
Abstract
The INFORM (Index for Risk Management) identifies risk hotspots by assessing Hazard and Exposure, Vulnerability, and Coping capacity across 76 indicators. However, the original index may have overlooked the specific vulnerabilities of women and children, even within the vulnerable group in emergencies. This study recalibrated the index by redefining key indicators to better reflect risks for these groups. INFORM Index Risk formulation is “Risk = Hazard and Exposure 1/3 x Vulnerability 1/3 x Lack of coping capacity 1/3’ resulted in a total score ranging from 0 to 10, with the higher score being the higher risk. We recalibrated the 2024 INFORM Risk formula by adjusting for female and child (ages 0–14) populations in 67 countries across the Eastern Mediterranean, South Asia, and Sub-Saharan Africa. We categorized the 76 metrics as (1) those with gender-disaggregated data, (2) those adaptable for specific populations using literature, and (3) generalized indicators needing no adjustment. Shifts in risk classifications were noted among 67 countries. Initially, 13 countries (19.4%) were at ‘very high’ risk, and 18 (26.9%) were at ‘high’ risk. After recalibration, 52 countries (77.6%) showed score changes from 0.1 to 0.6 points. Six countries moved from ‘high’ to ‘very high’ risk, raising this class to 19 (28.3%). The paired t-test revealed a statistically significant difference between the original and recalibrated risk scores (mean difference = -0.17, 95% CI: -0.20, -0.13, p < 0.001). The difference in Vulnerability scores (mean difference = -0.32; 95% CI: -0.44, -0.21; p-value < 0.000) and Coping capacity (mean difference = -0.18; 95% CI: -0.23, -0.12; p-value < 0.000) were significant, derived changes in the INFORM Risk Index. The recalibrated INFORM index highlights that accurate, disaggregated data is crucial for understanding the specific needs of vulnerable populations, enabling more informed decision-making in risk management and resilience planning.
Similar content being viewed by others


Introduction
Disaster risk management has evolved significantly over the past decades1,2. It has shifted from simply reacting to crises to proactively reducing risks3. Advances in technology and global collaborations have improved early warnings and community preparedness3,4,5. Data-driven strategies have been crucial in mitigating suffering caused by complex humanitarian emergencies6,7. 2015 was particularly significant because three key international frameworks were adopted: the Sendai Framework for Disaster Risk Reduction, the Sustainable Development Goals (SDGs), and the Paris Agreement on Climate Change8. These frameworks emphasized the importance of utilizing scientific data to track a country’s progress.
The INFORM initiative is a collaboration between the Inter-Agency Standing Committee (IASC) and the European Commission under the Disaster Risk Management Knowledge Centre (DRMKC)9,10. INFORM has become a globally recognized multi-hazard humanitarian risk tool designed as an open-source initiative. It can be contextualized and calculated over time to assess the risk of complex emergencies and evaluate and compare populations’ vulnerability and resilience to various exposures and hazards9,10,11. These indices are built to serve multiple critical purposes in disaster risk management. They identify vulnerable groups, support humanitarian organizations, and facilitate early action for improved crisis response and effective resource allocation9,10. They help policymakers address the root causes of risk and guide investments in infrastructure, education, healthcare, and other critical sectors to build long-term resilience plans11. Additionally, the risk index enables international comparisons and trend analyses by offering standardized measures, facilitating the identification of best practices, and supporting global strategies for disaster risk reduction11.
The INFORM Risk Index was officially launched in 2014, with annual updates to enhance its accuracy and relevance10. These updates typically include introducing new indicators, revising existing ones, and updating data sources. Key categories of updates involve socio-economic indicators, health metrics, conflict intensity measures, and natural hazard exposure data9,11. Each year, the index incorporates the latest available data, adjusts methodologies as needed, and refines its indicators to provide a more accurate assessment of global humanitarian risk9,12. The INFORM Risk Index has three core dimensions: ‘hazard and exposure,’ ‘vulnerability,’ and ‘lack of coping capacity.'9 The ‘hazard and exposure’ dimension assesses the likelihood and extent of exposure to hazards, including natural disasters such as earthquakes, floods, and cyclones, as well as human-induced events like conflict and political instability9. This dimension analyzes historical data and projections to identify regions that are prone to specific hazards, supporting targeted preparedness and mitigation efforts9. The ‘vulnerability’ dimension assesses the susceptibility of populations to the impact of hazards9. It considers socio-economic conditions, health status, and the presence of vulnerable groups to provide insights into the root causes of vulnerability. Indicators include poverty levels, educational attainment, and the prevalence of chronic diseases9. The ‘lack of coping capacity’ dimension measures the ability of populations to cope with and recover from the impacts of hazards9. It includes indicators related to institutional capacity, infrastructure, and economic stability, highlighting areas where resilience needs to be strengthened9.
This index was calculated using 76 indicators, of which 34 are linked to ‘hazard and exposure,’ 24 are related to ‘vulnerability,’ and 18 are related to ‘lack of coping capacity.‘9 The index was initially developed for global risk assessment. However, countries have recently customized it to the subnational and administrative levels to suit their specific contexts, allowing for more granular analysis and localized risk management11. For instance, INFORM subnational projects have been rolled out in Latin America, the Caribbean, Southern Africa, and Central Asia, enabling local lead organizations to assess and address risks at a more precise geographical scale11.
Female and child populations are at higher risk of disasters due to several interconnected factors that exacerbate their vulnerability2,13,14,15,16,17,18. Women and girls often face social, economic, and cultural barriers that limit their access to resources, information, and decision-making power13,19. These barriers can restrict their ability to respond effectively to disaster risks and impacts. For instance, women may have limited access to financial, educational, and technological resources crucial for disaster preparedness and recovery20. Gender roles and responsibilities, such as caregiving and household management, can increase their exposure to disaster risks and reduce mobility during emergencies13. Children are particularly vulnerable due to physical and developmental characteristics, making them more susceptible to injury, illness, and physical and mental trauma during disasters21,22. Their dependency on adults for protection and care further heightens their risk13,19. Studies have shown that women die at higher rates than men during disasters due to both direct and indirect impacts23. During the 1991 cyclone in Bangladesh, women were three to five times more likely to die than men, primarily due to limited access to risk information and lack of decision-making power regarding evacuation24. Similarly, in the 2004 tsunami in Indonesia, adult women were twice as likely to die compared to men, influenced by physiological differences, socioeconomic factors, and limited mobility25. Women also tend to show higher rates of post-traumatic stress disorder (PTSD), anxiety, and depression following disasters and conflict26. Likewise, mortality risk among women and children from non-violent causes significantly increases in response to nearby conflict; the risk becomes more significant with higher intensity and prolonged conflicts27. Between 1995 and 2015, more than 10 million under-five deaths globally were attributed to conflict27. Further, women of reproductive age living near high-intensity conflicts face a mortality rate three times higher than women in peaceful areas28.
Conflicts, natural disasters, or similar crises have a profound impact on vulnerable populations, including displaced individuals29,30,31,32. Despite efforts to improve resilience and outcomes for these groups, substantial obstacles have yet to be overcome33,34,35. Vulnerability in this context often refers to limited access to resources, inadequate infrastructure, and heightened exposure to hazards33,34,35. This is particularly true for maternal, neonatal, and child health (MNCH), where displaced populations are frequently overlooked in risk indexes despite progress in programs and outcomes over the past decade14,16,36,37. Therefore, although the INFORM Risk Index is valid at the country level, there are still opportunities to gain a deeper understanding of how this index can provide more insight into vulnerable populations. These crises affect nearly 300 million people worldwide who need assistance and protection38. Women and children represent a disproportionate percentage of those in need39,40,41. On average, more than half of these individuals are women and girls39,40. According to UN agencies, nearly 614 million women and girls are living in conflict, with a 50% increase compared to 201740. Nearly 1.05 billion reside in slums40. While 94 million children require protection, education, health, and nutrition support, more than 200 million people live in countries prone to disasters or are affected by conflicts41. Furthermore, this highlights the critical need to understand the specific risks that these vulnerable groups are facing.
The INFORM Risk index has considered the overall vulnerable groups at the population level, but the vulnerability of the female population and children becomes more crucial in emergencies and disasters15,18,42. The index’s current indicators are broad and not specific enough to fully capture the unique vulnerabilities of women and children aged 0 to 14. Moreover, many indicators are not disaggregated by gender, masking challenges these groups might face at the country level. To address this gap, our exploratory study recalibrated the existing index by redefining the selective indicators for women and children who are the most vulnerable of the vulnerable during disasters and emergencies. By doing so, we aimed to highlight their unique vulnerabilities and provide a more precise, specific description of their risk profiles in selected countries.
Methods
Study design
This exploratory study employed a secondary data analysis design to refine the INFORM Risk Index and redefine the risks for vulnerable groups. The study utilized existing data sheets in Excel files, which also contain built-in formulas available online12.
Study population
The study focused on the total female population and children aged 0–14 in the countries. General vulnerability indicators typically assess broad and population-level categories, such as economic status, human development index, literacy rate, displacement, and access to water and sanitation, capturing the average risk across the entire population. We specifically selected all 67 countries across the Eastern Mediterranean Region of the World Health Organization (EMRO), South Asia, and Sub-Saharan Africa, covering North, East, West, and Central regions. These regions were selected since they are among the most disaster-prone and conflict-affected globally, where women and children disproportionately face intensified risks due to systemic vulnerabilities and limited coping capacities11,12. Many selected regions have recently experienced significant humanitarian crises driven by natural disasters, armed conflicts, or severe economic downturns, making them particularly relevant for this study. The target selection ensures that the study focuses on areas needing the most detailed risk and vulnerability assessments, providing valuable insights for effective humanitarian response planning.
INFORM risk index
The index’s central equation is ‘Risk = Hazard and Exposure 1/3 x Vulnerability 1/3 x Lack of coping capacity 1/3’.9 These dimensions are calculated based on 76 indicators and using population data from 2015 to 2023. The Index is scored on a scale from 0.0 to 10.0, where lower values indicate better performance in managing humanitarian risk, and higher values indicate worse performance. Based on the scores derived from the equation, the countries are classified as very low (threshold: 0.0 to 2.1), low (threshold: 2.2 to 3.1), medium (threshold: 3.2 to 4.8), high (threshold: 4.9 to 6.7) and very high (threshold: 6.8 to 10.0)12. These dimensions are further divided into specific categories and components to provide a detailed assessment framework for humanitarian risk9. The hazard and exposure dimensions are divided into Natural and Human categories9. The Natural category includes earthquakes, floods, tsunamis, tropical cyclones, droughts, and epidemics9. The Human category consists of current conflict intensity and projected conflict risk9. The vulnerability dimension is categorized into socio-economic and vulnerable groups9. The socio-economic category includes components like development & deprivation (50%), inequality (25%), and aid dependency (25%).9 The vulnerable groups category encompasses uprooted people and other vulnerable groups. The lack of coping capacity dimension is split into the Institutional and Infrastructure categories9. The institutional category includes Disaster Risk Reduction (DRR) and governance components. The infrastructure category comprises communication, physical Infrastructure, and access to health systems9. Based on the scores, countries are ranked between 1 and 191; the lowest ranking indicates that countries are poorly ranked and the worst performing12. The original index, data used in the calculation, data sources, and all the formulas are open source and available on the official website of DRMKC12.
Approach
Recalibrating indicators for female gender and children
For this study, we classified the 76 indicators across all dimensions into three broad categories based on a review of the original index. These categories are: (1) Indicators where gender-disaggregated data is available from different data sources, therefore, can be changed and used as a proxy for our population of interest (2) Indicators that are not explicitly disaggregated but can be calculated for our target population using supporting literature based on the factor derived from the proportion of women and children affected by different types of disasters, and (3) Indicators that are not sensitive to gender, which were therefore not changed. Table 1 provides a description of the 76 indicators and the methodology adopted.
The indicators that were changed for this study were: adult literacy rate, percentage of female population, mobile cellular subscriptions, percentage of the population practicing open defecation, percentage of the population with basic handwashing facilities (including soap and water), Human Development Index, percentage of the population using at least essential sanitation services, and rate of the population using at least safe drinking water services, when the indicator data for the population of interest was unavailable for the specified time in the portals that we explored43,44,45,46. We retained the original reported values to ensure consistency in our analysis12. Given that most children aged 0–14 years (all genders) depend on their mothers, most indicators were explicitly examined for the female population and used as proxy indicators for children. A limitation encountered in the recalibration process was the lack of age-disaggregated data for children across most indicators. The INFORM Risk Index is primarily constructed using indicators that reflect general or adult population-level data. Very few indicators are specific to children or provide separate values by age group. In this context, and due to the critical dependency relationship between children and their caregivers, we used female-specific indicators as a proxy to approximate the vulnerability of children. Humanitarian reports are also highlighting how disruptions affecting women have direct implications for child health, safety, and survival in disaster settings47,48.
Data on indicators representing the population exposed to disasters and conflict were calculated by multiplying a standardized factor, ranging from 0.66 to 0.7513,3849–52. This indicates that, on average, 66–75% of the population affected by these hazards or crises are women and children. This factor was derived from an extensive literature review and reports published by the Internal Displacement Monitoring Centre, the United Nations Office for the Coordination of Humanitarian Affairs (OCHA), the United Nations Development Programme (UNDP), the World Bank Group, and European Civil Protection and ReliefWeb13,38,4649–55. These indicators were: annual expected exposure people to river floods, annual expected exposed people to tsunamis, annual expected exposed people to cyclone’s, wind Saffir-Simpson (SS)1, annual expected exposed people to cyclone wind SS3, annual expected exposure people to coastal floods, total affected by drought, people affected by natural disasters, For this study, we classified the indicators into three broad categories based on a thorough review of the original index. Moreover, for countries that are top priorities under Humanitarian Action, we obtained the indicator of the population needing humanitarian assistance due to complex emergencies, including internally displaced persons (IDPs), where applicable. The populations at risk of plasmodium vivax malaria (vector-borne) and plasmodium falciparum malaria (vector-borne) were calculated for target groups based on the prevalence reported in the original index12. While this multiplier is widely supported by humanitarian and displacement literature, it represents a standardized approximation and may not reflect context-specific differences in how disasters affect populations. Variations in age structure, gender roles, social protection systems, and the nature of the disaster or crisis could lead to either underestimation or overestimation of the actual proportion of women and children affected. The use of a uniform factor thus introduces potential bias and should be interpreted with caution.
Indicators that were kept constant, as they appeared in the original index are:12 physical exposure to earthquake-modified Mercalli intensity (MMI) VI, physical exposure to earthquake MMI VIII, frequency of drought events, agriculture drought probability, number of vets, IHR capacity score: food safety, population living in slums (% of urban population), children under 5 (% of the population), highly violent conflict probability, National power conflict intensity (highly violent), subnational conflict intensity (Highly Violent), multidimensional Poverty Index, humanitarian aid (FTS), development aid (ODA), net ODA received (% of GNI), volume of remittances (in USD) as a proportion of total GDP (%), under-five mortality rate, under-five underweight, incidence of tuberculosis, estimated number of people living with HIV - adult (> 15) rate, Incidence of HIV (per 1,000 uninfected population ages 15–49), malaria incidence per 1,000 population at risk, average dietary energy supply adequacy, prevalence of undernourishment, HFA scores last recent, government effectiveness, corruption perception index, access to electricity, road length, physicians density, proportion of the target population with access to 3 doses of diphtheria-tetanus-pertussis (DTP3) (%), Proportion of the target population with access to measles-containing-vaccine second-dose (MCV2) (%), Proportion of the target population with access to pneumococcal conjugate 3rd dose (PCV3) (%), current health expenditure per capita, maternal mortality ratio (modeled estimate), GDP per capita (current US$) and land area (sq. km).
Adjusting the population denominator
The original index was calculated using the total country population. Therefore, we adjusted the population denominator using World Bank population data to ensure accuracy56. We calculated the cumulative population by adding the total female population (including females aged 0–14 years) and male children aged 0–14 years from 2013 to 2023.
Data sources
We explored several data portals to obtain specific information on indicators for a population of interest, including the United Nations Women—Women Count, the World Bank’s Gender Data Portal, the Demographic Health Survey’s gender-related data, and Our World in Data43,44,45,46.
Index calculation
Using the INFORM Risk 2024 version 067 worksheet, which contains all necessary formulas and is available online, the index for a population of our interest was automatically calculated by changing specific indicators and the population denominator. This involved changes in scores for hazard and exposure, vulnerability, and lack of coping capacity, specifically for our population of interest. Recalculations were done automatically to ensure accuracy and consistency with the original methodology. To assess the impact of recalibration on country risk and ranking, we conducted paired and non-parametric tests on risk scores and rank positions. A paired t-test was applied to compare the original and updated risk scores, as both distributions were approximately normal. For rank comparison, we used the Wilcoxon signed-rank test, suitable for ordinal and skewed data, to test rank shifts following recalibration. Spearman’s rank correlation was also calculated to evaluate rank order consistency between original and recalibrated ranks. Analysis was performed on Microsoft® Excel® for Microsoft 365 MSO (Version 2410 Build 16.0.18129.20100), and Statistical analyses were performed using Stata, version 18.5 (StataCorp, College Station, (TX) (StataCorp, 2024).
Data files and details of all calculations and indicators are provided as under “Supplementary Material: All data sheets (15 September 2023 v 0.6.7) used in the data analysis.”
Ethical approval and informed consent procedure
This is the secondary analysis of open-sourced, publicly available data; therefore, ethical approval and informed consent are not applicable.
Results
Descriptives
Among the 67 countries studied, 13 (19.4%) were initially classified as ‘very high’ and 18 (26.9%) were ‘high’. Countries with a ‘very high’ original risk index included Afghanistan, Burkina Faso, Central African Republic, Chad, Congo DR, Ethiopia, Mali, Somalia, South Sudan, Sudan, Syria, Uganda, and Yemen. Additionally, countries with a ‘high’ original risk index included Angola, Bangladesh, Burundi, Cameroon, Congo, Djibouti, Egypt, Eritrea, India, Iran, Iraq, Kenya, Madagascar, Mozambique, Niger, Nigeria, Pakistan and Tanzania. In this study, six countries were reclassified as ‘very high’ from ‘high’ scores, i.e., Cameroon, Iraq, Kenya, Mozambique, Niger, and Nigeria. Libya reclassified to ‘high’ from ‘medium’ score. As a result, 19 (28.3%) countries appeared under ‘very high’ risk for the population of interest and 13 (19.4%) were reclassified as ‘high’. Table 2 presents a detailed description of the scores, classification and ranking changes among 67 countries.
Difference in scores and ranks
The paired t-test revealed a statistically significant difference between the original and recalibrated INFORM Risk Index (mean difference = -0.17; 95% CI: -0.20, -0.13; p-value < 0.001), indicating a slight but meaningful increase in overall risk levels across the 67 countries following recalibration. Among the key aspects of the index —Hazard and Exposure, Vulnerability, and Coping capacity —the difference in Vulnerability scores (mean difference = -0.32; 95% CI: -0.44, -0.21; p-value < 0.000) and Coping capacity (mean difference = -0.18; 95% CI: -0.23, -0.12; p-value < 0.000) were significant. Table 3 presents paired t-test results for risk scores before and after recalibration.
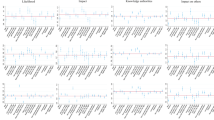
A comparative analysis of the original and recalibrated INFORM Risk Index, along with its corresponding regional rankings, was also performed. South Asia and East Africa exhibit the highest variability in risk differences, while regions like the Middle East and North Africa have relatively lower variability in recalibrated risk scores. Furthermore, South Asia and East Africa have some of the most significant changes in ranking positions (Figs. 1 and 2).

(a) presents the original and recalibrated INFORM Risk Index by region, while (b) shows the distribution of INFORM Risk Index differences by region. (c) depicts the original and updated INFORM Risk Index rankings by region, and (d) represents the rank differences by region.
The Wilcoxon signed-rank test further demonstrated a significant change in rank positions (z = 2.36, p = 0.018), suggesting that recalibration affected the relative rankings of countries, likely due to adjustments for vulnerable populations. Despite this shift, Spearman’s rank correlation (ρ = 0.994, < 0.001) indicated strong preservation of the original rank order, highlighting that while recalibration impacted ranks, it did not drastically alter the relative order among countries. Table 4 presents the Wilcoxon Signed-Rank Test for original and updated rank scores. Moreover, a slight shift was observed in risk scores among the countries after recalibration.

The scattered distribution of risk scores before and after calibration.
Country-level scores and ranking
The change in score varied from 0.1 to 0.6 in 52 (77.6%) countries and remained unchanged in 15 (22.4%) countries. The two countries that showed the highest change of 0.6-point in the score include Madagascar, where the risk index rose from 5.5 to 6.1, resulting in a drop in the ranking from position 27 to position 25 and Zimbabwe, which showed an increase in risk index, from 4.1 to 4.7, leading to a fall in the ranking from position 65 to position 45. In the case of Pakistan, the index changed to a 0.5-point increase in its risk index, from 6.1 to 6.6, maintaining its ranking at position 23. Further, six countries showed a 0.4-point increase: Bhutan’s risk index increased from 2.8 to 3.2, resulting in a change in ranking from position 124 to position 98, and Djibouti’s risk index rose from 4.9 to 5.3, with a change in ranking from 37 to 30. Mali’s risk index increased from 6.8 to 7.2, with a ranking shift from 15 to 11. Nepal’s index increased from 4.1 to 4.5, lowering the ranking from 65 to 53, and Saudi Arabia’s index rose from 3.6 to 4.0, resulting in a ranking shift from 81 to 74. Six countries showed 0.3-point increases in their risk indices. Algeria’s index rose from 3.6 to 3.9, with a change ranging from 81 to 76. Bangladesh’s index increased from 5.7 to 6.0, with a slight ranking change from 25 to 26. Burundi’s index increased from 5.6 to 5.9, resulting in a ranking alteration from 26 to 27. India’s index rose from 5.3 to 5.6, with a slight switch in ranking from 29 to 28. Niger had an increase in its index from 6.6 to 6.9, leading to a ranking of 16 from 19. Syria’s index increased from 7.2 to 7.5, ranking at 9. A total of 15 Countries showed a change of 0.2 points, including Afghanistan, Cameroon, Chad, Ethiopia, Eritrea, Guinea, Iran, Iraq, Kenya, Lebanon, Morocco, Nigeria, Palestine, Sierra Leone, and Somalia. Moreover, 22 countries had a 0.1-point change, which includes Angola, Benin, Burkina Faso, Central African Republic, Congo, Congo DR, Egypt, Gabon, Gambia, Ghana, Liberia, Libya, Mozambique, Oman, Rwanda, South Sudan, Sudan, Tanzania, Togo, Tunisia, Yemen. The remaining 22 countries showed no change in their risk indices. Although a few countries showed changes in ranking, such as Equatorial Guinea from 104 to 105, Jordan from 76 to 79, Kuwait from 139 to 140, and Mauritania from 58 to 63.
The changes were mainly driven by adjustments in the dimensions related to hazard and exposure, i.e., the number exposed to natural and human-made disasters, or the number expected to be exposed, the population’s vulnerability and poor factors contributing to a lack of coping capacity for the population of interest. Hazard and exposure increased in 16 (23.9%) countries, ranging from 0.1 to 0.4, decreased in 15 (22.4%) countries, ranging from 0.1 to 0.2 and remained unchanged in 36 (53.7%) countries. Vulnerability increased in 48 (71.6%) countries, ranging from 0.1 to 2.3, decreased in 3 (4.5%) countries, ranging from 0.1 to 0.3 and remained unchanged in 16 (23.9%) countries. The countries with the highest change in vulnerability ranged from 1.0 to 2.3 and included Madagascar, Mali, Pakistan, Togo, Zambia, and Zimbabwe. The lack of coping capacity for the target population increased in 52 (77.6%) countries, decreased in only one country and remained unchanged in 14 (20.9%) countries. Bangladesh, Bhutan, India, Nepal, and Pakistan are the top countries experiencing an increase in the score due to a lack of coping capacity. Table 5 presents a detailed overview of changes in scores for the three dimensions: hazard and exposure, vulnerability and lack of coping capacity.
Furthermore, Bahrain, Mauritius, Qatar, Seychelles, and the United Arab Emirates remained in the “very low” classification, with no change except for a 0.1-point change in Seychelles. Equatorial Guinea, Kuwait, Maldives, Oman, São Tomé and Principe, Sri Lanka, and Tunisia, originally classified as “low”, remained in the “low” classification with no change in score, except for Oman and Tunisia, which each increased by 0.1 point. Benin, Comoros, Gabon, Gambia, Ghana, Guinea, Jordan, Lebanon, Liberia, Malawi, Mauritania, Morocco, Nepal, Palestine, Rwanda, Saudi Arabia, Senegal, Sierra Leone, Togo, Zambia, and Zimbabwe remained in the “medium” classification. Comoros, Jordan, Malawi, Mauritania, and Senegal showed no change.
Discussion
When accounting for women and children aged 0–14, the shift observed in the INFORM Risk Index and the risk profiles of 67 countries indicates that ultra vulnerabilities exist within many countries when considering women and children. The recalibration has revealed essential shifts in assessing country-level risks, with a statistically significant increase in overall scores. This increase, though modest, suggests a heightened sensitivity of the recalibrated index to underlying risk factors, potentially offering a critical understanding of country vulnerabilities. The substantial changes in vulnerability and coping capacity are particularly remarkable, as recalibration has effectively captured critical socio-economic factors and resilience limitations that may amplify risk levels. The adjustment, which incorporates gender-specific indicators, provides ways to see how risk assessment and ranking change when gender and age are factored in, which could potentially impact decision-making. The recalibration of the INFORM Risk Index to specifically address the vulnerabilities of women and children has revealed substantial shifts in the risk landscape. This study highlighted that significant changes in risk classification are predominantly driven by increased vulnerability and diminished coping capacities rather than exposure to hazards alone. The refined indicators showed these populations’ profound socio-economic and institutional challenges, often masked in broader assessments. These findings underscore the critical need for disaster risk management frameworks to incorporate gender-specific and age-specific data, ensuring that the heightened risks to women and children are accurately captured and addressed.
Countries with initially “very high” or “high” indices tend to exhibit a greater impact on vulnerability due to preexisting disparities and inadequate coping mechanisms for dealing with complex emergencies affecting women and children. Changes in risk scores need to be understood and evaluated within the specific context of individual countries. Thus, countries like Afghanistan, the Central African Republic, Somalia, and South Sudan showed a change in the index but already had a very high index of greater than 8.0. These countries have a long history of protracted conflict, political instability, severe drought, food insecurity, and natural disasters38,52. Ethiopia’s significant increase in exposure to conflict and natural disasters, such as recurrent droughts, floods, and northern conflict, increases vulnerabilities and coping capacity57. These compounded risks have severe implications for women and children, who are particularly vulnerable to disruptions in health services, Water Sanitation and Hygiene (WASH), nutrition, and safety58. Madagascar’s high hazard index underscores the urgent need for resilient infrastructure and effective early warning systems to safeguard these populations against frequent cyclones and natural disasters59. The rising vulnerability indices in Nigeria, Zimbabwe, and Mali highlight worsening socio-economic conditions that exacerbate disaster risks38,52,60. For instance, Nigeria’s increasing vulnerability aligns with findings that socio-economic disparities and inadequate social safety nets significantly heighten disaster susceptibility among women and children38,52,61. Zimbabwe’s escalating poverty and health inequities underscore the urgent need for enhanced social protection mechanisms60. Mali’s socio-economic challenges and ongoing conflict emphasize the necessity for integrated development and humanitarian interventions62. Critical institutional and infrastructural resilience gaps exist in Madagascar and Pakistan. Madagascar’s rise in the coping capacity score reflects reduced institutional ability to manage and recover from hazards63, In contrast, Pakistan’s decline in institutional and infrastructural resilience highlights the need to strengthen institutions and social protection to enhance overall coping capacity64,65,66,67,68,69. Further, Pakistan is a prone country, and the government has still not fully recovered from the impact of devastating floods in 2022, where data suggest that 80% of the affected were women and children70.
The recalibrated index’s focus on gender and age-specific indicators has revealed critical gaps in data availability, particularly the scarcity of gender-disaggregated data. Whether this represented a true shift in risk requires further validation through in-depth data inclusion for more vulnerable groups and selecting more specific indicators in the index. Many indicators in existing data sources do not disaggregate by gender, making it challenging to capture the unique vulnerabilities of women and children accurately. This limitation highlights the need for improved data collection practices that prioritize gender and age disaggregation, as emphasized by UN Women and other organizations advocating for gender-sensitive data. Although not the primary outcome, this study indicated that investment in governance and institutional frameworks is vital to enhancing disaster preparedness and response capabilities. Countries with significant increases in their risk indices demonstrate the urgent need for comprehensive social protection programs, improved access to healthcare and education, and economic development initiatives. These measures are essential for reducing disparities and enhancing community resilience. This approach provides a better understanding of their vulnerability, which is often missed in broader assessments. However, the need for comprehensive gender-disaggregated data remains a significant limitation. Many data sources providing gender data still have missing indicators or indicators unavailable for the specified time frame. Given the open-source structure of the INFORM Risk Index and its increasing use at subnational levels, the recalibration method described in this study can serve as a flexible framework for adaptation in other regions or populations. We recommend that future applications define a structured process for selecting indicators based on the specific vulnerabilities of the population under study. This may include grouping indicators into thematic domains such as environmental exposure, socio-economic status, legal protection, health access, or education. We also suggest compiling a repository of data sources that are regularly updated, gender- or age-disaggregated, and aligned with international standards. Such guidance would strengthen consistency across different applications and help address limitations related to the current index’s limited representation of social and gendered impacts.
Future research should focus on developing robust methodologies for gender-sensitive data collection and analysis to ensure that the distinct needs of women and children are fully captured and addressed in disaster risk reduction policies and practices. There is a strong need for such approaches to consider other indicators that can improve the validity of this study with more robustness and accuracy. It is essential to consider additional indicators grouped into several coherent categories to enhance our study’s validity, robustness, and accuracy. These include violence and conflict impact (gender-based violence and child abuse in conflict zones, accurate numbers of women and children with IDP and refugee status), environmental factors (levels of air and water pollution), educational access and outcomes (primary and secondary school enrollment), nutritional status (prevalence of stunting, underweight, and wasting among children aged 0–14 years, prevalence of undernutrition among women and adolescent girls), healthcare access (access to prenatal, skilled birth attendance, and postnatal healthcare, access to sexual and reproductive health services including menstrual hygiene and safe abortion care), social and legal protection (child marriage rates, access to social protection services, orphanhood rates and child dependency ratios, availability of mental health support services for women and children, availability of legal protection), and childcare and support services (access to childcare services). Organizing these indicators into these categories ensures a more coherent and rigorous approach to improving the study’s comprehensiveness and accuracy. The explicit inclusion of these indicators will help better understand the more granular needs of these vulnerable groups at the country level. Moreover, strengthening institutional capacities to manage and utilize this data effectively will be crucial in shaping responsive and inclusive disaster management strategies. Investing in governance and institutional frameworks to enhance disaster preparedness and response capabilities is essential. Comprehensive social protection programs, improved access to healthcare and education, and economic development initiatives are vital for reducing disparities and enhancing community resilience. Developing infrastructure that can withstand natural disasters and support rapid recovery is also critical, not only for immediate protection but also for long-term sustainable development.
While the recalibrated INFORM Risk Index provides critical insights into the vulnerabilities of women and children, validating these adjusted scores remains a significant challenge due to the scarcity of comprehensive, gender-disaggregated data. This limitation underscores the need for continuous and robust data collection and methodology refinement to ensure the reliability and accuracy of risk assessments. Furthermore, there is limited availability of child-specific data in the original INFORM Risk Index, with most indicators reflecting aggregated population-level data or adult experiences. As a result, recalibrating the index to reflect children’s vulnerability was constrained. In several cases, we used indicators specific to women as a proxy for children, based on their caregiving roles and shared exposure in emergencies. While this was grounded in existing literature, it does not fully capture the independent vulnerabilities of children. We recommend that future revisions of risk indices should prioritize the inclusion of age-disaggregated indicators to enable a more precise understanding of risk among children. Another limitation of this study relates to the use of a uniform standard multiplier to estimate the proportion of affected women and children. This approach was based on a synthesis of global estimates; however, it does not account for variations in demographic composition, local risk profiles, or differential impacts of various types of hazards. Future recalibration efforts should prioritize the integration of country-specific or hazard-specific proportions where data allow, to improve the accuracy and sensitivity of risk estimation for vulnerable groups.
Another limitation of this study relates to the use of a uniform standard multiplier to estimate the proportion of affected women and children. This approach was based on a synthesis of global estimates; however, it does not account for variations in demographic composition, local risk profiles, or differential impacts of various types of hazards. Future recalibration efforts should prioritize the integration of country-specific or hazard-specific proportions where data allow, to improve the accuracy and sensitivity of risk estimation for vulnerable groups.
Conclusion
In conclusion, the recalibrated INFORM Risk Index highlights the critical vulnerabilities of women and children in high-risk countries, underscoring the need for targeted, gender-sensitive interventions. Addressing the specific risks will enable policymakers and humanitarian organizations to enhance resilience and reduce overall risk profiles for these vulnerable populations. This better understanding of risks and their associated consequences is essential for developing practical, inclusive, and sustainable disaster risk management strategies. This recalibration initiative highlights the value of refining established risk indices to reflect the realities of marginalized populations and demonstrates the potential of such approaches to inform more inclusive disaster preparedness and response planning.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
References
Graveline, M. H. & Germain, D. Disaster risk resilience: Conceptual evolution, key issues, and opportunities. Int. J. Disaster Risk Sci. 13 (3), 330–341 (2022).
Yodmani, S. Disaster Risk Management and Vulnerability Reduction: Protecting the Poor (The Center New York, 2001).
Scolobig, A., Prior, T., Schröter, D., Jörin, J. & Patt, A. Towards people-centred approaches for effective disaster risk management: Balancing rhetoric with reality. Int. J. Disaster Risk Reduct. 12, 202–212 (2015).
Grasso, V. F. & Singh, A. Early warning systems: State-of-art analysis and future directions. Draft Rep. UNEP. 1, 7 (2011).
Thomalla, F. & Larsen, R. K. Resilience in the context of tsunami early warning systems and community disaster preparedness in the Indian ocean region. Environ. Hazards. 9 (3), 249–265 (2010).
Li, T. et al. Data-driven techniques in disaster information management. ACM Comput. Surv. CSUR. 50 (1), 1–45 (2017).
Qadir, J. et al. Crisis analytics: Big data-driven crisis response. J. Int. Humanit. Action. 1, 1–21 (2016).
Saunders, W. S., Kelly, S., Paisley, S. & Clarke, L. B. Progress toward implementing the Sendai framework, the Paris agreement, and the sustainable development goals: Policy from Aotearoa new Zealand. Int. J. Disaster Risk Sci. 11 (2), 190–205 (2020).
Marin-Ferrer, M., Vernaccini, L. & Poljansek, K. Index for risk management - INFORM: concept and methodology, version 2017. [Internet]. LU: European Commission. Joint Research Centre.; [cited 2024 Jul 18]. Available from: https://data.europa.eu/doi/ (2017). https://doi.org/10.2760/094023
De Groeve, T., Poljansek, K. & Vernaccini, L. Index for risk management-INFORM. JRC Sci. Policy Rep. Bruss. Eur. Comm. (2015).
Inter-Agency Standing Committee and the European Commission. : 10 years of INFORM [Internet]. Luxembourg: Publications Office of the European Union; [cited 2023 Dec 17]. INFORM REPORT (2024). Available from: https://op.europa.eu/en/publication-detail/-/publication/b0ac7f32-e4f1-11ee-8b2b-01aa75ed71a1/language-en
Disaster Risk Management Knowledge Centre, European Union. DRMKC - INFORM. Results and Data [Internet]. [cited 2023 Oct 8]. Available from: https://drmkc.jrc.ec.europa.eu/inform-index/INFORM-Risk/Results-and-data/moduleId/1782/id/469/controller/Admin/action/Results
Brown, S., Budimir, M., Crawford, U., Clements, S. & Sneddon, A. R., and Gender and Age Inequality of Disaster Risk: Research Paper [Internet]. UNICEF and UN Women; 2019 [cited 2023 Oct 14]. Available from: https://www.unwomen.org/sites/default/files/2021-11/Policy-brief-Gender-and-age-inequality-of-disaster-risk-en.pdf
Källmark, A. Maternal health care in natural disasters: A study on the International Federation of the Red Cross’s maternal health care in flooding disaster relief. (2020).
Peterman, A. et al. Pandemics and violence against women and children. Vol. 528. Center for Global Development Washington, DC (2020).
Mueller, N. Public Health Emergency Preparedness and Maternal and Child Health: Recommendations for the Local Health Department. (2013).
Alston, M. Women and adaptation. Wiley Interdiscip Rev. Clim. Change. 4 (5), 351–358 (2013).
Sule, F. A. et al. Examining vulnerability and resilience in maternal, newborn and child health through a gender lens in low-income and middle-income countries: a scoping review. BMJ Glob Health. 7 (4), e007426 (2022).
Erman, A., De Vries Robbe, S. A., Thies, S. F., Kabir, K. & Maruo, M. Gender dimensions of disaster risk and resilience: Existing evidence [Internet]. World Bank; 2021 [cited 2024 Jun 2]. Available from: https://openknowledge.worldbank.org/server/api/core/bitstreams/80f2e78e-f04f-5a59-86a6-9cfe6bcd7b87/content
Alam, K. & Rahman, M. H. The role of women in disaster resilience. In: Handbook of Disaster Risk Reduction & Management. World Scientific; 697–719. (2018).
Kousky, C. Impacts of natural disasters on children. Future Child. 26:73–92. (2016).
Masten, A. S. & Osofsky, J. D. Disasters and their impact on child development: introduction to the special section. Child. Dev. 81 (4), 1029–1039 (2010).
Neumayer, E. & Plümper, T. The gendered nature of natural disasters: The impact of catastrophic events on the gender gap in life expectancy, 1981–2002. Ann. Assoc. Am. Geogr. 97 (3), 551–566 (2007).
Ikeda, K. Gender differences in human loss and vulnerability in natural disasters: A case study from Bangladesh. Indian J. Gend. Stud. 2 (2), 171–193 (1995).
Cas, A. G., Frankenberg, E., Suriastini, W. & Thomas, D. The impact of parental death on child Well-being: Evidence from the Indian ocean tsunami. Demography 51 (2), 437–457 (2014).
Sepahvand, H., Hashtjini, M. M., Salesi, M., Sahraei, H. & Jahromi, G. P. Prevalence of post-traumatic stress disorder (PTSD) in Iranian population following disasters and wars: A systematic review and meta-analysis. Iran. J. Psychiatry Behav. Sci. ;13(1), e66124 (2019).
Bendavid, E. et al. The effects of armed conflict on the health of women and children. Lancet 397 (10273), 522–532 (2021).
Chi, P. C. Impact of armed conflict on maternal and reproductive health in sub-Saharan Africa.; (2016).
UNHCR. Non-discrimination: groups in vulnerable situations. Special Rapporteur on the right to health [Internet]. [cited 2023 Jun 5]. Available from: https://www.ohchr.org/en/special-procedures/sr-health/non-discrimination-groups-vulnerable-situations
Crock, M. The protection of vulnerable groups. In: Research Handbook on Disasters and International Law. Edward Elgar Publishing: Cheltenham; 383–405. (2016).
Kuran, C. H. A. et al. Vulnerability and vulnerable groups from an intersectionality perspective. Int. J. Disaster Risk Reduct. 50, 101826 (2020).
UNHCR-IDC. Vulnerability Screening Tool - Identifying and addressing vulnerability: A tool for asylum and migration systems [Internet]. Division of International Protection United Nations High Commissioner for Refugees; 2016 [cited 2023 Jun 5]. Available from: https://www.unhcr.org/media/36038
Cannon, T. Reducing People’s Vulnerability To Natural Hazards Communities and Resilience9292300806 (WIDER Research Paper, 2008). Report No.
Coleman, N., Esmalian, A. & Mostafavi, A. Equitable resilience in infrastructure systems: Empirical assessment of disparities in hardship experiences of vulnerable populations during service disruptions. Nat. Hazards Rev. 21 (4), 04020034 (2020).
Bardosh, K. L., Ryan, S. J., Ebi, K., Welburn, S. & Singer, B. Addressing vulnerability, Building resilience: Community-based adaptation to vector-borne diseases in the context of global change. Infect. Dis. Poverty. 6, 1–21 (2017).
Sharma, B. B., Pemberton, H. R., Tonui, B. & Ramos, B. Responding to perinatal health and services using an intersectional framework at times of natural disasters: A systematic review. Int. J. Disaster Risk Reduct. 76, 102958 (2022).
Brunson, J. Maternal, newborn, and child health after the 2015 Nepal earthquakes: An investigation of the long-term gendered impacts of disasters. Matern Child. Health J. 21, 2267–2273 (2017).
United Nations Office for the Coordination of Humanitarian Affairs [OCHA]. Global Humanitarian Overview 2024 [Internet]. 2024 [cited 2024 May 17]. Available from: https://www.unocha.org/publications/report/world/global-humanitarian-overview-2024-enarfres
UN Women. Facts and figures: Humanitarian action [Internet]. 2024 [cited 2024 Jul 11]. Available from: https://www.unwomen.org/en/what-we-do/humanitarian-action/facts-and-figures
UN Women and United Nations Department of Economic and Social Affairs, Statistics Division. The Gender Snapshot 2023 [Internet]. 2023 [cited 2024 Jun 17]. Available from: https://bit.ly/gender-snapshot-2023
United Nations Children’s Fund (Unicef). UNICEF Humanitarian Action for Children 2024 Overview [Internet]. 2024 [cited 2024 Jul 11]. Available from: https://www.unicef.org/media/149906/file/Humanitarian-Action-for-Children-2024-Overview.pdf
Sahoo, K. C. et al. Challenges in Maternal and Child Health Services Delivery and Access during Pandemics or Public Health Disasters in low-and middle-income Countries: a Systematic Reviewp. 828 (In MDPI, 2021).
UN Women. UN Women Data Hub [Internet]. [cited 2023 Oct 13]. Available from: https://data.unwomen.org/data-portal
The Demographic and Health Surveys. The DHS Program. Gender Dashboard [Internet]. [cited 2023 Oct 29]. Available from: https://dhsprogram.com/data/visualizations/gender-dashboard.cfm
Global Change Data Lab. Our World in Data [Internet]. [cited 2023 Oct 13]. Available from: https://ourworldindata.org/human-development-index
World Bank Group. Gender Data Portal [Internet]. [cited 2023 Nov 11]. Available from: https://genderdata.worldbank.org/en/economies
Peek, L., Abramson, D. M., Cox, R. S., Fothergill, A. & Tobin, J. Children and disasters. Handb. Disaster Res. ;243–262. (2018).
Kiragu, A. W. et al. Pediatric trauma care in low resource settings: Challenges, opportunities, and solutions. Front. Pediatr. 6, 155 (2018).
United Nations Population Fund. Protecting Women in Emergency Situations [Internet]. 2023 [cited 2023 Oct 16]. Available from: https://www.unfpa.org/resources/protecting-women-emergency-situations
Hamidazada, M., Cruz, A. M. & Yokomatsu, M. Vulnerability factors of Afghan rural women to disasters. Int. J. Disaster Risk Sci. 10 (4), 573–590 (2019).
UN Refugee Agency (UNHCR). Global Trends - Forced Displacement in 2019 [Internet]. 2019 [cited 2023 Oct 14]. Available from: https://www.unhcr.org/flagship-reports/globaltrends/globaltrends2019/
United Nations Office for the Coordination of Humanitarian Affairs (OCHA). Global Humanitarian Overview 2019 [Internet]. 2019 [cited 2023 Oct 17]. Available from: https://reliefweb.int/report/world/global-humanitarian-overview-2019-enaresfrzh
UN Refugee Agency (UNHCR). UNHCR Refugee Data Finder. [Internet]. [cited 2023 Nov 13]. Available from: https://www.unhcr.org/refugee-statistics/
Europian Union. European Civil Protection and Humanitarian Aid Operations [Internet]. [cited 2023 Nov 3]. Available from: https://civil-protection-humanitarian-aid.ec.europa.eu/where/asia-and-pacific_en
Internal Displacement Monitoring Center. Country Profile [Internet]. [cited 2024 Oct 29]. Available from: https://www.internal-displacement.org/countries/algeria/
United Nations Department of Economic and Social Affairs. : Summary of Results.Population Division. World Population Prospects (2022).
Adaawen, S., Rademacher-Schulz, C., Schraven, B. & Segadlo, N. Drought, migration, and conflict in sub-Saharan africa: What are the links and policy options? Curr. Dir. Water Scarcity Res. 2, 15–31 (2019).
Gesesew, H. et al. The impact of war on the health system of the Tigray region in ethiopia: An assessment. BMJ Glob Health. 6 (11), e007328 (2021).
Randriamparany, S. T. & Randrianalijaona, T. M. The vulnerability of Antandroy women to droughts in Ambovombe Androy (Madagascar). Int. J. Disaster Risk Reduct. 72, 102821 (2022).
Nyandoro, M. & Hatti, N. Poverty and the politics of poverty in independent zimbabwe, 1980–2017. Soc. Sci. Spectr. 4 (2), 56–74 (2019).
Eniwotu, AR, Otite A. The ripple effects of flooding & on women in Nigeria. J. Public. Adm. Finance Law; (2023).
Tronc, E., Grace, R. & Nahikian, A. Realities and Myths of the’triple nexus’: local perspectives on peacebuilding, development, and humanitarian action in Mali. Humanit. Action Frontline Field Anal. Ser.; (2019).
Hochrainer-Stigler, S., Mechler, R. & Mochizuki, J. A risk management tool for tackling country-wide contingent disasters: A case study on Madagascar. Environ. Model. Softw. 72, 44–55 (2015).
Khan, N. A., Gao, Q. & Abid, M. Public institutions’ capacities regarding climate change adaptation and risk management support in agriculture: The case of Punjab province, Pakistan. Sci. Rep. 10 (1), 14111 (2020).
Shah, A. A. et al. Current capacities, preparedness and needs of local institutions in dealing with disaster risk reduction in Khyber pakhtunkhwa, Pakistan. Int. J. Disaster Risk Reduct. 34, 165–172 (2019).
Adnan, M. et al. Addressing current climate issues in pakistan: An opportunity for a sustainable future. Environ. Chall.; 15, 100887. (2024).
Ministry of Climate Chnage and Environmental Coordination. National Adaptation Plan Pakistan 2023 [Internet]. 2023 [cited 2024 May 6]. Available from: https://unfccc.int/sites/default/files/resource/National_Adaptation_Plan_Pakistan.pdf
Riaz, K., Ahmad, M., Gul, S., Malik, M. H. B. A. & Rehman, M. E. U. Climate change and its implications on health and the healthcare system: A perspective from Pakistan. Ann. Med. Surg.; 81. (2022).
Zangerl, K. E. et al. Child health prioritisation in National adaptation policies on climate change: A policy document analysis across 160 countries. Lancet Child. Adolesc. Health. 8 (7), 532–544 (2024).
The Government of Pakistan, Asian Development Bank, European Union, United Nations Development Programme, World Bank. Pakistan Floods 2022 Post-Disaster Needs Assessment [Internet]. 2022 [cited 2024 May 13]. Available from: https://thedocs.worldbank.org/en/doc/4a0114eb7d1cecbbbf2f65c5ce0789db-0310012022/original/Pakistan-Floods-2022-PDNA-Main-Report.pdf
Acknowledgements
This manuscript results from a study conducted in the International PhD in Global Health Humanitarian Aid and Disaster Medicine framework, jointly organized by the Università del Piemonte Orientale (UPO).Further, this scoping work was conducted under the scope of grant supported by Bill & Melinda Gates Foundation [Grant Number INV-061145]. The funder has played no role in the drafting of the manuscript or the decision to submit it for publication.
Funding
This study was supported by the scope under the grant from the Bill & Melinda Gates Foundation [Grant Number INV-061145]. The funder played no role in drafting the manuscript or in the decision to submit it for publication.
Author information
Authors and Affiliations
Contributions
Yasir Shafiq: Conceptualization, Methodology, Formal analysis, Investigation, Data Curation, Writing - Original Draft, Writing - Review & Editing, Visualization, Funding Ameer Muhammad: Formal analysis, Writing - Original Draft, Writing - Review & EditingSaba Noor: Writing - Review & EditingKantesh Kumar: Writing - Review & EditingUme e Aimen Chhipa: Writing - Review & EditingMartina Valente: Writing - Review & EditingJunaid Razzak: Writing - Review & EditingLuca Ragazzoni: Writing - Review & EditingFrancesco Barone-Adesi: Writing - Review & EditingPhuong N Pham: Conceptualization, Writing - Review & Editing, Supervision.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shafiq, Y., Muhammad, A., Noor, S. et al. The modification of risk assessment ranking when considering the female population and children in the INFORM risk index for selected countries. Sci Rep 15, 26527 (2025). https://doi.org/10.1038/s41598-025-10490-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-10490-4
