
Abstract
The nutrition transition in Small Island Developing States like Kiribati has led to a significant shift from traditional diets to processed, imported foods, resulting in a double burden of malnutrition. This study provides the first comprehensive assessment of nutrition-related health issues in Kiribati, analyzing data from a nationally representative household survey conducted in 2019–2020 (with over 12,000 participants). We examined anthropometric measures and biomarkers related to both under- and overnutrition across 21 islands, including obesity, anemia, hypertension, diabetes, and dyslipidemia. Results reveal high prevalence of overweight and obesity (78.6% in adults), alongside persistent undernutrition in children (23.9% stunting, 6.9% wasting in under-fives). Non-communicable disease indicators were alarmingly high, with 38.5% of adults having hypertension (i.e., stage 2 or hypertensive crisis), 16.5% diabetes, and 87.1% at risk for high cholesterol. Anemia affected 13.8% of the population. Age and sex were significant factors, with older individuals and women generally at higher risk for obesity and related conditions. Geographic analysis showed that total cholesterol and diabetes varied most across islands, while obesity and other markers varied more at the household level. These patterns suggest the need for both island-specific and household-level interventions. Our findings highlight the urgent need for targeted public health strategies and interventions to address the double burden of malnutrition in Kiribati. By providing baseline data on nutritional status and its geographic and demographic variations, this study informs evidence-based policies to improve food security, nutrition, and health outcomes in the face of ongoing environmental and socioeconomic challenges in this vulnerable island nation.
Similar content being viewed by others

Introduction
Given current trends in human diets, it is expected that nearly two-thirds of the global population will be either overweight or obese by 20501. The shift from undernourishment to excessive dietary consumption accompanied by increases in sedentary lifestyles, called the nutrition transition, leads to an increased prevalence of diabetes, cardiovascular disease, and other conditions related to overconsumption of ultra-processed foods that are high in sodium, sugar, and energy2,3. Of particular concern in the Global South, the double burden of malnutrition simultaneously affects vulnerable populations with a high prevalence of micronutrient deficiencies and adverse health outcomes related to food system transitions related to convenience4.
These diet related issues are critical to achieving the Sustainable Development Goals (SDG). SDG 2 (Zero Hunger) aims to end hunger, achieve food security, and promote sustainable agriculture, emphasizing the importance of access to nutritious food, which is critical for filling the micronutrient gap and preventing overconsumption related NCDs. In parallel, SDG 3 (Good Health and Well-being) focuses on ensuring healthy lives and promoting well-being for all across the life course, including the prevention of NCDs through nutrition and lifestyle factors.
SDG 12 (Responsible Consumption and Production) outlines a path toward sustainable consumption patterns, ideally following the EAT-Lancet planetary health diet5, which can help promote healthier diets and reduce food waste. These goals are also in line with the World Health Organization’s Global Nutrition Targets, which focus on reducing stunting, anemia, low birth weight, childhood overweight, and wasting6. Yet, none of these targets and SDGs can be met without cross-sectoral collaboration, relying on SDG 17 (Partnerships for the Goals), highlighting the need for global partnerships to address the challenges of obesity and malnutrition through collaborative efforts across health, environment, agriculture, economic and education sectors.
The nutrition transition is especially pronounced in Small Island Developing States (SIDS) of the Pacific where healthier traditional diets have been substituted by highly processed food products7. Cultural transitions, environmental resource degradation, and market isolation coupled with nutritionally compromising trade policies have led to food system restructuring that favors obesogenic diets8,9. In transitioning countries, the majority of food sales include sugar-sweetened beverages, noodles, cooking oils, sweets, and processed meats7. These dietary patterns, along with increases in sedentary lifestyles, have led to rapid increases in the prevalence and incidence of diet-related non-communicable disease (NCD) outcomes such as diabetes, hypertension, and cardiovascular disease.
In fact, in 2022, nine of the top ten countries most affected by adult obesity in women are all Small Island Developing States of the Pacific, ranging from 57.5% of the population in the Federated States of Micronesia to 81.5% of the population in Tonga according to modeled data from the NCD RisC Collaboration10. For adult men, the top ten countries with the highest prevalence of obesity are again nearly all Small Island Developing States of the Pacific, ranging from 47.0% in French Polynesia to 70.3% in American Samoa, with the exception of the USA ranking 10th at 41.6% prevalence. Of particular concern is the Pacific island nation of Kiribati due to its geographic isolation, declining marine resources, and increased reliance on Western foods. These shifts, with the added impacts of climate change, are likely to jeopardize food security in the near future. For women, Kiribati ranks 11th, with 57.2% of adults (18 years of age and older) classified as obese while ranking 22nd for men with 36.1% being obese. Without intervention to counter current trends, these trajectories will likely continue to worsen.
To achieve these SDGs and address the complex nutritional challenges facing SIDS we urgently need comprehensive baseline data to assess existing nutritional risks and inform evidence-based interventions. Kiribati particularly lacks information on broader diet-related health indicators, particularly biomarkers associated with the nutrition transition and the rise of non-communicable diseases. While some anthropometric data exist for the I-Kiribati population, there is a critical lack of information on broader diet-related health indicators, particularly biomarkers associated with the nutrition transition and the rise of non-communicable diseases. This study aims to fill these knowledge gaps by providing the first large-scale, nationally representative prevalence estimates of a comprehensive suite of anthropometric measures and nutritional biomarkers related to both under- and overnutrition among the I-Kiribati population11. These include measures of stunting, wasting, and overweight in children, as well as adult obesity, hypertension, diabetes, hyperglycemia, anemia, and dyslipidemia. Additionally, we quantify the demographic and geographic patterns of these nutritional conditions, including variations across islands, communities, and households. This analysis will help identify the populations and areas most in need of targeted interventions, while also examining the interplay between traditional diets, imported foods, and changing lifestyles in shaping nutritional outcomes. This research aims to provide crucial context for interpreting biomarker data and support evidence-based policy-making to improve nutrition and health outcomes in the face of ongoing environmental and socioeconomic challenges in this vulnerable Small Island Developing State.
Results
Nutritional status of the I-Kiribati people based on anthropometric assessment
The vast majority of the adult I-Kiribati population are affected by either overweight or obesity (78.6%, n = 6253), with 31.9% classified as overweight and 46.7% classified as obese (inclusive of obesity class I: 26.4%; obesity class II: 13.8%; and obesity class III: 6.4%) (Fig. 1). Only 20.4% of the adult population are considered to have normal weight, while 1.0% are classified as underweight. In children and adolescents ages 5–19 years of age inclusive (n = 3328), 0.8% of the population are classified as thin, 70.0% normal weight, 29.3% overweight or obese, of which 7.9% were affected by obesity (Fig. S1). In children under five years of age, 23.9% (n = 1436) of the population was stunted and 6.9% were wasted (Fig. S1).

Prevalence of biomarker-based health outcomes for adults. Percent observed in I-Kiribati adults by (a) body mass index classification, (b) anemia, (c) hypertension, (d) hyperglycemia, (e) hypercholesterolemia, (f) hypertriglyceridemia, and (g) diabetes separated by islands in order of population size at the time of sampling. Sample size of adults with biomarker status per island is stated on top of each panel. These are observed values (e.g., without accounting for potential demographic structures among islands). See Table S3 for the mean age of each biomarker by island. The reason for the difference in sample sizes (and number of islands included) for each biomarker relates to the research study design11 whereby anemia and anthropometry was assessed in all individuals, and all other biomarkers were assessed in a subset of individuals on only ten islands.
Classifying nutritional status based on biomarkers
The overall prevalence of anemia for individuals of all ages in Kiribati (n = 12,442), measured by hemoglobin levels, was 13.8%, with 6.3% classified as moderately anemic and 0.8% classified as severely anemic. In reproductive aged women between 15 and 49 years (n = 3821), the prevalence of anemia was 13.2% (5.8% moderate; 1.1% severe; Table 1; Fig. 1). In children under five years of age, 34.2% (n = 1609) of the population was affected by anemia (17.5% moderate; 2.7% severe Table 1).
Focusing on non-communicable disease outcomes related to the overconsumption of foods and other unhealthy behaviors, we also measured hyperglycemia, hypertension, diabetes, and cholesterol levels in individuals 18 and older (Fig. 1). The overall mean fasting blood glucose level was 128.5 mg/dL (ranging from 73.0 to 514.0) and the overall prevalence of hyperglycemia (> 180 mg/dL ) was 9.0% (n = 719) across the country. The overall prevalence of hypertension including stage 2 or hypertensive crisis (i.e. systolic blood pressure equal to or greater than 140mmHg and/or diastolic blood pressure equal to or greater than 90mmHg) in individuals 18 and older was 38.5% (n = 659), with 26.1% of the population having normal blood pressure, 5.6% with elevated levels (systolic blood pressure between 120 and 130mmHg and diastolic blood pressure below 80mmHg), and an additional 29.7% were classified with stage I that did not constitute hypertension (Table 1). Among those with hypertension, 36.4% with stage II, and 2.1% were in hypertensive crisis. Using HbA1c levels as a measure of diabetes, we found an overall prevalence of 20.2% of the population at risk of diabetes and 16.5% of the population diabetic (n = 509, HbA1c > 6.5; Table 1).
The overall prevalence of the adult population aged 18 and over deemed at risk for high total cholesterol (i.e., total cholesterol equal to or greater than 200 mg/dL, LDL cholesterol equal or greater than 130 mg/dL or HDL cholesterol below 40 mg/dL) was 87.1% (n = 619) while the adolescent population 12–17 years of age was 87.0% (n = 77). The mean levels of low-density lipoprotein (LDL) were 96.4 mg/dL (ranging from 0.0 to 225.0), high-density lipoprotein (HDL) were 34.7 mg/dL (ranging from 20.0 to 139.0), and triglycerides were 115.7 mg/dL (ranging from 40.0 to 500.0). There was an overall prevalence of 80.0% of the population with normal triglyceride values (with 12.7% being borderline, (150–199 mg/dL)), while 7.3% of the population had triglyceridemia (with 6.8% being moderate, (200–499 mg/dL) and 0.5% being severe; n = 614 (> 500 mg/dL).
Nutritional status dynamics by age and sex
After controlling for sex, increasing age was associated with an increased risk of obesity, hypertension, hyperglycemia, hypertriglyceridemia, and diabetes, while younger individuals were more likely to be at risk of anemia (Figs. 2 and 3a–f). There does not seem to be an effect of age on the risk of high total cholesterol (Fig. 2; Fig. S2). Within the adult population, both older people and women were more likely to be overweight and obese (estimated log-odds of 0.3 [0.2–0.4] (median [90% uncertainty intervals]) for standardized age and − 0.8 [− 0.8 to − 0.7] for males, respectively; Fig. 2). Younger adults and females were more likely to be anemic (estimated log-odds of − 1.8 [− 2.0 to − 1.5] for standardized age and − 0.6 [− 0.7 to − 0.5] for males, respectively). After controlling for age, men were more likely to be at risk for hypertension (log-odds of 0.4 [0.2–0.6]), high cholesterol (log-odds of 0.6 [0.3–0.9]), and triglyceridemia (log-odds of 0.4 [0.2–0.6]); while women were more likely to be at risk of hyperglycemia (log-odds for males of − 0.6 [− 0.9 to − 0.2]; Fig. 2, Fig. S3). There was no strong effect of sex observed on diabetes status (log-odds for males of − 0.05 [− 0.3 to 0.2]).

Age and sex patterns across (a) body mass index (BMI) classification, (b) anemia, (c) hypertension, (d) hyperglycemia, (e) hypercholesterolemia, (f) hypertriglyceridemia, and (g) diabetes. Points represent the median effect size (i.e., log-odds) and intervals are 90% uncertainty intervals. The dashed vertical line (at zero) represents the baseline (females and average population age).

Age trends in non-communicable disease status. Estimated probabilities of (a) body mass index (BMI) classification, (b) anemia, (c) hypertension, (d) hyperglycemia, (e) hypertriglyceridemia, and (f) diabetes as a function of age keeping all other variables constant (i.e., for our baseline sex category (females) and not including spatial group level effects). Lines are medians and polygons 90% uncertainty intervals. See Figure S1 for the remaining biomarker age trends.
As age increases, individuals become less likely to be underweight, normal weight, and overweight, and more likely to be obese (Fig. 3a). Similarly, older individuals become more prone to stage 2 hypertension and hypertensive crisis, while the likelihood of normal and elevated blood pressure declines (Fig. 3b). As low-normal levels of triglycerides become less prevalent as age increases, high-normal levels and all stages of hypertriglyceridemia increase (Fig. 3e), the same pattern holding for hyperglycemia (Fig. 3d). Lastly, older individuals become less likely to have healthy HbA1c values, and the prevalence of diabetes increases (Fig. 3f).
Geographic variation in nutritional status
When accounting for the differential age and sex structures of populations on each island, and examining the spatial variance, we found that only two of the seven examined health outcomes had the largest variation across islands (total cholesterol and diabetes; Fig. 4), indicating that risk factors among islands may be greatest for these two health challenges. Variation among communities within islands was greater than the variation across islands or across households within communities for anemia (Fig. 4), indicating that local geography within islands may present differential risk factors for anemia specifically. Lastly, four health outcomes (obesity, glucose, blood pressure, and triglyceride status) had the greatest variance among households within communities (Fig. 4), highlighting stronger behavioral than environmental risk factors.

Spatial sources of variation across measured health outcomes. Values are median estimated variances from different hierarchical levels accounting for age and sex (and smoking in the case of anemia).
Discussion
Our study, conducted in conjunction with a national socio-economic household survey, provides comprehensive statistics on a range of health outcomes related to dietary intake and nutritional status in Kiribati. This research is set against the backdrop of a dramatic nutrition transition occurring in Small Island Developing States (SIDS) across the Pacific. This transition is characterized by a shift from traditional diets - rich in locally produced fruits, vegetables, and seafood - to diets dominated by processed and imported foods high in sugars, fats, and salt8,9. Multiple factors drive this change, including ecological degradation, increased globalization, rapid urbanization, and expanding market access8. The consequences of this dietary shift are profound, manifesting in rising rates of non-communicable diseases such as obesity, diabetes, and heart disease throughout these island communities7. Compounding these challenges is the erosion of local food sovereignty and traditional agricultural practices, which further diminishes access to nutritious, locally-sourced foods.
Our research collected many measures that have been included in the Global Health Observatory Data Repository (i.e., anemia among women of reproductive age)12, the NCD Risk Factor Collaboration (NCD-Risc) estimates10,13,14, and the Joint Malnutrition Estimates Working Group15, including adult nutritional status (underweight, overweight, and obesity), child and adolescent nutritional status (thinness, overweight, and obesity), stunting, wasting, and overweight in infants and young children), hypertension and diabetes among those 18 years of age and older. Our research was the first to collect information on the prevalence of diabetes in Kiribati since 198116, when diabetes was measured using glucose rather than HbA1c as a measure, while other outcomes had been measured more recently and repeatedly. When comparing to NCD Risc’s estimates for 2019, we found that the prevalence of adult overweight and obesity was similar to our findings that 74.3% of males and 82.6% of females are overweight or obese, of which 38.3% of males and 56.8% of females are obese. While these findings for adults were similar, our findings for the prevalence of overweight and obesity among adolescents (ages 5–19) were strikingly different than the NCD Risc estimates. We found that 27.9% of males and 30.8% of females aged 5–19 were classified as overweight or obese, while NCD Risc had estimated 44.1% for males and 41.0% for females. Similarly, we found that 7.5% of males and 8.3% of females aged 5–19 were classified as obese, far lower than the 20.4% of males and 12.9% of females estimated by NCD Risc. This means we found far more adolescents to be classified as having a healthy weight (71.0% for males, and 68.7% for females) than the NCD Risc estimated (51.5% for males, and 55.0% for females). While the estimates of overweight and obesity among adolescents seem far lower than the estimates among adults, the prevalence increased from 19.5% for those aged 5–9 to 34.8% for those aged 10–14 and to 45.3% for those 15–19, showing an increased prevalence with age. While we used the same cutoffs for nutritional status as were used by NCD Risc, methodological differences may partially explain differences between our estimates and their predicted prevalence estimates. For instance, the NCD Risc estimates were age standardized using the WHO standard population and based on models that take into consideration prevalence estimates from the region and other countries from 2019 and previous years among other data.
For children 0–5 years of age, we found that 4.3% of males and 4.6% of females were considered overweight, which are higher findings than predicted by the Joint Child Malnutrition Estimates Working Group, which indicated that 3.3% of males and 0.9% of females aged 0–5 would be considered overweight in 2019. The differences were greater for measures of undernutrition among children aged 5, with our study finding that 24.9% of males and 22.7% of females were moderately or severely stunted (<-2SD). In comparison, the NCD Risc predicted 16.4% of males and 14.0% of females would be moderately or severely stunted. Based on the the Joint Child Malnutrition Estimates Working Group estimates, stunting was expected to be a medium level of public health significance (10 < 20%) in 2019; however, our findings indicate the level of public health significance is considered high (20 < 30%)17. A similar difference was found for wasting with 6.6% of males and 7.1% of females found to be moderately or severely wasted (<-2SD) in our study while the Joint Child Malnutrition Estimates Working Group predicted 3.7% of males and 3.4% of females would be moderately or severely wasted in 2019. Based on the NCD Risc estimates, wasting was expected to be a low level of public health significance (2.5 < 5%) while our findings indicate the level of public health significance is medium (5 < 10%). As described above, differences in estimates may be partially explained by methodological differences18.
Differences were also found between NCD Risc’s predictions and our findings for hypertension and diabetes among adults aged 18 years of age and older. We found that 39.9% of males and 37.3% of females were classified as hypertensive (systolic blood pressure equal to or greater than 140mmHg and/or diastolic blood pressure equal to or greater than 90mmHg) while NCD Risc predicted far lower estimates of 24.0% for males and 19.0% for females. While we used the same cutoffs for hypertension classification as NCD Risc, differences in estimates may be partially explained by methodological differences including age-standardization and our use of individuals 18 and older rather than individuals 30–69 years of age14,18. For diabetes, our estimates were lower than the NCD Risc estimates with 14.8% of males and 18.1% of females classified as diabetic in our study. NCD Risc predicted that 17.6% of males and 23.3% of females would be classified as diabetic. However, our team used Hemoglobin A1c as a more exact biomarker to assess diabetes, whereas past surveys of diabetes in 1981, 2004, and 2015–2016 all used fasting glucose as a proxy for diabetes13.
Among women of reproductive age (aged 15–49 years) we found the prevalence of anemia to be 13.2% while the Global Health Observatory Data Repository/World Health Statistics predicted that 32.6% would be found to be anemic. Based on these predictions, anemia would be considered a moderate level of public health significance (20.0 < 40.0%) while our findings would make anemia a mild level of public health significance (5.0 < 20.0%). Both our and the Global Health Observatory estimates for prevalence of anemia were based on the same WHO cutoffs for anemia by pregnancy status19; however, their 2019 projections were age standardized and modeled prevalence estimates using data from the region20. These modeled estimates were constructed without any baseline data from Kiribati because our sample collection include the first widespread measures of hemoglobin status in the country.
While these estimates are not directly comparable based on methodological and data input differences, it is informative to compare prevalence estimates in Kiribati to other SIDS, which share ongoing environmental, food system, and socioeconomic challenges. In comparison to Guell et al.21 that compares estimates for child stunting, anemia in women of reproductive age (age 15–49), obesity in children (age 5–19) and adults (age 18+), and prevalence of diabetes (age 18+) across 37 SIDS, estimates for Kiribati put it among the highest 5–10 SIDS (out of 37) for each of the included health outcomes. Using our estimates as a comparison to the other SIDS does not drastically change the rankings for Kiribati in terms of adult obesity. However, for childhood obesity, the Guell et al.21 estimates would place Kiribati among the top ten highest prevalence values while our estimates place it in the bottom ten. While our estimates for prevalence of childhood stunting are higher than theirs, both estimates place Kiribati within the top ten highest prevalences. For estimates of diabetes prevalence, comparing our estimates to other SIDS based on existing information21 only makes Kiribati fall slightly in the rankings for females but drops Kiribati out of the top ten highest prevalences for males. While the Global Health Observatory prevalence estimate for anemia among women of reproductive age places Kiribati among the highest prevalences12, our estimate would place Kiribati among the lowest – second only to Singapore. Despite these differences in data and measurement protocols, it is clear that Kiribati faces a high burden of the double burden of malnutrition.
There are several limitations to this study. First, we do not have access to comprehensive repeated measures of dietary intake information to draw robust associations with the clinical nutrition data we have produced. Secondly, many of these measures (e.g., hypertension, glucose, etc.) should be assessed multiple times before assessing a clinical diagnosis. Another weakness is that we did not use ethnic specific cut-points for anthropometric measures, although these metrics have been published22. We did, however, publish these estimates in Supplementary Table S2 to contrast with the measures we reported. Lastly, there is currently no funding in place to ensure follow-up measures to assess these conditions in the future to track and monitor trends in these important conditions that reflect responses to the nutrition transition. Nevertheless, this dataset represents a major advance in our understanding of the nutritional status of the I-Kiribati population, providing crucial decision-support data on a nationally representative sample.
As far as we are aware, these are the first measures of anemia, hypertension, diabetes, hyperglycemia, hypergtriglyceridemia, and cholesterol that had been conducted at large spatial and population scales in Kiribati11. Therefore, these data are critically important as each of these conditions has far ranging health effects that could harm the future wellbeing and productivity of the country, damaging hopes for achieving the SDGs. Anemia in pregnant women significantly increases the risk of maternal morbidity and mortality by contributing to complications such as preterm birth, low birth weight, and impaired fetal development23. Hypertension significantly elevates the risk of cardiovascular disease (CVD) and mortality by causing damage to blood vessels and the heart, often leading to heart attacks and strokes24. Diabetes and persistent hyperglycemia contribute to CVD through mechanisms like inflammation and endothelial dysfunction, increasing the likelihood of severe complications25. Adults with diabetes face a 2 to 4 times higher risk of cardiovascular issues compared to those without the condition, and this risk increases as glycemic control deteriorates26. Additionally, high triglyceride and cholesterol levels exacerbate these risks by promoting atherosclerosis, which further heightens the chances of fatal cardiovascular events27,28. These biomarker estimates should be viewed as a baseline assessment but must be evaluated repeatedly over time to both ensure an accurate diagnosis for individuals and to understand potential trajectories in non-communicable disease burden in the country.
Spatial and demographic differences in these health biomarkers could be attributed to diverse social, ecological, economic, and food system factors that vary geographically. Having analyzed the variance across islands, communities within islands, and households within communities, we can begin to understand what may be driving increases in some of these health challenges. Total cholesterol, diabetes, and anemia appear to be more geographically determined, whereas hypertension, glucose, triglycerides and obesity appear to be most variable across households within small spatial scales, indicating individual-level and household-level behavioral risk factors. These insights suggest that spatially targeted interventions can more effectively address the diverse drivers of health challenges across Kiribati. These interventions could include prioritizing environmental interventions and community-based and market-based nutrition programs on islands with high rates of diabetes and anemia, or focusing on household-level behavior change strategies (e.g., maternal education, cooking classes, voucher programs) in communities with elevated obesity and hypertension.
Beyond public health interventions that would target these diseases, policy makers must also understand the food system landscape and how that can be modified to improve these health outcomes. Kiribati’s food system faces significant challenges due to climate change, economic constraints, and limited agricultural resources. With rising sea levels causing saltwater intrusion into freshwater supplies and arable land, the cultivation of traditional crops like taro and breadfruit is threatened, limiting access to locally grown, nutrient-rich foods. At the same time, overfishing, habitat degradation, and climate-induced coral bleaching threaten coastal fish stocks and aquatic biodiversity, reducing access to traditional sources of protein and micronutrients29. As these ecological pressures worsen, Kiribati’s population becomes increasingly reliant on imported foods, including rice, canned meat, and sugar-sweetened beverages, which are high in salt, sugar, and saturated fats8,30. These parallel trajectories of ecological degradation and increased market integration will exacerbate the nutrition transition if current trajectories continue, leading to rising rates of non-communicable diseases. With high transportation costs, minimal existing distribution infrastructure (e.g., cold chains) and limited economic resources, healthy food is unavailable or prohibitively expensive for many remote island households, deepening food insecurity and health inequality. Together, these dynamics make it even more challenging to develop sustainable solutions that address both food security and public health in Kiribati.
Addressing the complex nutritional challenges faced by Kiribati requires a multifaceted approach that considers both the unique context of SIDS and the global trends driving the nutrition transition. Enhancing sustainable practices, such as integrating traditional food systems with modern agricultural techniques, could significantly improve resilience and food sovereignty31. This approach not only helps preserve cultural food heritage but also contributes to dietary diversity, which is crucial in combating both undernourishment and overconsumption. Investments in local fisheries and aquaculture are essential to diversify the food supply and reduce reliance on imported, often ultra-processed foods high in sugar, salt, and unhealthy fats32. However, these efforts must go beyond merely increasing production; they should promote equitable access to fishery resources, ensuring that benefits reach vulnerable communities and align with local consumption patterns33. As Seto et al.34 argue, fisheries investments must also reinforce existing pathways by which people actually access fisheries products, recognizing the complex social and economic factors that influence food choices. These food system interventions must be implemented in conjunction with improvements in trade policies, potentially restricting the imports of harmful dietary products, that contribute to the rising prevalence of non-communicable diseases (NCDs) such as obesity, diabetes, and cardiovascular diseases. Simultaneously, health interventions targeting sedentary lifestyles and promoting physical activity are crucial, given the high prevalence of obesity and related NCDs revealed in our study. Moreover, public health education programs could play a vital role in reshaping dietary preferences, promoting nutritious local foods, and raising awareness about the links between diet and health outcomes.
Overall, proactive measures that prioritize sustainability, community involvement, and cultural relevance will be crucial for strengthening the resilience of Kiribati’s food system in the face of looming challenges, including climate change and continued globalization. By adopting a holistic approach that integrates local knowledge, sustainable practices, equitable access, and supportive policy frameworks, Kiribati can foster a more resilient food system capable of improving public health outcomes and safeguarding future generations. This approach aligns with the Sustainable Development Goals, particularly SDG 2 (Zero Hunger), SDG 3 (Good Health and Well-being), and SDG 12 (Responsible Consumption and Production), while also addressing the unique challenges faced by SIDS in the Pacific region. Furthermore, it could serve as a model for other SIDS facing similar nutritional and environmental challenges, contributing to broader regional efforts to combat the negative impacts of the nutrition transition and move towards more sustainable and health-promoting food systems.
Methods
Study population
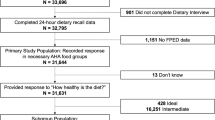
Data were drawn from subjects from the 2019–2020 Kiribati Household Income and Expenditure Survey, a nationally representative survey that is administered approximately every five years (Table S1). Anthropometric measurements (n = 12,481) and hemoglobin status (n = 12,442) were collected from individuals from 111 villages on 21 islands, and more detailed health measurements of glucose (n = 818), diabetes (i.e., Hemoglobin A1c (HbA1c); n = 670), triglycerides (n = 699), cholesterol (n = 703), and blood pressure (n = 748) were collected from individuals from 26 villages on 12 islands. All individuals within selected households were asked to participate in the research and, depending on the age of the individual, were enrolled and asked to provide comprehensive survey data and biological samples (fingernail and fingerprick of blood). Comprehensive information on randomization, recruitment, enrollment, and all other study-related methods can be found in the study protocol11.
Point-of-care analysis of biomarkers
All data and samples were collected as part of an Integrated Household Income and Expenditures Survey, administered by the Government of Kiribati and supported by the Pacific Community and several US universities: Harvard TH Chan School of Public Health, American University, University of California-Santa Barbara and University of California-Santa Cruz. A comprehensive study protocol describing all details of study design and sample collection has been published11. As part of this survey effort, clinical and anthropometric assessments were conducted in conjunction with standardized demographic and economic surveys. An I-Kiribati enumerator recorded anthropometric measurements: height/length and weight (all individuals); mid-upper arm circumference (children 5 years of age and under); and cranial circumference (children 2 years of age and under) using standardized WHO protocols35,36. Beyond anthropometry, a fingerprick of blood was collected from all individuals < 50 years of age, and hemoglobin and hematocrit measures collected through the use of a Hemochroma Plus device from Immunostics, Inc. In a subset of the surveyed population on 12 islands, a more comprehensive clinical health examination was conducted by an I-Kiribati nurse. We measured blood pressure for all individuals over 12 years of age using an OMRON 10 series monitor once participants had been seated for at least 10 min, ensuring that individuals were as relaxed as possible. We then proceeded with biological sample collection and subjects provided a maximum of three finger pricks of blood, using one 23-gauge lancet and two 30- gauge disposable lancets. Based on a subject’s age, they received a different set of tests (see Golden et al.11 for details). Using capillary whole blood, we analyzed the following using point-of-care diagnostics: (i) glucose levels with GenUltimate Blood Glucose Test Strips for use with the One Touch Ultra meter, (ii) total cholesterol, HDL cholesterol, and triglycerides using the CardioChek Plus Analyzer from PTS Diagnostics; and (iii) hemoglobin A1c (a measure of diabetes) through the use of a A1cNow + device from PTS Diagnostics.
Classifying nutritional status based on diagnostics
Anthropometric data were analyzed using standard cutoffs provided by the World Health Organization to assess nutritional status (Table S2)36. Children under 5 were assessed as underweight (weight-for-age z-score <-2), stunted [height-for-age z-score (HAZ) <-2], wasted (weight-for-height z-score <-2), and overweight (weight-for-height z-score > 2) based on the WHO Child Growth Standards36. In children aged 5–19, overweight was classified as a body-mass-index-for-age z-score (BMIZ) > 1, and obesity was classified as a BMIZ > 2. In adults aged 20 and above, body mass index (BMI) was used to classify nutritional status according to the following thresholds: underweight, BMI < 18.5; 18.5–24.9, normal weight; 25.0–29.9, overweight; 30.0–34.9, obesity class I; 35.0–39.9, obesity class II; and > 40, obesity class III. Outliers were classified as WAZ or HAZ > |6| (n = 527).
For classifying anemia, individuals were assigned to non-anemia or mild, moderate, or severe anemia based on hemoglobin levels (g/dL) with respect to age and pregnancy status per the WHO recommendations11,19. Blood pressure measurements were classified into various stages of hypertension based on guidance from the American Heart Association11,37. The thresholds associated with the various measures that comprise metabolic syndrome (glucose, cholesterol, triglycerides, diabetes) also followed from American Heart Association guidance11,38. For the CardioChekPlus, the diagnostic machine cannot read triglyceride values below 50 mg/dL, therefore neither triglyceride nor LDL cholesterol values were recorded for these individuals. LDL cholesterol is not directly measured by this machine but rather estimated as a function of triglyceride, HDL cholesterol, and total cholesterol levels using the Friedewald Equation (LDL cholesterol = total cholesterol—HDL cholesterol—triglycerides/5)39.
Statistical analysis
To characterize spatial variability of nutrient related health issues in Kiribati, while accounting for the nested structure of our data (i.e., individuals within households, households within villages, and villages within islands), we separately modeled each outcome using Bayesian multilevel models. We modeled each status (e.g., anemia status, blood pressure status) using cumulative logistic family distributions, with the exception of glucose and cholesterol status where we used a bernoulli family distribution because we only had samples within two categories (i.e., normal and hyperglycemic; normal and at risk; respectively). Note that sample sizes used in the models varied by biomarker (Table 1), depending on both data availability and biomarker status classifications. For each biomarker we ran two separate models, a null model that included the hierarchical spatial structure of our data, and a full model that also included fixed effects for age, and sex, with age standardized by subtracting the mean and dividing by two times the standard deviation40. The full model for anemia status also included the presence/absence of smoking (Fig. S4)41. All analyses were performed with RStan via the brms package in R42,43using default priors. Model selection through leave-out-one cross validation favored the full model for all biomarkers (Table S4)44. Convergence was assessed by inspecting the potential scale reduction factors for all parameters, and comparing it to the recommended nominal threshold of 1.0545. All models converged and fit the data well (Fig. S5).
Data availability
All anthropometric data from the Household Income and Expenditure Survey are available by request to the Pacific Community. All data relating to point-of-care blood biomarkers are not available to share based on conditions of the Harvard TH Chan School of Public Health’s Office of Human Research Administration’s IRB 18-0967.
References
Bodirsky, B. L. et al. The ongoing nutrition transition thwarts long-term targets for food security, public health and environmental protection. Sci. Rep. 10, 19778 (2020).
Baker, P. et al. Ultra-processed foods and the nutrition transition: Global, regional and National trends, food systems transformations and political economy drivers. Obes. Rev. 21, e13126 (2020).
Popkin, B. M., Adair, L. S. & Ng, S. W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 70, 3–21 (2012).
Popkin, B. M., Corvalan, C. & Grummer-Strawn, L. M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet (British edition) 395, 65–74 (2020).
Willett, W. et al. Food in the anthropocene: The EAT–Lancet commission on healthy diets from sustainable food systems. Lancet (British edition) 393, 447–492 (2019).
Global Targets. https://www.who.int/teams/nutrition-and-food-safety/global-targets-2025 (2025).
Sievert, K., Lawrence, M., Naika, A. & Baker, P. Processed foods and nutrition transition in the pacific: Regional trends, patterns and food system drivers. Nutrients 11, 1328 (2019).
Golden, C. D. et al. Social-ecological traps link food systems to nutritional outcomes. Glob. Food Secur. 30, 100561 (2021).
Thow, A. M. & Snowdon, W. The effect of trade and trade policy on diet and health in the Pacific Islands. in Trade, food, diet, and health: Perspectives and policy options 147–168 (2010).
Phelps, N. H. et al. Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 403, 1027–1050 (2024).
Golden, C. D. et al. Study protocol: Interactive dynamics of coral reef fisheries and the nutrition transition in Kiribati. Front. Public Health 10, 890381–890381 (2022).
World Health Organization. Global Health Observatory, Prevalence of anaemia in women of reproductive age (aged 15–49) (%), by pregnancy status. https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-women-of-reproductive-age-(-) (2025).
Zhou, B. et al. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: A pooled analysis of 1108 population-representative studies with 141 million participants. Lancet 404, 2077–2093 (2024).
Zhou, B. et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 398, 957–980 (2021).
UNICEF. UNICEF Data Warehouse. Kiribati. https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=KIR.NT_ANT_WHZ_NE3+NT_ANT_HAZ_NE2+NT_BW_LBW+NT_ANT_WHZ_NE2._T+M+F.&startPeriod=2016&endPeriod=2023 (2025). .
Zhou, B. et al. Global variation in diabetes diagnosis and prevalence based on fasting glucose and hemoglobin A1c. Nat. Med. 29, 2885–2901 (2023).
De Onis, M. et al. Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutr. 22, 175–179 (2019).
NCD Risk Factor Collaboration (NCD-RisC). NCD Risk Factor Collaboration (NCD-RisC) Methodology. https://www.ncdrisc.org/methods.html (2022).
World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity (World Health Organization, 2011). No. WHO/NMH/NHD/MNM/11.1.
Finucane, M. M., Paciorek, C. J., Stevens, G. A. & Ezzati, M. Semiparametric Bayesian density estimation with disparate data sources: A meta-analysis of global childhood undernutrition. J. Am. Stat. Assoc. 110, 889–901 (2015).
Guell, C. et al. Small Island developing states: Addressing the intersecting challenges of non-communicable diseases, food insecurity, and climate change. Lancet Diabetes Endocrinol. 12, 422–432 (2024).
Eme, P. E. et al. Obesity measures in the Kiribati population: A need to reclassify body mass index cut-points. BMC Public Health 20, 1092 (2020).
Scanlon, K. S., Yip, R., Schieve, L. A. & Cogswell, M. E. High and low hemoglobin levels during pregnancy: Differential risks for preterm birth and small for gestational age. Obstet. Gynecol. 96, 741–748 (2000).
Gosmanova, E. O. et al. Association of systolic blood pressure variability with mortality, coronary heart disease, stroke, and renal disease. J. Am. Coll. Cardiol. 68, 1375–1386 (2016).
Eckel, R. H., Bornfeldt, K. E. & Goldberg, I. J. Cardiovascular disease in diabetes, beyond glucose. Cell Metabol. 33, 1519–1545 (2021).
Dal Canto, E. et al. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur. J. Prev. Cardiol. 26, 25–32 (2019).
Peters, S. A. E., Singhateh, Y., Mackay, D., Huxley, R. R. & Woodward, M. Total cholesterol as a risk factor for coronary heart disease and stroke in women compared with men: A systematic review and meta-analysis. Atherosclerosis 248, 123–131 (2016).
Reiner, Ž. Hypertriglyceridaemia and risk of coronary artery disease. Nat. Rev. Cardiol. 14, 401–411 (2017).
Campbell, B. & Hanich, Q. Fish for the Future: Fisheries Development and Food Security for Kiribati in an Era of Global Climate Change (WorldFish, 2014).
Cauchi, J. P., Correa-Velez, I. & Bambrick, H. Climate change, food security and health in kiribati: A narrative review of the literature. Glob. Health Action 12, 1603683 (2019).
Baena, P. A. et al. In Brief: The White/Wiphala Paper on Indigenous Peoples’ Food Systems. in Science and Innovations for Food Systems Transformation (eds. von Braun, J., Afsana, K., Fresco, L. O. & Hassan, M. H. A.) (Springer, 2023).
Short, R. E. et al. Harnessing the diversity of small-scale actors is key to the future of aquatic food systems. Nat. Food 2, 733–741 (2021).
Marrero, A. et al. Equity as a priority in EAT–Lancet-aligned food system transformations. Nat. Food 5, 811–817 (2024).
Seto, K. L. et al. Characterizing pathways of seafood access in small island developing states. Proceedings of the National Academy of Sciences 121, e2305424121 (2024).
World Health Organization. WHO child growth standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. https://www.who.int/publications/i/item/924154693X (2006).
de Onis, M. The WHO child growth standards. Pediatric nutrition in practice 254–269 (2008).
Carey, R. M. & Whelton, P. K. Prevention, detection, evaluation, and management of high blood pressure in adults: Synopsis of the 2017 American college of cardiology/american heart association hypertension guideline. Ann. Intern. Med. 168, 351–358 (2018).
Grundy, S. M. et al. Diagnosis and management of the metabolic syndrome - An American heart association/national heart, lung, and blood Institute scientific statement - Executive summary. Circulation (New York N Y) 112, E285–E290 (2005).
Warnick, G. R., Knopp, R. H., Fitzpatrick, V. & Branson, L. Estimating low-density lipoprotein cholesterol by the Friedewald equation is adequate for classifying patients on the basis of nationally recommended cutpoints. Clin. Chem. 36, 15–19 (1990).
Gelman, A. Data Analysis Using Regression and Multilevel/Hierarchical Models (Cambridge University Press, 2007).
Sharma, A. J., Addo, O. Y., Mei, Z. & Suchdev, P. S. Reexamination of hemoglobin adjustments to define anemia: Altitude and smoking. Ann. N. Y. Acad. Sci. 1450, 190–203 (2019).
Bürkner, P. Brms: An R package for bayesian multilevel models using Stan. J. Stat. Softw. 80, 1–28 (2017).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.URL (2021). https://www.R-project.org/
Vehtari, A., Gelman, A. & Gabry, J. Practical bayesian model evaluation using leave-one-out cross-validation and WAIC. Stat. Comput. 27, 1413–1432 (2017).
Gelman, A. & Rubin, D. B. Inference from iterative simulation using multiple sequences. Stat. Sci. 7, 457–472 (1992).
Acknowledgements
We are grateful for the financial support of the National Science Foundation (CNH 1826668) and the leveraged funding from the Pacific Community (SPC) to collaborate with the Government of Kiribati on their Household Income and Expenditure Survey (HIES). We would like to thank the following people: Tebwebweiti Tikanibwebwe (MHMS), Tebano Bwabwa (MHMS), Nantebwebwe Toabo (MHMS), Bwaturia Temaua (MHMS), Baurina Kaburoro (MHMS), Tirite Irooti (MHMS) for collecting data in the field.
Author information
Authors and Affiliations
Contributions
CDG, KLS, JAG, JGE and JA designed the biomarker study with support from KN, ET, MKS, and AT. CDG, JZM, and JA designed the analysis. JZM led the data analysis with support from HMK. JAG, WF, MKS, and AT supported the overall data infrastructure for the project and linking with national data and statistics for the country of Kiribati. HM, KN, ET, RT, and AT supported the design of field data collection protocols with CDG and JA and locally oversaw the project. CDG wrote the manuscript and all authors edited the manuscript and approved the final version.
Corresponding author
Ethics declarations
Competing interests
I declare that the authors have no competing interests as defined by Nature Research, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Golden, C.D., Zamborain-Mason, J., Seto, K.L. et al. Prevalence and spatio-demographic variability of nutrition-related health issues in Kiribati. Sci Rep 15, 23390 (2025). https://doi.org/10.1038/s41598-025-07152-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07152-w
