
Abstract
Late recurrence of renal cell carcinoma (RCC) is observed in some postoperative patients. In addition, some of these patients do not continue postoperative follow-up. Improving the regular follow-up process for the increased convenience of patients is expected. This aimed to assess the follow-up of patients after surgery for RCC. We initiated the relationship between Chiba University Hospital and Clinics project, which is ongoing. In this prospective, observational study, postoperative patients were asked to attend follow-ups in urology clinics. Imaging was performed at nearby imaging clinics. A total of 404 patients with RCC who underwent radical and/or partial nephrectomy were included in this analysis. A total of 283 patients continued follow-up at university hospitals and 121 patients were followed up in clinics. The median follow-up was 12.4 months. Patients with a long postoperative observation period tended to request continued follow-up at a university hospital. Patients living in municipalities with affiliated clinics were more likely to request follow-up at these clinics. The total loss to follow-up rate was lower than previous data showed. Comprehensive QOL and serum creatinine concentrations were not decreased in clinic group. This is the first study successfully collaborated with clinics in follow-up observation after RCC surgery.
Similar content being viewed by others
Introduction
About 2–3% of adult malignancies worldwide is Renal cell carcinoma (RCC). More than 400,000 cases are diagnosed newly in each year. Over 170,000 deaths were occurred in 20201. Nowadays, the number of patients with localized RCC that was detected early has increased owing to an improvement in diagnostic imaging technology and the increase in thorough physical examinations. The prognosis of patients undergoing curative treatment such as surgery has also greatly improved. Approximately 7–30% of RCC patients performed curative surgery, such as partial or radical nephrectomy, relapse within 5 years, while another 20–40% develop metastases after image-based diagnosed cure2. There have also been some reports of late recurrence after curative surgery3,4,5. These reports suggest that patients should be followed up after RCC surgery throughout their lives5.
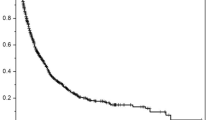
We previously reported that, even when patients are given outpatient appointments, 50% of patients are lost to follow-up within 25 years. About 2% of postoperative patients per year did not return for their scheduled follow-up visit. This number is not small, and there is a need to pursue ways to make it easier for patients to visit the hospital6. In addition, recurrence of RCC 5 years after curative surgery was observed. This result suggests that some patients who have surgery for RCC are lost during follow-up, delaying the detection of recurrence and resulting in subsequent death. On the other hand, we believe that patients at high risk of recurrence who require imaging examinations more than twice a year should continue to receive close examinations in university hospital. With the remarkable improvement in systemic treatment results for metastatic RCC in recent years, the prognosis may be improved by discerning metastatic RCC at a more appropriate time7,8,9,10,11. Regional collaboration for observation after curative surgery is essential to widely provide high-intensity RCC treatment.
There are no definitive biomarkers that predict late recurrence of RCC12. We believe that lifelong follow-up with imaging studies should be performed in patients who have surgery for RCC. We initiated the Relationship between Chiba University Hospital and Clinics (RCC) project in 2021. This is a prospective, observational study in which patients choose a university hospital or a nearby clinic for follow-up after radical surgery. There have not been any prospective studies in which patients were followed up at a urology clinic using a nearby imaging clinic after radical treatment for RCC. We report the preliminary results 1 year after starting the RCC project.
Methods
Study protocol
We started the RCC project in August 2021. We obtained approval for the study protocol from the Chiba University Ethics Review (IRB: M10055). The purpose of this study was a reduction in loss to follow-up, early detection of late recurrence, long-term changes in renal function, and long-term changes in quality of life (QOL). We hope to improve the overall survival rate by detecting recurrence early.
Definition of “Lost follow-up”
We identified patients who did not visit university hospital or the clinic on the scheduled outpatient day and contacted them by phone. We collect data from both the university hospital and clinic groups every March, then select and call that patients. We encouraged them to continue visiting again, and if we could not contact them at that time or they refused to visit again, we considered them lost to follow-up. Therefore, we did not define lost follow-up as cases of death, transfers to other hospitals, or termination of hospital visits at the discretion of the physician or at the patient’s request. If the patient died, the data were censored on the day of death. In addition, when a patient was referred to another hospital, the data were censored on the day of referral.
We recommended that postoperative patients should be followed up in cooperating urology clinics. Associated clinics are within a 30 km radius of the university hospital. The number of clinics has gradually increased, and currently, eight facilities are participating. Before starting this project, we explained this research to doctors in the clinic and confirmed their intention to participate. After starting this project, we had multiple meetings to determine the best way to carry out this research.
Inclusion criteria
This study included patients with no evidence of metastasis or recurrence more than 6 months after radical nephrectomy or partial nephrectomy for RCC. Patients with prolonged postoperative complications were excluded. We obtained written informed consent from all nonmetastatic patients who were followed up at the start of the study and from all patients who met the criteria after the start of the study. All patients participating in this study received informed written consent before beginning the study. When we explained to patients about participation in this study, we asked them to choose a clinic that was close to their home or easy to visit. Patients who accepted the clinic follow-up suggestion were followed up by a clinic. Patients who did not accept were continuously followed up by a university hospital. Information was collected prospectively.
Follow-up system
The follow-up system consists of systemic imaging, blood tests, quality of life surveys, and medical interviews. Imaging was mainly performed using computed tomography (CT). CT scans were generally performed once a year, and up to twice a year as required. In principle, if CT images were taken more than twice a year, follow-up was continued at a university hospital according to guideline. The decision of whether to perform contrast imaging was decided upon consultation between the attending physician and the patient. Diagnostic imaging was performed at a university hospital and clinics. In clinic follow-up, patients had a medical examination in a urology clinic and imaging at a radiology clinic. The diagnostic imaging clinic also performed interpretation of CT images. Therefore, the quality of image interpretation is the same at university hospitals and clinics. We created a system that allows patients to promptly return to the university hospital if a suspected recurrence is detected at the clinic.
Data collection
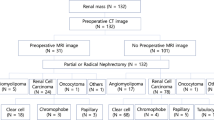
Data were anonymized and sent electronically from the clinic to the university hospital once a year. The first data collection was conducted in March 2023. At the time of registration for this study, information on age, sex, age at surgery, method of radical surgery, stage, and histopathological type were collected. Survival, loss to follow-up, change in the FACT-G7 QOL score (https://www.facit.org/measures/fact-g7), and serum creatinine concentrations during the observation period were evaluated. The reason why FACT-G7 was adopted for QOL evaluation is that it can be easily evaluated continuously in a short period of time in daily medical treatment. The reasons for refusing cooperation with the clinic were also collected. A study flowchart is shown in Fig. 1.

Schema of the RCC project according to the role of the university hospital and clinics.
Statistical analysis
Evaluation of QOL was performed after obtaining permission from the patients after the FACT-G7 was applied. Evaluations were conducted at enrollment in the study and 1 year later. All statistical comparisons between two groups were analyzed by Pearson’s chi-square test and Student’s t test. P values < 0.05 were considered statistically significant. This is a 1-year follow-up report and no survival time analysis was performed. All statistical analyses were performed using JMP version 16 (SAS Institute, Cary, NC, USA).
Results
Actual regional cooperation
A total of 404 patients who underwent radical and/or partial nephrectomy consented to participate in the RCC project. Table 1 shows the patients’ background data. A total of 283 patients selected follow-up by a university hospital, and 121 patients consented to follow-up by cooperating urology clinics. The median follow-up of the RCC project was 12.4 months.
Patients with a long postoperative observation period more frequently requested continued follow-up at a university hospital than those with follow-up at a clinic (P = 0.0122). Patients in the university hospital group were significantly older than those in the clinic group (P = 0.0144). The rate of total nephrectomy was higher in the university hospital group than in the clinic group (P = 0.0046). There were more T1 cases in the clinic group (P = 0.0389). There was no significant difference in sex, stage, histopathological type, ASA-PS or Charlson-Comorbidity index between the groups.
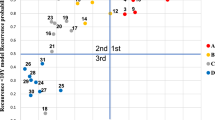
Figure 2 shows the distribution of patients in Chiba Prefecture and Chiba City with the clinic follow-up rate categorized by the patient’s address. A traffic map of Chiba Prefecture can be found on the Chiba Prefectural Government website (https://www.pref.chiba.lg.jp/). In Funabashi City and Ichihara City, more than 50% of patients consented to follow-up in clinics. In these cities, there are multiple cooperating clinics. However, in the east of Chiba Prefecture, where there is no cooperating clinic, patients tended to select university hospital follow-up.

Clinic follow-up rate categorized by the patient’s address. Chiba University Hospital and cooperating clinics are shown in the map. Bold font indicates municipalities with clinics that have participated since the start of the study. The left of the figure shows a map of the entire Chiba Prefecture and the right shows an enlarged map of Chiba City.
Actual events
Figure 3 show the actual events that occurred in patients in the RCC project. In the university hospital group, two patients had recurrence of RCC in this follow-up period. They had started systemic therapy. In the clinic group, two patients had a suspicion of recurrence and returned to the university hospital. As a result of re-evaluation, no recurrence was found in either case. One patient was re-referred to the clinic. We were able to respond promptly when a recurrence was suspected in a clinic follow-up.

Events during the follow-up in this study.
Loss to follow-up rate
In our previous study, 1.8% of patients were lost to follow-up after 1 year. (6) In this study, four (1.0%) patients were lost to follow-up. In the university group, two (0.7%) patients were lost to follow-up. Additionally, in the clinic group, two (1.6%) patients were lost to follow-up during observation (Table 1). After the RCC project started, the total loss to follow-up rate was decreased (P < 0.001).
Change in QOL and renal function
We evaluated QOL using the FACT-G7 at the time of registration in the RCC project and at 1 year after starting the project. Figure 4 shows changes in FACT-G7 QOL scores. In the university hospital group, GF5, GF3, GF7 scores were significantly higher after 1 year of follow-up than those at the beginning of the study (P = 0.001, P = 0.003, and P = 0.047, respectively). In the clinic group, although the GF5 score was significantly lower after 1 year of follow-up than that at the beginning of the study, and this result was more than “somewhat such as level2.” (P = 0.010). There was no significant decline in the overall GF7 score in either group, and QOL was maintained.

Comparison of the mean FACT-G7 QOL score between the beginning of the study and after 1 year in the university hospital group (A) and in the clinic group (B).
Evaluation of renal function was necessary because the patients had undergone radical treatment for RCC. Serum creatinine concentrations were not significantly different between both groups (Fig. 5). This finding confirmed that kidney function can be monitored through blood sampling even after a clinic follow-up.

Comparison of mean serum creatinine concentrations in the university group and in the clinic group. Patients on hemodialysis were excluded.
Discussion
We have created a system for follow-up after RCC surgery in collaboration with clinics, which has not been possible in Japan until the current study. Although the collaboration rate of the clinics was not high, we were able to identify some issues. Collaboration with the university hospital was possible when recurrence was suspected, and continued follow-up observation was also possible. We also found that clinic collaboration was adequate in managing renal function and maintaining comprehensive QOL score. We speculate that participation in this study has increased awareness of recurrence after RCC surgery and reduced lost follow-up.
First, there were significant differences between the university hospital and clinic follow-up groups in this study. Compared to the clinic follow-up group, the university hospital follow-up group was older, had more radical nephrectomy cases, had fewer T1 cases, and the period between surgery and enrollment in this study was longer. Patients with a high risk of recurrence were more likely to have preferred university hospitals, and this may have been influenced by the preferences of their attending physicians when patient selected the follow-up location.
The progress of RCC treatment is worthy of attention 7,8,9,10,11 and the specialty of treatment has increased13. This trend is toward centering in Japan. To confirm the presence or absence of recurrence, regular follow-up is required after curative surgery. The main purpose of follow-up after RCC surgery is to detect recurrence or metastasis in the earlier because no specific tumor markers for RCC have been identified yet. Therefore, the focus of follow-up relies on imaging modalities, such as CT and magnetic resonance imaging. Detection in earlier for recurrence and metastasis enables resection of recurrent and metastatic foci. Even if surgical resection is difficult, the effect of various treatments, such as immunotherapy and molecular targeted therapy, can prolong the RCC prognosis14,15,16. Although many studies have been made to identify risk factors for recurrence and metastasis after RCC surgery, an appropriate protocol for postoperative follow-up has not yet been established. Some patients who have surgery for RCC do not continue visiting the hospital during follow-up required by the doctor, delaying the detection of recurrence and resulting in subsequent death6.
We recommend that lifelong follow-up with imaging studies should be performed for patients who have surgery for RCC. Regional cooperation is essential to receive the best treatment for as many people as possible. Additionally, creating a regional follow-up system for patients who have had surgery for renal cancer in the suburbs of Chiba City, where diagnostic imaging clinics are widespread, is necessary. In this study, we collected data (loss to follow-up, early detection of recurrence, long-term changes in renal function, and long-term changes in QOL) in postoperative university hospital or clinic follow-up of RCC, and focused on regional medical cooperation with urology clinics. The study’s primary endpoint was to improve the overall survival rate.
In our previous study cohort, approximately 50% of patients were lost to follow-up 25 years after surgery6. Among these patients, there was a risk of recurrence in approximately 20% of stage I patients and in approximately 50% of stage II and III patients. Further analysis of risk factors for loss to follow-up showed that an older age (≥ 62 years) was the strongest factor, and other major factors were clear cell RCC and no recurrence of the tumor. In our previous study, if a patient was unable to attend the hospital because of death due to other causes, this was not included in a lost follow-up event6. We anticipated that patients living in distant regions would be more likely to be lost to follow-up, although we found that the patient’s address relative to the location of the hospital was not a significant factor in this loss.
The reason why older people are more likely to be lost to follow-up is thought to be the difficulty of visiting hospitals. If these older people could be followed up in their own area, consistent follow-up might be established. In this study, in Chiba City in which there are cooperating clinics, patents tended to consent to follow-up in clinics. A large number of cooperating clinics in a wide area is an important issue for the RCC project.
This study showed several patient preferences. As the follow-up period becomes longer after surgery, coordinating with the clinic becomes more difficult. This difficulty increases trust in the doctor who performed the surgery and the patient becomes accustomed to going to the hospital, making collaboration with clinics difficult. On the basis of these results, we are currently informing patients that we will cooperate with the clinic before and during surgery. Another important factor is the location of the affiliated clinic. Patients residing in municipalities with affiliated clinics had a high rate of clinic collaboration. Expanding the number of affiliated clinics is a future challenge. However, there is also the issue of increasing the amount of data collection. We cannot increase the number of affiliated clinics without addressing this issue.
Two clinic-affiliated patients were suspected of recurrence during the observation period. We were promptly contacted by a doctor at the clinic, and the patients visited a university hospital for another thorough examination. This situation enabled a quick response.
In this study, the 1-year loss to follow-up rate after the RCC project was less than that reported previously by our research team (Fig. 2)6. The medical system in our previous study was not the same as that in the current study. Therefore, comparison between the two studies is difficult. However, the RCC project may be helpful for reducing loss to follow-up. We will continue to collect data longitudinally and observe changes in loss to follow-up.
Maintaining the patient’s QOL is an important issue. In this study, patients in the university hospital group and the clinic group did not show a compromise in almost all QOL subgroups. Some QOL scores were increasing. The only worsening was GF5 (sleep quality) in the clinic group. Although the detailed reasons are unknown, there was no decline in GE6 (anxiety) or GF7 (comprehensive QOL). Follow-up in the clinic did not result in a decline in GF7. These results will be useful information for promoting clinic collaboration to patients in the future.
Renal function was similar between the groups in this study. Serum creatinine concentrations were not significantly different between the groups. Regarding renal function, collecting longitudinal data is important because there are many cases of long-term survival after surgery.
This study has several limitations. First, the follow-up period was not long. The overall survival rate could not be evaluated because the observation period was too short, and the number of events was limited. We plan to continue this research in the future. Second, regional cooperation differs depending on the living environment, and the results will not be the same in all regions. In this study, we conducted our research in Chiba Prefecture, which is next to Tokyo. Third, at the time we started this project, some patients were in the hospital more than 30 years after they had surgery. Therefore, we are not only recruiting new patients. Fourth, regarding QOL, we adopted the FACT-G7 for simplicity. Although a more detailed QOL evaluation is desirable, continuing the evaluation longitudinally is necessary. Therefore, we decided to choose a simple QOL assessment.
To the best of our knowledge, this is the first prospective, observational study to successfully collaborate with clinics in follow-up observation after RCC surgery. Currently, when surgery and systemic treatment are rapidly evolving, there is an extremely high demand for post-surgery regional collaboration. We believe that the establishment of a follow-up system after RCC surgery, in which imaging follow-up is the main method, will lead to further activation of advanced treatment at the hospital, leading to improved survival rates in the long term. This study needs to be continued in the future to confirm whether long-term survival rates are improved.
Data availability
The data presented in this study are available on request from the corresponding author.
Abbreviations
- CT:
-
Computed tomography
- QOL:
-
Quality of life
- RCC:
-
Renal cell carcinoma
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Dabestani, S., Marconi, L., Kuusk, T. & Bex, A. Follow-up after curative treatment of localised renal cell carcinoma. World J. Urol. 36(12), 1953–1959 (2018).
Frees, S. K. et al. Risk-adjusted proposal for >60 months follow up after surgical treatment of organ-confined renal cell carcinoma according to life expectancy. Int. J. Urol. 26(3), 385–390 (2019).
Stewart-Merrill, S. B. et al. Oncologic surveillance after surgical resection for renal cell carcinoma: a novel risk-based approach. J. Clin. Oncol. 33(35), 4151–4157 (2015).
Shindo, T. et al. Long-term outcome of small, organ-confined renal cell carcinoma (RCC) is not always favourable. BJU Int. 111(6), 941–945 (2013).
Arai, T. et al. A clinical investigation of recurrence and lost follow-up after renal cell carcinoma surgery: a single-center, long-term, large cohort, retrospective study. Int. J. Clin. Oncol. 27(9), 1467–1476 (2022).
Albiges, L. et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 4-year follow-up of the phase III CheckMate 214 trial. ESMO Open. 5(6), e001079 (2020).
Plimack, E. R. et al. Pembrolizumab plus axitinib versus sunitinib as first-line treatment of advanced renal cell carcinoma: 43-month follow-up of the phase 3 KEYNOTE-426 study. Eur. Urol. (2023).
Choueiri, T. K. et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 384(9), 829–841 (2021).
Motzer, R. et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N. Engl. J. Med. 384(14), 1289–1300 (2021).
Haanen, J. et al. Extended follow-up from JAVELIN Renal 101: subgroup analysis of avelumab plus axitinib versus sunitinib by the International Metastatic Renal Cell Carcinoma Database Consortium risk group in patients with advanced renal cell carcinoma. ESMO Open. 8(3), 101210 (2023).
Richards, K. A. & Abel, E. J. Surveillance following surgery for nonmetastatic renal cell carcinoma. Curr. Opin. Urol. 26(5), 432–438 (2016).
Calpin, G. G., Ryan, F. R., McHugh, F. T. & McGuire, B. B. Comparing the outcomes of open, laparoscopic and robot-assisted partial nephrectomy: a network meta-analysis. BJU Int. 132(4), 353–364 (2023).
Aurilio, G. et al. Image-guided ablations in patients with recurrent renal cell carcinoma. J. Clin. Med. 12(15) (2023).
Marconi, L. et al. Local treatment of recurrent renal cell carcinoma may have a significant survival effect across all risk-of-recurrence groups. Eur. Urol. Open Sci. 47, 65–72 (2023).
Lloyd, A., Reeves, F., Abu-Ghanem, Y. & Challacombe, B. Metastasectomy in renal cell carcinoma: where are we now?. Curr. Opin. Urol. 32(6), 627–633 (2022).
Acknowledgements
We thank Ellen Knapp, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
The present study was supported by a Grant-in-Aid for Scientific Research (C) (22K09494 to T.S.).
Author information
Authors and Affiliations
Contributions
R.T. contributed to data collection and analysis, table and figure preparation, reference collection, and manuscript writing. T.S. contributed to designing this project, data collection and analysis, table and figure preparation, reference collection, and manuscript writing. H.S. and T.A. contributed to data collection and analysis and supervised all parts of the research. M.K., K.A., Y.Y., Y.G., Y.I., S.S., J.R., H.K., K.M., Y.S., K.S., M.Y. and M.M. contributed to data collection. T.I. contributed to the supervision of all parts of the research. The first draft of the manuscript was prepared by R.T and T.S. All authors have read and approved the published version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
The protocol for this research project has been approved by a suitably constituted Ethics Committee of the institution, and it conforms to the provisions of the Declaration of Helsinki. This study was approved by the Institutional Review Board of Chiba University Hospital (IRB no. M10055).
Informed consent
Informed consent for publication was obtained from the patients.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tsukamoto, R., Sazuka, T., Sato, H. et al. Initial report of prospective study of regional cooperation for imaging-based follow-up after curative renal cell carcinoma surgery. Sci Rep 15, 21306 (2025). https://doi.org/10.1038/s41598-025-06635-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-06635-0
