
Abstract
It is well-documented that early recurrence of hepatocellular carcinoma following liver transplantation can markedly impact patient survival. Accurately identifying patients at risk for early recurrence, followed by timely interventions, could greatly improve the long-term efficacy of liver transplantation. The Milan criteria, the clinical gold standard for selecting patients with a low risk of post-transplant recurrence, fails to exclude high-risk patients with biologically aggressive hepatocellular carcinoma. Accordingly, there is an urgent need to develop and validate an improved model for predicting hepatocellular carcinoma post-liver transplantation. Herein, we established a new model to stratify the risk of early hepatocellular carcinoma recurrence following liver transplantation and facilitate decision-making regarding adjuvant therapy. Our newly established nomogram could predict early recurrence post-liver transplantation more effectively than the Milan criteria. Importantly, we found that adjuvant therapy could significantly benefit high-risk recipients but did not significantly affect low-risk recipients. Based on the new stratification criteria, adjuvant therapy should be actively considered for high-risk patients post-liver transplantation, whereas postoperative follow-up and observation are recommended for low-risk patients. Early recurrence of hepatocellular carcinoma (HCC) following liver transplantation (LT) can adversely affect long-term patient survival. The Milan criteria (MC) have limited capacity to predict early HCC recurrence, and no consensus regarding prophylactic adjuvant therapy (AT) after LT has been established. Herein, we developed an accurate model for predicting early HCC recurrence following LT to guide decision-making on AT. Overall, 364 patients with HCC from three transplantation centers in China were included and followed up for one-year post-LT. Baseline data were used to construct a nomogram, comparing performance with the MC. The efficacy of AT was compared between patients stratified into low- and high-risk subgroups based on nomogram scores.The nomogram included tumor burden score, alpha-fetoprotein level, platelet-to-lymphocyte ratio, pathological differentiation, and microvascular invasion as independent predictive factors. The concordance index and the area under the curve of the nomogram were 0·768 (95% confidence interval, 0·753–0·781) and 0·809, respectively, exceeding those of the MC. The results of the calibration curve and decision curve analysis were also satisfactory. Considering the high-risk subgroups, the AT group considerably outperformed the No-AT group in terms of 1-year recurrence-free survival (45·0 vs. 23·0%, P < 0·001). However, the low-risk AT and No-AT groups did not significantly differ (78·5 vs. 83·9%). In patients with HCC, the new nomogram predicted early recurrence post-LT more effectively than the MC. Based on the new stratification criteria, high-risk patients may benefit from AT, whereas AT is not recommended for low-risk patients.
Similar content being viewed by others


Introduction
Globally, hepatocellular carcinoma (HCC) is one of the most prevalent malignancies and the third leading cause of cancer-related mortality1. China bears the heaviest HCC burden, accounting for 55·4% of all newly diagnosed HCC cases and 53·9% of HCC-related deaths worldwide2,3,4. Liver transplantation (LT) is the preferred course of therapy for patients with unresectable HCC. However, the problem of HCC recurrence after LT persists, owing to the high propensity of HCC leading to vascular invasion and metastases. Intrahepatic recurrence or distant metastases within one year after LT are considered early recurrences5,6,7. Numerous investigations have revealed that a poorer prognosis is typically indicated by an early recurrence of HCC following LT5,8,9. Studies defining early recurrence as within two years after transplantation also found that early HCC recurrence is associated with inferior outcomes10. Hence, it is critical to establish accurate prediction of early recurrence and therapeutic strategies to prevent tumor relapse.
The Milan criteria (MC) were introduced in 199611 and have since been widely adopted as patient selection criteria for LT. However, the requirements are strictly based on the tumor morphology and fail to adequately portray how primary tumors behave biologically. Accordingly, developing a better model to predict HCC recurrence following LT remains a crucial field of research7,12,13.
The administration of adjuvant therapy (AT) following LT to avoid HCC recurrence remains debatable. Regarding chemotherapy, the FOLFOX regimen is an effective AT option with potent activity against liver metastasis in colorectal cancer14,15and HCC16,17,18. Recent studies have also demonstrated that the FOLFOX regimen is a useful AT option following hepatectomy17 and can enhance the prognosis of individuals with HCC. Several countries have approved targeted agents sorafenib19,20 and lenvatinib21,22,23 as first-line treatments for unresectable HCC. However, there is limited research on these therapeutic approaches in the context of transplantation.
In the present study, we aimed to develop a model to accurately predict the probability of early recurrence following LT in patients with HCC to facilitate AT decision-making.
Methods
Patients and follow-up
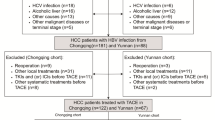
We retrospectively evaluated patients with primary HCC who received LT from January 2015 to December 2020 at three transplant centers in China, namely, the Shulan (Hangzhou) Hospital, The First Affiliated Hospital of the University of Science and Technology of China, and Huashan Hospital of Fudan University. This study was approved by the institutional ethics committees of the three hospitals and was in accordance with the Declaration of Helsinki’s principles. Only deceased donor liver transplantation was included in this study, and the surgical techniques employed included piggyback LT and conventional orthotopic LT. Inclusion criteria were as follows: (1) age above 18 years; (2) HCC diagnosis confirmed by postoperative histopathology. Exclusion criteria were as follows: (1) noncancer-related death within three months post-transplantation; (2) distant metastasis before LT; (3) retransplantation. (Fig. 1)

Flowchart for the patient selection process.
All patients included were followed up from the first day after LT and subsequently for at least one year; tumor recurrence or death served as the follow-up endpoint. Abdominal ultrasound and thoracoabdominal computed tomography scans were performed every 3 months for the first year of follow-up and thereafter. The assessment of serum tumor markers (alpha-fetoprotein [AFP] and protein induced by vitamin K absence or antagonist-II [PIVKA-II]) should be conducted once a month after transplantation. Diagnosis of tumor recurrence was based on imaging, and a biopsy was performed if the image was inconclusive.
Immunosuppression
The immunosuppressant regimen adopted in the three transplant centers was standardized. The immunosuppressant regimen consisted of an interleukin (IL)−2 antagonist on days 0 and 4 post-surgery routine initiation of tacrolimus for the first 3 months (6–10 ng/ml). After the first 3 months, the concentration of tacrolimus will be maintained at 3–6 ng/mL. Mycophenolate mofetil was given in the case of renal insufficiency. Glucocorticoids were withdrawn early post-surgery or not used, and in some patients, sirolimus was initiated one month after LT.
Treatment
We divided the included patients into the AT and No-AT groups based on the receipt of AT after LT. The AT included chemotherapy or targeted therapy; the modified-FOLFOX6 regimen was adopted as the only chemotherapy option, and the targeted agents included sorafenib or lenvatinib. All patients in the AT group underwent treatment with monotherapy regimens. For patients who have successfully downstaged through targeted therapy before liver transplantation, we adopt the targeted therapy. Chemotherapy is an alternative treatment option for patients who refused targeted therapy or patients with well-preserved liver function after transplantation.
Adjuvant chemotherapy (ACT) was initiated 6–8 weeks after LT without contraindications, such as leukocytopenia, infection, or hepatic insufficiency. The m-FOLFOX6 regimen comprised oxaliplatin 85 mg/m2, folinic acid 400 mg/m2, and 5-fluorouracil 400 mg/m2 on day 1, followed by 5-fluorouracil 2,400 mg/m2 as a 46 h continuous infusion. The treatment session was repeated every three weeks until completion of six treatment courses unless disease progression or unacceptable severe toxicities occurred or the patient refused to continue chemotherapy.
The drug dosage was adjusted based on the side effects reported by the patients. The patients prescribed sorafenib received a starting oral dose of 200 mg twice daily, titrated to the target dose of 400 mg twice daily if tolerated. The patients prescribed lenvatinib received a daily oral dose of 8 mg for body weight (BW) < 60 kg or 12 mg for BW ≥ 60 kg. Both agents were administered continuously until HCC recurrence, the occurrence of serious adverse events, or the patient’s request for drug discontinuation.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range). Counts (n) or percentages are used to report categorical variables. The Student’s t-test or Mann-Whitney U test was used to compare continuous variables, while the chi-squared or Fisher’s exact test was used to compare categorical variables. Univariate and multivariate analyses were conducted to identify risk factors strongly correlated with recurrence-free survival (RFS). A nomogram was created using variables in the multivariate Cox regression analysis with P < 0·05, and the nomogram performance was compared with the results of the MC. The patients were stratified into low- and high-risk subgroups based on the nomogram scores, and the Kaplan–Meier method was used to compare RFS between the AT and No-AT groups in different risk scenarios. The log-rank test was performed for intergroup comparisons. All statistical evaluations were performed using R software (version 4.2.2) and IBM SPSS Statistics 26.0 (IBM Corp., Armonk, NY, USA). A P value of < 0·05 was deemed statistically significant.
Results
Clinical characteristics of patients
This study examined 364 patients with HCC, of which 190 (52·2%) received LT only, and 174 (47·8%) received AT after LT, including 121 (69·5%) patients who received chemotherapy (the mean number of chemotherapy courses: 4.6) and 53 (30·5%) patients who received targeted therapy (sorafenib, n = 27; lenvatinib, n = 26). Table 1 displays the baseline features of patients. Most patients were males (n = 338, 92·9%). As for underlying disease, 92·3% (n = 336) were hepatitis B surface antigen positive, and the remaining patients include 1 patient with hepatitis C, 12 patients with alcoholic cirrhosis, and 15 patients with cryptogenic disease. Patients in the AT group were younger than those in the No-AT group (P = 0·003). Moreover, patients in the AT group exhibited more unfavorable tumor characteristics, including a higher tumor burden score (TBS) (P = 0·001), a higher level of PIVKA-II (P = 0·020), and the presence of portal vein tumor thrombus (PVTT) (P = 0·001) and microvascular invasion (MVI) (P < 0·001) than patients in the No-AT group.
Nomogram construction and assessment
The univariate analysis of all patients suggested age, body mass index, TBS, AFP and PIVKA-II levels, platelet-to-lymphocyte ratio (PLR), pathological differentiation, PVTT, MVI, and the use of sirolimus were significantly correlated with 1-year RFS. These characteristics were then employed in a multivariate Cox regression analysis to discover the ultimate predictive factors, including the TBS, AFP level, PLR, pathological differentiation, and MVI. Table 2 provides additional details.
To predict the probability of early HCC recurrence following LT, a nomogram (Fig. 2A) was created using the five above-stated factors and compared with 83 MC patients included in this study. The validation method used in this study was Bootstrap self-sampling, which was sampled 1000 times for internal validation of the model. The concordance index of the nomogram was 0·768 (95% confidence interval [CI], 0·753–0·781), and that of the MC was 0·629 (95% CI, 0·618–0·640). The receiver operating characteristic (ROC) curve (Fig. 2B) suggested that the areas under the curve of the nomogram and MC were 0·809 and 0·663, respectively, for predicting the 1-year RFS. Within the threshold probability across the whole cohort, the decision curve analysis (Fig. 2C) demonstrated that the nomogram afforded a more comprehensive net benefit than the MC. In addition, the calibration curve of the nomogram (Fig. 2D) showed a good consensus degree of the constructed model, i.e., a good agreement between the predicted and actual 1-year RFS rates.

(A) Nomogram for predicting the risk of early HCC recurrence after LT. (B) ROC curves of the nomogram and the MC for assessing 1-year RFS. (C) DCA curves of the nomogram and the MC. (D) The calibration curve of the nomogram. DCA, decision curve analysis; HCC, hepatocellular carcinoma; LT, liver transplantation; MC, Milan criteria; ROC, receiver operating characteristic.
Risk group classification
The recurrence risk score for each patient was calculated based on the nomogram, and the optimal cutoff value of the nomogram score was 236, as determined by the ROC analysis. Patients with nomogram scores < 236 were assigned to the low-risk subgroup (n = 213, 58·5%), and those with nomogram scores ≥ 236 were included in the high-risk subgroup (n = 151, 41·5%). The 1-year RFS rates were 34·6 and 81·5% for the high- and low-risk subgroups, respectively, with the patients in the low-risk subgroup having a significantly better prognosis (P < 0·001, Fig. 3A).

(A) Kaplan–Meier curves for patients in different risk groups based on the risk scores in the nomogram. (B) Kaplan–Meier curves for the AT and No-AT groups in all patients. (C) Kaplan–Meier curves for the AT and No-AT groups in high-risk patients. (D) Kaplan–Meier curves for the AT and No-AT groups in low-risk patients. AT, adjuvant therapy.
Effectiveness of AT
Overall, 136 (37·4%) patients experienced HCC recurrence by the end of the 1-year follow-up period, including 64 (36·8%) patients in the AT group and 72 (37·9%) patients in the No-AT group. There was no statistically significant between-group difference in the 1-year RFS rates between the AT and No-AT groups, which were 63·1 and 61·6%, respectively (P = 0·301, Fig. 3B).
In the high-risk cohort, the 1-year RFS rates were 45·0 and 23·0% in the AT and No-AT groups, respectively, thereby indicating that AT significantly reduced the risk of recurrence in the high-risk cohort (P < 0·001, Fig. 3C). In contrast, considering the low-risk cohort, the 1-year RFS rates were 78·5 and 83·9% in the AT and No-AT groups, respectively, with no statistically significant intergroup difference observed (P = 0·380, Fig. 3D).
Discussion
HCC recurrence after LT significantly shortens the long-term survival of patients; therefore, identifying patients prone to early recurrence and timely interventions are vital to improving the long-term efficacy of LT. In the present study, we established new criteria for stratifying the risk of early recurrence. Importantly, we found that AT could significantly benefit high-risk recipients with no significant effect on low-risk recipients.
In current clinical practice, MC have long been considered the gold standard for selecting patients with HCC with a low risk of post-LT recurrence. However, the screening criteria do not exclude high-risk patients with biologically aggressive HCC. With the increasing adoption of downstaging and locoregional therapy for HCC, the MC, based only on tumor morphological features, offer a gradually decreasing prognostic value for patients undergoing LT for HCC24. Alternatively, AFP is widely recognized as a reliable predictor of LT prognosis25,26,27. As markers of the aggressive biological behavior of HCC, MVI and histopathological differentiation are also substantial risk factors for HCC recurrence25,28,29. In addition, the tumor diameter and count constitute important tumor morphological parameters for assessing patient prognosis. Moreover, these two variables have traditionally been employed as dichotomous variables, as in the MC and Barcelona Clinic Liver Cancer classification system. The TBS indicates a paradigm shift from dichotomous to continuous prognostic stratification. Compared with other continuous or binary variables, the TBS provides a more comprehensive assessment of the overall tumor burden30. The PLR indicates the inflammatory state; previous studies have suggested that platelets and lymphocytes might play essential roles in tumor progression31,32. Elevated PLRs are typically attributed to simultaneous abnormalities in both measures rather than only thrombocytosis or lymphopenia, which disrupts the balance between antitumor and protumor immune responses. A meta-analysis has suggested that patients with high pre-LT PLRs have a 3.33-fold increased risk of experiencing HCC recurrence after LT32. Herein, the newly established nomogram, which incorporates these tumor morphological features, laboratory data, and pathological features, exhibited better performance in predicting early HCC recurrence after LT than the MC, thereby offering a higher clinical utility than MC.
Although HCC responds poorly to chemotherapy, chemotherapy can theoretically eliminate residual tumor cells if the tumor burden is eradicated, improving the prognosis. However, owing to the heterogeneity of different chemotherapy regimens and the lack of large randomized controlled trials, no definitive conclusion has been reached regarding the effectiveness of ACT. A systematic review and meta-analysis of 360 patients suggested that patients with advanced, poorly differentiated HCC might benefit from early implementation of ACT after LT33. The m-FOLFOX regimen is not commonly used as AT after LT, and there is limited research on its effectiveness in controlling tumor progression after LT. However, the administration of FOLFOX chemotherapy regimens has been shown to delay early tumor recurrence after LT, which may improve the survival rate of patients with HCC who do not meet the MC34. Collectively, these studies revealed that when classified using such prognostic factors, patients with more aggressive tumors may benefit from ACT, which is consistent with our findings.
Alternatively, in a prospective, randomized, multicenter study from Sweden35, authors detected no significant difference in efficacy between 19 patients with HCC in the chemotherapy group treated with doxorubicin perioperatively as ACT and 27 patients with HCC in the control group. However, it should be noted that in the subgroup analysis of patients who exceeded the MC, a tendency of improvement in 5-year disease-free survival (DFS) was observed in the chemotherapy group versus the control group (55 vs. 12%), although the sample size was markedly small to achieve a significant difference. Furthermore, Fujiki et al.36 have reported that future studies regarding AT should include patients with moderate-to-high risk of tumor recurrence, as determined using novel biomarkers or histologic diagnosis. Patients who meet the MC should be included with caution because these patients usually achieve a good outcome after LT. Our findings based on a comprehensive assessment of high-risk patients also support this perspective.
Sorafenib, the first molecular targeted drug approved for HCC treatment, impedes tumor angiogenesis by inhibiting the vascular endothelial growth factor and platelet-derived growth factor signaling pathway37. Several minor trials have attempted to evaluate the effectiveness of sorafenib in preventing the recurrence of HCC following LT. Shetty et al.38 have shown that AT with sorafenib after LT could decrease the risk of HCC recurrence in patients who exceeded the MC and prolong their 1-year DFS. In a phase I trial assessing adjuvant sorafenib in fourteen patients after LT who had carcinoma with vascular invasion or low differentiation, one patient (7.1%) died, and four patients (28.5%) experienced recurrence over the course of a median follow-up of 953 days, indicating a possible positive impact of sorafenib after transplant on RFS39. As a kinase inhibitor with activity against HCC tumors in a neogenic environment, sorafenib could theoretically prevent HCC recurrence in high-risk patients. However, Satapathy et al.40 have reported that sorafenib showed no efficacy in high-risk patients after LT. Considering the limited sample size in these studies and the lack of a universal standard for screening patients, no conclusion can be reached on whether sorafenib should be used as AT in patients who have undergone transplantation.
Conversely, the use of lenvatinib, a novel multitargeted tyrosine kinase inhibitor with efficacy against HCC, in the context of transplantation has been limited. Nevertheless, in a study assessing the adjuvant use of lenvatinib in fourteen patients who underwent LT for high-risk HCC, Han et al.41 have reported the possibility of lenvatinib lowering the post-transplant HCC recurrence. This promising result thus warrants verification by undertaking extensive randomized controlled trials.
In the present study, AT did not appear to confer a significant benefit in preventing early HCC recurrence in the overall study cohort, probably because AT is typically administered to patients with a heavy tumor burden and more unfavorable pathological features. Therefore, to elucidate the efficacy of AT, we evaluated outcomes of AT administration in subgroups stratified by risk. In the AT and No-AT cohorts, RFS differed significantly between the low- and high-risk subgroups (34·6 vs. 81·5%, P < 0·001). Moreover, 98·0% of patients in the high-risk subset exceeded the MC, which was consistent with our model. However, in the low-risk subgroup, 62·4% of patients exceeded the MC, and 54·9% received AT. For these patients, an issue of overtreatment may exist, which, in addition to imposing an unnecessary economic burden, may reduce their quality of life or even threaten their lives because of adverse reactions induced by chemotherapy or targeted agents. However, after long-term follow-up of high-risk patients for more than one year, we found that the AT group still had better RFS performance compared to the No-AT group (P = 0.002). Hence, an accurate prediction model is crucial in assisting clinicians in decision-making regarding precision treatment.
The present study has some limitations. First, this was a retrospective study with unavoidable bias. Second, most patients in the study cohort had hepatitis B virus infection, which may limit the applicability of our prediction model to a broader range of patients. Therefore, prospective randomized studies with large sample sizes must be undertaken to further validate our results.
In summary, although this study has limitations in retrospective analysis, according to the new stratification criteria validated in the present study, individualized adjuvant therapy post-LT might be effective in reducing the risk of recurrence for high-risk patients. Conversely, postoperative follow-up and observation are recommended for low-risk patients unless they express a strong willingness to undergo treatment.
Data availability
The dataset analyzed during the current study is available from the corresponding author upon reasonable request.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71 (3), 209–249 (2021).
Zhou, M. et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 394 (10204), 1145–1158 (2019).
Torre, L. A. et al. Global cancer statistics, 2012. CA Cancer J. Clin. 65 (2), 87–108 (2015).
Chen, W. et al. Cancer statistics in china, 2015. CA Cancer J. Clin. 66 (2), 115–132 (2016).
Sapisochin, G. et al. Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large Euro-American series. Ann. Surg. Oncol. 22 (7), 2286–2294 (2015).
Fernandez-Sevilla, E. et al. Recurrence of hepatocellular carcinoma after liver transplantation: is there a place for resection? Liver Transpl. 23 (4), 440–447 (2017).
Miao, W. et al. An FDG PET/CT metabolic parameter-based nomogram for predicting the early recurrence of hepatocellular carcinoma after liver transplantation. Eur. J. Nucl. Med. Mol. Imaging. 48 (11), 3656–3665 (2021).
Goldaracena, N. et al. Live donor liver transplantation for patients with hepatocellular carcinoma offers increased survival vs. deceased donation. J. Hepatol. 70 (4), 666–673 (2019).
Verna, E. C. et al. Liver transplantation for hepatocellular carcinoma: management after the transplant. Am. J. Transpl. 20 (2), 333–347 (2020).
El-Domiaty, N. et al. Early versus late hepatocellular carcinoma recurrence after transplantation: predictive factors, patterns, and Long-term outcome. Transplantation 105 (8), 1778–1790 (2021).
Mazzaferro, V. et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl. J. Med. 334 (11), 693–699 (1996).
Filgueira, N. A. Hepatocellular carcinoma recurrence after liver transplantation: risk factors, screening and clinical presentation. World J. Hepatol. 11 (3), 261–272 (2019).
Zhao, J. W. et al. Prediction of early recurrence of hepatocellular carcinoma after liver transplantation based on computed tomography radiomics nomogram. Hepatobiliary Pancreat. Dis. Int. 21 (6), 543–550 (2022).
Xu, J. et al. Preoperative hepatic and regional arterial chemotherapy in the prevention of liver metastasis after colorectal cancer surgery. Ann. Surg. 245 (4), 583–590 (2007).
Trojan, J. et al. Neoadjuvant treatment with cetuximab, 5-fluorouracil, folinic acid and oxaliplatin in unresectable retroperitoneal recurrent colon cancer. Z. Gastroenterol. 46 (8), 776–779 (2008).
Li, S. H. et al. Postoperative adjuvant hepatic arterial infusion chemotherapy with FOLFOX in hepatocellular carcinoma with microvascular invasion: A multicenter, phase III, randomized study. J. Clin. Oncol. 41 (10), 1898–1908 (2023).
Li, S. et al. Postoperative adjuvant transarterial infusion chemotherapy with FOLFOX could improve outcomes of hepatocellular carcinoma patients with microvascular invasion: A preliminary report of a phase III, randomized controlled clinical trial. Ann. Surg. Oncol. 27 (13), 5183–5190 (2020).
He, M. et al. Lenvatinib, Toripalimab plus FOLFOX chemotherapy in hepatocellular carcinoma patients with extrahepatic metastasis: A biomolecular exploratory, phase II trial (LTSC). Clin. Cancer Res. 29 (24), 5104–5115 (2023).
Llovet, J. M. et al. Sorafenib in advanced hepatocellular carcinoma. N Engl. J. Med. 359 (4), 378–390 (2008).
Cheng, A. L. et al. Efficacy and safety of Sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 10 (1), 25–34 (2009).
Vogel, A. et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 30 (5), 871–873 (2019).
Marrero, J. A. et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology 68 (2), 723–750 (2018).
European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu, European association for the study of the liver. EASL clinical practice guidelines. EASL clinical practice guidelines. management of hepatocellular carcinoma. J. Hepatol. 69 (1), 182–236 (2018).
Firl, D. J. et al. Reframing the approach to patients with hepatocellular carcinoma: longitudinal assessment with hazard associated with liver transplantation for HCC (HALTHCC) improves ablate and wait strategy. Hepatology 68 (4), 1448–1458 (2018).
Agopian, V. G. et al. A novel prognostic nomogram accurately predicts hepatocellular carcinoma recurrence after liver transplantation: analysis of 865 consecutive liver transplant recipients. J. Am. Coll. Surg. 220 (4), 416–427 (2015).
Merani, S. et al. The impact of waiting list alpha-fetoprotein changes on the outcome of liver transplant for hepatocellular carcinoma. J. Hepatol. 55 (4), 814–819 (2011).
Duvoux, C. et al. Liver transplantation for hepatocellular carcinoma: A model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 143 (4), 986–994e3 (2012).
Duffy, J. P. et al. Liver transplantation criteria for hepatocellular carcinoma should be expanded: A 22-year experience with 467 patients at UCLA. Ann. Surg. 246 (3), 502–509 (2007). discussion 9–11.
Sotiropoulos, G. C. et al. Meta-analysis of tumor recurrence after liver transplantation for hepatocellular carcinoma based on 1,198 cases. Eur. J. Med. Res. 12 (10), 527–534 (2007).
Vitale, A. et al. Utility of tumor burden score to stratify prognosis of patients with hepatocellular cancer: results of 4759 cases from ITA.LI.CA study group. ITA.LI.CA. ITA.li. J. Gastrointest. Surg. 22 (5), 859–871 (2018).
Zheng, J. et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: A meta-analysis and systematic review. Cell. Physiol. Biochem. 44 (3), 967–981 (2017).
Lai, Q. et al. Platelet-to-lymphocyte ratio in the setting of liver transplantation for hepatocellular cancer: A systematic review and meta-analysis. World J. Gastroenterol. 24 (15), 1658–1665 (2018).
Lin, H. S. et al. Adjuvant chemotherapy after liver transplantation for hepatocellular carcinoma: A systematic review and a meta-analysis. Hepatobiliary Pancreat. Dis. Int. 14 (3), 236–245 (2015).
Zhang, Q. et al. Combination adjuvant chemotherapy with oxaliplatin, 5-fluorouracil and leucovorin after liver transplantation for hepatocellular carcinoma: A preliminary open-label study. Invest. New. Drugs. 29 (6), 1360–1369 (2011).
Söderdahl, G. et al. A prospective, randomized, multi-centre trial of systemic adjuvant chemotherapy versus no additional treatment in liver transplantation for hepatocellular carcinoma. Transpl. Int. 19 (4), 288–294 (2006).
Fujiki, M., Aucejo, F. & Kim, R. Adjuvant treatment of hepatocellular carcinoma after orthotopic liver transplantation: do we really need this? Clin. Transpl. 27 (2), 169–177 (2013).
Wilhelm, S. M. et al. Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signaling. Mol. Cancer Ther. 7 (10), 3129–3140 (2008).
Shetty, K., Dash, C. & Laurin, J. Use of adjuvant Sorafenib in liver transplant recipients with high-risk hepatocellular carcinoma. J. Transpl. 2014, 913634 (2014).
Siegel, A. B. et al. Phase I trial of Sorafenib following liver transplantation in patients with high-risk hepatocellular carcinoma. Liver Cancer. 4 (2), 115–125 (2015).
Satapathy, S. K. et al. No apparent benefit of preemptive Sorafenib therapy in liver transplant recipients with advanced hepatocellular carcinoma on explant. Clin. Transpl. 32 (5), e13246 (2018).
Han, B. et al. Potential role of adjuvant lenvatinib in improving disease-free survival for patients with high-risk hepatitis B virus-related hepatocellular carcinoma following liver transplantation: A retrospective, case control study. Front. Oncol. 10, 562103 (2020).
Funding
This study was supported by grants from the National Key R&D Program of China (2023YFC2306800), the Major Research Plan of Key Research and Development Project of Zhejiang Province (2023C03046 and 2024C03149), Hainan Province Science and Technology Special Fund (ZDYF2025LCLH012), the National Natural Science Foundation of China (92159202 and 82470690).
Author information
Authors and Affiliations
Contributions
Zhe Yang, Chen-Hao Gao, Qi-Jian Yu and Shu-Sen Zheng designed this study. Xing-Yu Luo, Zhao-Xin Shang, Shuo Wang, Jian-Peng Liu, Jian-Hua Li and Ji-Zhou Wang collected the clinical data. Chen-Hao Gao, Qi-Jian Yu, Xing-Yu Luo and Kai-Wun Chang analyzed the data and performed the statistical analyses. Chen-Hao Gao, Qi-Jian Yu and Zhaoxin Shang wrote the manuscript. All the contributors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no other conflicts of interest.
Ethics approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by institutional ethics committees of the Shulan (Hangzhou) Hospital, The First Affiliated Hospital of the University of Science and Technology of China, and Huashan Hospital of Fudan University, and informed consent was waived by institutional ethics committees of the Shulan (Hangzhou) Hospital.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gao, CH., Yu, QJ., Luo, XY. et al. Prognostic nomogram for recurrence of hepatocellular carcinoma after liver transplantation for decision making on postoperative adjuvant therapy. Sci Rep 15, 26792 (2025). https://doi.org/10.1038/s41598-025-12178-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12178-1
