
Abstract
Climate change and extreme weather are increasing global disease burdens, but the association between weather conditions and hospital admissions in Macau remains unclear. This study was performed in the context of Macau, China. It analyzed daily hospital admissions from Macau’s hospitals with emergency departments and local meteorological data (2017–2022) using distributed lag nonlinear models with 21-day lag effects. Results revealed that 14.5 °C was associated with the lowest risk of hospital admissions. Colder temperatures exhibited prolonged effects, elevating risks for up to 21 days, while hotter temperatures’ impacts were shorter. Compared with mean relative humidity (81%), the risk was lowest when relative humidity was 33% (RR = 0.87, 95% CI: 0.66–1.14), and the risk was highest when relative humidity was 100% (RR = 1.50, 95% CI: 1.15–1.94). The effects of these weather conditions on hospital admissions varied by disease and age, with smaller differences between sexes. The increased hospital admissions in Macau are associated with hotter and colder temperatures, as well as humidity. As climate change intensifies weather extremes, healthcare systems may face escalating demands, necessitating targeted prevention strategies for high-risk groups and optimized resource allocation.
Similar content being viewed by others

Introduction
The Macau Special Administrative Region (SAR) of China (longitude 113°31’41.4’’~113°37’48.5’’, latitude 22°04’36.0’’~22°13’01.3’’) is situated on the west bank of the Pearl River Estuary. Macau is adjacent to Guangdong Province in the southern region of China, across the sea from Hong Kong. Macau comprises three areas: the Macau Peninsula, Taipa Island, and Coloane, with a total area of approximately 32.9 square kilometers1. The terrain of Macau is predominantly flat, although there are a few hills. The highest point is Mount Tasiktang on Coloane Island.
Over the past 20 years, Macau has undergone substantial changes in weather conditions, including more extreme temperatures, as well as high and low humidity. According to the Macau Meteorological and Geophysical Bureau2the average annual temperature has exhibited an upward trend, consistent with the global warming patterns, with an increase of approximately 0.2 °C per decade. Relative humidity displays a more complex pattern, characterized by extremes during seasonal variations. Notably, during the summer months, relative humidity increases compared to the previous decades3.
These weather changes substantially impact on human health, influencing both increases in mortality and morbidity rates. Between 2000 and 2019, non-optimal ambient temperatures were responsible for over 5 million deaths worldwide4. An example of this is that high heat exposure accounts for approximately 1% of overall mortality5. Numerous studies have demonstrated nonlinear relationships between extreme temperatures and poorer health outcomes, indicating that both excessively high and low temperatures elevate the risk of disease4,6,7. One study4 demonstrated that both low and high temperatures in Thailand were linked to increased hospital admissions for various diseases, particularly among women, children, and adolescents. Despite these preliminary findings, evidence of the association between temperature and hospital admissions in China remains limited to date.
Relative humidity also plays a crucial role in health outcomes. High humidity levels can hinder the body’s ability to cool itself through sweating, thereby increasing the risk of heat-related illnesses. Conversely, low humidity can result in dry skin, respiratory irritation, and increased susceptibility to respiratory infections8. Some studies demonstrated that higher relative humidity was associated with fewer hospital admissions, while lower relative humidity correlated with increased hospital admissions9,10. Additionally, a study10 indicated that low humidity often acts synergistically with cold exposure to substantially elevate the risk of cardiovascular disease. It is important to note, however, that the association between relative humidity and health remains largely understudied globally11.
The World Health Organization (WHO) emphasizes that changes in weather conditions, including temperature and relative humidity, pose a substantial threat to human health by increasing the frequency and intensity of extreme weather events12. Recognizing the need for a deeper understanding of this critical issue, our study aimed to investigate the association between various weather conditions and daily hospital admissions in Macau from 2017 to 2022, considering its unique climate and public health challenges.
Materials and methods
Study background
According to the Census and Statistics Department of Macau, the city’s resident population in 2022 is estimated to be around 683,000, with a population density of 20,620 inhabitants per square kilometer, making it one of the most densely populated areas globally1. Macau has a subtropical monsoon climate influenced by both the ocean and the monsoon, with a dual season dominant. Summer is usually hot and humid, with perceived temperatures often above 40 °C and frequent thunderstorms; winter is mild with little rain, but cold waves can cause temperatures to drop over 10 °C in a day; spring and autumn are shorter in duration2 .The average annual temperature is approximately 22 °C, and the annual precipitation is around 2,000 mm, resulting in high relative humidity. Tropical cyclones mainly occur from May to November, peaking from July to September, with an average of five events each year1,2. Strong typhoons can trigger storm surges, with destructive power increasing as wind speeds rise near the coast1,2. The extremely high population density and fragile climate environment increase the likelihood of adverse health outcomes; therefore, timely weather exposure warnings are essential.
Health data
-
We collected all daily hospital admissions records, regardless of patient age, from computerized case databases at Kiang Wu Hospital and Centro Hospitalar Conde Da São Januário dos Serviços de Saúde in Macau. These two hospitals are the only two in Macau with accident and emergency departments. We extracted the primary reason for admission using International Classification of Diseases, Tenth Revision (ICD-10) codes and categorized these into broad disease types, Neoplasms (C00-D48), Endocrine, nutritional, and metabolic diseases (E00-E89), Diseases of the circulatory system (I00-I99), Diseases of the respiratory system (J00-J99), Diseases of the musculoskeletal system and connective tissue (M00-M99), and Other and unspecified effects of external causes (T66-T78). The health data collected included the primary reason for hospital attendance upon admission, admission date, and the patient’s sex and age group (0–20, 21–70, 70 plus). Data were cleaned by removing cases with missing admission dates, sex, and age information (22 cases). This retrospective study used fully de-identified patient data, with all identifiers (e.g., name, date of birth) removed. As this study was intended to benefit the public health of Macau and involved no more than minimal risk to participants, the University of Macau Research Committee (SSHRE24-APP087-FHS; 09/08/2024) waived the requirement for informed consent. This study adhered to the ethical recommendations of the Declaration of Helsinki on the use of data13which permits the exemption of informed consent for de-identified retrospective data analyses under strict ethical oversight. We ensured data privacy and confidentiality throughout the study. Weather and air pollution data.
Daily weather and air pollution data were obtained from a database collected during the same period by the Macau Meteorological and Geophysical Bureau and the Macau Environmental Protection Bureau14. The data recorded included daily mean temperature, daily mean relative humidity, daily precipitation, daily average particulate matter 10 (PM10) concentration, daily peak 1-hour average nitrogen dioxide (NO2) concentration, and daily average sulfur dioxide (SO2) concentration, as measured at the meteorological and air pollutant monitoring stations in Macau. The weather data were taken from an average of 10 weather stations to reflect the average weather conditions for the entire region. Air pollution data were taken from an average of 6 air pollutant monitoring stations to represent the average air pollution situation. Because of the small size of the urban area of Macau and the small difference in measurement results among the stations, we used the average data from all the stations. All data was complete except for August 4, 2017, which had missing PM10 values.
Statistical analyses
Descriptive analyses
We used R version 4.4.1 for data analysis and descriptive statistics, including counts, percentages, means, and standard deviations (SD) for weather conditions, air pollutants, and the number of cause-specific hospital admissions. The R package ‘ggplot2’ was employed to visualize daily weather and air pollutants data from 2017 to 2022, while the ‘mice’ package was used to perform multiple imputations for the missing PM10 data.
Estimation of associations between hospital admissions and weather conditions
We conducted a time series analysis to examine the associations between daily temperature, relative humidity, and hospital admissions. Due to the over-discretization of daily hospital admissions, this analysis employed generalized linear models (GLM) based on negative binomial distributions. For the lag effects and nonlinear associations, we employed distributed lag nonlinear models (DLNM) to deal with them. We built two two-dimensional matrices for temperature-lag times and relative humidity-lag times using crossbasis functions from the R package ‘dlnm’15,16.
For exposure-response associations, we used natural cubic splines (three equal internal knots for temperature; three internal knots at the 10th, 75th, and 90th percentiles for relative humidity ) to capture nonlinearities and directional changes in weather conditions-hospitalization relationships17,18. For lag-response associations, we applied natural cubic splines with intercepts and four equidistant internal knots on a log scale to model a 21-day lag on hospital admissions, allowing for flexibility19. We addressed seasonality and long-term trends with a natural cubic spline with six degrees of freedom (\(\:df\)) per year and included categorical variables representing the days of the week and dichotomous variables representing public holidays to address the impact of weekday and holiday patterns on the model, respectively. We also included PM10, NO2, and SO2 as covariates, using natural cubic splines with \(\:3df\) for these variables. When studying the lag effect of temperature on the hospital admissions, we added the spline function with 3\(\:df\:\)of relative humidity as a covariate to control the co-occurrence in the model (the model for relative humidity also controls the co-occurrence for temperature). We selected the best-fitting model based on the AIC information criterion, likelihood ratio test, and generalized cross-validation7,20. We repeated analyses across subgroups, including disease type, sex, and age groups, to test result robustness.
To investigate the association between hospital admissions and weather conditions (daily mean temperature, relative humidity), we employed a GLM model based on a negative binomial distribution for temperature and relative humidity. For reference level, we designated the temperature corresponding to the lowest risk of hospital admission as the reference point, identifying the minimum risk temperature as 14.5 °C. For relative humidity, we selected the mean value of 81%. Details on the model and sensitivity analysis can be found in full in Supplementary Document 1.
By reporting cumulative effects within lag periods, adjustments for multiple comparisons to a single estimate for each exposure level are made. The contour maps of temperature and relative humidity at each lag time display only the trend to reduce multiplicity effects. Cumulative relative risk ratios quantify the total burden of patients caused by exposure events. To address issues of multiplicity across the exposure-response continuum, simultaneous confidence bands via 1,000 bootstrap resampling were computed21. This approach controls the family-wise error rate at α = 0.05, ensuring 95% confidence that the entire true association curve lies within the band16,18. More details are reported in Supplementary Document 1.
Results
Descriptive analysis
Descriptive statistics of hospital admissions are presented in Table 1. This study included a total of 106,794 admissions from January 1, 2017, to December 31, 2022, of which 18,858 (18%) were due to neoplasms, 29,566 (28%) were related to diseases of the circulatory system, and 48,232 (45%) were attributed to diseases of the respiratory system. Endocrine, nutritional, and metabolic diseases, as well as immune disorders, represented 4% of admissions, and diseases of the musculoskeletal system and connective tissue accounted for 5%. Among the total admissions, 55,542 were male and 51,230 were female, resulting in a male-to-female ratio close to 1.1:1. When stratified by age, 29,091 admissions were for individuals aged 0–20 years, 44,501 for those aged 21–70 years, and 33,197 for individuals aged 70 years or older. Descriptive statistics of daily hospital admissions are presented in Supplementary Document 1.
Descriptive statistics for weather conditions and air pollutants are presented in Table 2. We recorded yearly means of weather conditions in Macau from 2017 to 2022, where the mean temperature was 23.2 °C (SD: 5.1), mean relative humidity was 81% (SD: 11.3), precipitation was 5.4 mm (SD: 17.6), PM10 concentration was 42.6 µg/m³ (SD: 22.4), the peak one-hour NO2 concentration was 50.7 µg/m³ (SD: 28.1), and SO2 concentration of 4.4 µg/m³ (SD: 2.4). Descriptive statistics of daily weather conditions and air pollutants are presented in Supplementary Document 1. The time trends of these variables are also illustrated in Supplementary Document 1, which indicates that they exhibit strong temporal trends and seasonality.
Associations between hospital admissions and temperature
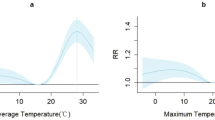
Figure 1 presents the cumulative risk-response curves illustrating the association between daily temperature and hospital admissions, along with a contour map across different lag days. A nonlinear association between admissions at both cold and hot temperatures (Fig. 1A). After 21 cumulative days compared to the minimum risk temperature, the relative risk (RR) of hospital admission in an extremely cold environment (1% of the temperature distribution: 10.3 °C) increased (RR: 1.21, 95% CI: 1.06–1.37). The RR in an extremely hot environment (99% of the temperature distribution: 30.4 °C) increased (RR: 1.42, 95% CI: 1.17–1.73). Figure 1B illustrates the effect of temperature on the risk of hospital admissions at a single lag time; the duration of the cold weather, temperature below 10 °C, appeared to have a sustained increased association of hospital admissions, with cold always remaining positively associated with higher RR, although a brief decrease in the RR brought about by low temperatures on days 2–3. The duration of the high temperatures on increased hospital admissions, above 20 °C, was shorter compared to cold temperatures, with 5 days of increased risk observed. The highest observed risk occurred in hot weather during the first day of lag, after which the risk of heat and hospital admissions continued to decrease with increasing lag time. Results with statistical significance are presented in Supplementary Document 1.

Cumulative risk-response curves and contour map for temperature Notes: a). Plot A shows the exposure-response association between temperature and total hospital admissions. The red lines represent the cumulative exposure-response specific relative risks (RR), and the shaded areas represent the 95% confidence intervals. All confidence intervals account for multiplicity via bootstrap-derived simultaneous inference. b). Plot B shows the exposure-lag-response contour map of temperature with specific RRs. In this plot, darker shades of red color represent larger RRs, and darker blue colors represent smaller RRs.
The association between temperature and hospital admissions demonstrated consistency across various types of diseases (Supplementary Document 1). The three groups (neoplasms, diseases of the circulatory system, and diseases of the respiratory system) exhibited similar cumulative risk-response curves, despite variations in minimum risk temperature (26.5 °C, 25.4 °C, and 15.1 °C, respectively). Among the age subgroups, a high degree of concordance was observed in the 0–20 and 21–70 age groups, with a notable exception in the 70-plus age group, where the curve generally tended to decline as temperature increased. In the sex subgroups, the cumulative risk-response curves displayed smaller differences between the sexes.
Associations between hospital admissions and relative humidity
Figure 2 illustrates the association between daily mean relative humidity and hospital admissions, along with a contour map across lag days. A positive association between relative humidity and risk of admissions was observed (Fig. 2A). After a cumulative period of 21 days, the RR tended to increase when the relative humidity exceeded 88% and reached 1.50 (95% CI: 1.15–1.94) at 100%. Conversely, the RR decreased when relative humidity fell below 81%, reaching a minimum RR of 0.87 (95% CI: 0.66–1.14) at 33%. Figure 2B illustrates the impact of relative humidity on the risk of hospital admission at a single lag time. When relative humidity was below 50%, the RR decreased at shorter lag times (days 0–2). In contrast, when relative humidity exceeded 50%, the risk tended to increase during lag days 0–1. Extending the lag time for relative humidity levels between 33% and 70%, the RR increased on days 3–4 of the lag but decreased on days 5–10 and 15–21. When relative humidity surpassed 90%, the RR increased during lag days 0–1 and 4–21 across two time periods, while it decreased on days 2–3. Results with statistical significance are presented in Supplementary Document 1.

Cumulative risk-response curves and contour map for relative humidity Notes: a). Plot A shows the exposure-response association between relative humidity and total hospital admissions. The blue line represents the cumulative exposure-response specific relative risks (RR), and the shaded areas represent the 95% confidence intervals. All confidence intervals account for multiplicity via bootstrap-derived simultaneous inference. b). Plot B shows the exposure-lag-response contour map of relative humidity with specific RRs. In this plot, darker shades of red color represent larger RRs, and darker blue colors represent smaller RRs.
The association between relative humidity and hospital admissions exhibited a non-linear curve for neoplasms and diseases of the circulatory system (Supplementary Document 1). The lowest RR was observed at 59% (RR: 0.65, 95% CI: 0.53–0.80) for neoplasms and at 58% (RR: 0.89, 95% CI: 0.75–1.05) for diseases of the circulatory system. When relative humidity exceeded 85%, the RR again displayed a decreasing trend followed by an increasing trend, with turning points at 93% and 91%, respectively. For diseases of the respiratory system, the trend was consistent overall, with an increasing risk as relative humidity rose. In the age subgroups, the risk was consistent with a whole in the 0–20 age group. The increased risk of hospital admission for those aged 21–70 had a non-linear pattern and reached a minimum at 60% (RR: 0.78, 95% CI: 0.67–0.90). The increased risk of hospital admissions for those aged 70-plus had a non-linear pattern, with a minimum RR at 84% (RR: 0.99, 95% CI: 0.97–1.02). In the sex subgroups, the differences in cumulative risk-response curves were smaller and remained in close agreement with the whole, but there was a downward and then upward trend in risk in the female group when below 88%.
Sensitivity analysis
In the sensitivity analyses (Supplementary Document 1), varying the \(\:df\:\)of the time variables in the model (\(\:df\) = 5, 7, 8), the maximum number of lag days (maximum lag = 19, 20, 22, 23), and the \(\:df\:\)of the covariates (\(\:df\) = 4, 5) demonstrated that the association between mean daily temperatures, relative humidity and the risk of hospital admissions remained robust. In addition, we included seasonal categorical covariates for further adjustment, and the results showed that the model also remained robust. The detailed results are presented in Supplementary Document 1.
Discussion
To the best of our knowledge, this is the first study conducted in Macau to evaluate the impact of environmental weather conditions on hospital admissions. Our findings indicate that different weather conditions are associated with increased hospital admissions over several days. Cold weather can have a prolonged association with increased hospital admissions, observed up to 21 days. The cumulative risk-response curves for temperature and relative humidity exhibited varying trends across different diseases and age groups. Furthermore, except for temperature, there were fewer differences in the cumulative risk-response curves among different sexes.
Consistent with previous studies, a V-like shaped association between temperature and hospital admissions4,5,22where the risk increased both when temperatures fell below and rose above the minimum risk temperature. However, unlike previous findings, the minimum risk temperature in Macau was notably low at 14.5 °C. A study examining all-cause hospital admissions in Hong Kong indicated that the risk was lowest at approximately 27°C6. This result is likely due to the differences in the types of diseases in the hospital admissions data of the two studies. The results of disease subgroups showed that the minimum risk temperatures of neoplasm and disease of the circulatory systems were similar to the results of Hong Kong. The lower minimum risk temperature of disease of the respiratory system and its larger proportion (45%) in the sample data contribute to this phenomenon. Other potential reasons include the key differences between Hong Kong and Macau’s population demographics, urban design and access to healthcare. Regarding the lag effects of temperature, heat effects (temperatures exceeding 20 °C) may have an immediate impact but tend to last for a shorter duration. In contrast, cold effects (temperatures below 10 °C) may exhibit a more prolonged lag effect, persisting for several weeks. This association was like previous papers5which found that the effects of high temperatures on cardiovascular-related hospital admissions were compared to cold weather effects that lasted for up to three weeks shorter in the south-central coast of Vietnam.
This study has indicated that relative humidity was associated with an increased risk of hospital admissions. The cumulative exposure-response curves exhibited a smaller increase when below the mean and a substantial increase when above the mean, consistent with findings from a previous multicenter study23. The combination of rainy and highly humid weather may lead to the effect of relative humidity and hospital admissions, as previously suggested24,25.
In the subgroup analysis, all three disease categories displayed similarly shaped cumulative risk-response curves. For neoplasms, a specific temperature was identified as showing the lowest risk of hospital admissions. Increased admissions due to circulatory system diseases were observed in hotter weather compared to other diseases, aligning with previous studies4,26. Conversely, the minimum risk temperature for respiratory system diseases was relatively cooler (15.1 ℃) compared to other disease types, indicating that respiratory system-related admissions are more sensitive to cold weather. This sensitivity may be attributed to colder temperatures causing bronchoconstriction and weakening the respiratory immune response, thereby increasing susceptibility to infections27,28.
Regarding age subgroups, there was a notable difference between the 70-plus age group and others. Older adults have previously been shown to face a higher risk of earlier mortality with temperature increases in summer29. Despite the 0–20 and 21–70 age groups displaying similar cumulative risk-response curves, the risk of hospital admissions among children and adolescents (0–20) was larger during temperature changes. This could be due to underdeveloped core thermoregulatory capacity in children and adolescents29,30. No substantial differences were found between the sexes, contrasting with prior studies suggesting males or females were more prone to hospitalization during extreme temperatures5,23.
For the neoplasms and circulatory system disease groups, the risk of hospital admissions reached its lowest point at 59% humidity. At approximately 60% humidity, the air feels neither too dry nor overly humid, facilitating efficient sweat evaporation31which helps in cooling the body and preventing potential heat-related illnesses. Children and adolescents are more sensitive to humidity changes due to their increased outdoor exposure32,33. Older individuals, who are often less capable of regulating body temperature, benefit from high humidity, which helps keep the respiratory tract moist and maintains blood volume, thus reducing the risk of dehydration and cardiovascular strain30. Consequently, the 70-plus age group experienced the lowest risk at around 80% humidity. Females exhibited a lower risk at higher humidity levels than males, possibly because females tend to have higher skin blood flow, improving the efficiency of heat dissipation and helping maintain a stable core temperature in humid environments34.
Our study has several strengths. First, the hospital data was extracted from the sole providers of accident and emergency departments in Macau, representing the total number of admissions from those departments for the region. Given the small land area of the Macao region (32.9 km2), the weather measurement stations and hospitals were near one another, and the daily weather measured would be similar to that experienced around the hospitals. The second strength of our study is that we examined the association between weather conditions and specific diseases in addition to all hospital admissions; this level of detail allows us to observe the association of weather factors on specific sub-populations of individuals with diseases27,35. Finally, our investigation also offers insights into the burden of morbidity across different sex and age subgroups, which helps in identifying vulnerable populations at risk from climate-related challenges22.
Several limitations of this study should be acknowledged. Firstly, the sample size was relatively small compared to similar previous studies, limiting the interpretation of the subgroup analysis. Second, while our models adjusted for humidity when assessing temperature effects (and temperature was adjusted for when assessing humidity), the high complexity of the DLNM model makes complete disentanglement challenging. Therefore, the complex interactive effect of these weather variables is not analyzed. Thirdly, the data were derived from only two hospitals in Macau and given that Macau is close to Zhuhai in Mainland China and Hong Kong, Macau residents may opt to seek medical treatment in these neighboring regions. Fourth, our identification of hospital admissions and disease-specific subgroups relied on diagnoses using ICD-10 codes. Misclassification of coding may have influenced these findings. Fifth, the data extracted from hospitals were daily counts of admissions and not individual-level data, meaning accounting for individual confounding factors was not possible22. Daily count data was extracted to compile with data protection, preventing individual patients from being identifiable within this study. Finally, data in this study included time during the COVID-19 pandemic affecting Macau from 2020 to 2022 and may have contributed some bias to our findings24,36.
This study revealed a unique climate-health pattern in Macau, which requires public health adaptation measures for its specific urban environment. Given the vulnerability of the elderly to low-temperature exposure, the temperature sensitivity of children and adolescents often shows significant lagged effects after exposure to extreme heat. These identified temperature thresholds and lagged patterns must provide a robust forecasting framework37. Healthcare systems can use local weather forecasts combined with epidemiological data to anticipate surges in demand for healthcare services, enabling proactive mobilization of resources and capacity planning ahead of predicted extreme temperatures37. Besides, this study also promotes integrating emergency data to break the blind spots in extreme weather conditions monitoring and provide a corresponding support for climate health decision-making in Macau38.
Furthermore, these insights can facilitate targeted public health interventions. Understanding specific weather-disease relationships, especially for diseases such as respiratory illnesses, can help optimize prevention programs. For example, seasonal influenza vaccination campaigns can be strategically timed to maximize population coverage ahead of predicted risk periods, incorporating local climate patterns and short-term weather forecasts12. Implementing such adaptive measures—including vaccination programs and dynamic resource allocation based on predicted demand—has demonstrated significant cost-effectiveness in increasing the climate resilience of healthcare systems worldwide39,40. In addition, Macau’s compact administrative structure enables rapid policy implementation, and our proposed threshold warning can be integrated into the health bureau’s real-time monitoring dashboard39. More information on precipitation is available in Supplementary Document 2.
Data availability
All data generated or analyzed during this study are included in this published article and its Supplementary Document. We are unable to directly share the original data used in this study as the data custodians, Kiang Wu Hospital and Centro Hospitalar Conde Da São Januário dos Serviços de Saúde have not given permission for data sharing.
Abbreviations
- CI:
-
confidence interval
- df :
-
degree of freedom
- DLNM:
-
distributed lag nonlinear models
- GLM:
-
generalized linear models
- ICD-10:
-
International Classification of Diseases, Tenth Revision
- Macau SAR:
-
Macau Special Administrative Region
- RR:
-
relative risk
- SD:
-
standard deviations
5 References
Census and Statistics Department of Macau Special Administrative Region. Macau Statistical Yearbook, Census and Statistics Department of Macau Special Administrative Region, (2022). https://www.dsec.gov.mo/zh-CN/Home/Publication/YearbookOfStatistics
Macau Meteorological and Geophysical Bureau. Climate Change. Macau Meteorological and Geophysical Bureau, (2024). https://www.smg.gov.mo/zh/page/363.
Li, X., Wei, Z., Wang, H., Ma, L. & Guo, S. - Variations in the Precipitation Extremes Over the Guangdong-Hong Kong-Macao Greater Bay Area in China (– 147, 2022).
Wen, B. et al. Association of cause-specific hospital admissions with high and low temperatures in thailand: a nationwide time series study. Lancet Reg. Health West. Pac. 46, 101058. https://doi.org/10.1016/j.lanwpc.2024.101058 (2024).
Thu Dang, T. A. et al. Short - term effects of temperature on hospital admissions for acute myocardial infarction: A comparison between two neighboring climate zones in Vietnam. Environ. Res. 175, 167–177. https://doi.org/10.1016/j.envres.2019.04.023 (2019).
Chan, E. Y., Goggins, W. B., Yue, J. S. & Lee, P. Hospital admissions as a function of temperature, other weather phenomena and pollution levels in an urban setting in China. Bull. World Health Organ. 91, 576–584. https://doi.org/10.2471/blt.12.113035 (2013).
Wondmagegn, B. Y. et al. Increasing impacts of temperature on hospital admissions, length of stay, and related healthcare costs in the context of climate change in adelaide, South Australia. Sci. Total Environ. 773, 145656. https://doi.org/10.1016/j.scitotenv.2021.145656 (2021).
Baldwin, J. W. et al. Humidity’s role in Heat-Related health outcomes: A heated debate. Environ. Health Perspect. 131, 55001. https://doi.org/10.1289/ehp11807 (2023).
Fan, J. F. et al. A systematic review and meta-analysis of cold exposure and cardiovascular disease outcomes. Front. Cardiovasc. Med. 10, 1084611. https://doi.org/10.3389/fcvm.2023.1084611 (2023).
Ford, T. E. et al. Using satellite images of environmental changes to predict infectious disease outbreaks. Emerg. Infect. Dis. 15, 1341–1346. https://doi.org/10.3201/eid1509.081334 (2009).
RECOVERY Collaborative Group. Baricitinib in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial and updated meta-analysis. Lancet 400, 359–368. https://doi.org/10.1016/s0140-6736(22)01109-6 (2022).
World Health Organization. Climate Change, World Health Organization (WHO), (2023). https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health
World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human participants. Jama 333, 71–74. https://doi.org/10.1001/jama.2024.21972 (2025).
Macau Environmental Protection Bureau. Environmental data, Macau Environmental Protection Bureau, < (2024). https://www.dspa.gov.mo/envdata.aspx
Gasparrini, A. Distributed lag linear and Non-Linear models in R: the package Dlnm. J. Stat. Softw. 43, 1–20 (2011).
Gasparrini, A., Armstrong, B. & Kenward, M. G. Distributed lag non-linear models. Stat. Med. 29, 2224–2234. https://doi.org/10.1002/sim.3940 (2010).
Zhang, R. et al. Association between air temperature and risk of hospitalization for genitourinary disorders: an environmental epidemiological study in lanzhou, China. PLoS One. 18, e0292530. https://doi.org/10.1371/journal.pone.0292530 (2023).
Gasparrini, A. et al. Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386, 369–375. https://doi.org/10.1016/s0140-6736(14)62114-0 (2015).
Chen, R. et al. Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. Bmj 363, k4306. https://doi.org/10.1136/bmj.k4306 (2018).
Tian, Y. et al. Association between ambient air pollution and daily hospital admissions for ischemic stroke: A nationwide time-series analysis. PLoS Med. 15, e1002668. https://doi.org/10.1371/journal.pmed.1002668 (2018).
Armstrong, B. Models for the relationship between ambient temperature and daily mortality. Epidemiology 17, 624–631. https://doi.org/10.1097/01.ede.0000239732.50999.8f (2006).
Burkart, K. G. et al. Estimating the cause-specific relative risks of non-optimal temperature on daily mortality: a two-part modelling approach applied to the global burden of disease study. Lancet 398, 685–697. https://doi.org/10.1016/s0140-6736(21)01700-1 (2021).
Huang, K. et al. Contributions of ambient temperature and relative humidity to the risk of tuberculosis admissions: A multicity study in central China. Sci. Total Environ. 838, 156272. https://doi.org/10.1016/j.scitotenv.2022.156272 (2022).
Yu, S. et al. Impact of temperature and relative humidity variability on children’s allergic diseases and critical time window identification. BMC Public. Health. 24, 2068. https://doi.org/10.1186/s12889-024-19573-9 (2024).
Pan, R. et al. Impacts of exposure to humidex on the risk of childhood asthma hospitalizations in hefei, china: effect modification by gender and age. Sci. Total Environ. 691, 296–305. https://doi.org/10.1016/j.scitotenv.2019.07.026 (2019).
Kephart, J. L. et al. City-level impact of extreme temperatures and mortality in Latin America. Nat. Med. 28, 1700–1705. https://doi.org/10.1038/s41591-022-01872-6 (2022).
Zhang, K. et al. The optimal degree of core temperature for hypothermic circulatory arrest in complex aortic arch surgery: results from 1310 patients. Eur. J. Cardiothorac. Surg. 66 https://doi.org/10.1093/ejcts/ezae311 (2024).
Conlon, K. C., Rajkovich, N. B., White-Newsome, J. L., Larsen, L. & O’Neill, M. S. Preventing cold-related morbidity and mortality in a changing climate. Maturitas 69, 197–202. https://doi.org/10.1016/j.maturitas.2011.04.004 (2011).
Flynn, A., McGreevy, C. & Mulkerrin, E. C. Why do older patients die in a heatwave? Qjm 98, 227–229. https://doi.org/10.1093/qjmed/hci025 (2005).
Xia, Y. et al. Effects of ambient temperature on mortality among elderly residents of Chengdu City in Southwest china, 2016–2020: a distributed-lag non-linear time series analysis. BMC Public. Health. 23, 149. https://doi.org/10.1186/s12889-022-14931-x (2023).
Fan, C. et al. An alternative comprehensive index to quantify the interactive effect of temperature and relative humidity on hand, foot and mouth disease: A two-stage time series study including 143 cities in Mainland China. Sci. Total Environ. 740, 140106. https://doi.org/10.1016/j.scitotenv.2020.140106 (2020).
Justine, J., Monteiro, J. M., Shah, H. & Rao, N. - The diurnal variation of wet bulb temperatures and exceedance of physiological thresholds relevant to human health in South Asia. – 4 (2023).
Vecellio, D. J., Wolf, S. T., Cottle, R. M. & Kenney, W. L. Evaluating the 35°C wet-bulb temperature adaptability threshold for young, healthy subjects (PSU HEAT Project). J. Appl. Physiol. (1985). 132, 340–345. https://doi.org/10.1152/japplphysiol.00738.2021 (2022).
Pinho-Gomes, A. C. & Woodward, M. The association between gender equality and climate adaptation across the Globe. BMC Public. Health. 24, 1394. https://doi.org/10.1186/s12889-024-18880-5 (2024).
Deng, P. et al. - The Role of High Humidity on extreme-temperature-related Mortality in Central China (– 16, 2023).
Zhu, G. et al. The association between ambient temperature and mortality of the coronavirus disease 2019 (COVID-19) in wuhan, china: a time-series analysis. BMC Public. Health. 21, 117. https://doi.org/10.1186/s12889-020-10131-7 (2021).
Tao;, L. et al. Current status of public health system in Guangdong-Hong Kong-Macao greater Bay area and improvement suggestion. Chin. J. Epidemiol. 44, 694–698. https://doi.org/10.3760/cma.j.cn112338-20221031-00927 (2023).
Guangzhou Municipal Health Commission. Representatives of the medical industry in Guangdong, Hong Kong and Macao discussed the high-quality development of the Healthy Bay Area, < (2023). https://wjw.gz.gov.cn/zzyyzq/wjdt/content/post_9318016.html
Ijjasz-Vasquez;, E. J. & Saghir, J. State and Trends in Climate Adaptation Finance 2024Global Center on Adaptation,. (2024).
Liu;, E. B., Kull;, D. & Chaponda, M. The Triple Dividends of Early Warning Systems and Climate Services, < (2024). https://wmo.int/media/magazine-article/triple-dividends-of-early-warning-systems-and-climate-services
Acknowledgements
The researchers would like to acknowledge the staff at both Macau hospitals for their kind cooperation with data extraction for this study. The researchers acknowledge that the data for this study are derived from Macau SAR hospital patients as part of their care and support.
Funding
This research was funded by the internal grant of the Faculty of Health Sciences, University of Macau.
Author information
Authors and Affiliations
Contributions
B.W. and S.S. contributed to the study in the conceptualization of the study, formal analysis, validation (B.W. conducted the formal analysis and S.S. validated the analysis), investigation, methodology and writing - original draft. R.D.S. contributed to the study in conceptualization, funding acquisition, project administration, supervision and writing - review & editing. E.P.L.L. contributed to the study in conceptualization, supervision and writing - review & editing. L.W.I., L.W.K., I.T.C., C.B.H., J.Q.H. and U.H.W. contributed to the study in conceptualization, methodology, data curation and writing - review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was conducted in accordance with the ethical standards of the University of Macau Research Committee. The health data used in this study were extracted from the computerized case databases of Kiang Wu Hospital and Centro Hospitalar Conde Da São Januário dos Serviços de Saúde in Macau. All cases in this study were de-identified at the hospital before researchers were granted access to the data. This study was approved by the University of Macau Research Committee reference number SSHRE24-APP087-FHS and got the support of Centro Hospitalar Conde Da São Januário dos Serviços de Saúde Ethics Committee and Kiang Wu Hospital Continued Medical Education and Research Department.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, B., Shen, S., I, L. et al. Associations of ambient temperature and relative humidity with hospital admissions in macau, China using time series analysis. Sci Rep 15, 25968 (2025). https://doi.org/10.1038/s41598-025-11913-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11913-y
