
Abstract
Current methods for hyoid suspension in the treatment of upper airway (UA) collapse have some shortcomings. The application of a magnetic force to displace the hyoid bone has been reported to improve UA geometry in a human cadaver model. Therefore, this study aimed to develop a novel magnetic device for improving UA geometry and to verify its safety and feasibility in beagle canines. Ten healthy beagle canines were assigned to receive hyoid suspension using a newly designed magnetic device. An improvement in UA geometry was evaluated by laryngeal inspection and X-ray imaging before and after hyoid suspension. The magnitude of the magnetic force and the distance between the internal and external magnets were measured before and after the improvement in UA geometry. The barking and swallowing functions of all dogs were also observed 1 week after surgery. The procedure was successful, and all dogs survived after surgery. UA geometry significantly improved after hyoid suspension using this magnetic device in all canines. The distance between the hyoid bone and the cervical vertebrae significantly increased after hyoid suspension. The distance between the internal magnet and external magnet was 2.5 ± 0.2 cm, while the magnetic force between the two magnets was 3.5 ± 0.4 N when UA geometry had improved. The barking and swallowing functions of all canines did not change after surgery. This newly designed magnetic device is reliable and effective in improving UA geometry in beagle dogs.
Similar content being viewed by others

Introduction
Obstructive sleep apnea (OSA) is an increasingly prevalent respiratory disorder characterized by recurrent upper airway (UA) collapse during sleep, which can lead to repetitive episodes of hypoventilation and breathing interruption1,2. Untreated OSA causes daytime sleepiness and increases the risk of disorders, such as hypertension, cardiovascular events, incident diabetes, cognitive impairment, and even cancer3,4,5,6. Currently, continuous positive airway pressure is the first-line therapy for mild OSA associated with comorbidities or cardiovascular risk factors, and for moderate or severe OSA7. Unfortunately, poor compliance owing to side effects, including poor mask fit, nasal congestion, and airway drying, remains a concern8,9,10. Surgical therapy can be considered if the patient does not achieve success with other therapies; however, these surgical procedures, including pharyngeal muscle suspension suturing, uvulopalatopharyngoplasty, and maxillomandibular advancement, alter the airway structure during non-sleep periods, leading to an increased incidence of postoperative speech and swallowing dysfunctions11. Surgical hyoid repositioning has been demonstrated to enhance pharyngeal airflow dynamics through strategic anatomical realignment12,13. Moreover, biomechanical studies indicate that the resultant modifications in pharyngeal collapsibility are critically influenced by both the directional orientation and extent of anatomical adjustment14. Previous study utilizing human cadaveric models have demonstrated that magnetically induced anterior traction of the hyoid bone significantly enhances pharyngeal lumen dimensions and optimizes airflow dynamics15. However, unfortunately, no device is currently available for hyoid suspension in the improvement of UA geometry using magnetic force. Therefore, this study aimed to develop a novel magnetic device for hyoid suspensions and to verify its safety and effectiveness in beagle canines.
Results
After the experiment, all dogs were allowed to recover from anesthesia and resume normal feeding. The dogs received intravenous injections of 1.0 mg/kg flurbiprofen axetil (Beijing Taide Pharmaceutical Co., Ltd., Beijing, China) twice daily for 1 week after surgery to relieve pain. The barking and swallowing functions of all dogs were also observed at 1 week after surgery. All surgical procedures were completed successfully, and no complications, such as bleeding, infection, hoarseness, or coughing while drinking, were observed 1 week after surgery. The epiglottis appeared to be completely closed (or almost completely, > 90% obstruction) before the mutual attraction of the magnets (Fig. 1a, b), whereas it appeared to be almost completely opened after mutual attraction (Fig. 1c, d). In addition, UA geometry significantly improved with the magnetic force generated by the magnets to advance the hyoid, open the airway, and maintain a patent airway in all canines (Fig. 2a, b). The distance between the hyoid bone and the cervical vertebrae was 4.8 ± 0.4 cm before the hyoid suspension, and it increased to 7.0 ± 0.6 cm after the hyoid suspension (P < 0.05, Fig. 2c; Table 1). Besides, the between the anterior and posterior walls of the airway was 1.0 ± 0.1 cm before the hyoid suspension, and it increased to 2.5 ± 0.2 cm after the hyoid suspension (P < 0.05, Table 1). The magnetic force between magnets will significantly increase as the distance decreases (Fig. 3). The distance between the daughter and mother magnets was 2.5 ± 0.2 cm, and the magnetic force between the magnets at this distance was 3.5 ± 0.4 N after hyoid suspension (Fig. 3; Table 1). Postoperative examination following the internal magnet removal revealed no evidence of hyoid bone fractures or peri-hyoid muscular damage.

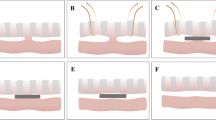
Magnetic hyoid suspension for epiglottic collapse. (a) Magnets position before hyoid suspension. (b) Epiglottic collapse before magnetic hyoid suspension. (c) Magnets position after hyoid suspension. (d) Epiglottic collapse is improved after magnetic hyoid suspension.

Changes in UA geometry after magnetic hyoid suspension. (a) Hyoid bone position and UA geometry before hyoid suspension (white arrow: vertebra; black arrow: hyoid bone; brown arrow: airway; red arrow: ruler; yellow double arrow: Anterior-Posterior airway walls distance; blue double arrow: Hyoid-Cervical distance). (b) Hyoid bone position and UA geometry after hyoid suspension. (c) Changes in distance between hyoid bone and cervical vertebrae before and after hyoid suspension.

(a) Magnetic force curve according to the distance between the mother and daughter ring. (b) Electronic Universal Testing Machine.
Discussion
Hyoid suspension, first described by Riley et al.16, is recommended as a procedure for advancing the hyoid bone to treat airway collapse. In 1993, this procedure was modified by fixing the hyoid bone to the thyroid cartilage but not upward to the chin17. Using this procedure, the posterior airway space and obstruction avoidance can be improved at the tongue base level with anteroinferior movement of the hyoid complex, because the hyoid bone position plays a key role in the pathophysiology of pharyngeal airway obstruction14,18. An isolated hyoid suspension may have a force vector applied either too caudally or rostrally, which is often combined with other operations to improve airway geometry more obviously19. However, the combined procedure increases the complexity of the surgery and the incidence of postoperative complications. A previous proof-of-concept study indicated that a magnetic hyoid suspension could improve UA geometry. Based on this, a novel magnetic device for isolated hyoid suspension with adjustable traction direction and magnitude was developed, and its safety and effectiveness in improving UA geometry were verified in this study. The results indicated that isolated magnetic hyoid suspensions can significantly improve UA geometry.
Compared to traditional surgical techniques for improving UA geometry, this method has the following potential benefits. First, unlike other surgical treatments involving complex procedures for improving UA geometry, the critical step in this procedure is fixing the internal device to the hyoid bone, which is simple and less invasive. Second, this method does not alter the anatomical structure of the neck compared to the traditional hyoid suspension technique. Thus, the laryngeal function during waking is not affected. In fact, the swallowing and barking functions of the canines were not affected after awakening in this study. Third, the direction of the hyoid suspension and the magnitude of the applied force are adjustable and noninvasive after surgery using this method, which may be more effective and desirable for airway opening than other methods. Fourth, previous study has indicated that anterior-based repositioning directions have the greatest impact on change of UA geometry14. In this study, the direction of hyoid suspension is also anterior.
However, several issues must be considered while performing this procedure. The biocompatibility of an internal magnetic device is inevitable because it remains in the body for a long time. The daughter magnet was covered with PEEK, a polyaromatic semi-crystalline thermoplastic polymer with mechanical properties favorable for bio-medical applications20. Therefore, biocompatibility of the internal device was not evaluated in this study. Another important issue is the optimal magnetic force for a hyoid suspension. Too little traction for hyoid suspension will lead to no improvement in UA geometry, whereas excessive traction may lead to other adverse events. The magnetic force that can improve UA geometry was found to be 3.5–3.9 N in this study; it can be adjusted by changing the distance between magnets to get the optimal magnetic force for hyoid suspension when this technique is applied in different individuals.
This study has some limitations. First, the device was only suitable for improving UA geometry during supine sleep. Future research is needed to develop devices for other sleeping positions. In fact, in humans, UA collapse has been observed to be twice as high when sleeping on the back than when sleeping on the side21. Second, this study successfully established the feasibility of magnetic hyoid suspension in beagle canines; however, additional experiments with long-term follow-up are required to further evaluate and verify its effectiveness in improving UA geometry before human clinical trials can commence. Third, when translating this magnet-based hyoid repositioning system to clinical applications, the potential interaction between the external magnet and surrounding ferromagnetic materials requires careful consideration and warrants further investigation to ensure operational safety.
In conclusion, magnetic hyoid suspension is safe and reliable for treating UA geometry in beagle canines.
Methods
Animals
Ten healthy beagle canines (six males and four females; aged 2–4 years; weight: 10–12 kg) were designated as the experimental group. Based on established anatomical studies of canine laryngeal morphology, we intentionally included both male and female Beagles in our experimental design because comprehensive anatomical analyses have demonstrated negligible sexual dimorphism in laryngeal structures between male and female Beagles. This study employed a before-and-after self-controlled design for each canine, eliminating the need for a separate control group. All canines were acclimatized to laboratory conditions (25 °C, 12 h light/12 h dark cycle, 60% humidity, adequate food and water) for 1 week prior to the commencement of the experiments. All dogs were anesthetized using a 3% pentobarbital sodium solution administered intravenously at 1 ml/kg and then placed in the supine position. The animals were provided by the Laboratory Animal Center at the Xi’an Jiaotong University School of Medicine, and this study was approved by the Ethics Committee of the Animal Experiments of Xi’an Jiaotong University (XJTUAE2024-613). All experiments complied with the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines and were performed in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Publications No. 8023, revised 1978).
Magnetic device
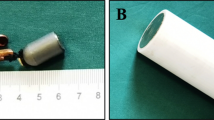
The magnetic devices consist of two components: an internal device (Fig. 4) and an external device (Fig. 5). The internal device was composed of a daughter magnet and a cylindrical shell with two ears. The daughter magnet was made of sintered neodymium-ferrum-boron materials (Ti-NdFeB) with diameter of 12–15 mm and thickness of 4–5 mm (Fig. 4a, b). There are four specifications of daughter magnets used in this study (15/5, 12/5, 15/4, and 12/4). The cylindrical shell was made of polyetheretherketone (PEEK) generated by 3D printing, and its size was determined by the magnet it was wrapped around (Fig. 4c). The external device was composed of a lifting table and a mother magnet. The lift table was made of polylactic acid generated by 3D printing, and its platform height was adjusted during the application process (Fig. 5a). The cylindrical mother magnet was also made of Ti-NdFeB with a diameter of 50 mm and thickness of 30 mm (Fig. 5b, c).

Internal device. (a) Lateral view of the daughter magnet. (b) Frontal view of the daughter magnet. (c) The cylindrical shell with two ears.

External device. (a) The lift table. (b) Frontal view of the mother magnet. (c) Lateral view of the mother magnet.
Surgical procedure
The hyoid body was palpated and identified in the anterior neck region and surface markings were made on the skin for surgical reference after anesthesia. A vertical incision approximately 6 cm long was made at the marked location, cutting through the skin and subcutaneous fat to reveal the sternocleidomastoid muscle underneath. The incision was extended to expose both the upper and lower groups of the hyoid muscles around the neck area, eventually exposing the hyoid bone. After the hyoid bone was exposed, an internal device matching the size of the hyoid bone was selected for implantation. The internal device was secured with nonabsorbable sutures, and the incision was closed using no. 4 silk thread (Fig. 6). Next, an external device was placed above the internal magnet. The daughter and mother magnets attract each other to pull on the hyoid bone as the distance between the two magnets is gradually shortened, and the suspension direction of the hyoid bone is anterior (Fig. 7). The head/neck angle of the dogs was controlled in our study, and all dogs had their heads tilted back during the experiment. The distance between the daughter and mother magnets was measured before and after UA geometry improvement (Fig. 2a, b).

Magnetic device in use for hyoid suspension. (a) External device in use. (b) Internal device after implantation.

schematic diagram of the hyoid suspension using magnetic device.
Magnetic force measurement
To clarify the magnitude of the magnetic attraction for improving airway geometry, the magnetic forces between the daughter and mother magnets were quantitatively assessed using an Electronic Universal Testing Machine (Fig. 3, UTM 6202; Shenzhen Suns Technology Stock Co., Ltd., Shenzhen, China). The mother parent magnet was positioned at the lower part of the setup, whereas the daughter magnet was placed directly above it. The distance between the two magnets was decreased progressively from 10 cm during the measurement process. Consequently, the daughter magnet was gradually lowered from a starting point 10 cm above the external parent magnet, and the magnetic forces were continuously measured during this descent. This method was applied uniformly across four daughter magnets of different sizes to determine the magnetic force relative to the distance. Only one run was conducted per magnetic force intervention, and the data was presented in Table 1. The data obtained from these measurements were used to plot four magnetic force-distance curves (Fig. 3).
Evaluation of UA improvement
UA improvement was evaluated based on changes in epiglottis collapse, hyoid bone position, and UA geometry. Epiglottis collapse was evaluated by direct laryngeal inspection, and the hyoid bone position and UA geometry were determined by radiography in all canines. Changes in UA geometry was evaluated by the distance changes between the anterior and posterior walls of the airway in the same vertebral plane. Changes in the distance between the hyoid bone and the cervical vertebrae were also measured.
Postoperative treatment
Following the surgical intervention, the internal magnet was aseptically explanted through the original incision. A comprehensive intraoperative assessment was performed to evaluate potential iatrogenic trauma, including hyoid bone integrity and peri-hyoid musculature status. The incision was meticulously closed in layers using interrupted 2 − 0 non-absorbable silk sutures (Ethicon®, Somerville, NJ, USA). Postoperative analgesia was maintained via intraperitoneal administration of buprenorphine hydrochloride (0.05 mg/kg body weight) at 12-hour intervals for 72 h, following established veterinary pain management protocols.
Statistical analysis
Quantitative data were expressed as mean ± standard deviation. Differences were assessed using a two-sample paired t-test and were considered statistically significant at P < 0.05. All statistical analyses were performed using IBM SPSS Statistics version 29.0 (IBM, Chicago, IL, USA).
Data availability
The original data can be obtained from the corresponding author by email.
References
Landry, S. A. et al. A review of supine position related obstructive sleep apnea: classification, epidemiology, pathogenesis and treatment. Sleep. Med. Rev. 72, 101847. https://doi.org/10.1016/j.smrv.2023.101847 (2023).
Hartfield, P. J. et al. Anatomical determinants of upper airway collapsibility in obstructive sleep apnea: A systematic review and meta-analysis. Sleep. Med. Rev. 68, 101741. https://doi.org/10.1016/j.smrv.2022.101741 (2023).
Vazir, A. & Kapelios, C. J. Sleep-disordered breathing and cardiovascular disease: who and why to test and how to intervene? Heart 109, 1864–1870 (2023). https://doi.org/10.1136/heartjnl-2019-316375
Olaithe, M., Bucks, R. S., Hillman, D. R. & Eastwood, P. R. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep. Med. Rev. 38, 39–49. https://doi.org/10.1016/j.smrv.2017.03.005 (2018).
Reutrakul, S. & Mokhlesi, B. Obstructive sleep apnea and diabetes: A state of the Art review. Chest 152, 1070–1086. https://doi.org/10.1016/j.chest.2017.05.009 (2017).
Kendzerska, T. et al. Obstructive sleep apnea and incident cancer: A large retrospective multicenter clinical cohort study. Cancer Epidemiol. Biomarkers Prev. 30, 295–304. https://doi.org/10.1158/1055-9965.Epi-20-0975 (2021).
Gottlieb, D. J. & Punjabi, N. M. Diagnosis and management of obstructive sleep apnea: A review. Jama 323, 1389–1400. https://doi.org/10.1001/jama.2020.3514 (2020).
Patel, S. R. Obstructive Sleep Apnea. Ann Intern Med 171, Itc81-itc96 (2019). https://doi.org/10.7326/aitc201912030
Sánchez-de-la-Torre, M. et al. Adherence to CPAP treatment and the risk of recurrent cardiovascular events: A Meta-Analysis. Jama 330, 1255–1265. https://doi.org/10.1001/jama.2023.17465 (2023).
Delijaj, F. et al. Effects of telemonitoring follow-up, side effects, and other factors on CPAP adherence. J. Clin. Sleep. Med. 19, 1785–1795. https://doi.org/10.5664/jcsm.10686 (2023).
Dicus Brookes, C. C. & Boyd, S. B. Controversies in obstructive sleep apnea surgery. Sleep. Med. Clin. 13, 559–569. https://doi.org/10.1016/j.jsmc.2018.07.005 (2018).
Baisch, A., Maurer, J. T. & Hörmann, K. The effect of hyoid suspension in a multilevel surgery concept for obstructive sleep apnea. Otolaryngol. Head Neck Surg. 134, 856–861. https://doi.org/10.1016/j.otohns.2006.01.015 (2006).
Salman, D. & Amatoury, J. Influence of natural hyoid bone position and surgical repositioning on upper airway patency: a computational finite element modeling study. J. Appl. Physiol. (1985). 137, 1614–1631. https://doi.org/10.1152/japplphysiol.00657.2024 (2024).
Samaha, C. J., Tannous, H. J., Salman, D., Ghafari, J. G. & Amatoury, J. Role of surgical hyoid bone repositioning in modifying upper airway collapsibility. Front. Physiol. 13, 1089606. https://doi.org/10.3389/fphys.2022.1089606 (2022).
Rosenbluth, K. H., Kwiat, D. A., Harrison, M. R. & Kezirian, E. J. Hyoid bone advancement for improving airway patency: cadaver study of a magnet-based system. Otolaryngol. Head Neck Surg. 146, 491–496. https://doi.org/10.1177/0194599811429522 (2012).
Riley, R. W., Powell, N. B. & Guilleminault, C. Inferior sagittal osteotomy of the mandible with hyoid myotomy-suspension: a new procedure for obstructive sleep apnea. Otolaryngol. Head Neck Surg. 94, 589–593. https://doi.org/10.1177/019459988609400510 (1986).
Riley, R. W., Powell, N. B. & Guilleminault, C. Obstructive sleep apnea syndrome: a surgical protocol for dynamic upper airway reconstruction. J Oral Maxillofac Surg 51, 742–747; discussion 748–749 (1993). https://doi.org/10.1016/s0278-2391(10)80412-4
Jo, J. H., Park, J. W., Jang, J. H. & Chung, J. W. Hyoid bone position as an indicator of severe obstructive sleep apnea. BMC Pulm Med. 22, 349. https://doi.org/10.1186/s12890-022-02146-0 (2022).
Kezirian, E. J. & Goldberg, A. N. Hypopharyngeal surgery in obstructive sleep apnea: an evidence-based medicine review. Arch. Otolaryngol. Head Neck Surg. 132, 206–213. https://doi.org/10.1001/archotol.132.2.206 (2006).
Panayotov, I. V., Orti, V., Cuisinier, F. & Yachouh, J. Polyetheretherketone (PEEK) for medical applications. J. Mater. Sci. Mater. Med. 27, 118. https://doi.org/10.1007/s10856-016-5731-4 (2016).
Srijithesh, P. R., Aghoram, R., Goel, A. & Dhanya, J. Positional therapy for obstructive sleep Apnoea. Cochrane Database Syst. Rev. 5, Cd010990. https://doi.org/10.1002/14651858.CD010990.pub2 (2019).
Author information
Authors and Affiliations
Contributions
Lu Q., Yao Z.W., and Lv Y. designed the study; Yao Z.W., Nadiya N., Li P.X., Qi X.Y., Wang R.Z., Zhang J.H., Xiang L.B., Shi A.H., and Ren L. performed the research and acquired the data; Lu Q. and Yu J.W. analyzed the data; Lu Q. and Yao Z.W. drafted the manuscript; Wu R.Q., Zhang L., Yao Y.M. and Lv Y. contributed significantly to the revision of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yao, ZW., Nuerbolati, N., Li, PX. et al. A novel method for hyoid suspension using a magnetic device in beagles: A preliminary study. Sci Rep 15, 21611 (2025). https://doi.org/10.1038/s41598-025-09193-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09193-7
