
Abstract
We aim to investigate if myocardial bridging (MB) provides predictive value beyond its association with non-obstructive coronary artery disease (CAD) burden in a long-term follow-up and multicenter study. This study included 4176 consecutive patients with suspected CAD underwent coronary computed tomography angiography (CTA) at two hospitals in Wuhan, China, between September 2016 and December 2017 for finial analysis. Kaplan-Meier method was used to estimate the cumulative event-free survival of non-obstructive CAD burden and MB burden classifications, respectively. Further, cox regression models were applied to calculate hazard ratios (HR) for increasing non-obstructive CAD and MB burden classifications. In total, during the 6.04 years (interquartile range 5.73–6.32) follow-up, 276 (6.61%) patients occurred main adverse cardiovascular events (MACE). MB was found in 44% of patients without CAD and in 40.5% of those with non-obstructive CAD. The annualized MACE rate was 1.07 (95% confidence interval (CI): 0.92–1.24) for the no MB group and 1.13 (95% CI: 0.95–1.34) for the MB group. Univarite and Multivariate Cox regression showed that neither the depth nor the length of MB was associated with the risk of MACE. However, after adjusting with sex, age, smoke, drink, hypertension and diabetes, 2-vessel non-obstructive CAD and 3-vessel non-obstructive CAD showed significant association with the risk of MACE, with HR of 1.53 (95% CI: 1.06–2.21, P = 0.023) and 1.93 (95% CI: 1.32–2.82, P = 0.001), respectively, using no CAD as the reference group. Non-obstructive CAD, not presence of MB, is the main predictor of risk for future MACE in patients without obstructive CAD. Prospective registries in the future should include validated quality of life measures and CT-FFR with long-term outcomes to enhance the understanding of symptomatic burden and functional assessment in MB risk stratification.
Similar content being viewed by others

Introduction
Myocardial bridging (MB) is a congenital variation of coronary artery that most frequently involves the middle-left anterior descending artery (mLAD)1,2,3,4. The results derived from previous studies suggest that MB has been considered as a benign incidental finding5,6,7. Nevertheless, recent reports reveal that the presence of MB is associated with an increased risk of ischemia, acute coronary syndrome, non-fatal myocardial infarction (MI) and death4,8,9,10,11. Furthermore, a recent meta-analysis report indicates that MB is associated with a poor prognosis12. Therefore, the prognosis of MB remains controversial, with the exact clinical significance still unclear according to previous studies.
Previous studies mainly focus on the prognosis between MB and MI with non-obstructive coronary arteries or non-obstructive coronary artery disease (CAD)6,10. Nonetheless, these studies primarily included patients with stenosis due to coronary plaque, which might be a confounding factor influencing the results. Therefore, it is still uncertain if the high risk of adverse events is due to the presence of MB or if it is related to its association with stenosis from atherosclerotic plaque. In the current study, we aim to investigate the prevalence of MB detected by coronary computed tomography angiography (CTA) and explore if the presence of MB provides predictive value beyond its association with non-obstructive CAD burden in a long term follow-up study.
Methods
The trial protocol of this retrospective and observational study has been reviewed and approved by the ethics committee of the Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology. Written informed consent in the current study was waived as it was a retrospective observational study design. We confirmed that all methods were performed in accordance with the relevant guidelines and regulations.
Study population
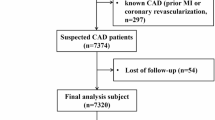
This current study was conducted on 6581 consecutive patients with suspected CAD underwent coronary CTA at two hospitals in Wuhan, China, between September 2016 and December 2017. Our previous research has reported the rational details of the study with parts of patients13. If the same patient underwent multiple coronary CTA examinations during the study period, we select the earliest one to characterize CAD extent. The inclusion and exclusion criteria of the study were as follows: Inclusion criteria consisted of patients who were at least 18 years old and had a coronary CTA. The exclusion criteria included patients with inadequate imaging quality, no record of CAD severity, a previous MI or revascularization, obstructive CAD, and those who dropped out. Finally, 4176 patients in total were analyzed in the present study.
Coronary CTA protocol
Patients underwent coronary CTA examination based on the guidelines of Society of Cardiovascular Tomography (SCCT)14. The following multi-detector CT scanners were used in the current study: Philips Brilliance iCT (Philips Medical Systems, Best, the Netherlands); Aquilion 64 (Toshiba Medical Systems, Otawara, Japan); Somatom Definition AS (Siemens Healthineers, Germany). Coronary anatomy was evaluated using an 18-segment coronary artery tree. Curve planar reformat (CPR), volume rendering (VR), multiple planar reformat (MPR) and maximum intensity projection (MIP) images were reconstructed based on coronary tree segmentation. No CAD was defined as no visible stenosis in any coronary artery. Non-obstructive CAD was defined as minimal or mild stenosis (1–49%) in any other epicardial coronary artery15. We noted the presence of MB and defined MB as a segment of an epicardial coronary artery which overlaid by myocardium7. In this study, we use two classifications according to the depth and length of MB. Superficial MB was defined as with depth ≤ 2 mm and > 2 mm was defined as deep MB5. Short MB was defined as with length < 25 mm and ≥ 25 mm was defined as long MB16.The test of depth and length of MB was attributed to the more proximal segment if a coronary CTA case involving 2 MBs17. Short-axis and CRP images were used to measure the depth of MB and MPR images were used to measure the length of the MB.
Follow-up and endpoint
Main adverse cardiovascular events (MACE), defined as MI and stroke was the primary endpoint in this study. The local Community Health Service Centers provided the status of MACE. If MACE occurs outside of the city, we then ascertained the outcome through telephone call or medical records. The deadline date of follow-up was April 30, 2022. We guarantee that no new research participants are added between the inclusion deadline and the follow-up deadline.
Statistical analysis
Continuous variables were summarized as mean (± standard deviation), and categorical variables as numbers and percentages. Continuous variables were compared by using the one-way ANOVA test and categorical variables were compared by using chi-square test, as appropriate. The positional correlation between MB and plaque in non-obstructive CAD was determined using the Spearman correlation. We first used Kaplan-Meier method and log-rank test to estimate the cumulative event-free survival of non-obstructive CAD burden and MB burden classifications, respectively. Further, univariate and multivariate Cox proportional regression models were applied to calculate hazard ratios (HR) for increasing non-obstructive CAD and MB burden classifications. In the current study, we used a two-sided P < 0.05 as statistically significant. All statistical analyses were performed using R statistical package (version 4.0, R foundation for Statistical Computing, Vienna, Austria) and MedCalc Statistical Software (version16.8.4 Ostend, Belgium).
Results
In the final analysis, coronary CTA identified 2414 patients (57.8%) without MB and 1762 patients (42.2%) with MB. The average age of the 4176 patients was 59.8 ± 9.9 years, and 39.8% (1663 of 4176) were male. There is no significant difference between the no MB group and the MB group in the mean age and the proportion of drink, hypertension, diabetes (all P > 0.05). Higher proportion of male patients, patients with smoking and no CAD was found in MB group. The most frequent location was LAD, accounting for 1554 of the 1762 MB cases. The baseline characteristics of the current study patients were presented in Table 1. We have performed the positional correlation between MB and plaque of non-obstructive CAD and indicated a relatively poor correlation (supplementary Table 1). In addition, since MB and plaque are occasionally located in different vessels (for instance, MB in the LAD and plaque in the RCA), we explored the relationship between MB and plaque when they are in the same vessel. Out of the 711 cases where both plaque and MB were present in the same branch, 667 (93.8%) of the plaques were found proximal to the MB segments, compared to 6.2% distal (p < 0.001).
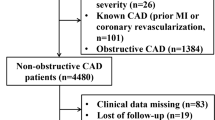
As showed in Fig. 1. No MB group had a higher prevalence of non-obstructive CAD than that of MB group. Among the patients with MB group, 49.5% had no CAD, 31.2% had 1-vessel non-obstructive CAD, 10.8% had 2-vessel non-obstructive CAD, and 8.5% had 3-vessel non-obstructive CAD.

Prevalence of patients with MB and no obstructive CAD in the present study. MB myocardial bridging, CAD coronary artery disease.
During the 6.04-year follow-up period (interquartile range 5.73–6.32), 276 patients, accounting for 6.61%, had MACE. The annualized MACE rate of the study patients was 1.09 (95% CI: 0.98–1.23). Furthermore, the annualized MACE rate was 1.07 (95% CI: 0.92–1.24) for the no MB group and 1.13 (95% CI: 0.95–1.34) for the MB group. In addition, the annualized MACE rate of the no CAD group and non-obstructive CAD group was 0.65(95% CI: 0.52–0.81) and 1.49 (95% CI: 1.31–1.70), respectively (Table 2). Figure 2 showed a significant association between the involvement vessel number of non-obstructive CAD and the increasing of cumulative events (P < 0.001). On the other hand, patients with MB did not show a significant difference in MACE rates compared to those without MB (P = 0.633). In addition, the classifications of depth (P = 0.601) or length (P = 0.841) with MB did not show significant association with MACE.

Cumulative event survivals. A No CAD vs. Non-obstructive CAD in all patients; B No MB vs. Any MB; C Depth classification of MB; D Length classification of MB. MB myocardial bridging, CAD coronary artery disease.
We then performed additional analyses to evaluate the relative importance of MB burden versus non-obstructive CAD burden for MACE. Both univariate and multivariate Cox regression analyses indicated that there was no correlation between the depth or length of MB and the risk of MACE. However, after adjusting with sex, age, smoke, drink, hypertension and diabetes, 2-vessel non-obstructive CAD and 3-vessel non-obstructive CAD showed significant association with the risk of MACE, with HR of 1.53 (95% CI: 1.06–2.21, P = 0.023) and 1.93 (95% CI: 1.32–2.82, P = 0.001), respectively, using no CAD as the reference group (Table 3).
Discussion
In this retrospective observational multicenter study, we first investigate MACE rate during a 6.04-year follow-up and observed that MB was found in 44% of patients without CAD and in 40.5% of those with non-obstructive CAD. Moreover, the present study suggested that non-obstructive CAD, not MB, is the main predictor of future MACE in patients without obstructive CAD.
Epidemiological studies have discovered that the prevalence of MB differs widely based on the methods used to identify this anatomical variant. Necropsy series have reported that the incidence rate of MB ranges from 5 to 86%18,19. The current study showed that the prevalence of MB is 42.2%, which is similar or higher than the previous retrospective and prospective studies6,20. Tarantini et al.. revealed that the average prevalence of MB was 25% in a recent review4. In addition, the depiction rate of MB in autopsy, coronary CTA and invasive coronary angiography (ICA) has decreased in descending order according to recent meta-analysis studies21,22. This trend suggests that the detection rate of MB via coronary CTA is more consistent with autopsy results, which may be attributed to the multiplane and 3-dimensional capabilities of new generation CT capable of refining MB4,12,23.
The present study found a low rate of MACE during a median follow-up of 6.04 years and there was no association between MB and the increased risk of MACE in patients without obstructive CAD. These findings were in consistent with previous study reported by Rubinshtein et al.6. However, there were only 334 patients enrolled in their study. Our sample size was larger within the similar follow-up time range. More importantly, we performed a subgroup analysis and suggested that non-obstructive CAD, not MB, was the main predictor of future MACE in patients without obstructive CAD. Recent studies have demonstrated that non-obstructive was found in patients with poor prognosis than in those with no CAD24,25,26. Our study confirmed these findings. Additionally, the presence of MB showed no significant impact on MACE in the cox regression analysis, confirming that MB is a non-threatening finding in patients without obstructive CAD. Although some studies, including a recent meta-analysis report, have showed that MB had an association with poor prognosis4,8,9,12, it may affect the results as the difference of non-obstructive CAD in no MB and MB groups was not considered in these studies.
Length of MB in the present study varies widely (2 to 54 mm), which is similar to previous studies7,27. Reports suggest that symptomatic patients are associated with long and/or deep MB, and the degree of proximal endometrial lesions in MB is closely linked to the MB’s length and thickness28. Moreover, the correlation between deep MB and long MB and occurrence of MI has been reported in some autopsy studies29. The length of coronary arteries stenosis without MB has been reported to accurately assess functional ischemia and related to hemodynamic disorders30. According to this theory, some researchers suggested that MB acts as a dynamic stenosis compressed across the myocardium during systole, which may influence hemodynamics due to its length. The current study found no link between MB length and future MACE, contrasting with a recent report suggesting MB length predicts abnormal fractional flow reserve derivation from coronary CTA (CT-FFR)1. However, this report included a small sample size (120 patients with MB and 41 controls). Furthermore, our study directly investigates the association between MB and prognosis, rather than hemodynamic status. The association between depth of MB and hemodynamic disturbances or poor prognosis is controversial. Previous research has revealed that deep MB is a predictor of risk for cardiovascular disease, and the MB thickness is significantly greater in patients with MI than those without MI31. Conversely, recent research showed that the depth of MB did not correlate with abnormal CT-FFR values or the development of coronary atherosclerosis1,30, aligning with our findings.
Some studies suggested the hemodynamic significance of MB should be assessed32. The latest study suggested that MB resulted in decreased efficiency of coronary perfusion during exercise in patients with angina and non-obstructive CAD33. In addition, in patients with non-obstructive CAD, coronary spasm linked to MB might indicate a more severe clinical presentation with MI and non-obstructive CAD and an increased likelihood of angina-related hospitalizations over the long term, despite a low incidence of major events9. In contrast, Negin et al. included 1251 patients with angia with non-obstructive CAD and showed that abnormal coronary flow reserve was not predictive of MACE in patients with MB34. While functional significance was not assessed in the present study, our finding that anatomic MB lacked prognostic importance may due to the largely asymptomatic or functionally insignificant MB. However, our findings partly imply that most MB visible on CT scans are not hemodynamically significant and may not present a long-term risk like atherosclerosis. Prospective studies combining thin-slice CT-FFR with long-term outcomes are needed to determine whether functional assessment improves MB risk stratification.
The study presents long-term comparative data showing that MB, when not accompanied by CAD, has a much better prognosis compared to non-obstructive CAD. Non-obstructive CAD plaque is the key determinant of MACE risk, not the presence of MB. This contributes to resolving the continuous debate regarding whether MB is an incidental finding or holds clinical significance. Moreover, this questions the existing practice where MB frequently gets more clinical focus than warranted. Our findings suggest reassurance can be provided to MB patients without concomitant atherosclerosis and more aggressive risk factor management should target non-obstructive CAD patients. In addition, the interpretation of our findings is restricted to the prognostic implications of MB for MACE, without considering its symptomatic influence. While MB did not predict MACE in our cohort, this does not preclude its importance as a cause of debilitating symptoms. The dissociation between anatomic findings and symptoms in MB patients warrants careful clinical evaluation. Future prospective registries that include validated quality of life tools are necessary to thoroughly understand the symptomatic burden of MB across different demographic groups.
Some limitations were present in the current study. First, as a retrospective design, this study had the selection bias and this may affect the prevalence of MB. However, we focus on comparing the rate of MACE in relation to the finding of MB in patients without obstructive CAD using coronary CTA. More importantly, considering non-obstructive CAD is a poor prognostic factor, we further performed subgroup analysis to reduce this bias. However, the lack of data on underlying systemic diseases and medications, combined with the retrospective nature of this study, suggests that selection bias might be present. In addition, as a retrospective study, we lacked systematic assessment of angina frequency or quality of life measures that might better reflect MB’s clinical impact, particularly in younger or female patients. This represents an important area for future prospective studies. Second, coronary CTA data are recorded based on the reports. As such, it is possible to record some incorrect classification of CAD severity. However, the individual characteristics of this CAD degree and its inherent inaccuracy are standard clinical care, which accurately reflect the CAD classification of the real world, thus providing information for contemporary clinical practice. Third, our findings based on coronary CTA data in the present study should not generalize to other patients or populations. As such, the current findings need to be further investigating in other populations. Forth, the current study had limited data on other indexes derived by coronary CTA, such as coronary artery calcium (CAC) or total plaque volume, which has been showed association with risk of MACE in non-obstructive CAD. Last, the anatomic definition of MB without functional correlation represents a study limitation. However, this reflects real-world practice where most MB is initially detected by CT without subsequent invasive assessment.
Non-obstructive CAD, not presence of MB, is the main predictor of risk for future MACE in patients without obstructive CAD. Prospective registries in the future should include validated quality of life measures and CT-FFR with long-term outcomes to enhance the understanding of symptomatic burden and functional assessment in MB risk stratification.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MB:
-
Myocardial bridging
- CTA:
-
Computed tomography angiography
- CI:
-
Confidence interval
- mLAD:
-
Middle-left anterior descending artery
- MACE:
-
Main adverse cardiovascular events
- MI:
-
Myocardial infraction
- CAD:
-
Coronary artery disease
- SCCT:
-
Society of Cardiovascular Tomography
- MPR:
-
Multiple planar reformat
- CPR:
-
Curve planar reformat
- VR:
-
Volume rendering
- MIP:
-
Maximum intensity projection
- HR:
-
Hazard ratios
- ICA:
-
Invasive coronary angiography
- CAC:
-
Coronary artery calcium
- LAD:
-
Left anterior descending artery
- LCX:
-
Left circumflex
- RCA:
-
Right coronary artery
References
Zhou, F. et al. Fractional flow reserve derived from CCTA May have a prognostic role in myocardial bridging. Eur. Radiol. 29, 3017–3026. https://doi.org/10.1007/s00330-018-5811-6 (2019).
Tarantini, G. & Cademartiri, F. Myocardial bridging and prognosis: more evidence but jury still out. Eur. Heart J. Cardiovasc. Imaging. 14, 515–517. https://doi.org/10.1093/ehjci/jet021 (2013).
Matta, A., Roncalli, J. & Carrie, D. Update review on myocardial bridging: new insights. Trends Cardiovasc. Med. 34, 10–15. https://doi.org/10.1016/j.tcm.2022.06.002 (2024).
Tarantini, G., Migliore, F., Cademartiri, F., Fraccaro, C. & Iliceto, S. Left anterior descending artery myocardial bridging: A clinical approach. J. Am. Coll. Cardiol. 68, 2887–2899. https://doi.org/10.1016/j.jacc.2016.09.973 (2016).
Dimitriu-Leen, A. C. et al. Long-Term prognosis of patients with intramural course of coronary arteries assessed with CT angiography. JACC Cardiovasc. Imaging. 10, 1451–1458. https://doi.org/10.1016/j.jcmg.2017.02.013 (2017).
Rubinshtein, R. et al. Long-term prognosis and outcome in patients with a chest pain syndrome and myocardial bridging: a 64-slice coronary computed tomography angiography study. Eur. Heart J. Cardiovasc. Imaging. 14, 579–585. https://doi.org/10.1093/ehjci/jet010 (2013).
Alegria, J. R., Herrmann, J., Holmes, D. R. Jr., Lerman, A. & Rihal, C. S. Myocardial bridging. Eur. Heart J. 26, 1159–1168. https://doi.org/10.1093/eurheartj/ehi203 (2005).
Corban, M. T. et al. Myocardial bridging: contemporary Understanding of pathophysiology with implications for diagnostic and therapeutic strategies. J. Am. Coll. Cardiol. 63, 2346–2355. https://doi.org/10.1016/j.jacc.2014.01.049 (2014).
Montone, R. A. et al. Interplay between myocardial bridging and coronary spasm in patients with myocardial ischemia and Non-Obstructive coronary arteries: pathogenic and prognostic implications. J. Am. Heart Association. 10, e020535. https://doi.org/10.1161/JAHA.120.020535 (2021).
Matta, A. et al. Myocardial bridging is significantly associated to myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. Acute Cardiovasc. Care. 11, 501–507. https://doi.org/10.1093/ehjacc/zuac047 (2022).
Laborante, R. et al. Antiplatelet therapy in myocardial bridge: insights from the RIALTO registry. J. Am. Heart Association. 14, e040513. https://doi.org/10.1161/JAHA.124.040513 (2025).
Zhu, C., Wang, S., Cui, H., Tang, B. & Wang, S. Associations of myocardial bridging with adverse cardiac events: a meta-analysis of published observational cohort studies involving 4,556 individuals. Annals Translational Med. 8, 369. https://doi.org/10.21037/atm.2020.02.24 (2020).
Huang, Z. et al. Prognostic value of CAD-RADS classification by coronary CTA in patients with suspected CAD. BMC Cardiovasc. Disord. 21, 476. https://doi.org/10.1186/s12872-021-02286-x (2021).
Leipsic, J. et al. SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the society of cardiovascular computed tomography guidelines committee. J. Cardiovasc. Comput. Tomogr. 8, 342–358. https://doi.org/10.1016/j.jcct.2014.07.003 (2014).
Huang, Z. et al. Clinical evaluation of the automatic coronary artery disease reporting and data system (CAD-RADS) in coronary computed tomography angiography using convolutional neural networks. Acad. Radiol. 30, 698–706. https://doi.org/10.1016/j.acra.2022.05.015 (2023).
Sternheim, D. et al. Myocardial bridging: diagnosis, functional assessment, and management: JACC State-of-the-Art review. J. Am. Coll. Cardiol. 78, 2196–2212. https://doi.org/10.1016/j.jacc.2021.09.859 (2021).
Brolin, E. B. et al. Prevalence of myocardial bridging in patients with myocardial infarction and nonobstructed coronary arteries. Am. J. Cardiol. 116, 1833–1839. https://doi.org/10.1016/j.amjcard.2015.09.017 (2015).
Mohlenkamp, S., Hort, W., Ge, J. & Erbel, R. Update on myocardial bridging. Circulation 106, 2616–2622. https://doi.org/10.1161/01.cir.0000038420.14867.7a (2002).
Rossi, L. et al. Myocardial bridges and ischemic heart disease. Eur. Heart J. 1, 239–245. https://doi.org/10.1093/oxfordjournals.eurheartj.a061125 (1980).
Sheu, M. H. et al. Myocardial bridging in taiwanese: noninvasive assessment by 64-detector row coronary computed tomographic angiography. J. Chin. Med. Association: JCMA. 74, 164–168. https://doi.org/10.1016/j.jcma.2011.01.037 (2011).
Roberts, W. et al. Myocardial bridges: A meta-analysis. Clin. Anat. 34, 685–709. https://doi.org/10.1002/ca.23697 (2021).
Hostiuc, S., Negoi, I., Rusu, M. C. & Hostiuc, M. Myocardial bridging: A Meta-Analysis of prevalence. J. Forensic Sci. 63, 1176–1185. https://doi.org/10.1111/1556-4029.13665 (2018).
Lee, M. S. & Chen, C. H. Myocardial bridging: an Up-to-Date review. J. Invasive Cardiol. 27, 521–528 (2015).
Maddox, T. M. et al. Nonobstructive coronary artery disease and risk of myocardial infarction. Jama 312, 1754–1763. https://doi.org/10.1001/jama.2014.14681 (2014).
Wang, Z. J., Zhang, L. L., Elmariah, S., Han, H. Y. & Zhou, Y. J. Prevalence and prognosis of nonobstructive coronary artery disease in patients undergoing coronary angiography or coronary computed tomography angiography: A Meta-Analysis. Mayo Clin. Proc. 92, 329–346. https://doi.org/10.1016/j.mayocp.2016.11.016 (2017).
Investigators, S. H. et al. Coronary CT angiography and 5-Year risk of myocardial infarction. N. Engl. J. Med. 379, 924–933. https://doi.org/10.1056/NEJMoa1805971 (2018).
Iguchi, T. et al. Impact of lesion length on functional significance in intermediate coronary lesions. Clin. Cardiol. 36, 172–177. https://doi.org/10.1002/clc.22076 (2013).
Herrmann, J., Higano, S. T., Lenon, R. J., Rihal, C. S. & Lerman, A. Myocardial bridging is associated with alteration in coronary vasoreactivity. Eur. Heart J. 25, 2134–2142. https://doi.org/10.1016/j.ehj.2004.08.015 (2004).
Ishikawa, Y. et al. Histopathologic profiles of coronary atherosclerosis by myocardial Bridge underlying myocardial infarction. Atherosclerosis 226, 118–123. https://doi.org/10.1016/j.atherosclerosis.2012.10.037 (2013).
Javadzadegan, A., Moshfegh, A., Mohammadi, M., Askarian, M. & Mohammadi, M. Haemodynamic impacts of myocardial Bridge length: A congenital heart disease. Comput. Methods Programs Biomed. 175, 25–33. https://doi.org/10.1016/j.cmpb.2019.03.017 (2019).
Ishikawa, Y. et al. Anatomic properties of myocardial Bridge predisposing to myocardial infarction. Circulation 120, 376–383. https://doi.org/10.1161/CIRCULATIONAHA.108.820720 (2009).
Beijk, M. A. M. et al. Myocardial bridging as a trigger in angina with no obstructive coronary artery disease. JACC Case Rep. 29, 102382. https://doi.org/10.1016/j.jaccas.2024.102382 (2024).
Sinha, A. et al. Characterizing mechanisms of ischemia in patients with myocardial bridges. Circ. Cardiovasc. Interv. 17, e013657. https://doi.org/10.1161/CIRCINTERVENTIONS.123.013657 (2024).
Mahmoudi Hamidabad, N. et al. Prognostic implications of resistive reserve ratio in patients with nonobstructive coronary artery disease with myocardial bridging. J. Am. Heart Association. 13, e035000. https://doi.org/10.1161/JAHA.124.035000 (2024).
Acknowledgements
We confirm that all methods were carried out in accordance with relevant guidelines and regulations.
Author information
Authors and Affiliations
Contributions
Study concepts: XW, ZFH, Study design: XW, ZFH, BBC, YY, YD, Data acquisition and analysis: XYD, WPW, ML, ZQL, XZ, Statistical analysis: ZFH, XW, Manuscript preparation: ZFH, BBC, YY, YD, Manuscript editing and review: XW, ZFH.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Review Committee of The Central Hospital of Wuhan (WHZXKYKL2022-140) and the written informed consent was waived by institutional ethics committee of The Central Hospital of Wuhan because of retrospective observational nature of the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Z., Cao, B., Yang, Y. et al. Prognostic value of myocardial bridging versus non-obstructive CAD: a long-term follow-up study. Sci Rep 15, 28159 (2025). https://doi.org/10.1038/s41598-025-13939-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-13939-8
Keywords
This article is cited by
-
Exploring the relationships between cardiac conditions and myocardial bridging in sudden cardiac death: a case control autopsy study
Egyptian Journal of Forensic Sciences (2025)
