
Abstract
This study focuses on the structural brain changes, alterations in Apparent Diffusion Coefficient (ADC) values, and the morphological characteristics of distal intracranial arteries in chronic alcohol consumption. A total of 50 chronic alcoholics and 43 non-alcoholics were recruited from neurology inpatient and outpatient services. Using the Brainnetome Atlas to segment the brain into 246 regions, ADC values were observed to be consistently higher in alcoholics, with statistically significant differences in 134 of these regions. This number is far greater than the number of brain regions where changes in gray matter volume were observed. The alcohol group exhibited lower mean arterial density, mean arterial radius, and mean arterial tortuosity, along with higher mean arterial flexibility, though mean arterial length did not differ significantly between groups. But correlation analysis revealed a negative relationship between alcohol consumption and mean arterial density and mean arterial length. Gray matter volume was positively correlated with mean arterial length, density, and radius. White matter volume also showed a positive correlation with mean arterial length and density. Conversely, cerebrospinal fluid volume was negatively correlated with mean arterial length and density. These results suggest that the diffusion of water molecules in the brains of alcoholics is altered before observable changes in gray matter structure occur. Changes in cerebrovascular morphology are a contributing factor to the structural brain changes observed in chronic alcoholics.
Similar content being viewed by others

Introduction
Extensive brain atrophy in alcohol-dependent individuals (ALC) has been consistently documented in both pathological and magnetic resonance imaging (MRI) studies1. MRI research provides compelling evidence that chronic alcohol consumption results in significant alterations in gray and white matter2. Chronic heavy drinking predominantly impacts the frontal lobe, mesencephalon, hippocampus, and cerebellar structures. A negative correlation has been observed between alcohol intake and overall brain volume, regional gray matter volume, and white matter microstructure3. Recently, Zhou et al. (2024) conducted a meta-analysis of structural MRI studies and further confirmed the relationship between long-term alcohol consumption and brain atrophy, providing more comprehensive evidence for this well-established finding4. In studies examining alcohol use and brain development in adolescents, findings revealed that alcohol consumption is associated with thinner total, frontal, temporal, and cingulate cortices compared to non-drinkers5. Higher levels of alcohol consumption correlate with multiple markers of white matter microstructure, including reduced fractional anisotropy and increased mean and radial diffusivity, with a widespread distribution across the brain6.
Voxel-based morphometry (VBM) is an automated, comprehensive, and objective technique for voxel-based analysis of brain structures via magnetic resonance imaging (MRI), allowing for the quantitative calculation and analysis of gray and white matter density or volume changes in each voxel, thereby highlighting differences in corresponding anatomical structures7. Surface-based morphology (SBM) offers a computational approach to MR imaging data, quantifying the brain’s gray matter morphological structure through parameters such as thickness, surface area, volume, and curvature8.
In this study, VBM analysis was employed to obtain measurements of gray matter volume, white matter volume, cerebrospinal fluid volume, cerebral white matter high signal volume, and regional gray and cerebrospinal fluid volumes. SBM was used to derive morphological indicators such as cortical thickness, curvature, and sulcal depth. Quantitative calculations of DWI images were performed using FMRIB’s Software Library9 to generate ADC images for each participant. Based on the Brainnetome Atlas10, mean values of all quantitative metrics were extracted for each brain region. By comparing these indicators between the alcohol group and the non-alcohol group, the study assessed the correlation between these metrics and the degree of alcohol consumption and the morphological characteristics of distal intracranial arteries.
Research has established that alcohol abuse heightens the risk of cerebrovascular events by altering cerebral blood flow, increasing blood pressure, and compromising the blood–brain barrier. Short-term alcohol consumption significantly enlarges the perivascular space surrounding small vessels in brain tissue, whereas long-term consumption induces pathological changes in the basilar arteries (BAs), such as endothelial detachment, fragmentation of the internal elastic lamina (IEL), and thickening of the peritubular middle and outer layers11. Significant correlations have been identified between cerebral blood flow and structural parameters across various brain regions, including the temporal, frontal, parietal, and occipital lobes, precentral gyrus, periaqueductal cortex, internal olfactory cortex, supramarginal gyrus, fusiform gyrus, precuneus, and pallidum in patients with cognitive dysfunction12. Additionally, a marked correlation exists between reduced cerebral blood flow and gray matter atrophy, affecting cortical volume, surface area, and thickness across numerous regions12. Gould et al. demonstrated that vascular characteristics of distal arteries on 3D-TOF MRA, such as vessel length and branching patterns, can serve as surrogate markers of cerebral blood flow. Morphological features of distal intracranial arteries—including arterial length, density, and mean tortuosity—measured by 3D-TOF MRA, were found to correlate with systemic or focal atrophy in cerebral small vessel disease13. 3D-TOF MRA remains the most commonly employed angiographic technique in clinical practice, particularly for evaluating the head and carotid arteries14. Advances in image processing techniques have facilitated the extraction of cerebrovascular features using 3D-TOF MRA15,16,17,18.
The primary subjects of this study are individuals characterized by a long-standing pattern of alcohol consumption behavior, as opposed to those who have already manifested alcohol use disorders. This study quantified the morphological characteristics of distal intracranial arteries, including mean arterial density, radius, length, curvature, flexibility, and tortuosity, by processing MRA images with MIMICS and 3D Slicer19,20. Differences in these metrics between the alcohol group and the non-alcohol group were analyzed, alongside their relationships with various brain structures, such as gray matter volume (GMV), white matter volume (WMV), cerebrospinal fluid volume (CSFV), cerebral white matter high signal volume (WMH). Previous studies mainly focused on either brain structural changes or vascular alterations in chronic alcoholics separately.
Our study innovatively combines vascular morphological data, such as mean arterial density, radius and length, with standard neuroimaging metrics like GMV, WMV, CSFV and WMH. This integrated approach allows for a more comprehensive understanding of the complex relationship between chronic alcohol consumption, cerebrovascular changes, and brain structural remodeling, filling a gap in the existing literature.
The primary research question of this study is: By quantitatively assessing the morphological characteristics of distal intracranial arteries, including parameters such as density, radius, and length, to investigate how these characteristics of distal intracranial vessels change in long-term alcoholics and study the relationship between them and structural brain alterations. We hypothesize that there is a significant association between cerebrovascular morphological changes and structural brain modifications in long-term alcoholics. In particular, changes in arterial density, radius, and length are expected to be related to changes in gray matter volume (GMV), white matter volume (WMV), and cerebrospinal fluid volume (CSFV). It is anticipated that these vascular changes will contribute to the overall structural brain changes resulting from long-term alcohol consumption.
Materials and methods
Participants
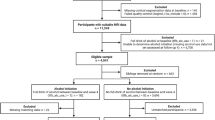
From December 2022 to December 2023, a total of 71 participants with chronic alcohol consumption and 82 participants in the control group with no history of alcohol consumption were consecutively recruited from neurology inpatients and outpatient services.
In the chronic alcohol consumption group, Twenty-one cases were excluded. Nineteen cases did not complete the nuclear magnetic examination as required. Two cases had MRI scans with significant motion artifacts.
In the control group without alcohol consumption history, Thirty-nine cases were excluded. Fourteen cases did not complete the required nuclear magnetic examination. Twelve cases had acute cerebral infarction after examination. Six cases had intracranial aortic stenosis after examination. Seven cases had a clear white matter lesion.
Eventually, a total of 50 chronic alcoholics and 43 non-alcoholics were recruited.
Long-term Alcohol Consumption Group.
Inclusion criteria: (1) Complete medical records; (2) Age 22 to 65 years; (3) Right-handed; (4) Males with an alcohol intake exceeding 40 g (degree × mL) per day or more than 280 g per week, and females with an alcohol intake exceeding 20 g (degree × mL) per day or more than 140 g per week, with a history of alcohol consumption spanning more than 5 years21,22; (5) Informed about the study and provided voluntary participation.
Exclusion criteria: (1) Neurological damage due to other diseases; (2) History of traumatic brain injury or other brain tissue damage; (3) Use of psychotropic drugs in the last 3 months; (4) Drug dependence or other substance abuse; (5) Cognitive dysfunction; (6) Epilepsy; (7) Contraindications to MRI examination.
The participants of our study are from Jincheng City, Shanxi Province, where females basically do not consume alcohol. All the enrolled participants were male, with ages ranging from 22 to 65 years.
Classification of alcohol consumption groups (based on weekly alcohol intake × years of consumption): Light drinking group: 4000–10000 g; Moderate drinking group: 10001–20000 g; Heavy drinking group: More than 20000 g23.
Inclusion criteria for the no alcohol consumption group: (1) Age and gender matched, no history of continuous alcohol consumption; (2) Complete medical history with no serious neurological or psychiatric diseases; (3) Right-handed; (4) No history of traumatic brain injury or other brain tissue damage; (5) No recent use of psychotropic medications; (6) Informed about the study content and provided voluntary participation.
This study was approved by the Ethics Committee of Jincheng City People’s Hospital (JCPH.NO20230710004). All participants, or their guardians, provided written informed consent.
Data collection
Demographic data
Information was recorded on participants’ age, gender, body mass index (BMI), hypertension, diabetes mellitus, coronary atherosclerotic heart disease, smoking history, and previous incidents of cerebral infarction or cerebral hemorrhage.
Collection of general metabolic markers
The general metabolic indices were derived from the laboratory of Jincheng People’s Hospital. The subjects provided fresh blood samples through venous blood collection, which were then collected into inert separator gel procoagulant tubes. The collected venous blood was centrifuged at 2000 rpm for 20 min at 4 °C as rapidly as possible. Subsequently, the supernatant was aspirated using a pipette gun to obtain serum.
Leukocytes, erythrocytes, hemoglobin, hematocrit, MCV, MCH, MCHC, platelets, plateletcrit, absolute lymphocyte count, lymphocyte percentage, absolute monocyte count, monocyte percentage, absolute neutrophil count, neutrophil percentage, absolute eosinophil count, eosinophil percentage, absolute basophil count, basophil percentage, nucleated red blood cell count, nucleated red blood cell percentage and large platelet percentage were measured using an automated hematology analyzer. Biochemical markers such as calcium, carbon dioxide, phosphorus, magnesium, ALT, AST, total bilirubin, urea, creatinine, cholinesterase, alkaline phosphatase, gamma-glutamyl transferase, lactate dehydrogenase, adenosine deaminase and uric acid were determined by enzymatic methods on a biochemical analyzer. For lipid markers such as total cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-C), enzymatic colorimetric assays were employed. Glycated Hemoglobin was measured using the high-performance liquid chromatography (HPLC) method. Homocysteine levels were determined using the enzymatic cycling method. Prothrombin time (PT), fibrinogen (FIB), thrombin time (TT), and activated partial thromboplastin time (APTT) were measured using the coagulation method. D-dimer levels were measured via the immunoturbidimetric method. Serum myoglobin, CK–MB mass, FT3, FT4, TSH, folate, vitamin B12, and ferritin levels were measured using the electrochemiluminescence immunoassay method.
Cognitive and psychometric assessments
Participants were evaluated using the AUDIT scale24, Alcohol Dependence Self-Rating Scale, PSQI Sleep Scale, MMSE, MoCA, and Symptom Checklist 90 (SCL-90).
Blood sample collection and processing
Fresh blood samples were obtained via venipuncture and collected into inert separator gel procoagulant tubes. The samples were centrifuged at 4 °C for 20 min at 2000 rpm, and the supernatant was carefully extracted using a pipette, then stored in 1.5 ml polypropylene tubes at − 80 °C until analysis. The following markers were measured: IL-1b, complement C1q, IL-2, IL-4, IL-6, IL-10, TNF-α, INF-γ, GFAP, and sTREM2.
MRI imaging and image processing
All participants underwent MRI using a standard protocol. Scanning was performed with a 3.0 T Philips Intera scanner (Ingenia 3.0 T, Philips Medical Systems, The Netherlands) in the imaging department of Jincheng People’s Hospital. The imaging consists of the following sequences: DWI (repetition time (TR) = 3240 ms, echo time (TE) = 113 ms, flip angle (FA) = 90°, slice = 20, field of view (FOV) = 230 × 230mm2, acquisition matrix = 164 × 134, thickness = 5.5 mm, voxel size = 1.4 × 1.7 × 5.5 mm3), T1-weighted (repetition time (TR) = 1800 ms, echo time (TE) = 20 ms, flip angle (FA) = 90°, slice = 20, field of view (FOV) = 230 × 185 mm2, acquisition matrix = 322 × 134, thickness = 5.5 mm, voxel size = 1.4 × 1.7 × 5.5 mm3), T2-weighted (TR = 4,000 ms, TE = 107 ms, FA = 90°, slice = 20, FOV = 230 × 230 mm2, acquisition matrix = 384 × 384, thickness = 5.5 mm, voxel size = 0.6 × 0.7 × 5.5 mm3), FLAIR (TR = 11,000 ms, TE = 120 ms, FA = 90°, slices = 20, FOV = 230 × 187mm2, acquisition matrix = 356 × 115, thickness = 5.5 mm, voxel size = 0.65 × 1 × 5.5mm3), TOF-MRA (TR = 23 ms, TE = 3.5 ms, FA = 18°, slice = 160, FOV = 200 × 200 mm2, acquisition matrix = 444 × 294, thickness = 1.2 mm, voxel size = 0.45 × 0.68 × 1.2 mm3), 3D-T1 (TR = 7.9 ms, TE = 3.5 ms, FA = 8°, slice = 360, FOV = 256 × 256 mm2, acquisition matrix = 256 × 256, thickness = 1 mm, voxel size = 1 × 1 × 1 mm3).
Based on Matlab 2020, data preprocessing and statistical analysis of brain structure images were carried out using the CAT12 software package. The specific procedures are as follows:
① Data Conversion: Convert the DICOM data collected by the device into the analyzable NIFTI format. ② Data Inspection: Check the imaging quality of the data one by one, mainly focusing on the integrity of data collection and whether there are serious artifacts. ③ Brain Structure Image Segmentation: Utilize CAT12 to segment the images into gray matter, white matter, and cerebrospinal fluid, and perform modulation to enable volume analysis. ④ Cortical Segmentation: Employ CAT12 for cortical segmentation, and estimate the thickness, curvature, and sulcal depth of the cortical regions. ⑤ Quantitative Calculation: Extract the total intracranial volume (TIV), as well as the volumes of gray matter and white matter in each brain region, and store them in a table. ⑥ Region-of-Interest Extraction: Use the HCP-MMP125atlas to extract the average thickness, curvature, and sulcal depth of each cortical region. Use the Neuromorphometrics atlas to extract the average volume information of gray matter and white matter in each region. ⑦ Gaussian Smoothing of Brain Structure Images: Apply Gaussian smoothing to the segmented images with a Gaussian kernel having a full-width at half-maximum of 12 mm3. ⑧ Voxel-Based Morphometry (VBM) Pixel-by-Pixel Statistical Analysis: Based on the general linear model, establish a statistical analysis model for the smoothed brain structure data and conduct pixel-by-pixel statistical analysis. ⑨ Surface-Based Morphometry (SBM) Statistical Analysis: Based on the general linear model, establish a statistical analysis model for the smoothed cortical quantitative information and carry out pixel-by-pixel statistical analysis.
Preprocessing and quantitative calculations of DWI images were conducted using FMRIB’s Software Library (FSL). ① Data Conversion: Convert the DICOM data collected by the device into the analyzable NIFTI format. ② Data Inspection: Check the imaging quality of the data one by one, mainly focusing on the integrity of data collection and whether there are serious artifacts. ③ Quantitative Calculation: Use FSL to perform quantitative calculations on DWI images to obtain the ADC image for each patient. ④ Spatial Alignment: Taking each subject’s T1 image as a reference, perform a 6-parameter rigid body transformation to spatially align the ADC image with the T1 image. ⑤ Spatial Normalization: Since the shape and size of each subject’s brain differ, in order to conduct voxel-by-voxel statistical analysis on one or more groups of data, all subjects need to be aligned voxel by voxel first. Using the T1-weighted brain template in MNI space as the reference standard, estimate the registration parameters with the T1 image as the source image. Then, perform a 12-parameter affine transformation and non-linear deformation on the ADC index image for spatial transformation, normalizing the quantitative index brain images of all subjects to the template space to eliminate inter-subject differences. ⑥ Gaussian Smoothing: Apply Gaussian smoothing to the spatially normalized data with a Gaussian kernel having a full-width at half-maximum of 8 mm3 to further remove noise and make the data for statistical analysis conform to a normal distribution. ⑦ Quantitative Index Extraction: Based on the BrainnetomeAtlas atlas, extract the average value of all quantitative indices in each brain region and store it in an Excel spreadsheet. ⑧ Pixel-by-Pixel Statistical Analysis: Based on the general linear model, establish a statistical analysis model for the smoothed ADC data and conduct pixel-by-pixel statistical analysis.
All MRA images were processed using MIMICS and 3D Slicer. Initially, the medical images were meticulously examined one by one to ensure their completeness and quality. Subsequently, the 3D VR function of RadiAnt DICOM Viewer 2023.1 (Medixant, Poznan, Poland) was utilized to segment the DICOM images into blood vessels, bones, and other tissues. Through this process, patient-specific cerebral artery models were reconstructed. By carefully adjusting the display threshold, the visibility of non-cerebral artery parts was significantly reduced. In the next step, the adjusted models were imported into Mimics Research 19.0 (Materialise, Leuven, Belgium), and the Edit Mask function was employed to further refine the models, precisely retaining only the regions of interest. Finally, in 3D Slicer (Harvard Medical School, Boston, MA, USA), the centerlines of the cropped models were computed. This enabled the extraction of average morphological parameters, such as radius, curvature, and tortuosity, for various regions in each case. Additionally, the 3D models were converted into volumes for volumetric analysis. The vascular centerlines were obtained using 3D Slicer software. Subsequently, the perpendicular distances from each point on the centerline to the straight line connecting the starting and ending points were calculated. The sum of the squares of these distances was normalized to obtain the arterial tortuosity index. Regarding arterial flexibility, we employed a method based on the centerline deviation method. The flexibility was evaluated according to the curvature changes of the vascular centerlines. Moreover, to minimize the impact of head movement and vascular pulsation on the measurement results, during the scanning process, we requested patients to remain stationary. Additionally, electrocardiogram-gated (ECG-gated) technology was used to synchronously collect data, ensuring image acquisition during the relatively stable phases of vascular pulsation. The geometric information of all cases was collated and stored in Excel 2016 (Microsoft, Redmond, WA, USA) for subsequent statistical analysis. To validate the accuracy of the automated extraction of vascular features, we assigned two experienced radiologists to independently conduct a manual review of the vascular segmentation results and feature extraction. The radiologists carefully examined each vascular model, comparing the automated segmentation results with the actual vascular morphology. They manually corrected any parts with segmentation errors or inaccuracies. In addition, we carried out both intra-rater and inter-rater reliability evaluations. In the intra-rater reliability evaluation, a single researcher performed two vascular measurements on the identical samples at separate time points. The Intraclass Correlation Coefficient (ICC) was then calculated based on these two sets of measurement results to assess the consistency within the same rater. For the inter-rater reliability evaluation, two distinct researchers measured the same samples. The ICC of their measurement outcomes was determined to evaluate the agreement between different raters. By conducting these evaluations, we are able to efficiently validate the consistency of arterial measurement data and guarantee the reliability of our research results. Mean vessel density was calculated as the ratio of vessel volume to total intracranial volume. The extracted intracranial artery group included segments M2, M3, and M4 of the MCA, segments A2, A3, and A4 of the ACA, and segments P2, P3, and P4 of the PCA.
Statistical analysis
Continuous variables conforming to a normal distribution were presented as the mean ± standard deviation (SD), whereas those with a non-normal distribution were reported as the median (interquartile range). Categorical variables were expressed as frequencies (percentages). The Shapiro–Wilk test was utilized to assess the normality of continuous variables.
Differences in normally distributed continuous data between two groups were analyzed using Student’s t-test, while comparisons among multiple groups were performed using one-way ANOVA. For continuous data that did not follow a normal distribution, the Wilcoxon test was used for two-group comparisons, and the Kruskal–Wallis rank sum test was employed for multiple-group comparisons. Differences in categorical data between groups were assessed using the chi-square test.
When comparing gray matter volume (GMV), white matter volume (WMV), cerebrospinal fluid volume (CSFV), and white matter hyperintensity volume (WMH) across different alcohol-consuming groups, multiple testing was necessary. Bonferroni correction was applied for multiple-comparison adjustment to ensure result validity and reliability.
Multiple-comparison corrections were carried out in:
Comparing ADC values, GMV, CSFV, cortical thickness, curvature, and sulcal depth between the alcohol-consuming and control groups.
Examining the associations between alcohol consumption levels and ADC values, GMV, CSFV, cortical thickness, curvature, and sulcal depth in relevant brain regions within the alcohol-consuming group.
In these multiple-comparison analyses, adjusted p-values from Bonferroni correction were used, with adjusted p < 0.05 indicating statistical significance.
Control variables including age, previous cerebral infarction history, previous cerebral hemorrhage history, hypertension, diabetes mellitus, coronary atherosclerotic heart disease, and smoking status were included in correlation analyses between alcohol consumption levels and ADC values, GMV, CSFV, cortical thickness, curvature and sulcal depth.
To account for brain size effects, distal artery length, radius, curvature, flexibility, and tortuosity were normalized by taking the cube root of total intracranial volume (TIV). GMV, WMV, CSFV, WMH, regional gray matter and cerebrospinal fluid volumes were also normalized using TIV. In each brain region, cortical thickness, sulcal depth, and tortuosity were normalized relative to TIV.
For statistical analyses without multiple-group comparisons, uncorrected p-values were reported, with p < 0.05 for significance. All analyses were conducted using SPSS 26.0 (IBM, Armonk, NY, USA), and correlation coefficients were visualized as a matrix in Origin2024b.
Results
Baseline characteristics
A total of 50 alcoholics and 43 non-alcoholics, aged 22–65 years, were enrolled in the study. MR imaging was successfully completed for all participants. Clinical data were collected upon admission, and laboratory data were obtained within 24 h of admission.
Among the general metabolic indices, significant differences were observed in MCH, MCHC, platelets, platelet pressure product, total bilirubin, alkaline phosphatase, glutamyltransferase, triglycerides, ferritin, MMSE score, and MoCA score.
Specifically, the levels of MCH, MCHC, total bilirubin, glutamyltransferase, triglycerides, and ferritin were higher in alcoholics. In contrast, the levels of platelets, platelet pressure product, alkaline phosphatase, as well as MMSE and MoCA score were lower in alcoholics compared to the non-alcoholics. The data are presented in Table 1.
Regarding cytokines and neuroinflammatory markers, significant differences were found in IL-1b, IL-6, IL-10, GFAP, and sTREM2. IL-1b, GFAP, and sTREM2 levels were lower in alcoholics, whereas IL-6 and IL-10 levels were higher. The data are presented in Table 2.
Brain structures and vascular differences between alcoholics and non-alcoholics
Significant differences were observed in gray matter volume, white matter volume, cerebrospinal fluid volume, and cerebrospinal fluid high signal volume between alcoholics and non-alcoholics. Alcoholics exhibited lower gray matter and white matter volumes, while cerebrospinal fluid volume and cerebral white matter high signal volume were higher. These data are presented in Table 3.
Significant differences were also found in mean arterial density, mean arterial radius, mean arterial flexibility, and mean arterial tortuosity between the two groups. Alcoholics had lower mean arterial density, mean arterial radius, and mean arterial tortuosity, while mean arterial flexibility was higher. These data are presented in Table 3.
Additionally, with increasing alcohol consumption, there was a progressive decrease in gray matter and white matter volumes, accompanied by a gradual increase in cerebrospinal fluid volume and cerebral white matter high signal volume. These data are presented in Table 4.
Correlation analysis
Alcohol consumption was negatively correlated with gray matter volume (P < 0.05)and white matter volume (P < 0.05) and positively correlated with cerebrospinal fluid volume (P < 0.05) and cerebral white matter high signal volume (P < 0.05). Notably, alcohol consumption was negatively correlated with mean arterial density (P < 0.05), mean arterial radius (P = 0.051), and mean arterial length (P < 0.05), with significant correlations observed for mean arterial density and mean arterial length. The correlations with mean arterial curvature (P = 0.83), mean arterial flexibility (P = 0.56), and mean arterial tortuosity (P = 0.22) were not significant.
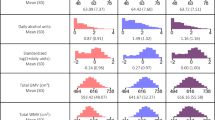
Furthermore, in alcoholics, gray matter volume was positively correlated with mean arterial density (P < 0.05), mean arterial radius (P < 0.05), mean arterial length (P < 0.05), and mean arterial tortuosity (P < 0.05), with significant correlations. White matter volume showed a significant positive correlation with mean arterial density (P < 0.05) and mean arterial length (P < 0.05). Conversely, cerebrospinal fluid volume was negatively correlated with mean arterial density (P < 0.05) and mean arterial length (P < 0.05), with significant correlations. These relationships are illustrated in Fig. 1.

Correlation analysis of alcohol consumption, gray matter volume, white matter volume, cerebrospinal fluid volume, cerebral white matter high signal volume, and morphological characteristics of distal intracranial arteries. The numerical values within the matrix denote correlation coefficients.
Comparison of alcoholics and non-alcoholics
ADC values across all brain regions were higher in alcoholics compared to non-alcoholics. Using the Brainnetome Atlas to segment the brain into 246 regions, ADC values were observed with statistically significant differences in 134 of these regions. The corresponding brain regions with significant correlations are detailed in Table 5.
Additionally, the brain regions that showed significant differences in gray matter volume mainly included the following areas: Left Hippocampus, Left Basal Forebrain, Left Middle Occipital Gyrus, Right Amygdala, Right Basal Forebrain, Right Inferior Occipital Gyrus, Right Middle Occipital Gyrus and Right Posterior Orbital Gyrus. These data are presented in Table 6.
Moreover, the brain regions exhibiting significant differences in cerebrospinal fluid volume mainly encompass the following areas: Left Cerebrospinal Fluid (Left CSF) region, Left Hippocampus, Left Angular Gyrus, Left Central Operculum, Left Inferior Temporal Gyrus, Left Subcallosal Area, Right Cerebrospinal Fluid (Right CSF) region, Right Calcarine Cortex and Right Cuneus. These data are presented in Table 6.
Cortical thickness, sulcal depth, and curvature were classified according to HCP-MMP1 mapping. The statistically significant differences in cortical thickness were tabulated in Table 7. Specifically, four brain regions demonstrated significance in cortical thickness: Left Area anterior 9-46v, Left Area_TA2, Left Medial Belt Complex, and Right Pirform_Cortex. In contrast, after multiple-test correction, no significant differences in sulcal depth and curvature were detected across any of the brain regions between the two groups. In regions where differences were statistically significant, alcoholics exhibited lower cortical thickness.
In addition to these results, a correlation analysis was conducted to explore the relationships between alcohol consumption levels and apparent diffusion coefficient (ADC) values, gray matter volume (GMV), cerebrospinal fluid volume (CSFV), cortical thickness, curvature, and sulcal depth in relevant brain regions among individuals in the alcohol-consuming group. Variables such as age, history of previous cerebral infarction, history of previous cerebral hemorrhage, hypertension, diabetes, coronary heart disease, and smoking history were taken into account as potential confounding factors.
Correlation of ADC values in alcoholics
In individuals with alcoholism, the apparent diffusion coefficient (ADC) values were positively correlated with the quantity of alcohol consumed. Before accounting for confounding factors, 50 brain regions exhibited significant correlations. The specific brain regions with significant correlations are presented in Table 8. After controlling for confounding factors, the ADC values in 45 brain regions remained associated with the amount of alcohol consumed. The detailed information can be found in Table 9.
Correlation of gray matter volume in alcoholics
Prior to controlling for confounding factors, the gray matter volume in 11 brain regions was correlated with the amount of alcohol consumed. These regions were the Left 4th Ventricle, Left Amygdala, Left Brainstem, Left Cerebellum White Matter, Left Hippocampus, Left Entorhinal Area, Right 4th Ventricle, Right Brainstem, Right Entorhinal Area, Right Fusiform Gyrus, and Right Gyrus Rectus.
Among these regions, the gray matter volumes of the Left 4th Ventricle, Left Brainstem, Left Cerebellum White Matter, Right 4th Ventricle, and Right Brainstem showed a positive correlation with the amount of alcohol consumed. In contrast, the gray matter volumes of the remaining regions were negatively correlated with the amount of alcohol consumed. The detailed information is presented in Table 10.
After controlling for confounding factors, it was found that the gray matter volumes in 5 brain regions were correlated with the amount of alcohol consumed. These regions included the Right Accumbens, Left Hippocampus, Left Posterior Insula, Right Posterior Orbital Gyrus, and Left Planum Polare. Furthermore, the gray matter volumes in all of these regions showed a positive correlation with the amount of alcohol consumed. The detailed data can be found in Table 11.
Correlation of cerebrospinal fluid volume in alcoholics
Prior to controlling for confounding factors, the cerebrospinal fluid volume in 10 brain regions was correlated with the amount of alcohol consumed. These regions were the Left Caudate, Left Hippocampus, Left Thalamus Proper, Left Inferior Temporal Gyrus, Left Middle Cingulate Gyrus, Left Posterior Insula, Left Planum Polare, Right Accumbens, Right Lateral Orbital Gyrus, and Right Posterior Orbital Gyrus. All of these brain regions exhibited a positive correlation between their cerebrospinal fluid volumes and the amount of alcohol consumed. The detailed information can be found in Table 12.
After accounting for confounding factors, the cerebrospinal fluid volume in 5 brain regions was found to be correlated with the amount of alcohol consumed. These regions were the Right Accumbens, Left Hippocampus, Left Posterior Insula, Right Posterior Orbital Gyrus, and Left Planum Polare. Moreover, the CSFV in all of these regions showed a positive correlation with the amount of alcohol consumed. The detailed data are presented in Table 13.
Correlation of cortical thickness in alcoholics
After controlling for confounding factors, the cortical thickness in 13 brain regions was found to be correlated with the amount of alcohol consumed. These brain regions encompassed Area_3a, Area_43, Area_52, Posterior Insular Area 2, Area_TA2, Frontal Opercular_Area 1, Area_Posterior Insular_1, Medial Belt Complex, and Para-Insular_Area on the left hemisphere, and Area_3a, Area_52, Area_TA2, and Para-Insular_Area on the right hemisphere. The cortical thickness in all of these brain regions exhibited a negative correlation with the amount of alcohol consumed. The detailed information can be found in Table 14.
Correlation of curvature in alcoholics
After controlling for confounding factors, the curvature in 5 brain regions was found to be correlated with the amount of alcohol consumed. These regions included the Frontal_Opercular_Area_2, Area_Posterior Insular_1, and Insular Granular Complex in the left hemisphere, as well as the RetroInsular Cortex and Area_Posterior Insular_1 in the right hemisphere. The curvature in all of these brain regions was negatively correlated with the amount of alcohol consumed. Details can be found in Table 15.
Correlation of sulcal depth in alcoholics
After accounting for confounding factors, the sulcal depth in eight brain regions was determined to be correlated with the amount of alcohol consumed. On the left hemisphere, these regions were the Eighth_Visual_Area, Primary_Motor_Cortex, Frontal_Opercular_Area_2, Area_Posterior Insular_1, and Insular Granular Complex. On the right hemisphere, they were the Middle Temporal_Area, RetroInsular Cortex, and Area_Posterior Insular_1. All of these brain regions demonstrated a negative correlation between their sulcal depth and the amount of alcohol consumed. The detailed information is presented in Table 16.
Discussion
Alcohol consumption is linked to reduced brain volume, with even light to moderate drinking capable of causing brain damage. Alcohol intake is negatively correlated with overall brain volume, regional gray matter volume, and white matter microstructure, with this correlation intensifying as alcohol consumption increases3. Numerous studies have established that higher alcohol use and alcohol abuse are associated with reduced cortical and subcortical volumes26,27. A case–control study of adolescents highlighted a detrimental association between alcohol use and the integrity of white matter microstructure, with widespread FA alterations observed in those beginning to abuse alcohol. Notably, white matter atrophy and demyelination of the corpus callosum are two of the most significant markers of alcoholism in adults28.
In our study, our primary study population consisted of long-term chronic drinkers who have not yet developed alcohol dependence or alcohol use disorders. In examining the association between neuroimaging measures and alcohol use, gray matter volume and white matter volume were reduced in alcoholics, while cerebrospinal fluid volume and cerebral white matter high signal volume were increased. Previous research has also shown similar trends in these brain volume changes among alcohol-consuming populations. However, our study further differentiates by focusing on a population without overt alcohol-use disorders, providing insights into the early-stage effects of long-term alcohol consumption on the brain structure.
In our study, cortical thickness, curvature, and sulcal depth all showed negative correlations with alcohol consumption. This indicates that as alcohol intake rises, these structural features of the brain tend to decrease correspondingly. We also found that the brain regions where cortical thickness is correlated with alcohol consumption are mainly concentrated in the frontal lobe, temporal lobe, insular lobe, and the medial surface of the brain. These regions play crucial roles in functions such as sensation, movement, language, memory, and emotion. A previous study involving 436 twin individuals found that genetic susceptibility to alcohol exposure and alcohol use led to reduced cortical thickness in several regions29. Our findings not only validate the decrease in cortical thickness but also pinpoint specific regions that are more severely impacted within our group of long-term drinkers. By demonstrating the regional specificity of these alterations in a distinct study population, our results contribute to the existing body of knowledge.
Employing Neuromorphometrics mapping, our study carried out a more detailed segmentation of the gray matter and cerebrospinal fluid throughout the entire brain. In alcoholics, the structural brain changes mainly affected the orbital surface of the frontal lobe, including the bilateral gyrus rectus, the right lateral orbital gyrus, and the right posterior orbital gyrus; the limbic system, such as the bilateral amygdala, bilateral hippocampus, the middle and posterior parts of the left cingulate gyrus; the bilateral brainstem; the bilateral fusiform gyrus; the left caudate nucleus; the left thalamus; the left inferior temporal gyrus; the bilateral cerebellum; bilateral CSF regions and the bilateral fourth ventricles. Previous research has shown that higher alcohol consumption is associated with an increased risk of hippocampal atrophy in a dose-dependent manner. Even moderate drinkers (14–21 units/week) were three times more likely to experience right hippocampal atrophy compared to non-drinkers. Higher alcohol use has also been linked to differences in corpus callosum microstructure and a rapid decline in lexical fluency30. The thalamus, limbic system, cerebellum, and particularly the frontal lobe, are more vulnerable to alcohol-related brain damage than other brain regions. The limbic system primarily includes the nucleus ambiguus, amygdala, and hypothalamus31. Alcohol consumption leads to a reduction in cortical gray matter volume, particularly in the dorsolateral prefrontal cortex (DLPFC) and premotor cortex32. In comparison with previous research, our detailed mapping of the brain regions affected by alcohol offers a more comprehensive perspective on the spatial distribution of alcohol-induced structural alterations. This enhanced understanding can facilitate a more accurate comprehension of the functional implications of alcohol-related brain damage. Given that different brain regions are associated with specific cognitive and emotional functions, our findings contribute significantly to elucidating how alcohol consumption impacts various aspects of brain function.
These brain structures play an integral role in functions including memory, judgment, abstract thinking, cognition, emotion, and impulsive behavior. The amygdala, a central hub in the subcortical region, has been linked to various psychiatric disorders, including anxiety disorders (such as post-traumatic stress disorder, phobias, and panic), depression, schizophrenia, and autism33. Additionally, the amygdala forms extensive circuits with the medial prefrontal cortex, orbitofrontal cortex, and hippocampus, mediating abnormal social functioning through complex interactions34. The medial frontal cortex is believed to govern cognitive functions, including thinking and perception, and is closely associated with memory, problem-solving, and emotions. It is intricately connected to the limbic system, particularly the amygdala, orbitofrontal cortex, and hippocampus35,36,37. Stimulation of the insula can disrupt visceral functions, causing symptoms such as nausea, belching, increased gastrointestinal motility, or fullness. The anterior insula is involved in olfactory, gustatory, and limbic functions, while the posterior insula is associated with auditory and autonomic sensory-motor functions, as well as addiction38,39,40,41.
Patients with chronic alcohol consumption frequently present symptoms such as anxiety, dysphoria, depressed mood, insomnia, nausea, vomiting, sweating, palpitations, agitation, and tremors. Notably, these symptoms closely resemble those resulting from the structural lesions mentioned above.
In our study, even though the alcoholics had not yet shown obvious cognitive impairment, their Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) scores were lower compared to those of non-alcoholics. This finding reflected the impaired functions in the frontal lobes and hippocampus42,43. Zhao et al. (2024) explored the molecular mechanisms of alcohol-induced neurotoxicity and its role in Alzheimer’s disease pathology44.
The ADC value reflects the diffusion rate of water molecules, indirectly indicating changes in microstructure and the movement of water molecules within the extracellular matrix45. The Brownian motion of water molecules is inversely proportional to cellular tissue density, and the DWI signal is inversely proportional to tissue integrity46.
The apparent diffusion coefficient (ADC) in various brain regions was quantified by means of a semi-automated processing program. In our study, we utilized the Brainnetome Atlas to divide the brain into 246 regions. We observed that, across these regions, the apparent diffusion coefficient (ADC) values in alcoholics were consistently higher than those in non-alcoholics. Statistical analysis revealed significant differences in 134 of these regions, which was substantially more than the number of regions showing gray matter alterations. This finding suggests that changes in water molecule diffusion within the brains of alcoholics may occur prior to alterations in gray matter. Previous studies have also suggested that the brain MRI apparent diffusion coefficient (ADC) reflects increased hydrogen movement in areas of neurodegeneration, with pathological changes in the shell nuclei detectable as elevated ADC even in the early stages of MSA-P47. These findings are consistent with our results. Wang et al. (2024) used diffusion tensor imaging to study the impact of chronic alcohol intake on cognitive function and brain microstructure. They found that chronic alcohol intake was associated with cognitive decline and alterations in brain microstructure, which is also consistent with our results48.
In contrast to previous studies, our research does not solely focus on directly observing the structural changes in the brain’s gray and white matter induced by long-term alcohol consumption. Instead, we also direct our attention to the influence of alcohol on the brain’s microstructure and water molecule diffusion, as assessed by Apparent Diffusion Coefficient (ADC) values. By doing so, we explore the early-stage changes from a microscopic viewpoint. Regarding research methods, previous investigations may have utilized relatively simple or traditional brain atlases, which divided the brain into a smaller number of regions. In our study, however, we employ the Brainnetome Atlas to partition the brain into 246 regions. This allows for a more detailed analysis of regional variations, enabling us to detect subtle differences and relationships that might have been overlooked in prior research. This approach not only offers a more comprehensive understanding of the effects of alcohol on the brain but also contributes to a more in-depth exploration of the underlying mechanisms of alcohol-related brain alterations.
In alcoholics, the apparent diffusion coefficient (ADC) values showed a positive correlation with alcohol consumption. The increase in ADC values can likely be ascribed to several factors. These include a reduction in tissue density, a decrease in the volumes of both gray and white matter, an expansion in cerebrospinal fluid volume, and the infiltration of cerebrospinal fluid into the brain parenchyma. The influx of cerebrospinal fluid into the brain has been shown to enhance free water diffusion, thereby increasing ADC49. In fetuses and neonates, as the brain matures, there is an increase in lipid content and tissue density, the formation of new synapses, and the bundling of fibrous tissue, all of which correspond with decreased water content and a gradual reduction in water diffusion rates50.
Cerebral blood flow (CBF) plays a pivotal role in maintaining brain function and is closely linked to structural changes in the brain. Intracranial vascular characteristics, such as vessel radius and length, serve as indicators of cerebral blood flow13. In subjects with deep subcortical lesions, significantly increased capillary wall thickness and decreased capillary density have been observed, both of which contribute to reduced cerebral blood flow51. Additionally, a study found that mice in the high-alcohol group had significantly smaller blood vessel diameters compared to their low-alcohol counterparts in weight-matched pairs52.
While alterations in CBF have been linked to various neurological disorders, including stroke and dementia, chronic reductions in CBF may contribute to brain atrophy and increased signaling in white matter53. In patients with Alzheimer’s disease, reductions in CBF within the cortical gray matter primarily affect the parietal and temporal lobes, with microstructural abnormalities predominantly observed in the parietal, temporal, and frontal lobes. Lower CBF values in the left occipital lobe, left frontal lobe, and right parietal lobe have been associated with higher mean diffusivity (MD), lower fractional anisotropy (FA), or lower mean kurtosis (MK) values54. In white matter, CBF has shown a positive correlation with subject anisotropy scores in the corpus callosum, right posterior thalamic radiation, right inferior fronto-occipital fasciculus, right inferior longitudinal fasciculus, and right superior longitudinal fasciculus. Additionally, radial diffusivity is negatively correlated with CBF in similar regions, and a positive correlation exists between CBF and FA within the inner white matter bundle55. Studies of patients with ketonuria have also demonstrated that white matter lesions are associated with reduced cerebral blood flow, particularly in the occipital lobe, where CBF to the left posterior cerebral artery is significantly diminished56.
Relatively few studies have been dedicated to quantifying the cerebrovascular morphology in alcoholics. In our research, we utilized 3D-Time-Of-Flight Magnetic Resonance Angiography (3D-TOF MRA) to acquire vascular information. Subsequently, image processing techniques were employed to quantify relevant characteristics of the intracranial distal arteries in alcoholics, such as the mean arterial density, mean arterial radius, and mean arterial length. The analysis indicated that in alcoholics, the mean arterial density, mean arterial radius, and mean arterial tortuosity were lower, while the mean arterial flexibility was higher. There was no significant difference in mean vessel length. Notably, a positive correlation was found between gray matter volume and mean arterial length, density, and radius, with significant associations. Similarly, white matter volume demonstrated a positive correlation with mean arterial length and density, with significant correlations. However, the positive correlation between white matter volume and mean arterial radius was not significant. In contrast, the cerebrospinal fluid volume (CSFV) was negatively correlated with mean arterial length and density. Although there was a negative correlation between CSFV and arterial radius, it was not highly pronounced. This gives rise to the hypothesis that the altered cerebrovascular morphology in alcoholics serves as a contributing factor to the alcohol-induced structural changes in the brain. Zhang et al. (2023) also explored the association between cerebrovascular changes and alcohol-related brain damage in a longitudinal study. Their findings support our hypothesis that altered cerebrovascular morphology is a contributing factor to alcohol-induced structural changes in the brain57.
The MRI biomarkers identified in our study hold substantial clinical significance. In the brains of alcoholics, elevated ADC values, which are observable in numerous regions, can function as an early indicator of alcohol-related brain damage. They might signal the onset of early neurodegeneration even before gray matter alterations become visually detectable, thus enabling the early detection of damage for timely intervention.
The changes in cerebrovascular features, such as decreased arterial density, radius, and length, also bear clinical relevance. These alterations are associated with modified cerebral blood flow, which can contribute to brain structural changes. Measuring these vascular biomarkers can assist clinicians in understanding disease mechanisms and devising more effective treatments.
For the utilization of these biomarkers in diagnosis, it is advisable to implement a comprehensive MRI protocol that includes DWI, T1-weighted, T2-weighted, and MRA sequences for patients under suspicion. Advanced image processing techniques can be employed to extract these biomarkers. By combining them with clinical evaluations, more accurate diagnoses and prognoses can be achieved.
Clinicians can utilize these biomarkers to screen high-risk individuals, such as heavy drinkers, and to monitor the progression of brain damage over time. Additionally, these biomarkers can be used to assess the efficacy of interventions, like alcohol cessation programs. If, following a period of intervention, an individual demonstrates an improvement in these biomarker values, it may suggest a positive response to the treatment.
This study has several limitations.
First, being a cross-sectional study, it provides only a static snapshot of the brain’s structural and vascular morphological features at a single point in time. Without dynamic follow-up, we cannot observe how these features evolve over time.
Second, the sample size in our study is relatively small. This may have impeded our ability to detect some potential relationships between vascular morphological features and structural brain changes. A larger and more diverse sample would be required to confirm and generalize our findings.
Third, due to the fact that our examination room does not routinely perform more advanced diffusion-weighted imaging techniques, this study relied solely on the Apparent Diffusion Coefficient (ADC) value to represent the diffusion coefficient of water molecules. For example, Diffusion Tensor Imaging (DTI), which could provide more comprehensive diffusion-related information, is not part of our standard examination protocol. Consequently, we were unable to use these techniques to gain a deeper understanding of the brain’s microstructural changes related to water molecule diffusion.
Fourth, the accuracy of Magnetic Resonance Angiography (MRA) in evaluating terminal small vessels is inherently limited. In the hospital where this study was conducted, many MRA-based microvascular assessment items, as well as imaging techniques such as arterial spin labeling (ASL) and dynamic susceptibility contrast (DSC) perfusion MRI, are not yet available. As a result, our study had to rely solely on MRA to obtain the morphological characteristics of distal intracranial arteries. We were restricted to examining segments M2, M3, and M4 of the Middle Cerebral Artery (MCA), segments A2, A3, and A4 of the Anterior Cerebral Artery (ACA), and segments P2, P3, and P4 of the Posterior Cerebral Artery (PCA). This constrained approach, due to the lack of more comprehensive techniques, may reduce the accuracy of measurements related to vessel volume, curvature, and other crucial parameters.
Fifth, the Neuromorphometrics mapping used in this study only differentiates between different regions of gray matter and cerebrospinal fluid, excluding white matter from its scope.
Finally, the techniques for voxel-based structural MRI analysis and the assessment of intracranial vessel morphological characteristics via MRA are not yet widely used in clinical practice. This lack of widespread implementation, combined with the unavailability of relevant examination items in our facility, severely restricts their current practical application in real-world medical settings.
Nevertheless, we are committed to overcoming these limitations in our future research. This will involve conducting longitudinal studies to track changes over time, significantly increasing the sample sizes to enhance statistical power and generalizability, and exploring more advanced imaging modalities. By doing so, we aim to achieve a more comprehensive and in-depth understanding of the research topic.
Conclusion
The diffusion of water molecules in the brains of alcoholics is modified before any detectable alterations in gray matter structure occur. In chronic alcoholics, cerebrovascular morphological features, including mean arterial density, mean arterial radius, and mean arterial length, are strongly correlated with structural changes in the brain. These changes in cerebrovascular morphology are regarded as a contributing factor to the structural alterations seen in the brains of chronic alcoholics.
Data availability
Data is provided within the manuscript and supplementary information files, further inquiries can be directed to the corresponding author Jia Yanjie.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- MRA:
-
Magnetic resonance angiography
- ADC:
-
Apparent diffusion coefficient
- VBM:
-
Voxel-based morphometry
- SBM:
-
Surface-based morphology
- DWI:
-
Diffusion-weighted imaging
- DTI:
-
Diffusion tensor imaging
- TIV:
-
Total intracranial volume
- GMV:
-
Gray matter volume
- WMV:
-
White matter volume
- CSFV:
-
Cerebrospinal fluid volume
- WMH:
-
Cerebral white matter high signal volume
- MCV:
-
Mean corpuscular volume
- MCH:
-
Mean corpuscular hemoglobin
- MCHC:
-
Mean corpuscular hemoglobin concentration
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate transaminase
- PT:
-
Prothrombin time
- PTA:
-
Prothrombin activity
- INR:
-
International normalized ratio
- FIB:
-
Fibrinogen
- TT:
-
Thrombin time
- APTT:
-
Activated partial thromboplastin time
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- FT3:
-
Free triiodothyronine
- FT4:
-
Free thyroxine
- TSH:
-
Thyroid-stimulating hormone
- AUDIT:
-
Alcohol use disorders identification test
- PSQI:
-
Pittsburgh sleep quality index
- MMSE:
-
Mini-mental State Examination
- MoCA:
-
Montreal cognitive assessment
- IL-1b:
-
Interleukin-1b
- IL-2:
-
Interleukin-2
- IL-4:
-
Interleukin-4
- IL-6:
-
Interleukin-6
- IL-10:
-
Interleukin-10
- TNF-α:
-
Tumor necrosis factor-α
- INF-γ:
-
Interferon-γ
- GFAP:
-
Glial fibrillary acidic protein
- NFL:
-
Neurofilament light chain
- sTREM2:
-
Soluble Triggering receptor expressed on myeloid cells 2
- HCP-MMP1:
-
Human Connectome Project Multi-modal Parcellation 1.0
- MCA:
-
Middle cerebral artery
- ACA:
-
Anterior cerebral artery
- PCA:
-
Posterior cerebral artery
- FA:
-
Fractional anisotropy
- MD:
-
Mean diffusivity
- MK:
-
Mean kurtosis
- MSA-P:
-
Multiple system atrophy-P
- mL:
-
Milliliter
- STL:
-
Stereolithrography
References
Zou, X., Durazzo, T. C. & Meyerhoff, D. J. Regional brain volume changes in alcohol-dependent individuals during short-term and long-term abstinence. Alcohol Clin. Exp. Res. 42(6), 1062–1072. https://doi.org/10.1111/acer.13757 (2018).
Bühler, M. & Mann, K. Alcohol and the human brain: A systematic review of different neuroimaging methods. Alcohol Clin. Exp. Res. 35(10), 1771–1793. https://doi.org/10.1111/j.1530-0277.2011.01540.x (2011).
Daviet, R. et al. Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat. Commun. 13(1), 1175. https://doi.org/10.1038/s41467-022-28735-5 (2022).
Zhou, X. et al. Long-term alcohol consumption and brain atrophy: A meta-analysis of structural MRI studies. J. Neurol. Sci. 456, 120056. https://doi.org/10.1016/j.jns.2024.120056 (2024).
Pfefferbaum, A. et al. Adolescent development of cortical and white matter structure in the NCANDA sample: Role of sex, ethnicity, puberty, and alcohol drinking. Cereb. Cortex. 26(10), 4101–4121. https://doi.org/10.1093/cercor/bhv205 (2016).
Topiwala, A., Ebmeier, K. P., Maullin-Sapey, T. & Nichols, T. E. Alcohol consumption and MRI markers of brain structure and function: Cohort study of 25,378 UK Biobank participants. Neuroimage Clin. 35, 103066. https://doi.org/10.1016/j.nicl.2022.103066 (2022).
Ashburner, J. & Friston, K. J. Voxel-based morphometry—The methods. Neuroimage 11(6 Pt 1), 805–821. https://doi.org/10.1006/nimg.2000.0582 (2000).
Dale, A. M., Fischl, B. & Sereno, M. I. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 9(2), 179–194. https://doi.org/10.1006/nimg.1998.0395 (1999).
Jenkinson, M., Beckmann, C. F., Behrens, T. E., Woolrich, M. W. & Smith, S. M. FSL. Neuroimage 62(2), 782–790. https://doi.org/10.1016/j.neuroimage.2011.09.015 (2012).
Fan, L. et al. The human brainnetome atlas: A new brain atlas based on connectional architecture. Cereb. Cortex. 26(8), 3508–3526. https://doi.org/10.1093/cercor/bhw157 (2016).
Qi, Q. et al. Morphological changes of cerebral vessels and expression patterns of MMP-2 and MMP-9 on cerebrovascular wall of alcoholic rats. Int. J. Clin. Exp. Pathol. 7(5), 1880–1888 (2014).
Liu, X. et al. Progressive mechanical and structural changes in anterior cerebral arteries with Alzheimer’s disease. Alzheimers Res. Ther. 15(1), 185. https://doi.org/10.1186/s13195-023-01331-5 (2023).
Cheng, H. et al. Association between morphologic features of intracranial distal arteries and brain atrophy indexes in cerebral small vessel disease: A voxel-based morphometry study. Front. Neurol. 14, 1198402. https://doi.org/10.3389/fneur.2023.1198402 (2023).
Edelman, R. R. & Koktzoglou, I. Noncontrast MR angiography: An update. J. Magn. Reson. Imaging. 49(2), 355–373. https://doi.org/10.1002/jmri.26288 (2019).
Gao, X. et al. A fast and fully automatic method for cerebrovascular segmentation on time-of-flight (TOF) MRA image. J. Digit. Imaging. 24(4), 609–625. https://doi.org/10.1007/s10278-010-9326-1 (2011).
Chen, L. et al. Quantification of morphometry and intensity features of intracranial arteries from 3D TOF MRA using the intracranial artery feature extraction (iCafe): A reproducibility study. Magn. Reson. Imaging. 57, 293–302. https://doi.org/10.1016/j.mri.2018.12.007 (2019).
Wang, X. et al. Skeleton-based cerebrovascular quantitative analysis. BMC Med. Imaging. 16(1), 68. https://doi.org/10.1186/s12880-016-0170-8 (2016).
Deshpande, A. et al. Automatic segmentation, feature extraction and comparison of healthy and stroke cerebral vasculature. Neuroimage Clin. 30, 102573. https://doi.org/10.1016/j.nicl.2021.102573 (2021).
Fedorov, A. et al. 3D slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging. 30(9), 1323–1341. https://doi.org/10.1016/j.mri.2012.05.001 (2012).
Mandolini, M. et al. Comparison of three 3D segmentation software tools for hip surgical planning. Sensors (Basel). 22(14), 5242. https://doi.org/10.3390/s22145242 (2022).
Rehm, J. The risks associated with alcohol use and alcoholism. Alcohol Res. Health. 34(2), 135–143 (2011).
China Nutrition Society. Dietary Guidelines for Chinese Residents (2022 Edition). People’s Medical Publishing House, 2022.
Wang, L. M. et al. Epidemiological study on alcohol consumption and agricultural profession-related injuries among minority residents from the northern parts of China. Zhonghua Liu Xing Bing Xue Za Zhi 30(12), 1252–1257 (2009) (in Chinese).
Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R. & Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 88(12), 1795–1805. https://doi.org/10.1111/j.1360-0443.1993.tb02093.x (1993).
Glasser, M. F. et al. A multi-modal parcellation of human cerebral cortex. Nature 536(7615), 171–178. https://doi.org/10.1038/nature18933 (2016).
Baranger, D. A. A. et al. Convergent evidence for predispositional effects of brain gray matter volume on alcohol consumption. Biol. Psychiatry. 87(7), 645–655. https://doi.org/10.1016/j.biopsych.2019.08.029 (2020).
Hatoum, A. S., Johnson, E. C., Agrawal, A. & Bogdan, R. Brain structure and problematic alcohol use: A test of plausible causation using latent causal variable analysis. Brain Imaging Behav. 15(6), 2741–2745. https://doi.org/10.1007/s11682-021-00482-z (2021).
Zhao, Q. et al. Association of heavy drinking with deviant fiber tract development in frontal brain systems in adolescents. JAMA Psychiat. 78(4), 407–415. https://doi.org/10.1001/jamapsychiatry.2020.4064 (2021).
Harper, J. et al. The effects of alcohol and cannabis use on the cortical thickness of cognitive control and salience brain networks in emerging adulthood: A co-twin control study. Biol. Psychiatry. 89(10), 1012–1022. https://doi.org/10.1016/j.biopsych.2021.01.006 (2021).
Topiwala, A. et al. Moderate alcohol consumption as risk factor for adverse brain outcomes and cognitive decline: Longitudinal cohort study. BMJ 357, j2353. https://doi.org/10.1136/bmj.j2353 (2017).
Kong, L. M., Zeng, J. Y., Zheng, W. B., Shen, Z. W. & Wu, R. H. Effects of acute alcohol consumption on the human brain: Diffusional Kurtosis imaging and arterial spin-labeling study. AJNR Am. J. Neuroradiol. 40(4), 641–647. https://doi.org/10.3174/ajnr.A5992 (2019).
Morris, L. S., Dowell, N. G., Cercignani, M., Harrison, N. A. & Voon, V. Binge drinking differentially affects cortical and subcortical microstructure. Addict. Biol. 23(1), 403–411. https://doi.org/10.1111/adb.12493 (2018).
LeDoux, J. The amygdala. Curr. Biol. 17(20), R868–R874. https://doi.org/10.1016/j.cub.2007.08.005 (2007).
Meisner, O. C., Nair, A. & Chang, S. W. C. Amygdala connectivity and implications for social cognition and disorders. Handb. Clin. Neurol. 187, 381–403. https://doi.org/10.1016/B978-0-12-823493-8.00017-1 (2022).
Vaidya, A. R. & Fellows, L. K. Ventromedial frontal lobe damage affects interpretation, not exploration, of emotional facial expressions. Cortex 113, 312–328. https://doi.org/10.1016/j.cortex.2018.12.013 (2019).
de la Vega, A., Chang, L. J., Banich, M. T., Wager, T. D., Yarkoni, T. Large-scale meta-analysis of human medial frontal cortex reveals tripartite functional organization. J. Neurosci. 36(24), 6553–6562. https://doi.org/10.1523/JNEUROSCI.4402-15.2016 (2016). Erratum in: J. Neurosci. 37(13):3735. https://doi.org/10.1523/JNEUROSCI.0471-17.2017 (2017).
Minxha, J., Adolphs, R., Fusi, S., Mamelak, A. N. & Rutishauser, U. Flexible recruitment of memory-based choice representations by the human medial frontal cortex. Science 368(6498), eaba3313. https://doi.org/10.1126/science.aba3313 (2020).
Ellingsen, D. M. et al. Cyclic vomiting syndrome is characterized by altered functional brain connectivity of the insular cortex: A cross-comparison with migraine and healthy adults. Neurogastroenterol. Motil. 29(6), 2. https://doi.org/10.1111/nmo.13004 (2017).
Haaranen, M. et al. Anterior insula stimulation suppresses appetitive behavior while inducing forebrain activation in alcohol-preferring rats. Transl. Psychiatry. 10(1), 150. https://doi.org/10.1038/s41398-020-0833-7 (2020).
Nicolas, C. et al. Linking emotional valence and anxiety in a mouse insula-amygdala circuit. Nat. Commun. 14(1), 5073. https://doi.org/10.1038/s41467-023-40517-1 (2023).
Roquet, D. & Conti, F. Disentangling the association between the Insula and the autonomic nervous system. J. Neurosci. 41(14), 3051–3053. https://doi.org/10.1523/JNEUROSCI.2225-20.2021 (2021).
Sui, H., Yang, J., Xiang, H. & Yan, C. Combining ADC values in DWI with rCBF values in arterial spin labeling (ASL) for the diagnosis of mild cognitive impairment (MCI). Medicine (Baltimore) 102(37), e34979. https://doi.org/10.1097/MD.0000000000034979 (2023).
Tao, J. et al. Mind-body exercise improves cognitive function and modulates the function and structure of the hippocampus and anterior cingulate cortex in patients with mild cognitive impairment. Neuroimage Clin. 23, 101834. https://doi.org/10.1016/j.nicl.2019.101834 (2019).
Zhao, Y. et al. Molecular mechanisms of alcohol-induced neurotoxicity and its role in Alzheimer’s disease pathology. J. Neurosci. Res. 102(8), 1521–1533. https://doi.org/10.1002/jnr.25340 (2024).
Han, Y., Wu, P., Tian, J., Chen, H. & Yang, C. Diffusion Kurtosis imaging and diffusion weighted imaging comparison in diagnosis of early hypoxic-ischemic brain edema. Eur. J. Med. Res. 28(1), 159. https://doi.org/10.1186/s40001-023-01090-x (2023).
Lindt, B., Richter, H. & Del Chicca, F. Investigated regional apparent diffusion coefficient values of the morphologically normal feline brain. J. Feline Med. Surg. 24(8), e214–e222. https://doi.org/10.1177/1098612X221101535 (2022).
Umemura, A. et al. Diagnostic accuracy of apparent diffusion coefficient and 123I-metaiodobenzylguanidine for differentiation of multiple system atrophy and Parkinson’s disease. PLoS ONE 8(4), e61066. https://doi.org/10.1371/journal.pone.0061066 (2013).
Wang, Z. et al. Impact of chronic alcohol intake on cognitive function and brain microstructure: A diffusion tensor imaging study. Alcohol Alcohol. 59(2), 193–200. https://doi.org/10.1093/alcalc/agad097 (2024).
Demiral, ŞB. et al. Apparent diffusion coefficient changes in human brain during sleep—Does it inform on the existence of a glymphatic system?. Neuroimage 185, 263–273. https://doi.org/10.1016/j.neuroimage.2018.10.043 (2019).
Schönberg, N. et al. The influence of various cerebral and extracerebral pathologies on apparent diffusion coefficient values in the fetal brain. J. Neuroimaging 30(4), 477–485. https://doi.org/10.1111/jon.12727 (2020).
Tu, M. C., Chung, H. W., Hsu, Y. H., Yang, J. J. & Wu, W. C. Stage-dependent cerebral blood flow and leukoaraiosis couplings in subcortical ischemic vascular disease and Alzheimer’s disease. J. Alzheimers Dis. 86(2), 729–739. https://doi.org/10.3233/JAD-215405 (2022).
Mozumder, M. et al. Quantitative histomorphometry of capillary microstructure in deep white matter. Neuroimage Clin. 23, 101839. https://doi.org/10.1016/j.nicl.2019.101839 (2019).
Meombe Mbolle, A., Yang, H. & Jiang, H. Photoacoustic imaging for in vivo quantification of alcohol-induced structural and functional changes in cerebral vasculature in high alcohol-preferring mice (HAP). Alcohol 100, 23–30. https://doi.org/10.1016/j.alcohol.2022.01.001 (2022).
Niu, X. et al. The correlation between changes in gray matter microstructure and cerebral blood flow in Alzheimer’s disease. Front. Aging Neurosci. 15, 1205838. https://doi.org/10.3389/fnagi.2023.1205838 (2023).
Giezendanner, S. et al. Microstructure and cerebral blood flow within white matter of the human brain: A TBSS analysis. PLoS ONE 11(3), e0150657. https://doi.org/10.1371/journal.pone.0150657 (2016).
Steiner, L. et al. Cerebral blood flow and white matter alterations in adults with phenylketonuria. Neuroimage Clin. 41, 103550. https://doi.org/10.1016/j.nicl.2023.103550 (2024).
Zhang, Y. et al. Association between cerebrovascular changes and alcohol-related brain damage: A longitudinal study. Stroke Vasc. Neurol. 8(4), e000787. https://doi.org/10.1136/svn-2023-000787 (2023).
Acknowledgements
We would like to extend our sincere gratitude to Dr. Binbin Nie from the Chinese Academy of Sciences for her invaluable assistance in the NMR image analysis. Additionally, we are thankful to our colleagues in the Neurology, Laboratory, and Imaging departments. Their contributions have been highly appreciated. Moreover, we are deeply indebted to the associate editor and the reviewers. Their constructive feedback has significantly enhanced the quality of this paper.
Author information
Authors and Affiliations
Contributions
Yanjie Jia conceived the research idea. He provided guidance and supervision during the implementation of the study, offered expert opinions, and reviewed and revised the manuscript. Longbin Jia, Lina Xu, Fengbing Yang, Jinna Li, and Hongjiang Cheng contributed ideas and expert opinions throughout the execution of the study. Huanhuan Cui was in charge of administering all the scales. Jing Guo was responsible for collecting blood specimens, as well as extracting and preserving the serum. Jianqiang Wang and Chong Li oversaw the collection of qualified MRI and 3D-TOF MRA data. Cuiqin Wang was accountable for the detailed experimental design, its execution, data collection, organization, analysis, graphing, and for writing and revising the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
In accordance with the Declaration of Helsinki, this study was approved by the Ethics Committee of Jincheng City People’s Hospital (JCPH.NO20230710004). All participants, or their guardians, provided written informed consent.
Consent for publication
All authors contributed to this article and approved its submission.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, C., Jia, Y., Jia, L. et al. Morphologic characteristics of distal intracranial arteries in relation to structural changes in the brain after chronic alcohol consumption. Sci Rep 15, 23654 (2025). https://doi.org/10.1038/s41598-025-07984-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-07984-6
