
Abstract
The relationship between body composition and fracture sites is complex. Previous studies have reported that a site-dependent relationship between body mass index (BMI) and fractures in postmenopausal women and older men. This study aimed to investigate sex-specific associations of fat and lean indices with vertebral fractures. This cross-sectional study included 1,479 participants, with body composition assessed using dual-energy X-ray absorptiometry. Fat indices included BMI, body fat percentage, and waist circumference, whereas the lean index was represented by appendicular lean mass (ALM)/height². Prevalent vertebral fractures were identified through radiographic confirmation. When both fat and lean indices simultaneously were considered, BMI (odds ratio [OR], 1.15; 95% confidence interval [CI] 1.08–1.22), body fat percentage (OR, 1.06; 95% CI 1.02–1.10), and waist circumference (OR, 1.06; 95% CI, 1.03–1.08) were significantly associated with vertebral fractures in postmenopausal women, whereas ALM/height² did not show such an association. In contrast, for men aged ≥ 50 years, ALM/height² was significantly associated with vertebral fractures, whereas fat indices showed no such an association. Furthermore, a significant interaction between ALM/height² and sex was observed. Fat indices were predominantly associated with vertebral fractures in women, whereas the lean index was more strongly associated with vertebral fractures in men. These findings highlight a sex-specific association between body composition and vertebral fractures.
Similar content being viewed by others

Introduction
Obesity is considered a protective factor against fractures; however, this relationship has been challenged. The association between body mass index (BMI) and fractures appears to be site-dependent. In postmenopausal women, obesity is associated with proximal humerus1,2,3, upper leg4, ankle4, and vertebral fractures5, while it may protect against hip2,3, and distal forearm fractures2. In men aged ≥ 65 years, Nielson et al. reported that obesity was associated with an increased risk of hip fractures6, whereas Premaor et al. showed that obesity was associated with a reduced risk of clinical spine, hip, and distal forearm fractures7. Furthermore, the association between obesity and fractures differed according to the definition. Gandham et al. showed that obesity, defined by body fat percentage, was associated with an increased risk of incident fractures, whereas obesity defined by BMI was not8. This highlights the need for further investigation into the association of fat indices, such as BMI, body fat percentage, and waist circumference, with fractures.
Beyond fat mass, the association between appendicular lean mass (ALM) and fractures varied by sex. In postmenopausal women, greater ALM/height² was protective against hip fractures, although this association was not statistically significant after adjusting for total hip bone mineral density (BMD) in the Women’s Health Initiative and Health ABC studies9,10. In older men, greater ALM/height² value was a risk factor for incident hip fracture after adjusting for BMD in the Health ABC and Men studies10,11. However, the association between ALM/height² and fractures at other sites, such as vertebral fractures, remains unclear.
Both fat and lean indices are linked to fractures, with associations varying by fracture sites and sex. Higher fat or lean mass has been thought to indicate stronger bones due to greater skeletal load12,13. Additionally, fat indices contributed more to BMD in women, while lean indices were more strongly associated with BMD in men13. This study aimed to explore the associations between fat and lean indices and vertebral fractures in both women and men. We hypothesize that fat indices will be more strongly associated with vertebral fractures in women, whereas the lean index will show a stronger association in men.
Methods
Participants
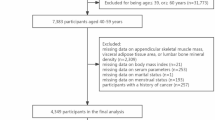
This cross-sectional study was conducted between 2019 and 2024. Participants were randomly recruited from individuals who underwent dual-energy X-ray absorptiometry (DXA) at our hospital. The inclusion criteria were men aged 50 years or older and postmenopausal women. The exclusion criteria were those who were unable to undergo anthropometric measurements or body composition analysis due to physical or cognitive impairments. A total of 1479 participants were included, and all of them provided written informed consent. The study was approved by the institutional review board.
Anthropometric measurements
The participants were instructed to wear light clothing, and their weight and height were measured. Waist circumference was measured at the approximate midpoint between the lower margin of the last palpable rib and the top of the iliac crest.
Measurements of muscle strength
Hand grip strength was used to estimate the muscle strength. A digital hand dynamometer (EH101; Camry, Guangdong Province, China) was used to assess the hand grip strength. Participants completed three trials per hand, with the best performance of each hand considered for the analysis. Hand grip strength is a key measure for diagnosing sarcopenia, as recommended by both the Asian Working Group for Sarcopenia and the European Working Group on Sarcopenia in Older People14,15. Additionally, sarcopenia is a well-established risk factor for fractures16.
Bone mineral density
Lumbar spine BMD was evaluated using a DXA scanner (Horizon W; Hologic Inc., Bedford, MA, USA). The coefficient of variation of the lumbar spine BMD was 1.28%.
Measurements of body fat percentage and appendicular lean mass
Body fat percentage and ALM were evaluated using a DXA scanner (Horizon W; Hologic Inc., Bedford, MA, USA). The ALM was normalized for height squared to account for body size, representing the lean index. Normalizing ALM by height squared is a standard method to account for variations in body size, providing a more accurate assessment of lean mass relative to height14,15. Coefficients of variation for body fat percentage and ALM were 1.20% and 0.96%, respectively.
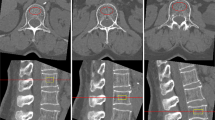
Assessment of vertebral fractures
Vertebral fractures were retrospectively reviewed from the hospital medical records, and only radiographically confirmed fractures were included in this study. Because our hospital is a regional hospital, distal extremity fractures are often treated in local medical facilities. Thus, distal extremity fractures were not included in this study.
Additional covariates
The independent variables included age, physical activity for at least 30 min per day on more than three days per week (yes/no), dairy product intake (yes/no), and medications affecting bone density (yes/no). Medications affecting bone density included bisphosphonates, parathyroid hormones, and estrogens.
Statistical analysis
Independent t test and chi-squared test were used to compare demographic characteristics between women and men. Multivariate logistic regression analysis was used to evaluate the association between fat and lean indices and vertebral fractures in both sexes. An interaction model was built to investigate the statistical interaction between body composition indices and sex. Due to the low statistical power associated with tests for interaction, a p-value < 0.10 was used to assess the statistical significance of interaction terms. All other statistical significance was set at p < 0.05. All analyses were performed using IBM SPSS Statistics for Windows, version 19.0 (IBM Corp., Armonk, NY, USA).
Results
Table 1 showed the characteristics of participants stratified by sex. The prevalence of osteoporosis in this study was 49.4%, while that of sarcopenia was 18.1%. These relatively high rates were likely attributable to the hospital-based nature of the study population. Of 1,479 participants included in this study, 77.3% were women. Age, weight, height, BMI, waist circumference, body fat percentage, ALM/height², hand grip strength, medications, and spinal BMD differed between women and men. Considering these differences, separate analyses were performed by sex.
The associations between fat or lean indices and vertebral fractures stratified by sex were shown in Table 2. In postmenopausal women, BMI, body fat percentage, and waist circumference were positively associated with vertebral fractures, whereas ALM/height² was not. In contrast, in men aged ≥ 50 years, both BMI and ALM/height² were positively associated with vertebral fractures.
To consider fat and lean indices together, various fat indices, including BMI, body fat percentage, and waist circumference, were analyzed alongside with the lean index of ALM/height². In women, BMI, body fat percentage, and waist circumference remained positively associated with vertebral fractures (Table 3), whereas ALM/height² was not. Therefore, fat indices were predominantly linked to vertebral fractures in women. In contrast, in men, analyses revealed that ALM/height², rather than BMI, body fat percentage, or waist circumference was associated with vertebral fractures (Table 3), although BMI was significant in the absence of the lean index (Table 2). Thus, the lean index was predominantly associated with vertebral fractures in men. Additionally, a significant interaction between ALM/height² and sex was observed. The effect remained similar when the models were adjusted for medications use only, excluding other lifestyle factors, as part of a sensitivity analysis.
Discussion
This study found an association of fat and lean indices with vertebral fractures in women and men. This largely support our hypothesis that fat indices were associated with vertebral fractures in women, while the lean index was more strongly associated with fractures in men. Furthermore, a sex-specific association of the lean index with vertebral fractures was observed.
With no adjustment for BMD, Prieto-Alhambra et al. showed that obesity based on BMI was not associated with an increased risk of vertebral fractures in postmenopausal women3. In contrast, Compston et al. reported that linear BMI showed a significant negative association with clinical spine fracture in postmenopausal women17. Nevertheless, the association between BMI and fractures can be attenuated by adjusting for BMD2. In the present study, fat indices, including BMI, body fat percentage, and waist circumference, were associated with vertebral fractures after adjusting for BMD in women. This finding is consistent with previous findings reported by Laslett et al. and Pirro et al., where BMI was associated with spinal deformity or vertebral fracture after adjusting for BMD in women5,18.
However, there is limited understanding regarding the relationship between obesity and fracture sites in men. Premaor et al. found that obesity, as determined by BMI, was associated with a decreased risk of hip, spine, and distal forearm fractures, without adjusting for BMD7. However, after adjusting for BMD, Nielson et al. showed that obesity was associated with an increased risk of hip fractures6. In this study, BMI was associated with vertebral fractures in men after adjusting for BMD, whereas body fat percentage and waist circumference were not. In contrast to women, the association between fat indices and vertebral fractures varied by sex.
ALM/height², as determined by DXA, has become a key measure of sarcopenia14,15 and has been shown to be associated with BMD13. Without adjusting for BMD, a greater ALM/height² was protective against hip fracture in women but not in men; after adjusting for BMD, a greater ALM/height2 showed no significant association with hip fractures in women but became a risk factor for hip fracture in men9,10,11. In the present study, after adjusting for BMD, a greater ALM/height² was not associated with vertebral fractures in women, even when fat indices were included in the models. However, fat indices were still associated with vertebral fractures. In contrast, a greater ALM/height² was consistently associated with vertebral fractures in men, with and without adjusting for fat indices. Laslett et al. also reported that after adjusting for fat mass and lean mass, men with higher lean mass had a higher likelihood of vertebral deformities18. Therefore, the association of the lean index with vertebral fractures differed according to sex.
The association of high ALM with fractures may be linked to both physical activity and fall risk18 or a pro-fracture state due to the larger loads from greater ALM10, which remains controversial11. The biological connections among fat, muscle, and bone, including both endocrine and mechanical interactions, are not yet fully established19. The complex interaction between altered body composition and hormonal changes may involve multifactorial pathogenesis. Given the distinct associations between fat and lean indices and vertebral fractures in women and men, clinicians should consider both fat and lean mass measurements as part of a comprehensive assessment of fracture risk, particularly in postmenopausal women and older men.
Analyzing data separately by sex is a common and expected practice in health research, especially when biological differences between men and women—such as body composition, hormone levels, and patterns of bone loss—are well established. While this approach is not novel, the clinical significance often lies in what these stratified analyses reveal. In this case, the study found that different components of body composition are linked to vertebral fractures in men and women in distinct ways. Specifically, fat indices were more strongly associated with fractures in women, while lean mass was more closely linked to fractures in men in this study. These findings challenge common assumptions, such as the belief that higher BMI protects against fractures due to increased mechanical loading on bones—a notion particularly questioned in women. Moreover, the association between lean mass and fractures in men remains unclear and warrants further research. The key insight is not simply that men and women were analyzed separately, but that the risk factors for fractures differ qualitatively between sexes. Therefore, the novelty of this study lies not in its methodology, but in the implications of the findings and their contribution to a deeper understanding of how body composition affects bone health differently in men and women.
Our study had several strengths. First, we investigated the association of lean and fat indices simultaneously with vertebral fractures. Second, we explored the sex differences, a topic not adequately investigated in the existing literature. Third, the fat and lean indices used in our study are commonly employed worldwide and are easily measured, which enhances their practical clinical applications. However, there are some limitations. First, as this was a cross-sectional study, we could not draw causal inferences. Longitudinal studies are needed to confirm this causal relationship. Second, the participants were exclusively Asian, which may limit the generalizability of our findings. Third, although DXA is widely used for estimating muscle mass14,15, alternative imaging modalities such as magnetic resonance imaging or computed tomography may offer more precise measurements, though they are less accessible due to higher costs and limited availability. Fourth, the number of men in the study was relatively small, and a smaller sample size can result in less precise estimates and greater variability. However, ALM has been identified as a risk factor for incident hip fractures in men in previous studies with larger sample sizes, supporting the relevance of this finding10,11.
In conclusion, the association of fat and lean indices with vertebral fractures differed by sex. Fat indices were predominantly associated with vertebral fractures in women, whereas the lean index was predominantly associated with vertebral fractures in men. A sex-specific association between the lean index and vertebral fractures was identified. Future research should aim to investigate the longitudinal relationship between changes in body composition and fracture risk, particularly at different anatomical sites.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at the IRB of Cheng Hsin General Hospital.
References
Gnudi, S., Sitta, E. & Lisi, L. Relationship of body mass index with main limb fragility fractures in postmenopausal women. J. Bone Min. Metab. 27 (4), 479–484 (2009).
Johansson, H. et al. A meta-analysis of the association of fracture risk and body mass index in women. J. Bone Min. Res. 29 (1), 223–233 (2014).
Prieto-Alhambra, D. et al. The association between fracture and obesity is site-dependent: a population-based study in postmenopausal women. J. Bone Min. Res. 27 (2), 294–300 (2012).
Compston, J. E. et al. Obesity is not protective against fracture in postmenopausal women: GLOW. Am. J. Med. 124 (11), 1043–1050 (2011).
Pirro, M. et al. High weight or body mass index increase the risk of vertebral fractures in postmenopausal osteoporotic women. J. Bone Min. Metab. 28 (1), 88–93 (2010).
Nielson, C. M. et al. BMI and fracture risk in older men: the osteoporotic fractures in men study (MrOS). J. Bone Min. Res. 26 (3), 496–502 (2011).
Premaor, M. O. et al. The association between fracture site and obesity in men: a population-based cohort study. J. Bone Min. Res. 28 (8), 1771–1777 (2013).
Gandham, A. et al. Incidence and predictors of fractures in older adults with and without obesity defined by body mass index versus body fat percentage. Bone 140, 115546 (2020).
Zaslavsky, O. et al. Association between body composition and hip fractures in older women with physical frailty. Geriatr. Gerontol. Int. 17 (6), 898–904 (2017).
Malkov, S. et al. Hip fractures risk in older men and women associated with DXA-derived measures of thigh subcutaneous fat thickness, cross-sectional muscle area, and muscle density. J. Bone Min. Res. 30 (8), 1414–1421 (2015).
Harvey, N. C. et al. Measures of physical performance and muscle strength as predictors of fracture risk independent of FRAX, falls, and aBMD: a meta-analysis of the osteoporotic fractures in men (MrOS) study. J. Bone Min. Res. 33 (12), 2150–2157 (2018).
Kim, Y. M. et al. Variations in fat mass contribution to bone mineral density by gender, age, and body mass index: the Korea National health and nutrition examination survey (KNHANES) 2008–2011. Osteoporos. Int. 27 (8), 2543–2554 (2016).
Lin, Y. H. & Teng, M. M. H. Different contributions of fat and lean indices to bone strength by sex. PLoS One. 19 (11), e0313740 (2024).
Chen, L. K. et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 21 (3), 300–307e302 (2020).
Cruz-Jentoft, A. J. et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 48 (1), 16–31 (2019).
Yeung, S. S. Y. et al. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. cachexia Sarcopenia Muscle. 10 (3), 485–500 (2019).
Compston, J. E. et al. Relationship of weight, height, and body mass index with fracture risk at different sites in postmenopausal women: the global longitudinal study of osteoporosis in women (GLOW). J. Bone Min. Res. 29 (2), 487–493 (2014).
Laslett, L. L., Just Nee Foley, S. J., Quinn, S. J., Winzenberg, T. M. & Jones, G. Excess body fat is associated with higher risk of vertebral deformities in older women but not in men: a cross-sectional study. Osteoporos. Int. 23 (1), 67–74 (2012).
Bauer, J. M. et al. Is there enough evidence for osteosarcopenic obesity as a distinct entity? A critical literature review. Calcif Tissue Int. 105 (2), 109–124 (2019).
Acknowledgements
Not applicable.
Funding
This work was supported by grants (CHGH114-14) and (CHGH114-113-N23) from the Cheng Hsin General Hospital, Taipei, Taiwan.
Author information
Authors and Affiliations
Contributions
Yen-Huai Lin and Michael Mu Huo Teng initiated the study, and all authors contributed to its design. Yen-Huai Lin and Michael Mu Huo Teng managed the data collection, performed the data analysis, and wrote the first draft of the manuscript. Yen-Huai Lin and Michael Mu Huo Teng are collectively responsible for interpreting the results and critically reviewed subsequent drafts of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the institutional review board of Cheng Hsin General Hospital (IRB no. (660)107 A-32).
Consent to participate
Informed consent was obtained from all the participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lin, YH., Teng, M. Sex-specific associations of fat and lean indices with vertebral fractures. Sci Rep 15, 23479 (2025). https://doi.org/10.1038/s41598-025-07552-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07552-y
Keywords
This article is cited by
-
Muscle mass, not fat mass, predicts vertebral fracture risk: Vietnam osteoporosis study
Osteoporosis International (2026)
