilization within the cancer population. In light of this, the primary objective of our population-based study was to assess whether PPI use was correlated with a greater risk of all-cause CRC mortality.
Methods
Data sources
We used electronic medical records from the TriNetX research network (Cambridge, MA, USA) to investigate any association between PPIs and all-cause mortality. The electronic supplementary material Methods contains details of the data source, quality checks, and diagnosis codes for patient selection (according to predefined International Classification of Diseases (ICD)-9 and ICD-10 codes). The TriNetX network HAS been described in previous reports22,23. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. All methods were carried out in accordance with relevant guidelines and regulations.
Study design and study participants
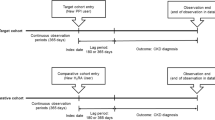
This was a large, population-based, retrospective cohort study. We identified all adults (aged ≥ 18 years) with a first-time CRC diagnosis from January 1, 2010, to December 31, 2022. The identification of CRC was based on specific predefined ICD-9 and ICD-10 codes. We limited the study cohort to at least 1 year of follow-up. Furthermore, to reduce reverse causality and detection bias, we only included individuals with > 1 year of follow-up after the start of the study. Patients were followed from the first date of CRC diagnosis to any cause of death or the end of the study (December 31, 2022), whichever occurred first.
Drug exposure
We adopted a new-user, active comparator design, which compared those newly treated with PPIs (esomeprazole, lansoprazole, omeprazole, pantoprazole, or rabeprazole) with non-users. We used non-users as primary analysis controls, defined as either H2RAs or PPIs. Finally, as recommended in the literature, we used a lag time of 6 months to allow for a sufficient latency period and minimize reverse causality (protopathic bias)24,25. Given the potential association between PPIs and a higher risk of developing CRC, we defined non-users as individuals without a recorded PPI prescription post-diagnosis. If individuals using PPIs are exposed from the moment of CRC diagnosis, it could introduce an immortal time bias because mortality cannot occur before the first use of PPI post-diagnosis.
Outcome
The primary outcome was all-cause mortality.
Matching process
We used a propensity score match (PSM) method to compare new PPI users and non-users. The PSM was performed using 1:1 to reduce confounding effects. The covariates were adjusted in the PSM model for priori-identified potential confounders, like age, sex, race/ethnicity, nicotine dependence, body mass index, cancer type, comorbidities, and medications (Table 1). Logistic regression obtained the propensity scores, and a greedy nearest-neighbor matching algorithm performed the matching with a caliper of 0.1 pooled SD. The balance of potential confounding variables was evaluated using standardized mean differences (SMD) with a threshold set a- priori at 0.10. We used SMD to measure the magnitude of differences between groups (rather than the p-value) because of their insensitivity to sample size. Logistic regression was performed using both Python (Python Software Foundation, Wilmington, Delaware, USA) and R 3.4.4 software (R Foundation for Statistical Computing, Vienna, Austria) to ensure outputs matched and the order of the rows in the covariate matrix was randomized to eliminate this bias.
Statistical analyses
All analyses were done using the TriNetX real-time analytics platform. This involved dynamic and immediate data analysis, enabling continuous processing and interpretation. Categorical variables with the Pearson χ2 test and continuous variables were compared using an independent-sample t-test. Continuous variables were expressed as mean ± SD and categorical variables as frequency and percentage. Analyses examined the outcome by using Cox proportional hazards models. HRs and CIs, along with tests for proportionality, were calculated using R’s Survival package v3.2-3. The results were validated by comparison with the output from SAS version 9.4. Patients were censored when the time window ended or the day after the last fact in their record. We utilized a 1:1 propensity matching strategy to establish comparable groups, including PPIs, H2RAs, and non-users. In addition, we used this approach to effectively balance covariates between the groups. We incorporated a robust variance estimator in the Cox regression model to account for clustering within the 1:1 propensity-matched sample and address any loss of independence among individuals from the matching procedure26. The robust variance estimator is essential to enhance the accuracy of our analytical approach and ensure study validity. A priori-defined two-sided alpha of < 0.05 indicated statistical significance.
Ancillary analysis
We analyzed new users of H2RAs (cimetidine, famotidine, nizatidine, and ranitidine) as a control in the ancillary analysis. In this, we matched new users of PPIs to new H2RA users on propensity scores. We deliberately chose H2RAs as the comparator because H2RAs are a clinically relevant cohort used for indications similar to PPIs; hence, H2RAs were chosen as it was aimed to minimize confounding by therapeutic indication. Concurrent prescriptions of PPIs and H2RAs at cohort entry were excluded to ensure a clear distinction between exposure groups. Furthermore, the study cohort included individuals who switched to or added on treatment between the study drug classes (PPI to H2RA or vice versa).
Sensitivity analyses
We conducted four sensitivity analyses to ensure robustness due to the study outcome’s heterogeneous nature. In the first analysis, we evaluated the relationship of PPI use to mortality using Cox proportional hazards models with a lag time of 24, and 36 months. Both used the same methods as the primary analysis. In the second analysis, we compared former users based on whether they had a history of PPIs before cancer diagnosis. In the third analysis, we estimated study outcomes by excluding outcomes 6 months and 1 year after the index event. In the fourth analysis, we compared former users based on whether they had a history of PPIs or H2RA before cancer diagnosis. All the analyses were performed the same methods as the primary analysis.
Results
Baseline characteristics (PPIs vs. Non-users)
In this cohort study, we examined the baseline characteristics and laboratory findings of 208,443 PPI users and 127,122 non-users with colorectal cancer before and after propensity score matching. Post-matching, each group contained 127,106 individuals (Supplementary Fig. 1). The average age of PPI users was 69.1 years (SD = 14.6) before matching, compared to 67.3 years (SD = 15.2) among non-users. Post-matching, the ages were comparable (67.5 years, SD = 15.0 vs. 67.3 years, SD = 15.2). Female representation was similar across both groups, with a slightly lower disparity post-matching (51.7% vs. 54.4% pre-matching; 54.5% vs. 54.4% post-matching, Table 1). The mean follow-up was 3.6 ± 1.1 years for the PPI group and 3.1 ± 1.0 years for the non-users.
Before matching, notable differences in health-related conditions were observed. PPI users had lower rates of alcohol and nicotine dependence, and other conditions like diabetes mellitus, hypertension, hyperlipidemia, and various cardiovascular and pulmonary diseases also differed (Table 1). After matching, these differences were significantly less, indicating effective matching. Specific gastrointestinal indications for PPI use, like gastroesophageal reflux disease and gastritis, showed expected variations between the groups but converged post-match (Table 1). Significant differences were found in cancer stage and treatment. The use of antineoplastics, chemotherapy, and surgery was more frequent among PPI users than non-users before matching. Post-matching adjustments effectively balanced these differences, particularly the utilization of specific cancer therapies and surgical interventions (Table 1).
Outcomes (Risk of mortality relative to non-users)
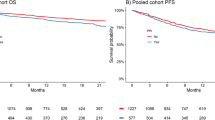
For the primary outcome assessed at 1 year, PPI users had a substantially higher mortality rate than non-users, with 7862 events in PPI versus 5563 in the non-PPI (HR = 1.42 (95% CI: 1.37–1.47). After 2 years, there were higher than 13304 events in the PPI versus 9419 in the non-users (HR = 1.44 (95% CI: 1.39–1.58). Throughout the total follow-up period, the cumulative incidence of death was 22190 for PPI users and 17277 for non-users (HR = 1.40 (95% CI: 1.29–1.61), Table 2).
Secondary analysis considered the effect of delayed exposure by 12 months to account for potential latency effects. At 12 months, the HR fell to 1.21 (95% CI: 1.16–1.54) for PPI users (Table 3). These findings suggest that earlier PPI is associated with a higher mortality risk, but this appears to decrease over time.
Ancillary analysis (H2RAs comparison)
Clinical characteristics of the PPIs and H2RA groups are compared in Supplementary Table 1. Post-matching, each group contained 127,106 individuals (Supplementary Fig. 2). The mean follow-up was 3.8 ± 1.0 years for the PPIs and 3.1 ± 1.1 years for the H2RA group. When comparing PPI to H2RA, among the 127,106 using PPIs, 32,481 deaths were recorded, whereas, among the 127,106 H2RA users, 30,301 deaths were observed. The hazard ratio (HR) for all-cause mortality in PPI users compared to H2RA users was 1.12 (95% CI: 1.05–1.68), a 12% greater risk of death in PPI users (Supplemental Table 2).
Sensitivity analysis
To assess the robustness of our findings, a time-stratified analysis showed variations in the hazard ratios for all-cause mortality at different intervals. At two years, the HR was 1.02 (95% CI: 1.01–1.05), with 21,030 PPI users and 20,749 deaths in H2RA users. At three years, the HR was 1.02 (95% CI: 1.00-1.04), with 24,867 deaths in PPI users and 24,633 in H2RA users (Supplemental Table 3).
In the second analysis, we examined all-cause mortality among former PPI users compared to non-PPI users, matching baseline characteristics in another cohort of 131,116 patients each. The HR for all-cause mortality among former PPI users was 1.39 (95% CI: 1.37–1.42, Supplemental Table 4). In a third analysis, we excluded outcomes from the first few months of the study. After excluding the first 6, and 12-month periods, the mortality HR for PPI users versus non-users was between 1.32 and 1.41 (Supplemental Table 5). In our fourth analysis, among former users, the all-cause mortality analysis included 131,126 former PPI users and 131,126 former H2RA users. There were 35,827 deaths among former PPI users compared to 35,668 deaths among former H2RA users. The hazard ratio for all-cause mortality in former PPI users versus former H2RA users was 1.01 (95% CI: 1.00-1.03, Supplemental Table 6).
Discussion
The primary objective of this study was to analyze all-cause mortality in CRC new users of acid suppression with PPI, H2RA, or non-users. We observed a moderate independent effect of new PPI use relative to non-users. PPI users had a 42% higher risk of all-cause mortality at 1 year (HR = 1.42) and a 44% higher risk after two years (HR = 1.44). These findings were confirmed in the sensitivity analysis, which excluded those who died within 1 year of index CRC diagnosis. The cumulative incidence of all-cause mortality risk over the follow-up period was 40% higher for PPI users (HR = 1.40). Even though the all-cause mortality risk seemed to decrease when accounting for delayed exposure, with an adjusted HR of 21% higher mortality (HR = 1.21), the overall risk remains substantial. Similarly, compared to those on H2RAs, the all-cause mortality risk for PPI users was 12% higher (HR = 1.12). New PPI users after CRC diagnosis who continued PPI treatment (compared to non-users) also showed a consistent yet small greater all-cause mortality through 3 years when varying the exposure ascertainment period.
PPIs are commonly used among cancer patients to prevent gastric ulceration that can result from chemotherapy, corticosteroids, and radiotherapy27,28. Furthermore, PPI use has been correlated to poorer overall health29. Specifically, PPIs may be associated with poorer overall health in CRC. The potential mechanisms underlying the possible effect of PPIs on CRC development warrant exploration. A systematic review highlighted that PPIs may not stimulate CRC development via the trophic effect of gastrin (as previously suggested)30. Instead, PPIs might paradoxically inhibit CRC development, possibly through their anti-tumor properties, mainly exhibited by omeprazole and pantoprazole. Moreover, certain PPIs, such as omeprazole and pantoprazole, are potential inhibitors of T lymphokine-activated killer cell-originated protein kinase, which could contribute to anti-tumor effects. In addition, PPI can also induce gut dysbiosis through their direct action on the HK/ATPase pump, which reduces gastric acidity31. This reduction in gastric acidity can lead to dysbiosis, gut microbiota overgrowth, and an increase in nitrites and N-nitroso compounds, which are carcinogenic. Additionally, dysbiosis caused by PPIs could result in increased altered autophagy, drug metabolism, or immunosuppression32,33,34.
Several studies have found an adverse relationship between PPI use and CRC prognosis. In a retrospective population-based study in Taiwan with nearly 21,000 patients in each cohort35, PPI use was associated with higher all-cause and cancer-specific mortality, with a dose-response effect evident. Notably, PPI use was not associated with earlier recurrence; a lower risk was noted in PPI users (although without a dose-response effect). Others reported similar findings36, i.e. PPI use during adjuvant Cape/CAPOX therapy was associated with poorer progression-free survival (PFS) and overall survival (OS). Furthermore, a post-hoc analysis of the AXEPT trial revealed that while there was improved survival with FOLFIRI in PPI users, no detriment was observed in PPI users on XELIRI15. However, the overall interaction by PPI treatment was significant for OS/PFS, which suggested a complex relationship between PPI use and treatment outcomes.
Other studies have also contributed to understanding the interaction of PPI use with CRC prognosis. A Danish population-based registry study found no association between PPI use and CRC prognosis37. However, Wong et al.17. suggested that adjuvant CAPOX plus PPI was associated with lower recurrence-free survival, unlike the lack of a similar association with FOLFOX. Chu et al.38. reported findings from a prospective study in gastrointestinal cancers, indicating that PPI use alongside CAPOX+/- lapatinib led to poorer PFS and OS than non-users. Graham et al.18 also noted that PPI use at CRC diagnosis was associated with shorter OS regardless of stage.
In contrast, several studies did not establish a clear association between PPI use and CRC prognosis. One suggested no association of PPI use with CRC prognosis in primarily early-stage CRC patients39. Similarly, others found no association of pathologic response to neoadjuvant treatment with PPI use, although higher rates of adverse events were noted34. Lin et al.23. conducted a meta-analysis and reported no clear association between PPI use and OS or PFS in Cape-based regimens. Still, subgroup analysis suggested a potential negative effect in early-stage PPI + Cape users. Wang et al.17. also showed that there was no significant association between PPI use and CRC prognosis in their studies.
Given the heterogeneous nature of CRC and the multifactorial influences on prognosis, study findings may arise due to differences in patient populations, study designs, treatment protocols, and outcome measures. In light of these diverse findings, it is imperative to consider the nuanced relationship between PPI use and CRC prognosis, highlighting the need for further research.
Our study also has several strengths. It is the largest study to date to examine the association of PPI with all-cause mortality in CRC, consisting of ‘real-world’ data with long follow-up times. First, we analyzed large population-based, multicentre data nationwide from healthcare organizations. Second, baselines and potential confounders were adjusted to create a robust control group. Third, the large sample size in the propensity-matched analyses resulted in narrower CIs, demonstrating higher precision. Hence, using PSM provided additional strength to the study. Furthermore, we used a new user cohort study design as a comparator, which reduced the potential for unmeasured confounding35. We used a detailed view of the association between PPI use and overall mortality by comparing it with H2RA users. Finally, our study highlighted the effects of immortal-time; when we used a time-varying approach to account for immortal-time bias, we found that PPI use was associated with higher mortality in CRC. The present study offers valuable insights into the relationship between PPI use and colorectal cancer outcomes. Moreover, the meticulous methodology in data collection and analysis enhances credibility. By rigorously controlling for confounding variables and utilizing robust statistical methods, we have strived to minimize bias and ensure reliability. Additionally, the large sample size and longitudinal nature provide a solid foundation for meaningful conclusions. Another major strength lies in its large sample size (high number of events > 30,000 deaths) and the robustness of the analytic methods, including propensity score matching.
Several limitations are noteworthy. First, the retrospective design and the reliance on an EHR-based database limited our results. Data from EHR-based databases are susceptible to coding errors whenever patient information is translated into diagnosis codes. Standardized measures identified cases to minimize documentation errors. Second, we did not account for some residual confounding - even after adjusting potential confounders. However, we used new users as a cohort to reduce the potential for unmeasured confounding. In addition, the “new user” criteria excluded only those with recorded PPI prescriptions 12 months prior, potentially overlooking prior use. Third, we lacked information about disease stage and grade, family history, and genetic risk factors. In addition, information on cancer stage, chemotherapy, and radiotherapy was unavailable for all patients. The cancer stage critically influences both prognosis and treatment decisions. Without this information, it is challenging to contextualize the effects of PPI use across different CRC profiles. However, medication prescription is not synonymous with actual adherence, as some patients may have been prescribed but did not take the medication. In addition, during the study period, some PPIs became available as over-the-counter medications, making it impossible to account for them. In addition, this study lacks information about PPI dosage, hampering the assessment of their potential association with treatment outcomes. This limitation could lead to inaccurate estimates of exposure and, consequently, the association with mortality. Drug adherence may be misclassified, but such misclassification would probably attenuate a correlation with PPI use, underestimating the “true” effect. We were also unable to account for the PPI therapeutic indication. We also did not differentiate between PPI types used by participants. Since different PPIs may have varying degrees of enzyme inhibition and drug interactions, this could significantly influence the specific effects of individual drugs. Fourth, the exclusion of details on anti-EGFR treatments is another limitation, particularly given the importance of EGFR pathways in CRC and the potential for PPI pharmacokinetic interactions. This omission could lead to an incomplete view of the factors influencing mortality in our cohort. The TriNetX database does not provide detailed information on whether patients underwent curative surgery or had advanced CRC. Therefore, we were unable to assess whether the increased mortality risk associated with PPI use differs between these groups. Future studies should investigate this potential difference. Finally, our study did not measure other clinical endpoints, like cause-specific mortality and progression-free survival, due to a lack of detailed clinical information in the dataset.
Conclusions
PPIs were associated with higher all-cause mortality in our CRC cohort. In line with this, our results suggest that PPI use may negatively affect the prognosis of CRC patients, which was supported by our statistically significant findings showing an association between post-diagnostic PPI use and all-cause mortality. Whether the use of PPIs is causally linked or contributes to a higher mortality risk in CRC, the findings have significant implications for better PPI prescribing. This could involve avoiding unnecessary use or reducing the duration as clinically indicated, given that assuming they are entirely harmless may be inappropriate. However, given the limitation of retrospective data, there remains a need for larger prospective studies to further investigate the causality of this association by extending the follow-up period, minimizing the potential impact of confounding, and evaluating the optimal timing for initiation. Additionally, microbiota changes in CRC patients treated with PPIs would be useful in identifying when the negative impacts of PPIs may appear. In addition, given the complexity of CRC etiology, further research is warranted to elucidate the mechanisms and clinical implications of PPI use in CRC management.
Data availability
Data is provided within the manuscript or supplementary information files. All data generated or analysed during this study are included in this published article and its supplementary information file.
Abbreviations
- CRC:
-
Colorectal cancer
- CI:
-
Confidence interval
- H2RA:
-
Histamine-2 receptor antagonists
- HR:
-
Hazard ratio
- ICD:
-
International classification of diseases
- OS:
-
Overall survival
- PPI:
-
Proton pump inhibitors
- PSM:
-
Propensity score match
- PFS:
-
Progression-free survival
- STROBE:
-
Strengthening the reporting of observational studies in epidemiology
- SMD:
-
Standardized mean differences
References
Siegel, R. L., Wagle, N. S., Cercek, A., Smith, R. A. & Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 73, 233–254 (2023).
Baghban, R. et al. Tumor microenvironment complexity and therapeutic implications at a glance. Cell. Commun. Signal. 18, 59 (2020).
Prendeville, H. & Lynch, L. Diet, lipids, and antitumor immunity. Cell. Mol. Immunol. 19, 432–444 (2022).
Sehdev, A. et al. Metformin for primary colorectal cancer prevention in patients with diabetes: a case-control study in a US population. Cancer 121, 1071–1078 (2015).
De Monte, A. et al. Metformin and aspirin treatment could lead to an improved survival rate for type 2 diabetic patients with stage II and III colorectal adenocarcinoma relative to non-diabetic patients. Mol. Clin. Oncol. 8, 504–512 (2018).
Rodríguez-Miguel, A. et al. Statins and colorectal Cancer risk: A Population-Based Case-Control study and synthesis of the epidemiological evidence. J. Clin. Med. 11, 1528 (2022).
Hwang, I. C., Chang, J. & Park, S. M. Emerging hazard effects of proton pump inhibitor on the risk of colorectal cancer in low-risk populations: A Korean nationwide prospective cohort study. PLoS One. 12, e0189114 (2017).
Lei, W. Y. et al. Association between use of proton pump inhibitors and colorectal cancer: A nationwide population-based study. Clin. Res. Hepatol. Gastroenterol. 45, 101397 (2021).
van Soest, E. M. et al. Proton pump inhibitors and the risk of colorectal cancer. Am. J. Gastroenterol. 103, 966–973 (2008).
Chubak, J., Boudreau, D. M., Rulyak, S. J. & Mandelson, M. T. Colorectal cancer risk in relation to use of acid suppressive medications. Pharmacoepidemiol Drug Saf. 18, 540–544 (2009).
Lee, J. K. et al. Proton pump inhibitor use and risk of gastric, colorectal, liver, and pancreatic cancers in a Community-Based population. Am. J. Gastroenterol. 115, 706–715 (2020).
Babic, A. et al. Acid-suppressive medications and risk of colorectal cancer: results from three large prospective cohort studies. Br. J. Cancer. 123, 844–851 (2020).
Abrahami, D. et al. Proton pump inhibitors and risk of colorectal cancer. Gut 71, 111–118 (2022).
Fais, S. Evidence-based support for the use of proton pump inhibitors in cancer therapy. J. Transl Med. 13, 368 (2015).
Tvingsholm, S. A., Dehlendorff, C., Østerlind, K., Friis, S. & Jäättelä, M. Proton pump inhibitor use and cancer mortality. Int. J. Cancer. 143, 1315–1326 (2018).
Wang, X. et al. Proton pump inhibitors and survival in patients with colorectal cancer: a Swedish population-based cohort study. Br. J. Cancer. 125, 893–900 (2021).
Graham, C. et al. A retrospective analysis of the role of proton pump inhibitors in colorectal cancer disease survival. Curr. Oncol. 23, 583–588 (2016).
Papagerakis, S. et al. Proton pump inhibitors and Histamine 2 blockers are associated with improved overall survival in patients with head and neck squamous carcinoma. Cancer Prev. Res. (Phila). 7, 1258–1269 (2014).
Spugnini, E. P. & Fais, S. Drug repurposing for anticancer therapies. A lesson from proton pump inhibitors. Expert Opin. Ther. Pat. 30, 15–25 (2020).
Raoul, J. L. et al. Prevalence of proton pump inhibitor use among patients with Cancer. JAMA Netw. Open. 4, e2113739 (2021).
Krishnan, A., Sims, O. T., Surapaneni, P. K., Woreta, T. A. & Alqahtani, S. A. Risk of adverse cardiovascular outcomes among people with HIV and nonalcoholic fatty liver disease. AIDS 37 (8), 1209–1216 (2023).
Krishnan, A. et al. Cardiovascular and mortality outcomes with GLP-1 receptor agonists vs other glucose-lowering drugs in individuals with NAFLD and type 2 diabetes: a large population-based matched cohort study. Diabetologia 67, 483–493 (2024).
Pottegård, A., Friis, S., Stürmer, T., Hallas, J. & Bahmanyar, S. Considerations for pharmacoepidemiological studies of Drug-Cancer associations. Basic. Clin. Pharmacol. Toxicol. 122, 451–459 (2018).
Pottegård, A. & Hallas, J. New use of prescription drugs prior to a cancer diagnosis. Pharmacoepidemiol Drug Saf. 26, 223–227 (2017).
Austin, P. C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 33, 1242–1258 (2014).
Uchiyama, A. A. T. et al. Proton pump inhibitors and oncologic treatment efficacy: A practical review of the literature for oncologists. Curr. Oncol. 28, 783–799 (2021).
Raoul, J. L., Moreau-Bachelard, C., Gilabert, M., Edeline, J. & Frénel, J. S. Drug-drug interactions with proton pump inhibitors in cancer patients: An underrecognized cause of treatment failure. ESMO Open. 8, 100880 (2023).
Xie, Y. et al. Estimates of all cause mortality and cause specific mortality associated with proton pump inhibitors among US veterans: Cohort study. BMJ 365, l1580 (2019).
Patel, A., Spychalski, P., Antoszewska, M., Regula, J. & Kobiela, J. Proton pump inhibitors and colorectal cancer: A systematic review. World J. Gastroenterol. 27, 7716–7733 (2021).
Bruno, G. et al. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J. Gastroenterol. 25, 2706–2719 (2019).
Clooney, A. G. et al. A comparison of the gut Microbiome between long-term users and non-users of proton pump inhibitors. Aliment. Pharmacol. Ther. 43, 974–984 (2016).
Imhann, F. et al. Proton pump inhibitors affect the gut Microbiome. Gut 65, 740–748 (2016).
Singh, A., Cresci, G. A. & Kirby, D. F. Proton pump inhibitors: Risks and rewards and emerging consequences to the gut Microbiome. Nutr. Clin. Pract. 33, 614–624 (2018).
Wu, C. C. et al. Long-Term usage of proton pump inhibitors associated with prognosis in patients with colorectal Cancer. Cancers (Basel). 15, 5304 (2023).
Kitazume, Y. et al. Proton pump inhibitors affect capecitabine efficacy in patients with stage II-III colorectal cancer: A multicenter retrospective study. Sci. Rep. 12, 6561 (2022).
Kim, S. Y. et al. Proton pump inhibitor use and the efficacy of chemotherapy in metastatic colorectal cancer: A post hoc analysis of a randomized phase III trial (AXEPT). Oncologist 26, e954–e962 (2021).
Chu, M. P. et al. Association of proton pump inhibitors and capecitabine efficacy in advanced gastroesophageal cancer: secondary analysis of the TRIO-013/LOGiC randomized clinical trial. JAMA Oncol. 3, 767–773 (2017).
Obeidat, A. E., Monti, G., Choi, H. & Acoba, J. The effect of proton pump inhibitor use on survival of patients with colorectal cancer: A study of a Racially diverse population. Cureus 15, e38707 (2023).
Cesca, M. G. et al. Influence of proton pump inhibitors on the pathological response of rectal cancer: A multicentre study. Ecancermedicalscience 17, 1586 (2023).
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
AK contributed to the concept of the study and study design. AK was responsible for data acquisition and statistical analysis. AK, CVS, and KCK drafted the manuscript and participated in literature research. All authors were involved with the interpretation of the data and critically revised the manuscript for important intellectual content. AK and SAA provided administrative, technical, and material support. DW and SAA supervised the project. AK is the guarantor of integrity of the entire study, has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors declare no conflict of interest.
Ethics approval
TriNetX data have been granted a waiver from the Western institutional review board as a federated network since only aggregated counts and statistical summaries of de-identified information.
Informed consent
Due to the study’s retrospective nature and de-identified data, TriNetX data have been granted a waiver from the Western institutional review board and waived the need to obtain informed consent.
Consent to participate
Not applicable.
Patients consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Krishnan, A., Schneider, C.V., Kadakia, K.C. et al. Proton pump inhibitors and all-cause mortality in colorectal cancer. Sci Rep 15, 21315 (2025). https://doi.org/10.1038/s41598-025-05570-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-05570-4
