
Abstract
This study evaluated specific effects of a blinded randomized controlled trial of a group-based social skills intervention, Socio-Dramatic Affective-Relational Intervention (SDARI), against an active attention control (AC) intervention. Fifty-five autistic youth (Mage=12.40; SDage=2.92; 73% boys) were randomly allocated to either the SDARI or the AC condition. Both interventions comprised 10 weekly sessions and were tightly matched for structure, participant age, IQ, and gender, such that the specific activities of SDARI were directly examined. Multimethod assessments at pre-, post-treatment, and 10-week follow-up included informant-reported social skills and autism-related behaviors, observer-rated spontaneous peer interaction, peer-rated friendships, and a metric of social information processing (the N170 event-related potential). Parent expectancy effect was also explored by examining perceived conditions by parents/caregivers, who were blinded to the condition assignment. Compared to the AC condition, the SDARI group evinced improvements in the N170 latency, rapid peer-liking, and reciprocal friendships at endpoint and follow-up. While the conditions did not differ on parent-reported social skills or autism-related behaviors, a parental expectancy effect was found where parent-rated social skills improvements were related to parents’ perceived conditions. These results provide support for the efficacy of the specific SDARI activities on several objective, reliable outcomes of social functioning in autistic youth.
Similar content being viewed by others


Introduction
Group-based social skills interventions (GSSIs) are one of the primary intervention methods for improving core social competence challenges in school-aged and adolescent autistic youth1,2. GSSIs have been shown to be both effective and efficacious for addressing social skills challenges in autism spectrum disorder (ASD)1,2,3,4, with overall medium effects1.
However, there are substantial and consistent methodological limitations that impact the reliability of this evidence. First, findings from GSSIs are often limited by reliance on highly subjective measures. For instance, it is often unclear whether parent-reported effects are due to parent expectancy and detection biases–that is, are they effectively a placebo effect5. It is thus important to use metrics that are less reliant on subjective perceptions of change, including neural constructs6 and observational methods7. For example, delayed latency of the N170 event-related potential indexed by electroencephalogram (EEG) to faces suggests atypical neural processing of social information, and exhibits robust evidence of being a promising biomarker for ASD8,9. Preliminary evidence suggests that N170 latency may decrease following behavioral treatment designed to enhance social communication in autistic children, indicating its potential as a measure of treatment response for this population10. Also, direct observation of peer interactions in naturalistic settings captures authentic social dynamics among autistic youth11. Similarly, examining peer-reported sociometric status assesses social outcomes within the context in which social relationships develop and function, and has been implemented in intervention settings12,13. Second, few randomized controlled trials (RCTs) using active control have been conducted in this literature, and most have used “straw man” comparison conditions14. Third, no study to date in this literature has sought to blind invested primary outcome reporters (e.g., parents) to participant condition assignment. While this has often been attributed to the methodological difficulty of ethically precluding participant awareness of condition assignment in behavioral interventions15, it nonetheless means that no study in this literature has adhered to this in gold-standard RCT designs4. Fourth, GSSIs are highly susceptible to other nonspecific treatment effects, such as exposure to peers, time spent in group, therapist training, differences in the intervention space, and presence of a supportive environment, precluding the ability to identify whether any effects are specific to a particular GSSI – or are simply the result of these nonspecific effects. Fifth, analytic limitations abound, such as lack of utilization of statistical methods that account for nesting within groups16, as well as limited examination of generalization and maintenance of effects17. While all of these issues may be addressed via the use of a blinded active attention component-control (AC) RCT design18 with appropriate analytic considerations, all but two studies19,20 have done so to examine a GSSI for autistic youth.
The current study utilizes such an approach, thereby representing the most rigorous examination of the efficacy of GSSIs for ASD to date. This study examined the efficacy of Socio-Dramatic Affective-Relational Intervention (SDARI), which has shown evidence of effectiveness for improving social skills among autistic youth across several preliminary studies13,21,22,23,24. For instance, the initial pilot study of 17 participants showed large effects on increasing assertion and decreasing social problems, with small effects on emotion recognition, with benefits maintained at 6-week follow-up21. A subsequent comparative study with another GSSI involving 13 participants found that SDARI was equally effective at promoting friendships, with SDARI participants showing decreased negative interactions and producing faster initial gains in social preference13. Additional studies demonstrated improvements in theory of mind, enhanced social knowledge, and better emotion recognition, particularly in community-based settings23. Overall, research to date suggests SDARI improves both social communication and social cognition in autistic children, with different benefits emerging in laboratory versus community settings.
In particular, using rigorous experimental controls and examining long-term maintenance of effects, we investigated SDARI’s impact on two key domains: (1) objective measures, including (1a) an EEG metric of social information processing, (1b) observer-rated social interactions, and (1c) peer-reported reciprocal friendships; and (2) assessment of parent-reported social skills while accounting for parent expectancy effects that often confound subjective measures.
Method
This trial was a randomized, single-blind, active-controlled study, with a 1:1 allocation ratio. This study was retrospectively registered on the Open Science Framework (OSF): https://osf.io/v7zrb.
Research participants
Fifty-five youth from a mid-Atlantic state (Mage=12.40, SDage=2.92; 40 male, IQ ≥ 70) participated in the current study from 2015 to 2017. Participants who met the recommended ASD cutoffs (scores ≥ 11) on the Social Communication Questionnaire25 were eligible for an initial screening visit for this study. Participants were eligible to participate in this study if they (1) met criteria for ASD as confirmed by the gold-standard diagnostic assessment, the Autism Diagnostic Observation Schedule-Second Edition (ADOS-2)26 assessed by research-reliable examiners; (2) between ages of 8–17; and (3) measured verbal and full-scale IQ ≥ 70 based on an IQ evaluation via the Kaufman Brief Intelligence Test-Second Edition (KBIT-2)27. Youth with significant medical or neurological illnesses that could impair participation were excluded from the study. Out of 100 youth assessed for eligibility, fourteen youth did not meet the inclusion criteria, and thirty-one participants declined enrollment, citing common barriers to participation in randomized controlled trials, including scheduling conflicts, transportation limitations, and time constraints. Written informed consent from a parent and/or legal guardian and assent from minors were obtained prior to any research activity. The current study sample has been described in other publications28,29.
Procedures
The study was approved by the University Institutional Review Board, and all methods were conducted in accordance with relevant guidelines and regulations. Autistic youth participated in 1.5 h/week groups for 10 weeks. Each 10-week period is considered one “cycle” of intervention. There were 4 cycles in each condition (total of 8 groups). Interventions were implemented in a Psychology laboratory setting at a University. All group members were involved in the study, but participants were recruited individually from the surrounding communities and did not have known connections outside of intervention setting.
As is standard practice for SDARI, participants within a group were within 3 years of age of one another. We carefully considered developmental age and appropriateness of the groups, such that younger groups had participants aged 8–12 and older groups had participants 13 and older. This grouping approach was refined through years of implementation of SDARI, ensuring that participants were developmentally similar, facilitating more effective peer interactions, appropriate social challenges, and engagement in age-relevant activities. AC groups were also matched to a paired SDARI group on age (within 3 years), IQ, and gender. There were 2 groups of younger children (aged 8/9 to 11/12) and 2 groups of older children (aged 13/14 to 16/17) for each intervention condition.
Table 1 summarizes demographic characteristics of the sample as well as comparison between the two groups on key variables.
Interventions
The two interventions followed an identical structure, including unstructured time (break) for 20 min during the middle of each of the sessions. Both groups consisted of 6 to 9 participants.
Socio-Dramatic Affective-Relational intervention (SDARI)
SDARI is a group-based performance-based social skills intervention designed to provide participants the experience of successfully engaging in and learning a target social skill, with minimal didactic instruction or instrumental reinforcement of that skill. Detailed description of SDARI procedure have been previously described13,21,30. SDARI has three main aspects: (1) SDARI utilizes affectively-motivating acting games adapted for this age group and population. Specifically, the SDARI manual contains more than 100 games that target specific goals of the day (e.g., perspective-taking or interpretation of body language), and clinicians and participants collaboratively choose games among the available games that align with the goals and are developmentally-appropriate for the participants in the group. For example, a group with younger participants may engage in cooperative play-based games, while a group with older adolescents participates in team challenges or improvisational games centered on real-world social scenarios that are relevant to adolescents. In the current study, the goals were consistent across cohorts and we assessed fidelity to these weekly curriculum and goals. (2) Clinicians promote strong relationships between participants, and between participants and clinicians, to support positive social reinforcement by fostering a supportive and enjoyable environment, facilitating structured and unstructured social interactions, encouraging collaborative problem-solving, and reinforcing positive peer engagement. (3) SDARI also uses strong motivators—such as noncompetitive physical activities, shared interests, and goal-oriented activities—to enhance social motivation and engagement.
Fun activities for children and teens (FACT)
The other intervention used structured recreational activities that are not necessarily inherently social (e.g. art projects). Similar to SDARI, FACT aimed to provide enriched environments for reinforcing peer interaction in the absence of explicit instruction. However, unlike the SDARI condition, there was no use of affectively-motivating acting games. The core program principles of FACT were as follows: (1) Use of recreational, motivational activities adapted for this age/population, (2) Positive social reinforcement through the use of activities, and (3) Use of strong age-appropriate motivators.
Comparisons of modules between the two conditions are described in Supplementary Material 1.
Therapists and treatment integrity
Both interventions were led by graduate-level and postdoctoral-level clinicians (three clinicians in each group), who received extensive training and weekly supervision by a PhD-level psychologist with 15 + years of experience. Notably, therapists received tightly-matched training (identical in length, materials, location, except for the core activities associated with conditions). To limit the potential impact of individual clinician or allegiance effects on obtained outcomes31, we systematically rotated clinicians between conditions throughout the study cycles to the extent possible. This rigorous, balanced approach ensured that no single clinician was predominantly associated with any particular condition.
Clinicians completed fidelity measures13 each week to ensure that curriculum content and staff behaviors are consistent across groups, and do not significantly deviate from, training materials of each condition. Fidelity was also monitored each week via staff discussion and session tape review by the supervisor to minimize intervention cross-contamination. Clinicians showed excellent manual fidelity (activities completed in the session were indicated in the treatment manual) in both conditions (SDARI = 96.8%, FACT = 97.0%; n.s.). Conceptual fidelity (how much intervention staff members adhered to performance-training principles) of SDARI approach was higher in SDARI (mean score out of 5, SDARI = 3.68 vs. FACT = 3.49, p < .001), indicating that—as expected—while clinicians in both groups were equally adherent to the manualized elements of their respective interventions, SDARI clinicians endorsed greater adherence to the principles of SDARI.
Measures
EEG metric of social information processing
Participants completed the Diagnostic Analyses of Nonverbal Accuracy (DANVA-2)32, a measure of visual (facial) emotion recognition while EEG was simultaneously recorded. During the DANVA-2 facial emotion categorization task, participants viewed 48 color photographs of adult and child faces that ranged in emotional intensity (24 high- and 24 low-intensity) and emotional valence (12 happy, 12 sad, 12 angry, and 12 fearful). Each face was presented on the screen for a minimum of 1,000 ms and a maximum of 3,000 ms. Participants categorized the emotion of each face using a button box and their responses cued trial advancement. There was a 1,000 ms inter-trial interval during which a blank screen was presented. EEG data was recorded using a Brain Products 32-channel BrainVision actiCAP with active electrodes and amplified using an actiCHamp amplifier. The N170 latency was scored as the negative-going peak between 160 and 220 ms at electrode sites P7 and P8. Details of EEG data acquisition and reduction are described in Supplementary Material 3.
Observer-rated spontaneous peer interactions
Video recordings of sessions were used for observational coding of social interactions from unstructured play sessions each week within the SDARI and AC sessions, using a modified version of Social Interaction Observation Scale (SIOS)11,33. SIOS is an observational measure to assess positive, negative, and low-level social interactions in autistic youth, where raters observe and rate a maximum of three characteristic behaviors within each 1-minute segment. In the current study, overall spontaneous peer interaction (across positive, negative, and low-level) was examined. Each session was double-coded by a team of research assistants who were naïve to study hypotheses and blinded to group conditions, chronology of videos, and the mean score between two coders was used in analyses to reduce measurement error. Additional details related to training, coding process, and reliability assessments are described in Supplementary Material 2.
Peer-reported reciprocal friendships
The peer-reported Sociometric interview was conducted after sessions 1, 5, and 10, regarding the peers within their group to assess friendship-making patterns and perceived acceptance by within-group peers (liking, disliking, desire to play again, and reciprocal friendship)34. Questions were read aloud to participants by trained research assistants, and participants responded by pointing to the picture of the child they were nominating or saying the number on the Likert-type scale with visuals. To account for different group size, reciprocal friendships were calculated by considering the number of peers the participant nominated as a friend who also nominated them as a friend in return, then deriving a proportion score of the total number of participants in the group.
Parent-report social skills
At pre-test, post-test, and 10-week follow-up, participants and their parents completed the Social Skills Improvement System (SSIS)35. The SSIS is a widely-used 46-item measure of overall frequency of social skills behavior. Social skills ratings were quantified using Social Skills Standard Scores. Parents also completed Social Responsiveness Scale-Second Edition (SRS-2)36, which is a measure developed specifically to address the level of social skills related to autism in autistic youth. Additionally, parents reported the perceived condition at endpoint via a participant condition assignment questionnaire that asked in which condition that parents believed their child participated. To ensure that parents are blinded to treatment condition, this measure was administered to parents after all intervention sessions have been completed.
Randomization and blinding
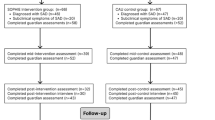
After eligibility was determined and participants provided consent, participants were randomly assigned to SDARI or AC (see Fig. 1 for CONSORT Flow Diagram and Checklist). Randomization was accomplished via a random number generator, using assignment procedures corresponding to those used in previous randomized control studies, including those examining group social skills interventions for autistic youth37,38. Participants and their caregivers were blinded to the randomization sequence and unaware of study hypotheses.

CONSORT Flow Diagram.
Statistical analysis
Generalized Estimating Equations (GEE)39 were used to estimate effects of timepoints on change in dependent variables while accounting for nesting within groups. These models are appropriate for the present data structure, in which participants are nested within small groups, and group-level variation must be accounted for, but no group-level predictors are of interest. As all outcome measures were continuous variables, a normal distribution and identity link function were used. To determine the best-fitting model for the data, (1) we modeled timepoint as either a continuous or an ordinal variable in the model, and (2) ran independent, unstructured, and autoregressive correlation matrix structure models for each outcome measure. We compared the goodness of fit of the model using the quasi-likelihood information criterion (QIC). Significant effects using two-tailed tests were followed up using Fisher’s least significant difference (LSD). Separate models were run for each outcome measure. If significant effects of timepoint*condition were found for an outcome measure, we probed the subscales to see if effects were also present. In all analyses, if the best-fitting model represented timepoint as an ordinal variable, we conducted post-hoc difference contrasts between timepoints, using LSD adjustment for multiple comparisons. Please contact the authors for inquiries regarding the fit comparisons across all tested models.
We conducted an exploratory analysis examining parent expectancy effect by comparing SSIS-Parent scores and SRS-2 scores using perceived condition rather than actual condition.
Results
Sample characteristics and baseline information
Table 1 summarizes demographic information in SDARI and AC conditions, as well as means and standard deviations of primary outcome measures. There were no differences in demographic characteristics across conditions.
Outcomes
EEG metric of social information processing
The SDARI and AC conditions differed in their changes in N170 latency to faces (Wald’s X2 = 6.00, p < .05), where the SDARI group evinced accelerated N170 latency to faces (Fig. 2) over the course of the intervention, which remained at follow-up.

Changes in N170 Event-related potential (ERP) latency to faces following Socio-Dramatic Affective Relational Intervention (SDARI) and Active Control (AC) at endpoint and follow-up.
Observer-rated spontaneous peer interactions
As measured by the SIOS, differences were seen between conditions (Wald’s X2 = 4.87, p < .05), where greater amount of spontaneous peer interactions were observed during the earlier sessions in SDARI group (Wald’s X2 = 35.87, p < .001; Fig. 3A). In terms of specific interaction types, there were no significant differences between conditions for either negative or low-level interactions (p > .15), while positive peer interactions revealed marginal differences across conditions (Wald’s X2 = 2.97, p = .085), where a trend was observed for more positive peer interactions in SDARI group (Wald’s X2 = 2.75, p < .10).

(A) Mean levels of spontaneous peer interaction during unstructured break time across 10 sessions, and (B) peer sociometrics, specifically in reciprocal friendship ratio, after first session and last session of Socio-Dramatic Affective Relational Intervention (SDARI) and Active Control (AC). Error bars denote standard error.
Peer-reported reciprocal friendships
In comparison to the AC condition, SDARI led to improvements in peer sociometrics, specifically in reciprocal friendships (Wald’s X2 = 6.52, p < .05). SDARI participants evinced higher levels of reciprocated friendships after Session 1, whereas AC participants reached similar level of reciprocated friendships by Session 10 (Fig. 3B).
Parent-reported social skills
There were no differences between actual conditions for both parent and self-reported SSIS or the SRS-2 (p > .90). However, in terms of exploratory analysis of parent expectancy effect, improvements on the SSIS-Parent were attributable to perceived condition (Wald’s X2 = 6.256, p < .05; Fig. 4). There were no differences between perceived conditions on the SRS-2 scores (p = .69).

Parent-report social skills scores by perceived condition, not actual condition, of Socio-Dramatic Affective Relational Intervention (SDARI) and Active Control (AC) at endpoint and follow-up.
Discussion
The present study is the one of the first single-blind randomized attention-controlled trials of a GSSI for autistic youth, and the first to explicitly control for perceived condition among informants and utilize a tightly-matched active control condition, representing a significant step forward in improving the evidence base in autism intervention research40. Incorporating multi-informant measurement approaches, including neural and behavioral indices, results indicate SDARI-specific and durable improvements in the N170, a neural biomarker associated with ASD8,41, as well as faster achievement of positive spontaneous peer interaction and reciprocal friendships. Utilizing the most rigorous methodology to date in the GSSI for ASD literature, these results indicate that this intervention evinces changes on multiple objective and reliable outcome metrics that are minimally subject to reporter bias.
SDARI has demonstrated positive effects on range of outcomes13,21,23; however, it was previously unclear if these effects were due to activities specific to SDARI, nonspecific supportive elements, or expectancy effects – as is the case for all prior studies evaluating GSSI for autistic youth. In contrast, one major contribution of this study was to isolate – for the first time – a putative active ingredient of a specific GSSI for autistic youth by comparing it to a rigorous AC design that is tightly-matched and otherwise identical to the SDARI model. These results offer support for the efficacy of specific activities of this intervention, which focus on providing spontaneous social learning opportunities in the context of an enriched environment rather than providing explicit social knowledge. Autistic youth appear to have greater difficulty with actually carrying out social skills during interactions than acquiring explicit social knowledge42,43, suggesting that this model may offer specific benefits for improving social skills in autistic youth. Relatively higher conceptual fidelity in SDARI in the current study, as well as in a prior RCT13, may represent that SDARI activities, compared to recreational activities of FACT or knowledge-based approaches, may align well with its core theoretical framework and intended mechanisms around using performance-based approaches, focus on relationship-building, and the use of strong age-appropriate motivators. Indeed, maintaining high fidelity to these core principles are in line with neurodiversity-affirming interventions focusing on authentic social connections and building social competence on their own terms, rather than enforcing neurotypical social norms that may pressure autistic individuals to mask autistic traits and approximate non-autistic behaviors43,44. Specifically, SDARI activities support participants in navigating social interactions by leveraging their strengths and interests and by fostering environments that encourage and reinforce them.
This study also assessed the effects of SDARI on parent-reported variables identified to be relevant to social skills development, while addressing the question of parental expectancy. Results suggest that parent-report effects were attributable to expectations of perceived condition, not SDARI-specific. The lack of group differences in parent-reported measures may reflect two possibilities. First, these measures might not be sensitive enough to detect the specific social and cognitive changes captured by objective assessments, or behavioral changes may take longer to manifest outside the intervention setting. Second, these results are in line with findings that revealed placebo-like response in caregiver ratings and how participation alone can reliably influence how caregivers perceive their children’s behaviors5. Our results suggest that parents’ expectations and hopes about the effects of a given intervention may account for more variance in reported changes than previously recognized. This highlights the need for caution regarding the use of parent-report as the sole outcome marker in treatment research without accounting for expectancy effects.
Considering the impact of expectancy effects on parent-reported outcomes, development of novel and objective markers of treatment progress is essential45. Nonetheless, limited work has explored neural changes in response to behavioral interventions for autistic46. This study is among the first to show changes in relevant neural indices of social cognition, demonstrating their utility as outcome measures of interventions. It is possible that the latency of the N170 ERP may be a target engagement biomarker, which would indicate response of social brain circuitry from an intervention45,47. Currently, there are no biomarker that can consistently predict treatment response in ASD clinical trials48. Future work should examine whether the N170 may serve as a predictor of treatment response, thereby providing insights to clinicians for identifying who will most likely benefit from psychosocial intervention41,45. Moreover, it would be important to understand how changes in N170 latency may be linked to other social outcomes. Existing literature suggests mixed associations between N170 and social functioning, highlighting the complexity of using early neural markers to predict real-world social competencies. Given these inconsistencies, future research should employ multi-level analyses—integrating neural, social cognitive, and ecological (behavioral and informant-reported) measures—to better capture the nuanced relationships between N170 and broader social abilities in autistic youth. Understanding how N170 responses relate to social outcomes will strengthen its potential utility as a biomarkers in clinical trials, both for participant selection and stratification, and for elucidating mechanisms of change49.
It is also significant that SDARI group evinced increased reciprocal friendship, as many autistic youth have few or no reciprocated friends but report wanting them50,51. Indeed, loneliness is a great concern among autistic youth52. Although many GSSIs focus on facilitating friendship-making outside the group, it is especially encouraging that participants in this study were able to increase friendship-making within group given the importance of having even one friend. Additionally, a growing body of literature on neurodiversity-affirming approaches highlights the unique importance of friendship-making among autistic individuals44,53,54, with these results highlighting this as a feasible and critical outcome for this intervention.
Further, observed change in social behavior in unstructured social interaction over the course of the intervention represents an objective marker of change and may indicate real-time generalization of skills54. Our findings from sociometrics and observed behaviors suggest that SDARI may be linked to rapid peer liking by facilitating social interaction during unstructured time from early in the intervention. One possible SDARI-specific mechanism involves naturalistic modeling of successful interactions that allow for performance-based learning approaches for autistic youth55. Notably, these patterns were similarly found in a previous RCT, where more immediate interactions were shown in SDARI13. Taken together, these findings show initial benefits following the SDARI intervention, although these differences diminish over time. This aligns with research that positive first impressions can lead to increased social interaction and can play a role in shaping new friendships56,57. Similarly, structured interventions like SDARI may help autistic individuals establish rapid peer connections. It will be important to consider how early social gains in SDARI can be sustained in real-world settings and whether additional supports, such as follow-up group sessions or school- or community-based interventions, can help promote more sustainable friendships.
Several limitations bear mentioning that also serve as fertile grounds for exploring future directions. First, the current RCT employed a 10-week version of an intervention originally designed as a more intensive summer program13,21,22. Given our findings, future work should examine optimal dosing of this intervention to maximize benefits for autistic youth. Although we maintained three-year age ranges within groups and tailored engagement methods to the participants’ developmental levels, this age span may present challenges. For example, the difference between elementary and secondary school contexts may significantly impact social dynamics and peer relationships, even within a three-year range. This limitation in not fully accounting for age-related factors should be addressed in future research. Another potential limitation of this study is that intervention fidelity was based on self-reports from clinicians who rotated between two conditions, which may not accurately reflect inadvertent mixing of intervention approaches. Future research should incorporate observational coding of a subset of sessions by independent study personnel to corroborate fidelity assessments. In addition, changes in neural indices require more frequent sampling of EEG is warranted to parse out directionality of effects. Future work should employ designs to better elucidate what specific activities of SDARI may be responsible for their effects. The findings of the study also provide avenues for considering potential moderators of the intervention outcome to better understand for whom and under what conditions to maximize benefit from treatment.
The present study expands the GSSI literature by providing one of the first single-blind randomized attention-controlled trials of a GSSI for autistic youth, and the first to utilize a tightly-matched active control condition as well as control for perceived condition by informants. Using standardized observational, electrophysiological, parent-report, and sociometric measures, along with rigorously controlled active attention control design, the current study provides evidence for SDARI-specific effects that are not attributable to non-specific supportive elements. Results demonstrate specific effects on neural indices of social processing, sociometrics, and observer-rated social behavior, and demonstrate the utility of objective markers of treatment response. However, our findings also suggest that outcomes such as spontaneous peer interactions and reciprocal friendships may be accomplished – albeit more slowly – without SDARI activities in a supported group setting. Finally, our results raise caution regarding the use of parent-report as the sole outcome marker in treatment research without accounting for expectation effects. In sum, our results provide clear directions for future work in research and implementation of GSSIs for autistic youth.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on a reasonable request.
References
Gates, J. A., Kang, E. & Lerner, M. D. Efficacy of group social skills interventions for youth with autism spectrum disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 52, 164-181 (2017).
McMahon, C. M., Lerner, M. D. & Britton, N. Group-based social skills interventions for adolescents with higher-functioning autism spectrum disorder: a review and looking to the future. Adolesc Health Med Ther 2013, 23–28 (2013).
Reichow, B., Steiner, A. M. & Volkmar, F. Social skills groups for people aged 6 to 21 with autism spectrum disorders (ASD). Campbell Systematic Reviews 8, 1-76 (2012).
White, S., Keonig, K. & Scahill, L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J. Autism Dev. Disord. 37, 1858–1868 (2007).
Jones, R. M., Carberry, C., Hamo, A. & Lord, C. Placebo-like response in absence of treatment in children with autism. Autism Res. 10, 1567–1572 (2017).
Aldao, A. & De Los Reyes, A. Commentary: a practical guide for translating basic research on affective science to implementing physiology in clinical child and adolescent assessments. J. Clin. Child. Adolesc. Psychol. 44, 341–351 (2015).
Dolan, B. K. et al. Brief report: assessment of intervention effects on in vivo peer interactions in adolescents with autism spectrum disorder (ASD). J. Autism Dev. Disord. 46, 2251–2259 (2016).
Webb, S. J. et al. The autism biomarkers consortium for clinical trials: initial evaluation of a battery of candidate EEG biomarkers. Am. J. Psychiatry. 180, 41–49 (2023).
Kang, E. et al. Atypicality of the N170 Event-Related potential in autism spectrum disorder: A Meta-analysis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 3, 657–666 (2018).
Kala, S. et al. Brief report: preliminary evidence of the N170 as a biomarker of response to treatment in autism spectrum disorder. Front. Psychiatry. 12, 1–7 (2021).
McNair, M. L., Keenan, E. G., Houck, A. P. & Lerner, M. D. Seeking contexts that promote neurodiverse social success: patterns of behavior during minimally-structured interaction settings in autistic and non-autistic youth. Dev. Psychopathol. 36, 1669-1684 (2023).
Locke, J., Kasari, C., Rotheram-Fuller, E., Kretzmann, M. & Jacobs, J. Social network changes over the school year among elementary school-aged children with and without an autism spectrum disorder. School Ment Health. 5, 38–47 (2013).
Lerner, M. D. & Mikami, A. Y. A preliminary randomized controlled trial of two social skills interventions for youth with High-Functioning autism spectrum disorders. Focus Autism Other Dev. Disabl. 27, 147–157 (2012).
Weisz, J. R., Weersing, V. R. & Henggeler, S. W. Jousting with straw men: comment on westen, novotny, and Thompson-Brenner (2004). Psychol. Bull. 131, 418–426 (2005).
Koenig, K. et al. Promoting social skill development in children with pervasive developmental disorders: A feasibility and efficacy study. J. Autism Dev. Disord. 40, 1209–1218 (2010).
Lopata, C., Donnelly, J. P., Rodgers, J. D. & Thomeer, M. L. Systematic review of data analyses and reporting in group-based social skills intervention RCTs for youth with ASD. Research in Autism Spectrum Disorders 59, 10–21 (2019).
Kamps, D. et al. A comprehensive peer network intervention to improve social communication of children with autism spectrum disorders: A randomized trial in kindergarten and first grade. J. Autism Dev. Disord. 45, 1809–1824 (2015).
Kazdin, A. E. Research Design in Clinical Psychology (Cambridge University Press, 2021).
Corbett, B. A. et al. Peers, play, and performance to build social salience in autistic youth: A multisite randomized clinical trial. J. Consult Clin. Psychol. 91, 411-425 (2023).
Afsharnejad, B. et al. KONTAKT® social skills group training for Australian adolescents with autism spectrum disorder: a randomized controlled trial. Eur. Child. Adolesc. Psychiatry 31, 1695–1713 (2022).
Lerner, M. D., Mikami, A. Y. & Levine, K. Socio-dramatic affective-relational intervention for adolescents with asperger syndrome & high functioning autism: pilot study. Autism 15, 21–42 (2011).
Kang, E. et al. Alliance-Outcome associations in a Community-Based social skills intervention for youth with autism spectrum disorder. Behav. Ther. 52, 324-337 (2021).
Marro, B. M. et al. Social performance–based interventions promote gains in social knowledge in the absence of explicit training for youth with autism spectrum disorder. Bull. Menninger Clin. 83, 301–325 (2019).
Gerber, A. H. et al. Predictors of treatment response to a Community-Delivered group social skills intervention for youth with ASD. J. Autism Dev. Disord. 53, 3741-3754 (2023).
Rutter, M., Bailey, A. & Lord, C. The Social Communication Questionnaire: Manual (Western Psychological Services, 2003).
Lord, C. et al. Autism Diagnostic Observation Schedule–2nd Edition (ADOS-2) (Western Psychological Services, 2012).
Kaufman, A. S. & Kaufman, N. L. Kaufman Brief Intelligence Test, 2nd Edition (Pearson, 2004).
Kang, E., Santore, L. A., Rankin, J. A. & Lerner, M. D. Self-reported social skills importance ratings, not social skills themselves, predict sociometric status among youth with autism spectrum disorder. Res. Autism Spectr. Disord. 74, 101552 (2020).
Kang, E., Clarkson, T., Keifer, C. M., Rosen, T. E. & Lerner, M. D. Discrete electrocortical predictors of anxiety and anxiety-related treatment response in youth with autism spectrum disorder. Biol. Psychol. 146, 107710 (2019).
Lerner, M. D. & Levine, K. The spotlight program: an integrative approach to teaching social pragmatics using dramatic principles and techniques. J. Dev. Processes. 2, 91–102 (2007).
Mohr, D. C. et al. The selection and design of control conditions for randomized controlled trials of psychological interventions. Psychotherapy and Psychosomatics 78, 275–284 (2009).
Nowicki, S. Manual for the Receptive Tests of the Diagnostic Analysis of Nonverbal Accuracy 2 (Emory University, 2004).
Bauminger, N. The facilitation of social-emotional Understanding and social interaction in high-functioning children with autism: intervention outcomes. J. Autism Dev. Disord. 32, 283–298 (2002).
Coie, J. D., Dodge, K. A. & Coppotelli, H. Dimensions and types of social status: A cross-age perspective. Dev. Psychol. 18, 557–570 (1982).
Gresham, F. & Elliott, S. Social Skills Improvement System: Rating Scales Manual (NCS Pearson, 2008).
Constantino, J. N. Social Responsiveness Scale, Second EditionWestern Psychological Services, Torrance, CA,. (2012).
Laugeson, E. A., Frankel, F., Mogil, C. & Dillon, A. R. Parent-assisted social skills training to improve friendships in teens with autism spectrum disorders. J. Autism Dev. Disord. 39, 596–606 (2009).
Owens, G., Granader, Y., Humphrey, A. & Baron-Cohen, S. LEGO® therapy and the social use of Language programme: an evaluation of two social skills interventions for children with high functioning autism and asperger syndrome. J. Autism Dev. Disord. 38, 1944–1957 (2008).
Hanley, J. A., Negassa, A., de Edwardes, M. D., Forrester, J. E. & B. & Statistical analysis of correlated data using generalized estimating equations: an orientation. Am. J. Epidemiol. 157, 364–375 (2003).
Bottema-Beutel, K. We must improve the low standards underlying evidence-based practice. Autism 27, 269–274 (2023).
Kang, E. et al. Archival report atypicality of the N170 Event-Related potential in autism spectrum disorder: A Meta-analysis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 3, 657–666 (2018).
Gates, J. A., Gerber, A. H., Miller, C. E. & Lerner, M. D. Quantifying social skill deficits and strengths profiles in autistic youth. Child Dev. 94, 659-673 (2023).
Gates, J. A., McNair, M. L., Richards, J. K. & Lerner, M. D. Social knowledge & performance in autism: A critical review & recommendations. Clin. Child. Fam Psychol. Rev. 26, 665–689 (2023).
Lerner, M. D., Gurba, A. N. & Gassner, D. L. A framework for neurodiversity-affirming interventions for autistic individuals. J. Consult Clin. Psychol. 91, 503–504 (2023).
McPartland, J. C. Developing clinically practicable biomarkers for autism spectrum disorder. J. Autism Dev. Disord. 47, 2935–2937 (2017).
Stavropoulos, K. K. M. Using neuroscience as an outcome measure for behavioral interventions in autism spectrum disorders (ASD): A review. Res. Autism Spectr. Disord. 35, 62–73 (2017).
McPartland, J. C. Considerations in biomarker development for neurodevelopmental disorders. Curr. Opin. Neurol. 29, 1 (2016).
Parellada, M. et al. In search of biomarkers to guide interventions in autism spectrum disorder: A systematic review. Am. J. Psychiatry 180, 23–40 (2023).
Lerner, M. D. & Day, T. C. Beyond the landmarks: where to next with biomarkers of autism?? Am. J. Psychiatry. 180, 5–7 (2023).
Bauminger, N. et al. Children with autism and their friends: A multidimensional study of friendship in high-functioning autism spectrum disorder. J. Abnorm. Child. Psychol. 36, 135–150 (2008).
Mendelson, J. L., Gates, J. A. & Lerner, M. D. Friendship in school-age boys with autism spectrum disorders: A meta-analytic summary and developmental, process-based model. Psychol. Bull. 142, 601–622 (2016).
Hymas, R., Badcock, J. C. & Milne, E. Loneliness in autism and its association with anxiety and depression: A systematic review with Meta-Analyses. Rev. J. Autism Dev. Disord. 35, 815–825 (2022).
Granieri, J. E., McNair, M. L., Gerber, A. H., Reifler, R. F. & Lerner, M. D. Atypical social communication is associated with positive initial impressions among peers with autism spectrum disorder. Autism 24, 1841–1848 (2020).
Heasman, B. & Gillespie, A. Neurodivergent intersubjectivity: distinctive features of how autistic people create shared Understanding. Autism 23, 910–921 (2019).
McDonald, R. G. et al. Performance- and Theater-Based interventions for supporting social cognition and social communication in autistic youth: A review and theoretical synthesis. Semin Speech Lang. 43, 255–276 (2022).
Sunnafrank, M. & Ramirez, A. At first sight: persistent relational effects of get-acquainted conversations. J. Soc. Pers. Relat. 21, 361–379 (2004).
Baker, L. R., Sizemore, R. N. & Vrshek-Schallhorn, S. Biased first impressions yield positive illusions that facilitate friendship initiation. J. Soc. Pers. Relat. 42, 873-900 (2025).
Acknowledgements
This study was supported by the Stony Brook Department of Psychiatry Pilot Grants Program. The funder had no role in study design; the data collection, analysis, and interpretation; manuscript writing; and the decision to submit the article for publication. The authors wish to thank Rebecca J. Weber for coordinating recruitment and data collection. Authors report no biomedical financial interests or potential conflicts of interest.
Author information
Authors and Affiliations
Contributions
M.D.L. acquired funding for the study and supervised the study. E.K., T.E.R., and M.D.L. designed the study. E.K., T.E.R., C.M.K., A.H.G., and M.D.L. collected data. E.K. and M.D.L. analyzed the results. All authors wrote the manuscript text and E.K. prepared the figures and A.H.G. prepared the table. E.K. revised the manuscript based on reviewer feedback, and A.H.G. and M.D.L. provided input and edits. All authors reviewed and approved the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kang, E., Rosen, T.E., Keifer, C.M. et al. A single-blind active-control randomized controlled trial of group-based social competence intervention. Sci Rep 15, 28872 (2025). https://doi.org/10.1038/s41598-025-12876-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12876-w
