
Abstract
This study investigated the impact of post-traumatic kyphosis (PTK) on the lumbar spine using a local Cobb angle of 30° as the cutoff point. The measurements included the local Cobb angle, lumbar lordosis angle (L1–L5), intervertebral space angle (IVSA), lumbar disc degeneration, and posterior wall height loss (PWHL). Patient characteristics such as sex, age, disease duration, American Spinal Injury Association (ASIA) grade, fracture site, bone mineral density (BMD), Oswestry Disability Index (ODI), and visual analogue scale (VAS) score were also recorded. Patients were divided into two groups based on the thoracolumbar local Cobb angle: Group 1 (local Cobb angle > 30°, n = 48) and Group 2 (local Cobb angle ≤ 30°, n = 28). Comparative analysis revealed that Group 1 had a significantly longer disease duration, higher VAS and ODI scores, greater lumbar lordosis angle, increased L4/5 IVSA, and more severe lumbar disc degeneration (p < 0.05). Furthermore, across all patients, disease duration, lumbar lordosis angle, and L4/5 IVSA were positively correlated with the local Cobb angle (p < 0.05). These findings suggest that when the local Cobb angle exceeds 30°, PTK may aggravate lumbar degeneration.
Similar content being viewed by others
Introduction
The thoracolumbar segment (T11–L2) is the junction point between the physiological kyphosis of the thoracic vertebra and the physiological lordosis of the lumbar vertebra, which is an essential biological stress hinge area of the human spine1,2,3. Patients with thoracolumbar fractures are more likely to experience post-traumatic thoracolumbar kyphosis (PTK)1,4. PTK is the result of malunion of thoracolumbar fractures caused by various reasons in the early stage of trauma, and the main reasons for PTK include failed diagnosis or non-formal treatment4,5,6.
When patients with PTK are in an unbalanced state of the thoracolumbar segment, it leads to excessive lordosis of the lumbar spine to regulate the balance of the entire spine, often leading to issues such as low back pain, nerve damage, and aesthetics, affecting the quality of life of patients; in severe cases, respiratory and abdominal organ functions are threatened7,8,9,10,11. The selection of surgical timing for patients with PTK is controversial, and surgical treatment at different periods will lead to various postoperative complications. It is widely accepted that surgical intervention should be performed when the local Cobb angle is 30°–40°12,13. Simultaneously, in the preoperative examination of these patients, we found that the lumbar lordosis angle increased significantly, resulting in deterioration of the overall spinal balance. Few studies have analysed the effect of local kyphosis on the compensatory lordosis of the lumbar spine in patients with PTK.
Our study had several objectives: (1) to measure the thoracolumbar local Cobb angle and lumbar lordosis parameters using radiography and MRI, and (2) to compare the differences in the parameters of the lumbar spine. (3) To investigate the compensation and degeneration of the lumbar vertebrae in patients with PTK, analyse its pathogenesis, and explore its clinical significance.
Methods
Patients
This was a retrospective radiographic study. This study was approved by the Ethics Committee of the Affiliated Hospital of Southwest Medical University and strictly followed the guidelines of the Declaration of Helsinki (KY2024098). The ethics committee approved the waiver of written informed consent. We collected information from patients admitted to our hospital for kyphosis between January 2018 and December 2021.
The inclusion criteria were: (i) patients aged >18 years, (ii) a clear history of trauma without formal surgery treatment, (iii) single vertebral body fracture (T11-L2), (iv) no history of thoracolumbar surgery, and (v) Bone mineral density (BMD, T-Score >-2.5). The exclusion criteria were: (i) course of fracture not less than 6 months, (ii) other serious lumbar degenerative diseases (severe lumbar spondylolisthesis, congenital spinal stenosis, scoliosis, etc.), (iii) spinal infection, (iv) craniocerebral diseases and spinal cord neuropathy, and (v) severe hip and knee diseases and unequal length of the lower limbs.
Finally, 76 patients met the inclusion and exclusion criteria (Fig. 1), who were then divided into two groups according to the local Cobb angle. The first group was Cobb angle > 30 °(Group1, n = 48), and the second group was Cobb angle ≤ 30 °(Group2, n = 28).

Case screening flow chart.
Radiographic assessment
Pretreatment radiologic parameters were measured using plain radiography, including the local Cobb angle, lumbar lordosis angle, intervertebral space angle (IVSA), and posterior wall height loss (PWHL). The degree of disc degeneration was assessed using MRI according to the modified disc degeneration grading system proposed by Pfirrmann14.
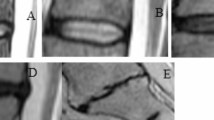
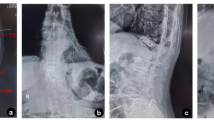
The local Cobb angle was defined as the angle formed by the upper endplate of the adjacent vertebral body above the injured vertebral body and the adjacent vertebral body below the injured vertebra (Fig. 2a)15. The lumbar lordosis angle was defined as the angle between the upper endplate of L1 and the lower endplate of L5 (Fig. 2b)16. The IVSA was defined as the angle between the lower endplate of the upper vertebra and the upper endplate of the lower vertebra (Fig. 2c). The PWHL of the injured vertebral body was measured using the following formula: PWHL = (2×P1)/(P2 + P3), where P1 was the height of the posterior wall of the injured vertebral body; P2, was the height of the posterior wall of the adjacent vertebral body above the injured vertebra, and P3 was the height of the posterior wall of the adjacent vertebral body below the injured vertebral body (Fig. 2d). According to PWHL, the fracture type was divided into burst fracture (PWHL ≤ 0.80) and compression fracture (PWHL > 0.80)17.

Relevant parameters were measured in all enrolled cases. (a) Local Cobb angle was defined as the angle formed by the upper end plate of the adjacent vertebral body above the injured vertebra and the adjacent vertebral body below the injured vertebra. (b) The lumbar lordosis angle was defined as the angle between the upper end plate of L1 and the lower end plate of L5. (c) Intervertebral space angle was defined as the angle between the lower end plate of the upper vertebral and the upper end plate of the lower vertebral(α, β, γ, θ, δ). (d) Posterior wall height loss = (2×P1)/(P2 + P3); P1, the height of the posterior wall of the injured vertebral body; P2, the height of the posterior wall of the adjacent vertebral body above the injured vertebral; P3, the height of the posterior wall of the adjacent vertebral body below the injured vertebral.
General information
Data on sex, age, disease duration, American Spinal Injury Association (ASIA) grade, fracture site, BMD, Oswestry Disability Index (ODI), and visual analogue scale (VAS) scores were obtained from clinical notes and evaluated.
Statistical analysis
All statistical analyses were performed using SPSS software (version 26.0; IBM, Armonk, NY, USA). Counting data were expressed as percentages, and measurement data were expressed as mean ± standard deviation (SD). A Student t test or a nonparametric test and X2 test were used to evaluate differences between the two groups. Logistic regression was used to analyse the influence of controlling disease duration factors on the degree of disc degeneration, and Spearman’s correlation coefficient was used for correlation analysis.
Results
Patient characteristics
A total of 76 patients with PTK, there were 23 men and 53 women (average age, 61.45 ± 9.91 years; range, 32–84 years). The average local Cobb angle was 37.13°±15.61° (range, 16°–119°). The average disease duration was 8.01 ± 7.37 years (range, 0.6–40 years). The average lumbar lordosis angel was 46.67°±13.29° (range, 10.20°–85.40°). Injured vertebrae included T11 (n = 16), T12 (n = 25), L1 (n = 23), and L2 (n = 12). The fracture types included burst (n = 39) and compression (n = 37) fractures.
Comparison of general information
Age, sex, ASIA grade, fracture site, fracture type, and BMD were not significantly different between the two groups (P > 0.05). Disease duration, VAS, and ODI were significantly different between the two groups (Group1 vs. Group2, 9.87 ± 7.85years vs. 4.81 ± 5.16years, 4.60 ± 1.50 vs. 3.39 ± 0.97, 28.21 ± 6.50 vs. 21.64 ± 4.40; p < 0.05) (Table 1).
Comparison of imaging parameters
There were no significant differences in the parameters of L1/2, L2/3, L3/4, and L5/S1 IVSA between the two groups (P > 0.05). The lumbar lordosis angle, L4-5 IVSA and L2/3 as well as L3/4 and L4/5 disc degeneration were significantly different between the two groups (Group1 vs. Group2, 51.24°±12.01°vs. 38.83°±11.78°, 13.46°± 4.48°vs. 10.41°± 4.09°; p < 0.05)(Table 2).
Correlation analysis
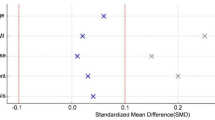
The Spearman’s correlation analysis showed that the Cobb angle was significantly positively correlated with the lumbar lordosis angle (r = 0.558, p < 0.05), disease duration (r = 0.584, p < 0.05), and L4/5 IVSA (r = 0.475, p < 0.05) (Fig. 3).

Correlation of the local Cobb angle with lumbar lordosis angle, course of disease, and L4/5 intervertebral space angle. The local Cobb angle was positively correlated with the lumbar lordosis angle (a), the L4/5 intervertebral space angle (b), and the disease course (c).
Discussion
In this study, we found that when the local Cobb angle in patients with PTK was greater than 30°, the lumbar spine would appear to have obvious compensatory lordosis. The main compensatory segment was L4/5, and the degree of lumbar disc degeneration was aggravated. Patients experience lower back pain, nerve damage, and other clinical symptoms affecting their quality of life.
Over the past few decades, increasing attention has been paid to the importance of sagittal spinal balance and lumbar degeneration18,19. However, few studies have focused on the functional and structural effects on the lumbar spine in patients with PTK. The current evidence suggests a significant correlation between thoracolumbar kyphosis and lumbar lordosis in the normal population20,21. When the spine maintains its physiological curvature, the gravitational line of the body passes through the junctions of these curves22. Owing to the rigid thoracic spine above and the relatively mobile lumbar spine below, the thoracolumbar junction becomes a region of stress concentration and is thus the most common site of thoracolumbar fractures18,19. If such fractures are not managed in a timely or appropriate manner, they may progress to PTK, a severe complication of vertebral fractures. Inadequate restoration of the vertebral body height leads to local sagittal imbalance, contributing to paraspinal muscle fatigue and chronic low back pain. Symptoms are often more pronounced when the local Cobb angle exceeds 30°23,24.
As kyphotic deformity worsens, the centre of gravity shifts anteriorly. To maintain postural balance, the body compensates by increasing lumbar lordosis. However, this adaptation places considerable strain on the posterior musculature above the deformity, which is subjected to prolonged tension to maintain non-physiological alignment25,26. Over time, this leads to muscular fatigue and dysfunction, perpetuating a vicious cycle in which forward weight shift exacerbates kyphosis27,28. This cycle not only increases the mechanical load on the lumbar spine but also accelerates disc degeneration, which may result in secondary lumbar pathologies such as disc herniation, spinal stenosis, and spondylolisthesis29. Age-related changes in bone quality play a critical role in this process. With aging, a decline in BMD, trabecular thinning, and cortical bone loss compromise the mechanical integrity of the vertebral30,31. These changes significantly increase the risk of vertebral collapse, progressive wedge deformity, and kyphotic progression following fractures, further aggravating the global sagittal imbalance32,33.
Previous studies have consistently demonstrated that the lower lumbar segments exhibit significantly greater mobility than superior levels, with the L4/5 motion segment demonstrating the most pronounced kinematic characteristics34. This transitional zone plays a pivotal role in maintaining the lumbar biomechanical function and withstanding dynamic loads, rendering it particularly vulnerable to degenerative changes. Anatomically, the L4/5 segment serves as a primary contributor to the lumbar lordotic curvature and demonstrates remarkable compensatory mobility during sagittal imbalance35,36. This study revealed statistically significant differences (P < 0.05) in both IVSA and disc degeneration severity at the L4/5 level between the two groups. This finding is consistent with the unique anatomical structure and functional characteristics of the L4/5 segment. Based on previous literature and our results, we conclude that the L4/5 segment is not only the primary regulatory zone for compensatory lumbar lordosis, but also the most sensitive area for lumbar degeneration in patients with PTK. Degeneration at this segment may directly affect the compensatory efficiency and maintenance of overall sagittal balance. Therefore, L4/5 should be regarded as an important target for the evaluation and management of PTK-related low back pain, especially in patients undergoing nonoperative management.
Numerous studies have reported that early surgical intervention may help prevent the further progression of local kyphosis and lumbar degeneration in patients with PTK37. Surgical planning poses significant challenges in patients with severe deformities and long-standing multi-level compensatory mechanisms. Traditional procedures such as Smith-Petersen osteotomy (SPO) and pedicle subtraction osteotomy (PSO) have been widely used to correct PTK. However, these techniques are associated with extensive osteotomy, substantial intraoperative blood loss, and potential risks such as spinal cord shortening38,39,40. Recently, alternative techniques such as spinal joint release (SJR), proposed by Wang et al., have been reported to achieve sagittal correction with significantly less osteotomy and blood loss, offering a promising new surgical option for PTK41. Nevertheless, BMD remains a key determinant of surgical outcomes. If BMD is not adequately evaluated and optimised preoperatively, there is a heightened risk of complications such as implant failure and correction loss. Preoperative planning should incorporate BMD assessment and appropriate osteoporosis treatment, particularly in patients scheduled for corrective osteotomy or fusion procedures42. Ensuring adequate screw purchases and a favourable environment for bone fusion are essential. In patients with severe sagittal imbalance and limited compensatory capacity, more extensive correction strategies, including multilevel osteotomy or cement augmentation, may be required to restore alignment and enhance construct stability43. Based on the findings of this study, surgical intervention may be considered when the local kyphosis angle in PTK patients exceeds 30°. However, the local kyphosis angle alone should not serve as the sole criterion for surgical decision making. A comprehensive assessment should include the degree of local kyphosis, lumbar compensatory capacity, extent of intervertebral disc degeneration, and bone quality. These factors are essential for accurately determining the optimal timing of surgery and choosing between elective and semi-urgent procedures. Both global sagittal balance and local spinal stability should be considered to achieve precise sagittal correction. Semi-urgent surgery is recommended for patients presenting with rapidly progressing neurological symptoms or severe sagittal imbalances. Contrastingly, for patients with tolerable pain and preserved muscle function, elective surgery may be appropriate and ideally combined with preoperative rehabilitation to enhance postoperative recovery. By integrating these considerations, surgical outcomes can be optimised, the risk of postoperative complications can be reduced, and long-term prognosis can be improved.
Although our study yielded meaningful results, there were certain limitations that may affect the credibility of our findings. First, the sample size was relatively small and may not fully represent the overall population. Future studies should include a larger number of cases to provide a more comprehensive depiction of this situation. Second, measurement and observer subjectivity are inevitable. Furthermore, the relevant imaging features of patients with PTK are still under discussion and have yet to be fully validated for clinical evaluation and treatment plan selection. With advances in imaging technology, further research could offer a more detailed and accurate classification of PTK imaging features. Finally, this study did not systematically investigate the effect of the pelvic coefficient on the overall sagittal balance of the spine, nor did it observe the effects of cervical parameters on the thoracolumbar curvature, degeneration, and instability, as well as the compensation of cervical vertebrae in the whole cervical system.
Conclusion
When the local Cobb angle of patients with PTK is greater than 30°, the lumbar lordosis of the patients will be compensated for, mainly by the L4/5 segment. Simultaneously, the degree of lumbar disc degeneration in patients with PTK was aggravated. Diagnostic and treatment plans should be developed for such patients.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. This is not to restrict the use of our dataset but to allow the Research Ethics Committee of the affiliated hospital of Southwest Medical University to understand the actual use of the dataset.
References
Katsuura, Y., Osborn, J. M. & Cason, G. W. The epidemiology of thoracolumbar trauma: A meta-analysis. J. Orthop. 13, 383–388. https://doi.org/10.1016/j.jor.2016.06.019 (2016).
Lee, G., Wang, Q., Zhong, D., Li, S. & Kang, J. Relation between severity of injury and neurological deficit in thoracolumbar burst fracture. Clin. Spine Surg. 29, 208–211. https://doi.org/10.1097/BSD.0b013e3182779b9f (2016).
Cahueque, M., Cobar, A., Zuñiga, C. & Caldera, G. Management of burst fractures in the thoracolumbar spine. J. Orthop. 13, 278–281. https://doi.org/10.1016/j.jor.2016.06.007 (2016).
Wood, K. B., Li, W., Lebl, D. R. & Ploumis, A. Management of thoracolumbar spine fractures. Spine Journal: Official J. North. Am. Spine Soc. 14, 145–164. https://doi.org/10.1016/j.spinee.2012.10.041 (2014).
Mazel, C. & Ajavon, L. Malunion of post-traumatic thoracolumbar fractures. Orthop. Traumatol. Surg. Research: OTSR. 104, S55–s62. https://doi.org/10.1016/j.otsr.2017.04.018 (2018).
Bohl, M. A. et al. Posterior open-wedge anterior longitudinal ligament release: Cadaveric technique analysis. Clinical anatomy (New York, N.Y.) 32, 348–353, (2019). https://doi.org/10.1002/ca.23317
Bridwell, K. H. Decision making regarding Smith-Petersen vs. pedicle Subtraction osteotomy vs. vertebral column resection for spinal deformity. Spine 31, 171–178. https://doi.org/10.1097/01.brs.0000231963.72810.38 (2006).
Jackson, R. P. & McManus, A. C. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine 19, 1611–1618. https://doi.org/10.1097/00007632-199407001-00010 (1994).
Jang, J. S., Lee, S. H., Min, J. H. & Maeng, D. H. Influence of lumbar lordosis restoration on thoracic curve and sagittal position in lumbar degenerative kyphosis patients. Spine 34, 280–284. https://doi.org/10.1097/BRS.0b013e318191e792 (2009).
Kawahara, N. et al. Closing-opening wedge osteotomy to correct angular kyphotic deformity by a single posterior approach. Spine 26, 391–402. https://doi.org/10.1097/00007632-200102150-00016 (2001).
Schoenfeld, A. J. et al. Posttraumatic kyphosis: current state of diagnosis and treatment: results of a multinational survey of spine trauma surgeons. J. Spin. Disord. Tech. 23, e1–8. https://doi.org/10.1097/BSD.0b013e3181c03517 (2010).
Oe, S. et al. The risk of proximal junctional kyphosis decreases in patients with optimal thoracic kyphosis. Spine Deformity. 7, 759–770. https://doi.org/10.1016/j.jspd.2018.12.007 (2019).
Liu, F. Y. et al. Incidence and risk factors for proximal junctional kyphosis: a meta-analysis. Eur. Spine Journal: Official Publication Eur. Spine Soc. Eur. Spinal Deformity Soc. Eur. Sect. Cerv. Spine Res. Soc. 25, 2376–2383. https://doi.org/10.1007/s00586-016-4534-0 (2016).
Pfirrmann, C. W., Metzdorf, A., Zanetti, M., Hodler, J. & Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine 26, 1873–1878. https://doi.org/10.1097/00007632-200109010-00011 (2001).
Kuklo, T. R. et al. Measurement of thoracic and lumbar fracture kyphosis: evaluation of intraobserver, interobserver, and technique variability. Spine 26, 61–65. https://doi.org/10.1097/00007632-200101010-00012 (2001). discussion 66.
Porto, A. B. & Okazaki, V. H. A. Procedures of assessment on the quantification of thoracic kyphosis and lumbar lordosis by radiography and photogrammetry: A literature review. J. Bodyw. Mov. Ther. 21, 986–994. https://doi.org/10.1016/j.jbmt.2017.01.008 (2017).
Rajasekaran, S. et al. Osteoporotic thoracolumbar Fractures-How are they Different?-Classification and treatment algorithm. J. Orthop. Trauma. 31 (Suppl 4), S49–s56. https://doi.org/10.1097/bot.0000000000000949 (2017).
Glassman, S. D. et al. The impact of positive sagittal balance in adult spinal deformity. Spine 30, 2024–2029. https://doi.org/10.1097/01.brs.0000179086.30449.96 (2005).
Schwab, F. J. et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine 38, E803–812. https://doi.org/10.1097/BRS.0b013e318292b7b9 (2013).
Vaz, G., Roussouly, P., Berthonnaud, E. & Dimnet, J. Sagittal morphology and equilibrium of pelvis and spine. Eur. Spine Journal: Official Publication Eur. Spine Soc. Eur. Spinal Deformity Soc. Eur. Sect. Cerv. Spine Res. Soc. 11, 80–87. https://doi.org/10.1007/s005860000224 (2002).
Gelb, D. E., Lenke, L. G., Bridwell, K. H., Blanke, K. & McEnery, K. W. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 20, 1351–1358 (1995).
Le Huec, J. C., Thompson, W., Mohsinaly, Y., Barrey, C. & Faundez, A. Sagittal balance of the spine. Eur. Spine Journal: Official Publication Eur. Spine Soc. Eur. Spinal Deformity Soc. Eur. Sect. Cerv. Spine Res. Soc. 28, 1889–1905. https://doi.org/10.1007/s00586-019-06083-1 (2019).
Roberson, J. R. & Whitesides, T. E. Jr. Surgical reconstruction of late post-traumatic thoracolumbar kyphosis. Spine 10, 307–312. https://doi.org/10.1097/00007632-198505000-00003 (1985).
Malcolm, B. W., Bradford, D. S., Winter, R. B. & Chou, S. N. Post-traumatic kyphosis. A review of forty-eight surgically treated patients. J. Bone Joint Surg. Am. Vol. 63, 891–899 (1981).
Tang, M. et al. Nomogram development and validation for predicting postoperative recurrent lumbar disc herniation based on paraspinal muscle parameters. J. Pain Res. 17, 2121–2131. https://doi.org/10.2147/jpr.S459846 (2024).
Si, F. et al. Characteristics of paraspinal muscle fat infiltration in asymptomatic Chinese adults: a cross-sectional study. Quant. Imaging Med. Surg. 13, 4526–4539. https://doi.org/10.21037/qims-22-1131 (2023).
Diebo, B. G. et al. Adult spinal deformity. Lancet (London England). 394, 160–172. https://doi.org/10.1016/s0140-6736(19)31125-0 (2019).
Cui, X. L. et al. Characteristics and mechanical mechanisms of intervertebral disc degeneration in old thoracolumbar fractures with kyphosis: clinical observations and finite element analyses. BMC Musculoskelet. Disord. 25, 1040. https://doi.org/10.1186/s12891-024-08157-8 (2024).
Berven, S. H., Deviren, V., Smith, J. A., Hu, S. H. & Bradford, D. S. Management of fixed sagittal plane deformity: outcome of combined anterior and posterior surgery. Spine 28, 1710–1715. https://doi.org/10.1097/01.Brs.0000083181.25260.D6 (2003). discussion 1716.
Hart, N. H. et al. Mechanical basis of bone strength: influence of bone material, bone structure and muscle action. J. Musculoskel. Neuronal Interact. 17, 114–139 (2017).
Romero-Márquez, J. M. et al. Molecular interactions between dietary lipids and bone tissue during aging. Int. J. Mol. Sci. 22 https://doi.org/10.3390/ijms22126473 (2021).
Schmidt, T. et al. A retrospective analysis of bone mineral status in patients requiring spinal surgery. BMC Musculoskelet. Disord. 19 https://doi.org/10.1186/s12891-018-1970-5 (2018).
Kado, D. M. et al. Factors associated with kyphosis progression in older women: 15 years’ experience in the study of osteoporotic fractures. J. Bone Mineral. Research: Official J. Am. Soc. Bone Mineral. Res. 28, 179–187. https://doi.org/10.1002/jbmr.1728 (2013).
Morishita, Y., Buser, Z., D’Oro, A., Shiba, K. & Wang, J. C. Clinical relationship of degenerative changes between the cervical and lumbar spine. Asian Spine J. 12, 343–348. https://doi.org/10.4184/asj.2018.12.2.343 (2018).
Wu, M. et al. Dynamic motion characteristics of the lower lumbar spine: implication to lumbar pathology and surgical treatment. Eur. Spine Journal: Official Publication Eur. Spine Soc. Eur. Spinal Deformity Soc. Eur. Sect. Cerv. Spine Res. Soc. 23, 2350–2358. https://doi.org/10.1007/s00586-014-3316-9 (2014).
Bae, J. S., Jang, J. S., Lee, S. H. & Kim, J. U. A comparison study on the change in lumbar lordosis when standing, sitting on a chair, and sitting on the floor in normal individuals. J. Korean Neurosurg. Soc. 51, 20–23. https://doi.org/10.3340/jkns.2012.51.1.20 (2012).
Vaccaro, A. R. & Silber, J. S. Post-traumatic spinal deformity. Spine 26, 111–118. https://doi.org/10.1097/00007632-200112151-00019 (2001).
Gao, R. et al. Modified partial pedicle Subtraction osteotomy for the correction of post-traumatic thoracolumbar kyphosis. Spine Journal: Official J. North. Am. Spine Soc. 15, 2009–2015. https://doi.org/10.1016/j.spinee.2015.04.047 (2015).
Hu, W., Wang, B., Run, H., Zhang, X. & Wang, Y. Pedicle Subtraction osteotomy and disc resection with cage placement in post-traumatic thoracolumbar kyphosis, a retrospective study. J. Orthop. Surg, Res. 11, 112. https://doi.org/10.1186/s13018-016-0447-1 (2016).
Schwab, F. et al. The comprehensive anatomical spinal osteotomy classification. Neurosurgery 74, 112–120. https://doi.org/10.1227/NEU.0000000000000182o (2014). discussion 120.
Wang, Q. et al. Treatment of rigid post-traumatic thoracolumbar kyphosis by a novel technique of spinal joints release. J. Orthop. Surg, Res. 18 https://doi.org/10.1186/s13018-023-03599-7 (2023).
Bekas, K. N. & Zafeiris, C. The role of bone mineral density in a successful lumbar interbody fusion: A narrative review. Cureus 16, e54727. https://doi.org/10.7759/cureus.54727 (2024).
Schaefer, C., Mafi, A., Beil, F. T., Schroeder, M. & Rolvien, T. Skeletal status in patients scheduled for elective lumbar spine surgery: comparison of discectomy, decompression, fusion, and revision. Global Spine J. 14, 380–389. https://doi.org/10.1177/21925682221105005 (2024).
Acknowledgements
The authors are grateful for the help of the Imaging Department of the Affiliated Hospital of Southwest Medical University. This study was funded by the Science and Technology Strategic Cooperation Project between the Second People’s Hospital of Deyang City and Southwest Medical University (2022DYEXNYD007).
Author information
Authors and Affiliations
Contributions
J.J.Y. and Z.K.C. were responsible for the study concept and writing the article. Y. C. and H.Z. was responsible for reviewing and writing the article. All the authors contributed to the study conception and design. Material preparation, literature review, data collection, and quality assessment were performed by Q.W. Statistical analysis was performed by B.X.J. J.J.Y and Z.K.C. share the first authorship, due to equal contributions. The first draft of the manuscript was written by G.Z.L. and G.J.W.; J.J.Y. and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, J., Chen, Z., Chen, Y. et al. Impact of kyphosis exceeding 30° on lumbar spine in patients with post-traumatic kyphosis. Sci Rep 15, 20970 (2025). https://doi.org/10.1038/s41598-025-07046-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07046-x
