
Abstract
Exposure to occupational noise has emerged as a major health issue worldwide. To better evaluate changes in the health impacts of occupational noise exposure from 1990 to 2021, this study conducted stratified analyses of spatiotemporal variations across regions, genders, age, and sociodemographic index (SDI) levels. Results indicate that low-income and rapidly industrializing countries bear higher burdens of occupational noise-related diseases. Males and middle-aged to elderly populations are the primary high-risk groups for occupational noise exposure, with a particularly notable increase in the burden among those aged 45–74. Disability-adjusted life years (DALYs) significantly decreased with increasing SDI, while estimated annual percentage change (EAPC) showed significant positive correlations with both DALYs (R = 0.3) and SDI (R = 0.4). Regions with an SDI of 0.4–0.6 experienced the most pronounced EAPC growth. By 2035, DALYs rates are projected to decrease to 125.0 ± 1.9 per 100,000, although the burden for individuals aged 65 and above is expected to increase significantly. Population growth and aging were identified as key drivers of DALYs increases, contributing 68.2% and 20.9%, respectively. From 1990 to 2021, the slope inequality index changed from − 9.6 to 2.5, and the concentration index curve became smoother. Although health inequality has improved, the disease burden in low-SDI countries remains significantly higher than theoretical minimum levels. This study provides robust support for reducing global occupational noise exposure and its associated health inequalities.
Similar content being viewed by others
Introduction
With the development of society, there has been increasing attention to occupational health1. Hearing impairment resulting from exposure to occupational noise ranks among the most prevalent occupational health and safety concerns2. Prolonged occupational noise exposure also contributes to non-auditory health problems such as sleep disturbances, cardiovascular diseases, and diabetes3,4. It not only disrupts workers’ performance and physical and mental health5,6,7 but also poses challenges to social development. Therefore, understanding the health hazards of occupational noise exposure and formulating targeted and effective mitigation strategies are essential.
In recent years, growing attention has been paid to the detrimental impacts of noise exposure Li et al.7 revealed the association between noise exposure and sleep quality. Hahad et al.8 highlighted that noise exposure has harmful effects on brain function. In a comprehensive review, Thompson et al.9 examined the cognitive impacts of noise and identified a clear linear relationship between prolonged noise exposure and cognitive decline, particularly among middle-aged and elderly populations. Peris et al.10 reviewed 76 studies and found that noise exposure has substantial impacts on various health outcomes, including annoyance and endocrine disruption. Occupational noise, in particular, not only directly contributes to hearing loss but also affects work efficiency, operational safety, and overall health. To enhance public health and occupational safety, understanding the global patterns and determinants of the disease burden linked to occupational noise exposure is crucial for developing evidence-based public health interventions at the international level.
Occupational noise exposure is a widespread challenge globally11. Kerns et al.12 reported that 25.0% of U.S. workers experienced occupational noise exposure in 2014. Similarly, according to Thirion et al.13, in 2015, 28.0% of European workers were exposed to high levels of noise for at least 25.0% of their working time. Noise causes mechanical damage to the cochlear structures, particularly the hair cells on the basilar membrane, disrupting cochlear fluid dynamics11. Noise-induced hearing loss (NIHL) impairs both peripheral auditory function and central auditory processing mechanisms14. Dzhambov et al.15 reviewed evidence that occupational noise exposure increases adverse pregnancy outcomes among women. They also found in a meta-analysis that it raises the risk of workplace injuries16. Concha-Barrientos et al.11 emphasized the harmful impacts of occupational noise exposure on work performance, immune function, and body weight. Teixeira et al.17 found an increased prevalence of cardiovascular diseases linked to occupational noise exposure, especially above 85 dBA. While the neurobiological mechanisms linking noise exposure to various auditory and extra-auditory health effects have been widely examined14,18,19, comparatively little attention has been paid to the evolving patterns of health burdens attributable to such exposure over time.
Khoza-Shangase et al.6 highlighted the critical role of early hearing care by reviewing evidence linking occupational noise-induced hearing loss with HIV/AIDS. Guo et al.20 and Wu et al.21 investigated the health impacts of occupational noise exposure in the U.S., reporting its significant association with increased prevalence of cardiovascular disease and arthritis, respectively. While studies like that of Wang et al.22 provide important insights into country-specific burdens, a systematic investigation into how occupational noise-related disease burdens vary with Socio-demographic Index (SDI) across different developmental contexts remains insufficient. The evolving inequality of occupational noise burden across countries at different development stages has not yet been quantitatively assessed. Moreover, few studies have conducted comprehensive stratified analyses by sex, age, and region using multidimensional spatiotemporal data, limiting the identification of vulnerable subpopulations. Although Liu et al.23 assessed the occupational noise-related disease burden from 1990 to 2019 and explored the influence of sex, age, and SDI on age-standardized disability-adjusted life year (DALY) rates, their study did not delve into global health inequalities or project future trends in disease burden. The health hazards of occupational noise exposure are widespread and persistent, with significant impacts in developing and rapidly industrializing countries24. However, research has predominantly focused on developed regions like the United States25,26. Moreover, occupational noise exposure is influenced by socioeconomic factors like economic level and region, as well as population characteristics like age and gender27. Existing studies often target specific populations or diseases, with limited systematic stratification analyses across age and gender. Although the health risks associated with occupational noise have been widely discussed, there remains a lack of comprehensive, long-term analyses at the global level, particularly concerning disparities across populations and regions. To bridge the existing research gaps, this study investigates the dynamic trends in health inequalities associated with occupational noise exposure and examines the structural and contextual determinants underlying these disparities.
Against this backdrop, this study uses global burden of disease (GBD) data from 1990 to 2021 to systematically analyze the spatiotemporal distribution characteristics of occupational noise-related DALYs, examine their relationship with SDI, and predict future trends using average annual percentage change (AAPC) and Bayesian age-period-cohort models (BAPC). Furthermore, the study incorporates health inequality indices (SII and CI) to quantify disparities in occupational noise-related disease burdens across SDI levels. Through decomposition analysis, the contributions of population growth, aging, and epidemiological changes to DALYs are also elucidated. This research aims to provide data support for scientifically informed interventions addressing occupational noise-related health burdens and theoretical foundations for advancing global occupational health management and health equity.
Methods
GBD 2021
The GBD study employs a systematic modeling framework to integrate health data from diverse countries and sources, including vital registration systems, surveys, and hospital records28. Mortality data are estimated using the Cause of Death Ensemble model, which incorporates a variety of statistical models and automatically selects the optimal ensemble for each cause. DisMod-MR 2.1, a Bayesian meta-regression framework, is used to model non-fatal health outcomes by harmonizing data from heterogeneous sources and maintaining internal consistency across estimates29. All outputs are standardized by cause, age group, and geographical region to ensure comparability across settings. Uncertainty is quantified using posterior distributions derived from 1,000 Bayesian draws, with all estimates reported as 95% uncertainty intervals (UI).
DALYs quantify overall disease burden by summing years of life lost due to premature death (YLLs) and years lived with disability (YLDs). YLLs are computed using the number of deaths and the corresponding standard life expectancy, whereas YLDs are calculated by multiplying the prevalence of each health condition by its assigned disability weight30. The specific formula is as follows:
GBD 2021 database covers information on 369 diseases/injuries and 88 risk factors across 204 countries and regions from 1990 to 2021. The data are stratified by age, gender, year, region, and SDI31. SDI is a composite measure derived from income level, educational attainment, and fertility rate, ranging from 0.0 to 1.0, with higher SDI indicating higher development levels32. All countries are categorized into 5 SDI levels: low, low-middle, middle, high-middle, and high33. Based on geographical and epidemiological similarities, the GBD study classifies 204 countries and territories into 21 super-regions (see Fig. 1)34. As this study used open-source data without any identifiable personal information, it complies with ethical norms and moral requirements35.

Map of GBD Regional Classifications.
Occupational noise
The GBD database categorizes diseases into four levels, with the assessment of occupational noise-related disease burdens focusing on ONIHL36. The study population includes individuals aged 15 years and above, as defined by the WHO for the working-age population17. Population exposure levels were determined based on occupational noise exposure data from each country. Quantitative associations between occupational noise exposure and hearing loss have been established through epidemiological investigations. The population attributable fraction (PAF) method (see Eq. 2) was applied to estimate the proportion of ONIHL and calculate the number of cases27,37. Bayesian hierarchical models were employed to estimate disease burdens across different regions, providing 95.0% uncertainty intervals (UI)27. Further methodological details are available in the GBD 2021 report.
Statistics analysis
The age-standardized rates (ASRs) are obtained from the GBD 2021 database (http://ghdx.healthdata.org/gbd-results-tool)38. GBD 2021 uses the GBD World Standard Population, which was established in 2013 based on projected global population data from 2000 to 2025. The population was stratified into 5-year age groups, with predetermined weights assigned to each group to adjust for variations in age structure across populations39.
This study first employed the estimated annual percentage change (EAPC) of ASR DALYs to assess trends in the global diseases burden related to occupational noise exposure40. The calculation of EAPC is shown in Eqs. 3–441. A trend is deemed statistically significant if its 95% UI lies entirely above or below zero—indicating a significant increase or decrease, respectively42. If the interval spans zero, the trend is not considered statistically significant38,43.
Joinpoint regression was utilized to detect statistically significant time points at which the direction or magnitude of temporal trends shifted44. This approach segments the study period into multiple intervals, each characterized by a distinct slope, and fits a separate linear model within each segment39. For each segment, the APC was calculated, and the AAPC was used to reflect the overall trend from 1990 to 2021 (see Eq. 5)45. A Delta transformation was applied to each APC, and the 95% uncertainty intervals were determined using the Monte Carlo Permutation (MCP) test, which also selected the optimal number of joinpoints.
Where, di denotes the duration, and βi represents the slope of the segment.
Furthermore, this study conducted stratified analyses of the burden of occupational noise-related diseases by SDI, gender, and age. The associations between the SDI and DALYs as well as EAPC were quantified using locally weighted regression. UI was derived through 1,000 bootstrap resamples35,46. Using the APC model47, the study calculated net drift (total annual change percentage) and local drift (age-specific changes) based on cross-sectional and age-specific rate estimates, along with Wald tests to assess period and cohort effects48. Future trends of occupational noise-related DALYs were predicted using the BAPC model49. Specifically, the model assumes that DALYs follow a Poisson distribution, with the expected value modeled as a log-linear function of age, period, and cohort effects. To ensure temporal smoothness, second-order random walk priors were assigned to the age, period, and cohort effects50. Additionally, sum-to-zero constraints were imposed on the three effects to address identifiability. The precision parameters of the priors were assigned log-gamma hyperpriors. All model fitting and projections were conducted using the Integrated Nested Laplace Approximation (INLA) method (code available at: https://folk.ntnu.no/andrerie/software.html.)51.
To quantify inequality in DALYs across different SDI levels, the slope index of inequality (SII) and the concentration index (CI) are measured35,52. SII is the absolute difference in DALYs between the highest and lowest SDI countries, calculated through population-weighted regression after sorting by SDI to reduce data heteroscedasticity53. CI evaluates the deviation between the cumulative distribution of DALYs and the cumulative population distribution sorted by SDI using the Lorenz curve38. When health outcomes are evenly distributed across socioeconomic groups, the concentration curve aligns with the 45-degree line of equality. The CI is calculated as twice the area between the concentration curve and this line, capturing the extent of inequality54. A positive CI indicates DALYs are concentrated in high-SDI countries, while a negative CI shows concentration in low-SDI countries55. Finally, to assess the effectiveness of various regions in mitigating the health burden attributable to occupational noise exposure, an efficiency frontier model was developed. This model quantifies both the efficiency gap and the relative efficiency index of each region in comparison to the theoretical optimum. Frontier curves were constructed using different smoothing parameters, and 95% UI were derived from 1,000 bootstrap resamples to ensure the stability and reliability of the results56. p < 0.05 was considered statistically significant. All data processing and analyses were conducted using R software (version 4.2.3) and JD_GBDR (version 2.37, Jingding Medical Technology Co., Ltd.).
Results
Global regional differences
Substantial regional disparities are observed in the global occupational noise-related disease burden (see Fig. 2 and Appendix A). Regions with EAPC < −0.3 include 19 areas, primarily concentrated in developed countries and regions, such as parts of Europe, with the Netherlands recording the lowest EAPC (−0.7). Regions with EAPC between − 0.3 and − 0.1 include 50 areas, while those with EAPC between − 0.1 and 0.0 include 46 areas, and EAPC between 0.0 and 0.1 include 42 areas. These regions are distributed widely, encompassing both developed and certain developing countries. Regions with EAPC > 0.1 include 47 areas, primarily in rapidly industrializing countries and regions such as China, India, and Australia, which are shown in deep red on the map. The Solomon Islands recorded the highest EAPC (1. 1). This highlights that developing regions, such as India and some African countries, are most affected by occupational noise exposure.

Global distribution map of occupational noise-related EAPC.
From 1990 to 2021, the overall DALYs related to occupational noise exposure slightly increased globally (Fig. 3). The most significant growth occurred in East Asia (+ 10.7 per 100,000), followed by Andean Latin America (+ 5.4 per 100,000). Conversely, occupational noise-related DALYs significantly decreased in high-income regions, with the most pronounced reductions observed in North Africa and the Middle East (−5.3 per 100,000), followed by high-income North America (−4.3 per 100,000). Regions such as Western Europe and high-income Asia-Pacific consistently maintained low DALYs.

Occupational noise-related DALYs in different regions in 1990 and 2021.
Gender and age differences
Globally, DALYs related to occupational noise exposure among males are 1.6 times higher than those among females (Fig. 4). Both males and females in regions like Eastern Sub-Saharan Africa, East Asia, and Southeast Asia exhibit high DALYs values, with males significantly surpassing females. The largest gender disparity is observed in South Asia (79.1 per 100,000), followed by North Africa and the Middle East (70.0 per 100,000). Although high-income regions have lower overall burdens, gender differences remain evident.

Occupational noise–related gender differences across regions.
The 50–64 age group contributes the most to the burden of occupational noise-related diseases (Fig. 5). In individuals aged 65 years and above, the burden gradually declines due to reduced labor participation and decreased exposure duration. Among the 15–19 age group, males exhibit 1.5 times the DALYs of females. As age increases, the gender disparity peaks during young and middle adulthood (25–39 years), with males having approximately 1.7 times the DALYs of females, before gradually converging in later years. Overall, males are the primary at-risk population for occupational noise exposure, with middle-aged individuals particularly prone to disease manifestation.

Occupational noise–related gender differences by age groups.
Relationship between EAPC, dalys, and SDI
The ASR DALYs rate for occupational noise-related diseases decreases significantly with increasing SDI (Fig. 6). Eastern Sub-Saharan Africa has the highest DALYs burden (144.2 per 100,000). Despite relatively higher SDI levels, developing regions such as East Asia and Southeast Asia still experience substantial burdens, with DALYs of 126.7 per 100,000 and 120.4 per 100,000, respectively. Regions with SDI > 0.6 show the narrowest distribution, with a trend toward uniformly lower burdens.

Relationship between SDI and DALYs from occupational noise in 21 regions.
As shown in Fig. 7, countries with lower SDI values exhibit higher occupational noise-related DALYs, while those with higher SDI values have lower burdens. Countries like Madagascar and Burundi report high DALYs at 216.8 per 100,000 and 169.3 per 100,000, respectively. In contrast, countries such as Luxembourg, Israel, and Denmark have notably lower DALYs. Interestingly, despite its relatively high SDI, China’s DALYs exceed the expected trend line. Similarly, the Philippines and Vietnam report DALYs significantly above the trend for countries with comparable SDI levels.

Relationship between SDI and DALYs from occupational noise in 204 countries.
A significant positive association between EAPC and DALYs is observed in Fig. 8(a), with a correlation coefficient of R = 0.3 (p < 0.001). In regions with low DALYs (< 50.0 per 100,000), EAPC values are more concentrated and closer to 0.0. In regions with high DALYs (> 100.0 per 100,000), EAPC increases markedly, accompanied by greater variability. Figure 8(b) demonstrates a notable positive correlation between EAPC and SDI (R = 0.4, p < 0.001). In countries with SDI < 0.3, EAPC values are highly dispersed, with some countries showing negative EAPC. At SDI levels of 0.4–0.6, EAPC peaks. For countries with SDI > 0.7, EAPC stabilizes or slightly declines.

Relationship among (a) EAPC and DALYs, (b) EAPC and SDI (Each dot represents a country, the curve denotes the fitted regression trend, and the shaded area indicates the 95% UI. Larger circles indicate higher values.).
AAPC and BAPC analysis
As shown in Fig. S1, occupational noise-related DALYs experienced rapid annual changes between 1990 and 1995, with an AAPC of 4.7 × 10−1 (95% UI: 4.2 × 10−1, 5.1 × 10−1). From 1995 to 2005, the growth rate slowed significantly (AAPC = 2.8 × 10−1, 95% UI: 2.5 × 10−1, 3.0 × 10−1). Between 2005 and 2010, the trend stabilized, with an AAPC of only 6.3 × 10−2 (95% UI: 9.0 × 10−3, 1.2 × 10−1). From 2010 to 2021, the burden of occupational noise-related diseases continued to increase, with an AAPC of 2.3 × 10−1 (95% UI: 2.2 × 10−1, 2.5 × 10−1).
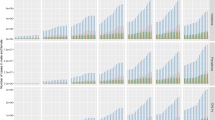
Predictions indicate that the ASR DALYs will exhibit a slight downward trend (Fig. S2), declining from 127.7 ± 0.05 per 100,000 in 2021 to 125.0 ± 1.9 per 100,000 by 2035. Among different age groups, the burden for individuals aged 15–34 (young adults) is expected to continue its declining trend through 2035 (Fig. 9). For those aged 35–64 (middle-aged adults), occupational noise-related DALYs have remained stable or shown slight fluctuations in the last three decades., with a potential slight increase in the future. For individuals aged 65 and above (older adults), DALYs have risen substantially in the last three decades, with this upward trend expected to persist. In summary, while the burden among individuals aged 15–34 is expected to decrease significantly, the burden for those aged 45 and above, particularly older adults (65+), is likely to increase further. Although a slight overall decline in DALYs is anticipated, health interventions for high-risk regions and populations remain critical and should not be neglected.

Future changes in DALYs due to occupational noise exposure by age group.
Decomposition analysis
As shown in Fig. 10, the global increase in occupational noise-related DALYs is primarily driven by population changes (green), which are estimated to contribute 68.2% of the total growth. Population aging (red) is another significant factor, accounting for 20.9%, particularly in high-income countries and middle-SDI regions, where it contributes approximately 45.0–50.0%. The minimal effect of epidemiological changes on DALYs suggests that limited effectiveness has been achieved in mitigating disease burdens through occupational health management. Overall, high-income regions are more influenced by population growth, while population growth has a more substantial impact on low- and middle-income regions.

Decomposition of changes in occupational noise-related DALYs.
APC analysis
As shown in Fig. 11(a), DALYs rates increase with age, peaking at approximately 74 years before rapidly declining. The trend shapes are consistent across time periods, with slightly higher DALYs observed at peak ages in 2017–2021 compared to earlier periods. Figure 11(b) shows that DALYs are notably higher in the 45–74 age group. Within each birth cohort, DALYs generally increase with age, and among individuals aged 60 and above, differences between birth cohorts become more pronounced. Overall, the 45–74 age group represents a critical period of rapid DALYs growth, with later birth cohorts in older age groups (particularly the very old) showing an upward trend in DALYs.

Analysis of age and cohort effects related to occupational noise.
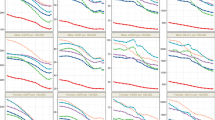
Figure 12(a) indicates a net drift of 0.3% per year, suggesting a slow overall increase in occupational noise-related DALYs. The drift rate is negative for individuals aged 15–30, while significant positive drift is observed for those aged 45–74. As shown in Fig. 12(b), DALYs rise with age, peaking around 74 years and then declining. Figure 12(c) illustrates a gradual increase in period effects, with rate ratios rising from 1.0 to 1.1, indicating a significant increase in recent time periods compared to 1995. Figure 12(d) shows that rate ratios increased steadily between 1900 and 1970 (0.8–1.1), suggesting higher disease burdens among earlier birth cohorts. After 1970, rate ratios declined, reflecting the positive impact of improved occupational health management on later-born cohorts. In summary, middle-aged and older adults, as well as cohorts born in the mid-20th century, experienced higher occupational noise exposure risks.

APC analysis of occupational noise-related DALYs. (a) Net drifts (b) Age effects; (c) Period effects; (d) Cohort effects.
Analysis of global health inequality
From 1990 to 2021, global inequality in occupational noise-related DALYs decreased significantly (Fig. 13). In 1990, DALYs rates showed a declining trend with increasing SDI, with an SII of −9.6 (95% UI: −18.4, −0.9), indicating that lower-SDI countries bore a higher burden. By 2021, this trend shifted, with DALYs rates increasing significantly in higher-SDI countries, resulting in an SII of 2.5 (95% UI: −9.2, 14.3), suggesting a gradual global rebalancing of burdens.

Changes of SII in DALYs attributable to occupational noise, 1990–2021.
As shown in Fig. 14, the 1990 curve deviated significantly from the 45-degree equity line, indicating that occupational noise-related DALYs were more concentrated in low-SDI countries, with a CI of 0.3 (95% UI: 0.01, 0.7). Low-SDI countries contributed the majority of the disease burden. By 2021, the curve moved closer to the equity line, reflecting reduced inequality. The CI remained 0.3 (95% UI: 0.02, 0.7), indicating minimal change in overall concentration compared to 1990, but the smoother curve suggests a reduction in extreme disparities. While the distribution trends have become more balanced, the overall concentration of the burden has not changed significantly.

Changes of CI in DALYs attributable to occupational noise, 1990–2021.
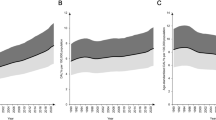
The frontier line provides a theoretical minimum DALYs benchmark for different SDI levels. As shown in Fig. 15(a), DALYs decline with increasing SDI along the frontier line. Countries with SDI ≤ 0.6 generally exhibit higher DALYs, with most data points lying above the frontier, indicating severe burdens from occupational noise-related diseases. For countries with SDI > 0.6, the frontier levels off, and data points gradually approach the line. As shown in Fig. 15(b), countries such as Somalia and Niger are far above the frontier line, indicating significant gaps from the theoretical minimum levels. In contrast, countries like Japan and the United States have DALYs levels that are already very close to the frontier minimum, while countries like China and Thailand have shown progress in aligning with the frontier in recent years. In summary, the frontier line decreases with increasing SDI, but many countries still deviate significantly, with DALYs remaining at high levels and continuing to rise in some cases. Reducing global health inequality remains a critical focus for further efforts.

Frontier analysis of occupational noise–related DALYs in relation to SDI. (a) Spatiotemporal distribution of DALY rates and SDI, with the frontier curve representing the theoretical minimum burden; (b) Comparison of DALY rates and SDI in 2021, showing deviation from the frontier and trends in disease burden across countries.
Discussion
Global spatiotemporal differences
This study revealed significant regional disparities in occupational noise-related DALYs. Among the 19 countries with EAPC < −0.3, most are developed nations, with the Netherlands having the lowest EAPC (−0.7). Conversely, countries with EAPC > 0.1 are concentrated in rapidly industrializing regions, including China, India, and Australia. The Solomon Islands recorded the highest EAPC (1.1). More advanced occupational health policies, industrial technologies, and noise control measures have been implemented in developed countries, resulting in a decreased burden of occupational noise-related diseases2. In contrast, developing countries may overlook the hazards of noise exposure during rapid industrialization and urbanization1, consistent with findings by Liu et al.23. Moving forward, improving workplace environments by implementing noise control regulations and strengthening occupational health management systems will be critical, particularly for industrializing countries with labor-intensive industries.
From 1990 to 2021, the overall level of occupational noise-related DALYs slightly increased. East Asia (+ 10.7 per 100,000) and Andean Latin America (+ 5.4 per 100,000) showed the most significant growth, while North Africa and the Middle East (−5.3 per 100,000) and high-income North America (−4.3 per 100,000) exhibited substantial declines. These trends reflect the success of occupational health management in high-income countries, where noise monitoring and standardized controls have led to notable improvements25. For example, since the mid-20th century, Europe and high-income North America have implemented stringent legal controls on occupational noise, with the European Union enforcing strict workplace noise limits17. In North Africa and the Middle East, economic transitions have reduced industries with high noise exposure. Conversely, rapid industrialization in East Asia has increased occupational noise exposure. The burden of occupational noise-related diseases in rapidly industrializing nations must be addressed urgently. Health risks, physical discomfort, and long-term health damage can be significantly reduced through the implementation of effective interventions, such as the use of low-noise equipment, the installation of soundproofing and noise-dampening devices, and the promotion of hearing protection devices (HPD)57. Establishing on-site noise monitoring systems to identify and prioritize high-risk noise areas is also essential. Future efforts should focus on optimizing industrial noise prevention technologies and developing adaptive occupational health intervention systems tailored to regional needs.
Although the trends in EAPC for certain countries did not reach statistical significance (i.e., the 95% UI includes zero), these findings are not without interpretive value. For instance, Central Asia (0.0, 95% UI: − 0.009 to 0.01) exhibited a largely stable burden over the study period. This stability may be attributed to the relatively slow pace of industrial development following the dissolution of the Soviet Union, as well as the continued reliance on outdated occupational disease surveillance systems and limited enforcement capacity. In contrast, Tropical Latin America (–0.06, 95% UI: − 0.1 to 0.03) showed a downward trend that did not achieve statistical significance. In this region, certain countries have implemented workplace exposure intervention strategies, which may have contributed to a gradual but unstable reduction in disease burden. These examples highlight the importance of interpreting non-significant trends in the context of regional development, policy implementation, and data quality, as they may still reveal meaningful patterns and potential areas for targeted public health interventions.
Population differences
Globally, occupational noise-related DALYs are significantly higher in males than females, particularly in regions such as Eastern Sub-Saharan Africa, East Asia, and Southeast Asia. South Asia exhibits the largest gender disparity (79.1 per 100,000), likely due to differences in occupational distribution. Males are more commonly employed in high-noise occupations, such as heavy industry and construction24. Occupational health interventions have historically paid little attention to gender differences, but addressing this gap is critical for improving the efficiency of occupational noise prevention, especially in high-risk professions. Among the 15–19 age group, the burden for males is 1.5 times that for females, with the gender disparity peaking in the 25–39 age group (males experiencing 1.7 times the burden of females). In the future, targeted occupational protection and noise monitoring for young and middle-aged male workers should be prioritized, with early health interventions to mitigate risks. Raising public awareness of occupational noise hazards and enhancing workers’ self-protection capabilities are key strategies.
The 50–64 age group contributes most to the burden of occupational noise-related diseases, with the 45–74 age range identified as a critical period for rapidly increasing DALYs. Middle-aged and older groups, as well as cohorts born during periods of industrial expansion, face higher risks of occupational noise exposure23. This may be due to the cumulative impact of prolonged noise exposure, including NIHL and cardiovascular diseases58. Noise exposure has been shown to activate both the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic–adrenal–medullary (SAM) system59, triggering chronic stress responses characterized by elevated levels of stress-related hormones such as cortisol. This cascade can lead to a range of physiological effects, including increased blood pressure, fluctuations in blood glucose levels, and elevated heart rate, thereby heightening the risk of cardiovascular diseases4. In addition, noise exposure induces oxidative stress and endothelial dysfunction, promotes the expression of pro-inflammatory cytokines and adhesion molecules, and facilitates vasoconstriction and the development of atherosclerosis. Chronic noise stimulation also disrupts autonomic nervous system balance, impairing regulatory functions between the brain and cardiovascular system60. Moreover, noise can interfere with melatonin secretion, disturbing circadian rhythms and sleep architecture, which in turn may result in sleep disorders, fatigue, and cognitive decline9. Neuroimaging studies have suggested that noise exposure may impair the functional connectivity between the limbic system and prefrontal cortex, negatively impacting emotional regulation and cognitive control8. A significant linear relationship between sound pressure levels and the risk of hypertension has been reported in several studies, with higher noise levels being associated with an increased likelihood of developing hypertension61. A dose–response relationship between cumulative occupational noise exposure and the incidence of hypertension among workers was also identified by Li et al.62. In China, the prevalence of hypertension was found to double among workers exposed to occupational noise for more than five years and to increase by more than fourfold with exposure durations exceeding fifteen years63. Older individuals are more susceptible to these conditions due to reduced metabolic and recovery capacities, which contribute to a heavier disease burden4,64. Additionally, cohorts born during periods of rapid industrial development often experienced higher noise levels and limited occupational protection, resulting in greater cumulative noise exposure. As individuals age, the degeneration of the auditory system, combined with cumulative noise-related damage, exacerbates health burdens. For individuals aged 45 and above, it is crucial to enhance screening and management of noise-related chronic diseases. To improve the accessibility of medical services, appropriate subsidies and healthcare support should be provided. Establishing long-term health records for high-risk populations to track the impacts of noise exposure and offering customized healthcare services are essential strategies for mitigating occupational noise-related health burdens.
Current and future state of health inequalities
Occupational noise-related DALYs significantly decrease with increasing SDI, with lower-SDI countries experiencing a notably higher burden. A strong positive correlation between EAPC and DALYs was observed (R = 0.3, p < 0.001), highlighting the urgency for health interventions in high-burden countries. At an SDI range of 0.4–0.6, EAPC peaks, emphasizing the severe burden in developing countries.
This study revealed that countries with relatively high SDI levels—such as China, the Philippines, and Vietnam—exhibited a higher-than-expected burden of occupational noise-related DALYs. This phenomenon may be attributed to factors including industrial structure, occupational safety policies, and enforcement capacity. First, during the course of rapid industrialization, these countries have developed labor-intensive economies dominated by high-noise exposure industries, drawing large segments of the workforce into potentially hazardous environments. Moreover, the increasing labor force participation rate and accelerating population aging have extended the duration of noise exposure among middle-aged and older workers, thereby exacerbating disease burden. Second, despite notable improvements in SDI, substantial gaps remain in legislation related to occupational health, disease recognition, and workers’ compensation systems. Third, the health risks of noise exposure are still not widely recognized by the public, while poor working conditions and inadequate protective measures persist. Many workers lack sufficient knowledge of the chronic health effects of noise and fail to consistently use hearing protection devices18,19,20. At the same time, some enterprises, driven by cost-saving considerations, neglect to implement required noise control standards, leading to persistent hidden exposure risks. This reflects a mismatch between economic development speed and the capacity of occupational health governance. When formulating occupational health strategies, it is insufficient to rely solely on economic indicators; a multidimensional assessment of industrial structure, regulatory systems, and enforcement capability is required11,17. For instance, establishing noise surveillance systems that comprehensively cover small and medium-sized enterprises, mandating hearing protection standards for high-risk industries, and strengthening regulatory enforcement are all essential to ensuring effective implementation of noise mitigation measures. In China, the Occupational Disease Prevention and Control Law (enacted in 2002) explicitly recognized noise as a hazardous occupational factor, which subsequently led to greater attention to occupational noise exposure. With the implementation of these policies, workplace noise regulation has become more standardized, workers’ safety awareness has improved significantly, and the use of personal HPD has increased, contributing to a marked reduction in the burden of noise-induced hearing loss22. Although these countries still experience high occupational noise burdens, signs of improvement have emerged. Their experiences offer valuable lessons for other nations at similar developmental stages. In the future, economic development must be paralleled by the strengthening of occupational health systems. This includes enhancing surveillance, early warning, and intervention mechanisms for noise exposure to promote equity and sustainability in global occupational health.
Although the growth of global occupational noise-related DALYs has slowed compared to the initial stages, the burden increased more rapidly during 2010–2021 (AAPC: 2.3 × 10−1, 95% UI: 2.2 × 10−1, 2.5 × 10−1) than during 2005–2010 (AAPC: 6.3 × 10−2, 95% UI: 9.0 × 10−3, 1.2 × 10−1). While projections indicate a decline to 125.0 ± 1.9 per 100,000 by 2035, the burden for individuals aged 45 and above, especially those 65 and older, may continue to rise. Targeted health interventions for high-risk regions and populations remain critical. Population growth and aging are key drivers of increased DALYs, contributing 68.2% and 20.9%, respectively. High-income regions are predominantly influenced by population growth, while population increases pose significant challenges for low- and middle-income regions.
In 1990, DALYs were heavily concentrated in low-SDI countries (SII = −9.6, 95% UI: −18.4, −0.9), but by 2021, the SII increased to 2.5 (95% UI: −9.2, 14.3), which, although not statistically significant, generally suggests a shift in disease burden toward countries with higher SDI. This trend may reflect ongoing global industrial restructuring, rising occupational health awareness and gradually improving protective measures in low- and middle-income countries, as well as an increasing proportion of non-manual workers in high-SDI countries. Moreover, although the 95% uncertainty interval for SII in 2021 remains wide—indicating considerable estimation uncertainty—the smoothed visualization curve shows a more consistent pattern compared to 1990, suggesting reduced volatility in disease burden disparities across SDI levels. This may imply that some countries have begun to make progress in reducing occupational noise-related health burdens. Notably, most countries with SDI ≤ 0.6 remain markedly above the optimal frontier, indicating continued lag in noise exposure control and early intervention capacity. Addressing structural risk factors and ensuring equitable allocation of health resources should remain priorities for future global occupational health initiatives.
The construction industry encounters more significant challenges with occupational noise exposure compared to other sectors65,66,67. Construction sites are often uncontrolled environments with highly variable and unpredictable noise exposure. Additionally, the high mobility of construction workers exacerbates the difficulty of managing noise exposure, making it an under-recognized but critical issue in this sector46. Risk perception is closely linked to health protection behaviors24,68. Xia et al.69 demonstrated that recognizing potential risks in the work environment increases workers’ likelihood of engaging in and adhering to safety education. Noise effect perception acts as a mediator for personal protective behaviors70. While noise discomfort may activate defensive mechanisms, encouraging protective behaviors, these effects depend on individual noise sensitivity71,72. Workers with low noise sensitivity may exhibit less emotional response, emphasizing the need for physiological monitoring. Noise effect perception is also influenced by exposure levels; even highly sensitive individuals may not experience significant psychological changes at low noise levels73,74. Portable noise dosimeters can help workers accurately monitor real-time noise exposure levels. With advancements in wearable technology, multi-parameter physiological monitoring devices can provide real-time tracking of noise exposure’s effects on physical health. Alerts can notify workers when noise or physiological levels exceed safe thresholds, prompting timely protective actions such as noise reduction or rest. These systems can also upload data to cloud platforms for recording and sharing, supporting occupational disease prevention and personalized health assessments. Transitioning traditional noise management to a dynamic, intelligent health management system is a necessary future development.
Practical recommendations
It was found that the burden of occupational noise-related diseases was significantly higher among males than females. This disparity has been attributed in part to the higher likelihood of smoking among males, with the ototoxic substances in cigarette smoke believed to exacerbate hearing damage when combined with occupational noise exposure75,76. In contrast, a protective effect on hearing has been reported for estrogen77, and women often exhibit a stronger awareness of self-protection. Therefore, greater attention should be given to male workers, especially regarding hearing loss and non-auditory conditions such as hypertension. Younger workers typically have shorter durations of noise exposure78, and with the rise of internet access and educational attainment, they are more likely to acquire knowledge about hearing protection79, proactively enhancing preventive awareness and adopting protective measures. Moreover, young individuals are more inclined to seek timely medical care upon detecting auditory abnormalities, which can reduce long-term damage. In contrast, older workers may face greater hearing-related issues due to insufficient awareness or neglect of protective measures. Given that males aged 45–74 were identified as a high-risk group in our analysis, it is recommended to establish regular occupational health screening programs for middle-aged and older workers, focusing on auditory function and hypertension detection. The likelihood of noise-induced hearing loss rises with advancing age22, especially in nations experiencing rapid population aging, underscoring the importance of implementing targeted protective measures for older workers. To strengthen occupational noise regulation, the U.S. Occupational Safety and Health Administration (OSHA) has established an 8-hour time-weighted average noise exposure limit of 90 dBA, while the Centers for Disease Control and Prevention (CDC) recommends 85 dBA, above which hearing damage may occur80. In China, jobs where noise levels exceed national occupational exposure limits are officially designated as “noisy work,” and employers are required to implement strict noise control measures to ensure compliance with exposure limits, thereby safeguarding workers’ hearing and safety.
Routine noise monitoring and risk assessment are essential for preventing occupational hearing loss81. Employers should install noise monitoring stations in high-exposure areas and conduct regular measurements to ensure compliance. If the 8-hour equivalent continuous sound level is ≥ 85 dBA, prompt implementation of control measures is required. Workers’ exposure durations should also be recorded, and work schedules adjusted accordingly to mitigate risk. Workers should be informed of monitoring results in a timely manner to raise awareness and encourage participation in protective measures. Quiet rest areas with adequate sound insulation should be provided in noisy work environments, allowing temporary escape from exposure. In highly dynamic and uncontrolled environments, such as construction sites, workers should be required to wear HPDs, undergo regular on-site noise monitoring, and receive individualized exposure assessments. Portable dosimeters and physiological monitoring devices should be introduced to enable real-time interventions for high-risk occupations. Since mining and manufacturing remain sectors with high incidence of NIHL, and new occupational categories continue to emerge, dynamic evaluation of occupational health across industries is increasingly crucial. Current regulatory standards should be regularly updated to effectively protect worker health. To reduce the burden of occupational noise-related diseases, local legislation should be strengthened to integrate noise control into urban planning, enterprise management, and workers’ compensation frameworks, especially in rapidly industrializing nations. Furthermore, public education campaigns should be expanded to improve awareness of noise-related health risks and encourage proactive use of protective measures.
The health impacts of occupational noise must be fully recognized and addressed. International collaboration should focus on optimizing intelligent noise reduction devices and personalized hearing protection solutions. High-burden countries can adapt successful strategies to their specific contexts, establishing targeted occupational noise management policies. Early interventions and protections against occupational noise exposure should be prioritized. Educational campaigns through media and community outreach can raise public awareness of occupational noise hazards. For high-burden populations, particularly middle-aged and older individuals, efforts should focus on monitoring and managing chronic diseases. Wearable devices and real-time monitoring technologies should be leveraged to build an international database of occupational noise exposure, enabling long-term, multi-dimensional health impact assessments. By adopting intelligent and dynamic health management practices, global occupational noise-related health outcomes can be improved, fostering equity and sustainable occupational health management.
Limitations and future work
While this study underscores the significance of addressing the health burden of occupational noise and provides a comprehensive analysis of global trends across dimensions such as region, time, gender, age, and SDI, it has several limitations. First, the data used in this study were sourced from the GBD 2021 which, despite its proven reliability in many studies, may have limitations in data collection in certain countries due to resource constraints. This could result in underreporting of occupational noise-related disease burdens in those regions. Second, the effects of occupational noise exposure on certain diseases (e.g., sleep disorders) might be confounded by factors such as exposure to traffic noise3, which could affect the accuracy of occupational noise-related disease burden estimates. Third, the study primarily focuses on the correlation between occupational noise and hearing loss, with limited discussion of other health impacts, such as mental health disorders, cardiovascular diseases, and sleep disturbances. The specific types of occupational noise-related diseases were not analyzed in depth. Future studies should aim to establish more comprehensive exposure–response models to quantitatively assess the long-term multi-systemic health effects of occupational noise, thereby enriching the occupational noise risk assessment framework. Given the current study’s finding that middle-aged and older men bear the greatest burden of disease, longitudinal cohort studies at the individual level are warranted. These should incorporate noise exposure dosage, physiological stress markers, and validated psychological scales to elucidate the biological pathways and critical inflection points through which occupational noise contributes to chronic disease development. Our frontier analysis further revealed that most low- and middle-SDI countries still fall significantly short of achieving the theoretically optimal level of health. Future research could integrate national industrial structures and occupational protection systems to develop SDI-stratified prioritization frameworks for interventions, thereby supporting evidence-based resource allocation. By applying interdisciplinary approaches combining socioeconomic and geospatial statistical methods, future studies may also investigate how social determinants—such as SDI, labor structure, and healthcare accessibility—interact with occupational noise exposure to exacerbate health inequities. Additionally, advances in wearable devices and mobile sensing technologies offer new opportunities to construct real-time, individualized occupational noise exposure assessment systems. These systems, combined with physiological monitoring and historical exposure records, could enable dynamic risk forecasting and personalized intervention strategies for high-risk occupations.
Conclusion
This study systematically evaluated the spatiotemporal distribution, gender and age differences, and the relationship with the sociodemographic Index (SDI) of occupational noise-related disease burden globally from 1990 to 2021. Future trends were also projected. The key findings are as follows:
-
(1)
Occupational noise-related disability-adjusted life years (DALYs) showed significant regional differences, with 47 countries having estimated annual percentage change (EAPC) > 0.1, mainly concentrated in rapidly industrializing nations. The Solomon Islands recorded the highest EAPC (1.1). Between 1990 and 2021, DALYs increased most rapidly in East Asia (+ 10.7 per 100,000) and Andean Latin America (+ 5.4 per 100,000), while significant decreases were observed in North Africa and the Middle East (−5.3 per 100,000) and high-income North America (−4.3 per 100,000). The burden was higher in low-income and developing countries.
-
(2)
Males and middle-aged groups were identified as major at-risk populations for occupational noise exposure. The 50–64 age group contributed most significantly to the disease burden, with a rapid increase observed in the 45–74 age range. The largest gender disparity was noted in the 25–39 age group, where males experienced 1.7 times the burden of females.
-
(3)
DALYs significantly decreased with increasing SDI. EAPC showed significant positive correlations with both DALYs (R = 0.3) and SDI (R = 0.4). Regions with high DALYs (> 100.0) and SDI in the 0.4–0.6 range exhibited the most pronounced EAPC growth.
-
(4)
By 2035, DALYs are projected to decrease to 125.0 ± 1.9 per 100,000. The burden is expected to decline rapidly among individuals aged 15–34 but increase significantly among those aged 65 and above.
-
(5)
Population growth (68.2%) and aging (20.9%) were identified as the primary drivers of DALYs increases. From 1990 to 2021, the slope inequality index (SII) changed from − 9.6 to 2.5, and the CI curve became smoother. Although global inequalities in occupational noise-related disease burdens have decreased, low-SDI countries continue to bear a disproportionately high burden, with significant gaps compared to theoretical minimum levels.
This study highlights low-income countries, males, and middle-aged to elderly populations as key targets for intervention. It recommends enhancing international collaboration to provide tailored health services for high-risk populations. Addressing occupational noise health burdens in construction industries is particularly urgent. Leveraging big data and physiological monitoring technologies, transitioning from traditional noise exposure management to dynamic and intelligent health management is an inevitable future trend. This research not only provides a comprehensive perspective on the current status and trends of occupational noise-related disease burdens but also offers scientific insights for policymakers and public health managers, advancing the shared goals of global occupational health and health equity.
Data availability
The data presented in this study are available on request from the corresponding author.
References
Chen, H., Hou, C., Zhang, L. & Li, S. Comparative study on the strands of research on the governance model of international occupational safety and health issues. Saf. Sci. 122, 104513 (2020).
Abidin, A. N. Z., Jusoh, M. & Zakaria, Z. Y. Simulation of noise exposure level of fire-fighters in emergency response services in Malaysia. Saf. Sci. 105, 121–127 (2018).
Rahmanian, M., Zare Sakhvidi, M. J., Mehrparvar, A. H., Sakhvidi, Z., Dadvand, P. & F. & Association between occupational noise exposure and diabetes: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health. 252, 114222. https://doi.org/10.1016/j.ijheh.2023.114222 (2023).
Basner, M. et al. Auditory and non-auditory effects of noise on health. Lancet 383, 1325–1332 (2014).
Lichenstein, R., Smith, D. C., Ambrose, J. L. & Moody, L. A. Headphone use and pedestrian injury and death in the united states: 2004–2011. Inj. Prev. 18, 287–290 (2012).
Khoza-Shangase, K. & The Association Between, H. I. V. A. I. D. S. Ototoxicity of its treatments, and occupational noise induced hearing loss: A narrative review mapping the existing literature and identifying research gaps. Int. J. Environ. Res. Public. Health. 22 https://doi.org/10.3390/ijerph22040487 (2025).
Li, W., Cai, J., Liao, G., Kwan, M. P. & Tse, L. A. Individual-level noise exposure and its association with sleep quality and duration: A cross-sectional study using real-time data. Sci. Total Environ. 955, 177047. https://doi.org/10.1016/j.scitotenv.2024.177047 (2024).
Hahad, O. et al. Cerebral consequences of environmental noise exposure. Environ. Int. 165 https://doi.org/10.1016/j.envint.2022.107306 (2022).
Thompson, R. et al. Noise pollution and human cognition: an updated systematic review and meta-analysis of recent evidence. Environ. Int. 158, 106905. https://doi.org/10.1016/j.envint.2021.106905 (2022).
Peris, E. & Fenech, B. Associations and effect modification between transportation noise, self-reported response to noise and the wider determinants of health: A narrative synthesis of the literature. Sci. Total Environ. 748 https://doi.org/10.1016/j.scitotenv.2020.141040 (2020).
Concha-Barrientos, M. et al. Occupational Noise: Assessing the Burden of Disease from work-related Hearing Impairment at National and Local Levels (World Health Organization, 2004).
Kerns, E., Masterson, E. A., Themann, C. L. & Calvert, G. M. Cardiovascular conditions, hearing difficulty, and occupational noise exposure within US industries and occupations. Am. J. Ind. Med. 61, 477–491 (2018).
Thirion, P. et al. (Published on, (2012).
Themann, C. L. & Masterson, E. A. Occupational noise exposure: A review of its effects, epidemiology, and impact with recommendations for reducing its burden. J. Acoust. Soc. Am. 146, 3879–3905 (2019).
Dzhambov, A. M., Dimitrova, D. D. & Dimitrakova, E. D. Noise exposure during pregnancy, birth outcomes and fetal development: meta-analyses using quality effects model. Folia Med. 56, 204 (2014).
Dzhambov, A. & Dimitrova, D. Occupational noise exposure and the risk for work-related injury: a systematic review and meta-analysis. Ann. Work Exposures Health. 61, 1037–1053 (2017).
Teixeira, L. R. et al. The prevalence of occupational exposure to noise: A systematic review and meta-analysis from the WHO/ILO joint estimates of the Work-related burden of disease and injury. Environ. Int. 154, 106380. https://doi.org/10.1016/j.envint.2021.106380 (2021).
Basner, M. & McGuire, S. WHO environmental noise guidelines for the European region: a systematic review on environmental noise and effects on sleep. Int. J. Environ. Res. Public Health. 15, 519 (2018).
Van Kempen, E., Casas, M., Pershagen, G. & Foraster, M. WHO environmental noise guidelines for the European region: a systematic review on environmental noise and cardiovascular and metabolic effects: a summary. Int. J. Environ. Res. Public Health. 15, 379 (2018).
Guo, X., Davies, H. W. & Karim, M. E. The intensity and duration of occupational noise exposure and cardiovascular disease in the united states: a nationally representative study, 2015 to 2020. Ann. Work Expo Health. 68, 36–47. https://doi.org/10.1093/annweh/wxad065 (2024).
Wu, Z., Liang, Y., Khan, A. & He, J. Is occupational noise associated with arthritis? Cross-sectional evidence from US population. BMC Public. Health. 24, 371. https://doi.org/10.1186/s12889-024-17897-0 (2024).
Wang, S. et al. A systematic analysis of the burden of disease attributable to occupational noise-induced hearing loss in China based on the 2019 global burden of disease study. BMC Public. Health. 24, 3423. https://doi.org/10.1186/s12889-024-21094-4 (2024).
Liu, C. et al. The burden of occupational Noise-Induced hearing loss from 1990 to 2019: an analysis of global burden of disease data. Ear Hear. 10, 1097 (2024).
Chong, D., Chen, L., Peng, Y. & Yu, A. Occupational noise-related perception and personal protection behavior among Chinese construction workers. Saf. Sci. 147 https://doi.org/10.1016/j.ssci.2021.105629 (2022).
He, J., Smith, L. M., Shkembi, A. & Neitzel, R. L. Evaluating the impact of occupational noise exposure on workplace fatal and nonfatal injuries in the U.S. (2006–2020). Int. J. Hyg. Environ. Health. 263, 114468. https://doi.org/10.1016/j.ijheh.2024.114468 (2024).
Tak, S. & Calvert, G. M. Hearing difficulty attributable to employment by industry and occupation: an analysis of the National health interview Survey—United states, 1997 to 2003. J. Occup. Environ. Med. 50, 46–56 (2008).
Dai, X. et al. Occupational noise and genetic variants in stress hormone biosynthesis-based genes and rates of blood lipid changes in china: A five-year longitudinal study. Int. J. Hyg. Environ. Health. 260, 114404. https://doi.org/10.1016/j.ijheh.2024.114404 (2024).
Hao, G., Shi, Z., Zhang, B., Dong, Y. & Liang, G. Global burden of ischemic stroke in middle-aged workforce population, 1990–2021: systematic analysis of the Global Burden of Disease Study 2021. Neuroepidemiology (2025).
Wang, Y. et al. Global burden of metabolic-associated fatty liver disease: A systematic analysis of global burden of disease study 2021. Chin. Med. J. 10, 1097 (2025).
Bernabe, E. et al. Trends in the global, regional, and National burden of oral conditions from 1990 to 2021: a systematic analysis for the global burden of disease study 2021. Lancet 405, 897–910 (2025).
Collaborators, G. U. N. D. et al. Burden of neurological disorders across the US from 1990–2017: A global burden of disease study. JAMA Neurol. 78, 165–176. https://doi.org/10.1001/jamaneurol.2020.4152 (2021).
Ekundayo, T. C., Swalaha, F. M. & Ijabadeniyi, O. A. Global and regional prevalence of Helicobacter pylori in drinking waters: A sustainable, human development and socio-demographic indices based meta-regression-modelling. Sci. Total Environ. 861 https://doi.org/10.1016/j.scitotenv.2022.160633 (2023).
Dadhania, K. et al. Global, regional, and National trends in cardiovascular disease burden and risk factors in individuals under 20 from 1990 to 2019: insights from the Gbd 2019 study. J. Am. Coll. Cardiol. 83 https://doi.org/10.1016/s0735-1097(24)04311-0 (2024).
Moran, A. E. et al. Assessing the global burden of ischemic heart disease: part 1: methods for a systematic review of the global epidemiology of ischemic heart disease in 1990 and 2010. Global Heart. 7, 315–329 (2012).
Guan, S. Y. et al. Global burden due to modifiable risk factors for autoimmune diseases, 1990–2021: Temporal trends and socio-demographic inequalities. Autoimmun. Rev. 23, 103674. https://doi.org/10.1016/j.autrev.2024.103674 (2024).
Organization, W. H. in WHO report on the global tobacco epidemic, 2021: addressing new and emerging products: web annex IX: tobacco taxes, prices and affordability: Table 9.3 (2021).
Collaborators, G. T. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of disease study 2019. Lancet (London England). 397, 2337 (2021).
Chen, Y. et al. Comparative diabetes mellitus burden trends across global, chinese, US, and Indian populations using GBD 2021 database. Sci. Rep. 15, 1–16 (2025).
Xiao, Y., Hong, X., Neelagar, R. & Mo, H. Age-standardized incidence, prevalence, mortality rates and future projections of autoimmune diseases in china: a systematic analysis based on GBD 2021. Immunol. Res. 73, 26 (2025).
Hankey, B. F. et al. Partitioning linear trends in age-adjusted rates. Cancer Causes Control. 11, 31–35 (2000).
Cen, J. et al. Global, regional, and National burden and trends of migraine among women of childbearing age from 1990 to 2021: insights from the global burden of disease study 2021. J. Headache Pain. 25, 96. https://doi.org/10.1186/s10194-024-01798-z (2024).
Zhang, K. et al. Global, regional, and National epidemiology of diabetes in children from 1990 to 2019. JAMA Pediatr. 177, 837–846. https://doi.org/10.1001/jamapediatrics.2023.2029 (2023).
Ni, Y. et al. Evidence of traditional Chinese medicine for treating type 2 diabetes mellitus: from molecular mechanisms to clinical efficacy. Pharm. Biol. 62, 592–606 (2024).
Xie, X. et al. Trends in stomach Cancer burden in china: A joinpoint and APC analysis based on GBD 2021. J. Gastroenterol. Hepatol. (2025).
Clegg, L. X., Hankey, B. F., Tiwari, R., Feuer, E. J. & Edwards, B. K. Estimating average annual per cent change in trend analysis. Stat. Med. 28, 3670–3682 (2009).
Lan, Y. et al. The burden of liver cirrhosis and underlying etiologies: results from the global burden of disease study 2019. Hepatol. Commun. 7, e0026 (2023).
Zou, Z. et al. Time trends in cardiovascular disease mortality across the BRICS: an age-period-cohort analysis of key nations with emerging economies using the global burden of disease study 2017. Circulation 141, 790–799 (2020).
Rosenberg, P. S., Check, D. P. & Anderson, W. F. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol. Biomarkers Prev. 23, 2296–2302. https://doi.org/10.1158/1055-9965.EPI-14-0300 (2014).
Fosse, E. In Age, Period and Cohort Effects,142–175 (Routledge, 2020).
Riebler, A. & Held, L. Projecting the future burden of cancer: bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom J. 59, 531–549. https://doi.org/10.1002/bimj.201500263 (2017).
Liu, Z. et al. Global trend of aetiology-based primary liver cancer incidence from 1990 to 2030: a modelling study. Int. J. Epidemiol. 50, 128–142. https://doi.org/10.1093/ije/dyaa196 (2021).
Jiang, C. Y. et al. Global, regional, and National prevalence of hearing loss from 1990 to 2019: A trend and health inequality analyses based on the global burden of disease study 2019. Ageing Res. Rev. 92, 102124. https://doi.org/10.1016/j.arr.2023.102124 (2023).
Organization, W. H. Handbook on Health Inequality Monitoring: with a Special Focus on low-and middle-income Countries (World Health Organization, 2013).
Guo, Z., Xiong, F., Lu, Y. & Lv, W. Global trends and regional disparities in inflammatory bowel disease burden: insights from the GBD 2021 study. Curr. Sci. 5, 2317–2334 (2025).
Mujica, O. J. & Moreno, C. M. From words to action: measuring health inequalities to leave no one behind. Rev. Panam. Salud Publica. 43, e12 (2019).
Bai, Z. et al. The global, regional, and National patterns of change in the burden of congenital birth defects, 1990–2021: an analysis of the global burden of disease study 2021 and forecast to 2040. EClinicalMedicine 77 (2024).
Sá, M. M., Azevedo, R., Martins, C. & Machado, O. Portuguese physical education instructors’ exposure to noise and perception of associated risk. Hum. Ecol. Risk Assessment: Int. J. 20, 448–460 (2014).
Münzel, T., Sørensen, M. & Daiber, A. Transportation noise pollution and cardiovascular disease. Nat. Reviews Cardiol. 18, 619–636 (2021).
Virkkunen, H., Kauppinen, T. & Tenkanen, L. Long-term effect of occupational noise on the risk of coronary heart disease. Scandinavian J. Work Environ. & Health, 291–299 (2005).
Goyal, S., Gupta, V. & Walia, L. Effect of noise stress on autonomic function tests. Noise Health. 12, 182–186 (2010).
Fu, W. et al. Association between exposure to noise and risk of hypertension: a meta-analysis of observational epidemiological studies. J. Hypertens. 35, 2358–2366 (2017).
LI, J. et al. Effect of cumulative noise exposure on hypertension in automotive manufacturing workers. China Occup. Medicine, 173–177 (2018).
Chen, S. et al. Noise exposure in occupational setting associated with elevated blood pressure in China. BMC Public. Health. 17, 1–7 (2017).
Stansfeld, S. A. & Matheson, M. P. Noise pollution: non-auditory effects on health. Br. Med. Bull. 68, 243–257 (2003).
Fernández, M. D., Quintana, S., Chavarría, N. & Ballesteros, J. A. Noise exposure of workers of the construction sector. Appl. Acoust. 70, 753–760 (2009).
Li, X., Song, Z., Wang, T., Zheng, Y. & Ning, X. Health impacts of construction noise on workers: A quantitative assessment model based on exposure measurement. J. Clean. Prod. 135, 721–731 (2016).
Neitzel, R. L., Andersson, M., Eriksson, H., Torén, K. & Andersson, E. Development of a job exposure matrix for noise in the Swedish soft tissue paper industry. Annals Work Exposures Health. 62, 195–209 (2018).
Tinoco, H. C., Lima, G. B. A., Sant’Anna, A. P., Gomes, C. F. S. & Santos, J. A. N. D. Risk perception in the use of personal protective equipment against noise-induced hearing loss. Gestão Produção. 26, e1611 (2019).
Xia, N., Wang, X., Griffin, M. A., Wu, C. & Liu, B. Do we see how they perceive risk? An integrated analysis of risk perception and its effect on workplace safety behavior. Accid. Anal. Prev. 106, 234–242 (2017).
Park, S. H., Lee, P. J. & Jeong, J. H. Effects of noise sensitivity on Psychophysiological responses to Building noise. Build. Environ. 136, 302–311 (2018).
Okokon, E. O. et al. Traffic noise, noise annoyance and psychotropic medication use. Environ. Int. 119, 287–294 (2018).
Baliatsas, C., van Kamp, I., Swart, W., Hooiveld, M. & Yzermans, J. Noise sensitivity: symptoms, health status, illness behavior and co-occurring environmental sensitivities. Environ. Res. 150, 8–13 (2016).
Lee, S. C., Hong, J. Y. & Jeon, J. Y. Effects of acoustic characteristics of combined construction noise on annoyance. Build. Environ. 92, 657–667 (2015).
Schreckenberg, D., Griefahn, B. & Meis, M. The associations between noise sensitivity, reported physical and mental health, perceived environmental quality, and noise annoyance. Noise Health. 12, 7–16 (2010).
Barone, J. A., Peters, J. M., Garabrant, D. H., Bernstein, L. & Krebsbach, R. Smoking as a risk factor in noise-induced hearing loss. Journal Occup. Medicine, 741–745 (1987).
Daniel, E. Noise and hearing loss: a review. J. Sch. Health. 77, 225–231 (2007).
Wang, X. et al. Estrogen as a guardian of auditory health: Tsp1–CD47 axis regulation and noise-induced hearing loss. Climacteric 28, 143–153 (2025).
Masterson, E. A. et al. Prevalence of hearing loss in the united States by industry. Am. J. Ind. Med. 56, 670–681 (2013).
Berkman, N. D., Sheridan, S. L., Donahue, K. E., Halpern, D. J. & Crotty, K. Low health literacy and health outcomes: an updated systematic review. Ann. Intern. Med. 155, 97–107 (2011).
Hertzano, R., Lipford, E. L. & Depireux, D. Noise: acoustic trauma to the inner ear. Otolaryngol Clin North Am. 53, 531–542 (2020).
Lie, A. et al. Occupational noise exposure and hearing: a systematic review. Int. Arch. Occup. Environ. Health. 89, 351–372 (2016).
Acknowledgements
This research was supported by Innovation Institute for Sustainable Maritime Architecture Research and Technology. We also glad to give our special thanks to all participants.
Funding
This study was supported by the Natural Science Foundation of Shandong Province (Grant No. ZR2023ME232).
Author information
Authors and Affiliations
Contributions
Y.W. and N.Z. wrote the main manuscript text.X.L. and W.D. prepared Figs. 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 and 14. H.W.and X.S. completed the data analysis.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Y., Zhang, N., Li, X. et al. Global health burden and inequality patterns of occupational noise exposure from 1990 to 2019. Sci Rep 15, 24844 (2025). https://doi.org/10.1038/s41598-025-09575-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-09575-x
Keywords
This article is cited by
-
Dual-Omics Mapping of Tinnitus Phenotype Transition in Noise-Exposed Auditory Cortex
Cellular and Molecular Neurobiology (2025)
