
Abstract
As the main undertakers of home care for urostomy patients after discharge, family caregivers play an important role in patients’ postoperative recovery. Family caregivers of patients with urostomy may be under greater pressure than patients themselves, and there is a heavy burden on caregivers, and their care needs are complicated and urgent. However, there is a lack of research on the care needs of family caregivers of bladder cancer patients with urostomy, and tools to assess the specific needs of family caregivers of bladder cancer patients with urostomy are lacking. This study aimed to develop an assessment tool to measure the specific needs of family caregivers for bladder cancer patients with urinary ostomies and to examine its reliability and validity. The development of the scale is based on the Supportive Care Framework, and the item pool is determined through literature retrieval and qualitative research. The items of the scale were revised via Delphi expert consultation, and 198 family caregivers of urostomy patients in five 3 A hospitals in Taiyuan City, China, were investigated. SPSS 26.0 and AMOS 22.0 were used for data analysis. Exploratory factor analysis and confirmatory factor analysis were carried out to evaluate the reliability, content validity, discrimination validity, structure validity, and convergence validity of the scale. Exploratory factor analysis identified three dimensions of the 21-item scale of care needs of family caregivers of patients with bladder cancer undergoing urostomy, namely, demand for disease information, demand for physical and mental comfort, and demand for social support. Cronbach’s α coefficient and half-reliability of the whole scale and each dimension are greater than 0.7, indicating high internal consistency. Confirmatory factor analysis shows that the scale fits the data well, and the content validity, discrimination validity, and convergence validity of the scale are excellent, which provides evidence of support. The scale developed by the authors is a relatively reliable and effective tool for evaluating the specific care needs of family caregivers of patients with bladder cancer undergoing urostomy. Future research could develop role-specific subscales tailored to distinct kinship categories (e.g., spouses, daughters, sons) to enable precision assessment of caregiving needs.
Similar content being viewed by others

Introduction
According to the global cancer statistics report, there were about 614,000 new cases of bladder cancer in the world in 20221. According to the prediction of the World Health Organization, the number of cases in 2050 may increase by 75% compared with 20222. Radical cystectomy plus urinary diversion is an effective method to treat non-muscle invasive bladder cancer, so the number of patients undergoing urostomy is increasing. Family caregivers can provide home care services for urostomy patients to help them adapt to life and integrate into society3. Family caregivers refer to non-employed relatives who provide unpaid and informal care without professional training and undertake the main care tasks in the family environment, rather than professional medical personnel. Their roles are usually played by spouses, siblings, children and relatives of patients. In Europe, 80% of patients need the help of their spouses, children and other relatives4; In the United States, the number of family caregivers assisting older adults increased by nearly 6 million between 2011 and 2022, rising from 18.2 million to 24.1 million5.
However, the family caregivers of urostomy patients face great challenges in the process of caring for patients, primarily manifested in caregiving skills, physical strain, and emotional support needs. Patients with urostomy of bladder cancer excrete urine through stoma of abdominal wall, so they need to wear urine collection bag for life. Family caregivers help patients with daily activities and personal tasks, such as bathing, dressing, caring for wounds, managing drugs, arranging transportation and managing finances6. Family caregivers are an important source of emotional support for patients and need to provide emotional support to patients7,8. Studies have shown that the family caregivers of patients with urostomy may be under greater pressure than the patients themselves, and they need medical staff to help them more6,9. Family caregivers will have a variety of caregivers’ burdens in the process of care, such as: sleep disorder, depression, anxiety, fatigue, gastrointestinal diseases, headache, loss of personal space, work conflict, interpersonal tension, economic crisis and so on10,11,12. Family caregivers provide about 35 h of care every week, and 22% of caregivers say their health has deteriorated because of taking care of their families13. Higher care burden will lead to a decline in the happiness of caregivers, which will reduce the quality of care provided by family caregivers, and then have a negative impact on the prognosis of patients14.
The needs of family caregivers of urostomy patients with bladder cancer are complicated and urgent, and many researchers have carried out research. The needs of family caregivers of colostomy patients need to be met urgently. Brazilian scholar Elisângela and others revealed the needs of family caregivers of colostomy patients through qualitative research. Family caregivers need to learn physiological knowledge, medical terminology and knowledge related to disease surgery15. A cross-sectional survey conducted by Italian scholar Marianna found that both ostomy patients and their family caregivers expressed a strong need for training in ostomy care skills, indicating a significant demand for caregiving competencies among family caregivers8. Family caregivers may suffer from insomnia, fatigue and other problems due to long-term care for patients16, which belongs to the demand of physical comfort. They have a variety of social support needs, including economic support, social support and organizational support mainly from the government and hospitals6,8,17. Family caregivers often have negative emotions such as stress, anxiety and depression, and have high psychological and emotional needs.
Many studies have focused on the needs of ostomy patients themselves, while relatively few have examined the needs of their family caregivers. There are no tools to measure the care needs of family caregivers of patients with bladder cancer undergoing urostomy, but most of them are universal tools to evaluate the care needs of family caregivers of cancer patients, which can not reflect their specific needs such as artificial urethral care, selection of ostomy care products, observation and care of skin around ostomy, and caregivers’ assistance in self-image management of patients. The concept of supportive care was first proposed by Fitch (1994)18 as “the provision of necessary support to cancer patients and their caregivers to address physical, emotional, social, psychological, informational, spiritual, and practical needs throughout diagnosis, treatment, and follow-up phases—including survivorship, palliative care, and bereavement.” This multidimensional framework emphasizes holistic support across biopsychosocial domains, establishing the theoretical foundation for our scale development. Therefore, the purpose of this study is1 To develop a measurement tool to measure the care needs of family caregivers of patients with bladder cancer undergoing urostomy based on the Supportive Care Framework. The scale was originally developed in Chinese2. To test the quality of the tool by studying its reliability and validity.
Methods
This study was conducted in five 3 A hospitals in Taiyuan, Shanxi Province, China, from January to April 2023. The research is divided into two different stages: item pool development and data collection. All participants completed the informed consent form before participating.
Item pool development
Document retrieval
A research group was established, and a literature search was conducted to find the initial items of the scale. The research group of this study consists of seven members, and the detailed information and division of labor are presented in Appendix Table A2. In the Medline, Embase, Web of Science, CINAHAL, Cochrane Library, Psych INFO, China HowNet and Wanfang databases, articles related to our research topic published from the establishment of the database to January 31, 2023, were systematically searched. The combination of MeSH terms and free-text terms was used to search the databases. The search keywords used for the databases are provided in Appendix Table A3. The inclusion criteria included quantitative studies, qualitative research, mixed-methods designs, case reports, systematic reviews, consensus documents, position statements, clinical guidelines, gray literature, and book chapters. Among them, the full-text literature could not be obtained; non-Chinese and English documents; repeated publications or summaries of the meeting; and literature irrelevant to the subject of this study were excluded. Based on the Supportive Care Framework, the research group formed an initial item pool with the commonly used domestic demand assessment scale for family caregivers of cancer patients as a reference.
Qualitative research
From July 2022 to December 2022, we conducted semi-structured interviews with 25 family caregivers of urostomy patients to supplement the item pool of the scale. The interviews, coding, and analysis were conducted by Xiaojuan Han, Linping Shang, and Kaixia Gao. All researchers received specialized training prior to data collection to ensure sufficient expertise in qualitative interviewing. Individual face-to-face interviews were performed, each lasting about 60 min. The interview guide comprised four core questions. Audio-recorded sessions were transcribed verbatim and analyzed using thematic analysis. The research results identified three key challenges—confusion, family crisis, and struggle psychology. Among these three topics, the coders constructed six subtopics. These factors include a lack of knowledge and skills, strong insecurity and uncertainty, role conflict, economic burden, emotional overload, and calm acceptance. The research results have been published elsewhere6.
Delphi expert consultation
The Delphi expert consultation method was used to revise the items in the scale of care needs of family caregivers of patients with bladder cancer undergoing urostomy. On the basis of a literature review and qualitative interviews, the initial scale includes four dimensions namely, disease information needs, physiological needs, psychological needs, and social support needs, with a total of 24 measurement items. The expert group scores the measurement items and deletes or modifies the items in the corresponding dimensions.
The expert group consists of 8 urology clinical medical experts, 10 urology clinical nursing experts, and 2 medical psychology experts, all of whom are distributed across China. The general information of the experts is provided in Appendix Table A4. A total of two rounds of expert letters were conducted. The questionnaire for the first round was distributed to the expert group between January and February 2023, and the responses from 20 participants were statistically analyzed. The second round of the scale was subsequently distributed for further refinement and revision between March and April 2023, and the responses were collected.
The data were statistically analyzed using Microsoft Excel (version 2019; Microsoft Corp., Redmond, WA, USA; https://www.microsoft.com/en-us/microsoft-365/excel) and IBM SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA; https://www.ibm.com/products/spss-statistics). The positive coefficient of experts is expressed by the response rate of questionnaire recovery, and the questionnaire recovery rates of the two rounds of expert consultation are 95% and 100%, respectively. The authoritative coefficient of experts, the concentration degree of opinions, including the mean of importance assignment and coefficient of variation, and the coordination degree, including Kendall’s W and coefficient of variation, all met the statistical requirements (P < 0.05). The results are provided in Appendix Tables A5, A6, A7, and A8.
Finally, the items of the scale were revised from 22 to 23, and the dimensions were merged from four to three. Detailed information can be found in Appendix Tables A9 and A10.
Data collection
Setting and subjects
The family caregivers of urostomy patients were investigated with the revised scale. The participants were from five 3 A hospitals in Taiyuan, Shanxi, China. The inclusion criteria for participants were family caregivers of urostomy patients who are over 18 years old, have been caring for urostomy patients for three months or more, can understand Mandarin, have no barriers to communication, and have signed informed consent forms. The exclusion criteria included patients with a previous history of mental illness and taking mental illness drugs; patients with cognitive dysfunction, including stroke or nervous system dysfunction caused by liver, lung, kidney or other system diseases; and those who could not complete the assessment due to serious illness, emergency surgery, or noncooperation. The exclusion criteria were as follows1: identical responses to five consecutive questions or discernible response patterns2. Incomplete questionnaires3. Missing responses to ≥ 5% of the items.
Procedure
Ethical considerations
Our research procedures were conducted in strict accordance with the relevant regulations and principles. The study was conducted in accordance with the Helsinki Declaration. Ethical approval was obtained from the Ethics Committee of the First Hospital of Shanxi Medical University (approval number: K085). All participants were informed of the voluntary nature of their involvement, with explicit assurance of withdrawal rights at any stage without penalty. Full disclosure regarding the study’s purpose and procedures was provided prior to obtaining written informed consent from each participant, thereby safeguarding the ethical standards of voluntary participation.
Scale distribution
Online and offline methods are used to distribute the scale. For the family caregivers of patients who visit the hospital for treatment, the paper version of the scale is used to fill out one-on-site. Considering that family caregivers are unable to attend hospital visits, we administered electronic questionnaires via Wenjuanxing, an online survey platform. Prior to scale administration, research staff obtained written informed consent from all the participants.
Data analysis
IBM SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA; https://www.ibm.com/products/spss-statistics) was used for item analysis and confirmatory factor analysis. IBM SPSS Amos (version 26.0; IBM Corp., Armonk, NY, USA; https://www.ibm.com/products/structural-equation-modeling-sem) was used for confirmatory factor analysis.
Results
General information of the respondents
The study contacted 220 potential participants; 10 individuals declined to participate, and 12 questionnaires were excluded because of incomplete data, yielding an analytical sample of 198 respondents. First, from the perspective of relationships with patients, most of the respondents were daughters, accounting for 37.88%, followed by husbands (21.21%) and wives (19.70%). In terms of age distribution, 54.55% of the respondents were aged over 50 years, followed by those aged over 40 years, accounting for 33.33% of the sample. In terms of gender, women account for the majority, accounting for 60.61% of the sample. In terms of the time needed to take care of patients, most respondents took care of patients for more than 8 h a day, accounting for 63.64% of the sample. Finally, 84.85% of the respondents said they had no religious belief. In general, the distribution of social demographic characteristics of the sample is relatively balanced, which can provide more comprehensive background information for further analysis. The detailed demographic data are shown in Table 1.
Reliability
The internal consistency of the scale was evaluated by Cronbach’s α coefficient and split-half reliability. The Cronbach’s α coefficient of the scale of care needs of family caregivers of patients with bladder cancer undergoing urostomy was 0.951, and removing any item did not increase Cronbach’s α value. The split-half reliability is between 0.733 and 0.954, which indicates that the scale has good internal consistency. The results are presented in Appendix Table A11.
Validity
Content validity
The research team once again invited 20 experts to evaluate the relevance of the items in the scale to evaluate its content validity. The expert evaluation results show that the scales of the Item-level Content Validity Index (I-CVI) are all 1.00, the Scale-level Content Validity Index based on Universal Agreement (S-CVI/UA)is 1.00, the Scale-level Content Validity Index based on Average (S-CVI/AVE) is 1.00, and all the items are considered to fully represent the measured structure. The results are presented in Appendix Table A12.
Discrimination validity
The discriminant validity of the scale was evaluated via the critical ratio method. The results revealed that the scores of 198 participants consisted of low scores (≤ 48 points) and high scores (≥ 72 points), and the independent sample t test revealed that the t value was between 0.274 and 21.812 and that the discrimination of each item was good. The results are presented in Appendix Table A13.
Construct validity
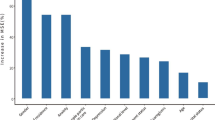
Exploratory factor analysis and confirmatory factor analysis were used to evaluate the structural validity of the scale. The results revealed that the Kaiser-Meyer-Olkin (KMO) value was 0.907, and the results of the Bartlett spherical test were significant (p < 0.001), which indicated that the data were very suitable for factor analysis. See Appendix Table 14 for details. Three factors with eigenvalues greater than 1 are extracted, and the sudden drop of the slope of the scree plot reveals three common factors (Fig. 1). The analysis confirmed that the scale included three dimensions, and the cumulative variance contribution rate was 68.493%. Following item screening via exploratory factor analysis (EFA), an expert panel discussion was conducted to reorganize the item structure, culminating in a finalized scale comprising 21 items across 3 dimensions. The factor loads of the 21 measurement items are all greater than 0.4. For details, see Appendix Table 15. Confirmatory factor analysis was used to test the hypothetical factor structure, and the fit indices of the model were satisfactory: Comparative Fit Index (CFI) = 0.900, Tucker-Lewis Index (TLI) = 0.972, Root Mean Square Error of Approximation (RMSEA) = 0.046, indicating that the data fit the hypothetical model well (Table 2). The fitted model is shown in Fig. 2. (The specific contents corresponding to A1–A11, B1–B7, and C1–C3 can be found in Table A1 of the Appendix.)

Scree Plot.

Three-Dimensional Model Fit of the Care Needs Scale for Bladder Cancer Urostomy Caregivers.
Convergent validity
The average variance extraction (AVE) and composite reliability (CR) of each potential structure were calculated to ensure the convergent validity of the scale. The AVE values and CR values of all the structures are > 0.50 and > 0.80, indicating good internal consistency. The results are shown in Appendix Table A16.
Discussion
The purpose of this study was to develop a scale to measure the care needs of family caregivers of patients with bladder cancer undergoing urostomy. Exploratory factor analysis revealed three dimensions of the scale, namely, demand for disease information, demand for physical and mental comfort, and demand for social support. The scale and each dimension have good internal consistency reliability, which is indicated by a Cronbach’s α coefficient > 0.7. We tested the validity of the scale in terms of discrimination validity, construct validity, content validity, and convergent validity. The results of the critical ratio method indicate that there are significant differences between the high and low groups in all the items, and the discriminant validity of the scale is good. Exploratory factor analysis revealed three common factors whose cumulative variance contribution rate exceeded 68%, and the factor load ranged from 0.693 to 0.866, both of which were greater than 0.4, indicating that the scale had strong structural stability. We once again invited 20 experts to evaluate the relevance of the items in the scale, and the I-CVI was 1.00. The results showed that the content validity of the scale was excellent. The average variance extraction (AVE) and composite reliability (CR) were used to evaluate the convergence validity of the scale. The AVE of each latent variable was greater than 0.50, and the CR was greater than 0.80, which indicated that the internal quality of the model was extremely ideal. The validation by confirmatory factor analysis shows that the fit index conforms to the statistical standard, which further supports the strong structural validity of the scale. We conducted two rounds of Delphi expert consultation when we revised the items in the scale. The experts involved in the survey were from many fields and had rich clinical experience. The degree of expert authority was greater than 0.8, and the experts were more enthusiastic during the consultation process, which increased the reliability of the research results.
The majority of studies have been conducted on the basis of the Supportive Care Framework, which aims to improve quality of life in diverse cancer patient populations. Sinead Benson and colleagues19 demonstrated that a nurse-led integrated enhanced supportive care (ESC) model effectively improved outcomes in patients with hepatopancreatobiliary cancer. A qualitative study by Leila Valizadeh and collaborators20 explored supportive care needs in adolescent cancer survivors, emphasizing that these needs should be met through collaborative efforts involving families and healthcare providers. This study focused on family caregivers of bladder cancer patients undergoing urostomy to develop a needs assessment tool. It aims to identify their specific care requirements, inform the design of tailored interventions, enhance caregivers’ capacity, and ultimately improve quality of life. Similarly, numerous researchers have developed caregiver needs assessment instruments. Notable examples include the Health Care Needs Survey (HCNS)21, the Support Person’s Unmet Needs Survey (SPUNS)22, and the Supportive Care Needs Survey for Partners and Caregivers (SCNS-P&C)23, which are all designed to assess needs across general cancer populations. The scale developed in this study specifically targets family caregivers of patients with bladder cancer undergoing urostomy. It aligns with existing instruments in core need domains—disease management, physical/psychological care, and social support—while showing robust psychometric validation, thus accurately reflecting caregivers’ distinctive requirements. The three questions of the scale we developed in the dimension of disease care demand are different from other universal care demand scales, which are specific to the care process of bladder cancer patients. That is, A1: “Mastering the knowledge of home care for urostomy (such as changing the ostomy bag and catheter)”; A4: “Guiding me to learn to evaluate the skin around the patient’s stoma (such as/moisture-related dermatitis/medical adhesive-related skin injury/allergic dermatitis/atypical hyperplasia around the stoma/urate crystal/pseudoverrucous hyperplasia, etc.)”; and A10: “Helping me choose the appropriate stoma care products (such as the types of stoma products and the ways of purchasing, etc.).”
We developed a scale for evaluating the specific care needs of family caregivers of patients with bladder cancer undergoing urostomy, which is in line with the national conditions of China and can identify the needs of family caregivers of urostomy patients in China. Bruna dos Santos Carmo24 demonstrated that religiosity/spirituality/religious-spiritual coping (RS) serves as a resource utilized by cancer patients to cope with illness and is associated with increased preference for aggressive end-of-life care. Influenced by traditional Chinese culture and Western culture, Chinese people have diverse religious beliefs, including Buddhism, Taoism, Christianity, Islam, and various other Chinese religions25. In the second dimension of the scale, item B6—“Understand and respect my religious beliefs (Buddhism/Christianity/Islam, etc.)”—reflects the importance of respecting the religious beliefs of Chinese family caregivers of urostomy patients and addressing their spiritual needs. WeChat is the most commonly used application software for communication in China26. In the third dimension of social support demand, item C2— “Help me keep in touch with other patients’ families (WeChat/telephone, etc.)”— emphasized the use of WeChat to help family caregivers keep in touch with others, which is also in line with the national conditions of China.
However, the recruitment hospitals interviewed in this study are all from Shanxi Province, and the sample is not representative enough. In the future, the sample size and area can be further expanded, and family caregivers with different cultural backgrounds can be selected for investigation to reduce selection bias. Second, budgetary constraints precluded test-retest reliability assessment of the scale’s temporal stability.
Conclusions
The scale of care needs of family caregivers of patients with bladder cancer undergoing urostomy includes 3 dimensions and 21 items, which shows strong reliability and effectiveness, and is a scientific, accurate and reliable tool to evaluate the care needs of family caregivers of patients with bladder cancer undergoing urostomy in China. The care needs of family caregivers for bladder cancer patients with urostomy in China are multifaceted. Future research could retrospectively apply novel theoretical frameworks adapted to China’s sociocultural context and healthcare system to further investigate these needs. Furthermore, developing role-specific subscales—tailored to kinship categories such as spouses, daughters, and sons—would enable precision assessment of distinct caregiving demands.
Data availability
The datasets generated and analyzed during this study can be obtained by contacting the first author upon reasonable request. The data are not publicly available due to confidentiality agreements and ethical restrictions protecting participant privacy.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74 (3), 229–263 (2024).
Cancer IAfRo. Global Cancer Observatory: Cancer Tomorrow - Bladder Cancer Projections. (2022).
Han, X. et al. Benefits of Chinese family caregivers of patients with urostomy: a qualitative study. Support Care Cancer. 32 (4), 266 (2024).
Antonella, S., Flavia, V., Daniela, T., Giuseppe, T. & Daniele, S. The ‘charter of rights for family caregivers’. The role and importance of the caregiver: an Italian proposal. ESMO Open. 2 (5), e000256 (2017).
Wolff, J. L., Cornman, J. C. & Freedman, V. A. The number of family caregivers helping older US adults increased from 18 million to 24 million, 2011-22. Health Aff (Millwood). 44 (2), 187–195 (2025).
Han, X., Gao, K., Shang, L. & Wei, L. Caregiver experiences of caring for family members with urostomy: a qualitative study. Support Care Cancer. 32 (3), 167 (2024).
Yao, H., Hou, Y., Zhang, X. & Zhang, Q. Extrinsic emotional regulation experienced by lung cancer patients and their family caregivers during progression-free survival. Eur. J. Cancer Care (Engl). 31 (6), e13750 (2022).
Masiero, M. et al. Quality of life and psycho-emotional wellbeing in bladder cancer patients and their caregivers: a comparative analysis between urostomy versus ileal orthotopic neobladder. Ecancermedicalscience 15, 1163 (2021).
Bolgeo, T. et al. Management of the patient with urostomy: caregiver needs during the three months after discharge. A qualitative study. Arch. Ital. Urol. Androl. 95 (1), 11024 (2023).
Ferrell, B. & Wittenberg, E. A review of family caregiving intervention trials in oncology. CA Cancer J. Clin. 67 (4), 318–325 (2017).
Adelman, R. D., Tmanova, L. L., Delgado, D., Dion, S. & Lachs, M. S. Caregiver burden: a clinical review. Jama 311 (10), 1052–1060 (2014).
Lambert, S. D. et al. The unmet needs of partners and caregivers of adults diagnosed with cancer: a systematic review. BMJ Support Palliat. Care. 2 (3), 224–230 (2012).
Sun, V., Raz, D. J. & Kim, J. Y. Caring for the informal cancer caregiver. Curr. Opin. Support Palliat. Care. 13 (3), 238–242 (2019).
Northouse, L. L., Katapodi, M. C., Schafenacker, A. M. & Weiss, D. The impact of caregiving on the psychological well-being of family caregivers and cancer patients. Semin Oncol. Nurs. 28 (4), 236–245 (2012).
Cerencovich, E. & Maruyama, S. A. T. Familiar Cuidador Da Pessoa com estoma family caregiver of a person ostomy Ciência. Cuidado E Saúde ;14(4), 1480–1490 (2016).
Rafiei, H., Rashvand, F. & Malmir, S. Quality of life of family caregivers of patients with a stoma: a cross-sectional study from Iran. Br. J. Nurs. 29 (22), S27–s30 (2020).
Kitko, L. A. & Hupcey, J. E. The work of spousal caregiving of older adults with end-stage heart failure. J. Gerontol. Nurs. 39 (7), 40–47 (2013).
Fitch, M. I. Supportive care framework. Can. Oncol. Nurs. J. 18 (1), 6–24 (2008).
Benson, S., Wong, H., Olsson-Brown, A., Coyle, S. & Monnery, D. Palliative care clinical nurse specialists leading enhanced supportive care in hepatopancreatobiliary cancer. Int. J. Palliat. Nurs. 29 (3), 129–136 (2023).
Valizadeh, L. et al. Adolescent cancer survivors’ experiences of supportive care needs: A qualitative content analysis. Nurs. Health Sci. 22 (2), 212–219 (2020).
Hileman, J. W., Lackey, N. R. & Hassanein, R. S. Identifying the needs of home caregivers of patients with cancer. Oncol. Nurs. Forum. 19 (5), 771–777 (1992).
Campbell, H. S. et al. The cancer support person’s unmet needs survey: psychometric properties. Cancer 115 (14), 3351–3359 (2009).
Girgis, A., Lambert, S. & Lecathelinais, C. The supportive care needs survey for partners and caregivers of cancer survivors: development and psychometric evaluation. Psychooncology 20 (4), 387–393 (2011).
Santos Carmo, B. D. et al. Relationship between religion/spirituality and the aggressiveness of Cancer care: A scoping review. J. Pain Symptom Manage. 65 (5), e425–e37 (2023).
Lizhu, F. Popular religion in contemporary China. Social Compass. 50 (4), 449–457 (2003).
Chen, X., Zhou, X., Li, H., Li, J. & Jiang, H. The value of WeChat application in chronic diseases management in China. Comput. Methods Programs Biomed. 196, 105710 (2020).
Author information
Authors and Affiliations
Contributions
Xiaojuan Han conceived and designed the study. Xinqian Shi, Taohong Ma, Kaixia Gao and Qiuju Wang were responsible for the acquisition of data. Xue Han, Ruining Zhao, Yue Zhou, Jiahui Zhu and Hao Guo contributed to the interpretation of data. Xiaojuan Han, Xinqian Shi and Linping Shang wrote the first draft of the paper. All authors were involved in the subsequent revision and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Han, X., Shi, X., Ma, T. et al. Development and preliminary verification of the scale of care needs of family caregivers of patients with bladder cancer undergoing urostomy. Sci Rep 15, 26588 (2025). https://doi.org/10.1038/s41598-025-12678-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12678-0
