
Abstract
Breast cancer is the most common malignant tumor among women worldwide. Hormone receptor-positive/HER2-negative (HR+/HER2-) breast cancer is the largest subgroup among these cases. The application of neoadjuvant chemotherapy (NACT) has rapidly increased in recent years, but its impact on long-term survival in HR+/HER2- breast cancer remains debated. This retrospective cohort study analyzed 21,299 stage II-III HR+/HER2- breast cancer patients from the SEER database (2010–2021), employing propensity score matching (PSM) to balance intergroup differences. Kaplan-Meier survival analysis and Cox proportional hazards regression were used to identify significant prognostic factors. Among 21,299 patients, 17.8% received NACT. After propensity score matching (PSM; n = 6,930), the NACT group still showed poorer OS (5-year 83.7% vs. 89.6%; 10-year 69.9% vs. 76.7%; P < 0.001) and BCSS (85.9% vs. 91.6%; 10-year 75.3% vs. 81.8%; P < 0.001). Multivariate analysis confirmed NACT as an independent risk factor for mortality (HR 1.44, 95% CI 1.30–1.59, p < 0.001). Notably, achieving Pathological Complete Response (pCR) (17.3% of NACT patients) did not improve survival, while non-pCR patients had worse outcomes than adjuvant chemotherapy (ACT) recipients (OS HR 1.58, BCSS HR 1.68, p < 0.001). Stratified analyses revealed consistent survival disadvantages for NACT in stage IIB–IIIC, T1–T3, and N0–N2 subgroups. For stage III patients undergoing Breast-Conserving Surgery(BCS), NACT was associated with significantly lower OS and BCSS compared to ACT. NACT in stage II-III HR+/HER2- breast cancer is associated with inferior long-term survival outcomes compared to ACT, particularly in patients with T1–T3 tumors or N0–N2 lymph node involvement. While NACT may enhance BCS rates, its use should be cautiously weighed against potential survival trade-offs. These findings highlight the need for personalized treatment strategies and further validation through prospective trials, especially given the limitations of retrospective SEER data.
Similar content being viewed by others

Introduction
Breast cancer remains one of the most prevalent malignancies and a leading cause of cancer-related mortality among women globally1,2. Hormone receptor-positive/HER2-negative (HR + /HER2-) breast cancer constitutes the largest subtype, accounting for approximately 70% of all breast cancer cases3,4. In recent years, the use of neoadjuvant chemotherapy (NACT) in breast cancer has increased rapidly5. NACT was historically employed as a preoperative treatment for inoperable breast cancer6. In recent years, its application has expanded to include operable breast cancer, where NACT is used to reduce tumor size before surgery7,8. This approach increases the feasibility of breast-conserving surgery and allows for the assessment of tumor response to chemotherapy9.
However, despite these theoretical benefits, its efficacy and necessity in HR + /HER2- breast cancer remain contentious. This is primarily due to lower pathological complete response (pCR) rates observed in this subtype, coupled with uncertain long-term benefits10. Moreover, limited comparative evidence exists regarding survival outcomes between non-pathological complete response(non-pCR) patients following NACT and those receiving postoperative adjuvant chemotherapy (ACT) 11.
Therefore, this study aims to reevaluate the role of NACT in Stage II-III HR + /HER2- breast cancer by comparing survival outcomes between patients undergoing NACT and those receiving ACT post-surgery, and by examining the correlation between pCR and both overall survival (OS) and breast cancer-specific survival (BCSS). Using the SEER database, we conducted a retrospective cohort study with propensity score matching (PSM) to create balanced cohorts. Kaplan–Meier survival analysis and Cox proportional hazards regression were employed to identify significant prognostic factors.
Our findings seek to provide deeper insights into the clinical management of HR + /HER2- breast cancer, potentially challenging the routine application of NACT in this subset, and emphasizing the importance of personalized treatment strategies.
Material and methods
Data source and patient selection
This study utilized data from the Surveillance, Epidemiology, and End Results (SEER) program managed by the U.S. National Cancer Institute, which provides critical national cancer statistics. Specifically, we used the SEER*Stat Database: Incidence—SEER Research Data, 17 Registries, November 2023 Submission (2000–2021), linked to county attributes and released in April 2024. All analyses adhered to SEER’s ethical guidelines and data use agreements, with all necessary permissions obtained.
Inclusion Criteria: Female patients;Diagnosed between 2010 and 2021; Diagnosed with infiltrating ductal carcinoma (ICD-O-3 code 8500/3);HR + /HER2- subtype; Single primary tumor;Primary site in the breast; Aged 15–79 years.
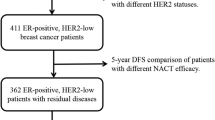
Exclusion Criteria:No surgical intervention;No chemotherapy;TNM stage I diagnosis;Metastatic (M1) disease;Incomplete neoadjuvant therapy information or missing key details (stage, grade, molecular type);Death or loss to follow-up within 3-months post-diagnosis.The detailed patient selection process is illustrated in Fig. 1.

Flowchart of patients.
Data classification and reclassification
Data were reclassified according to SEER guidelines. Age groups were defined based on BCY12, SIOG, EUSOMA13, and SEER standards: young (< 40 years), middle-aged (40–69 years), and elderly (≥ 70 years). Race categories were identified as "White," "Black," and “Other” (including Asian or Pacific Islander, American Indian/Alaska Native, and Unknown). Marital status was categorized as “Married” (including common law) and “Single” (including never married, divorced, widowed, unknown, and others). Tumor grades were divided into Grades I-II (well-differentiated) and Grades III-IV (poorly differentiated). Tumor staging included Stage IIA, IIB, IIIA and IIIB-IIIC;Tumor size was segmented into T1 (< 2 cm), T2 (≥ 2 cm and < 5 cm), and T3/T4;Lymph node status was simplified to N0, N1, N2, N3;Surgical procedures were classified as Breast-Conserving Surgery (BCS) and Mastectomy;Radiation treatments were classified as Radiation and No Radiation.
Patients categorized as "not given neoadjuvant chemotherapy" were considered part of the ACT group, as patients not receiving chemotherapy were excluded. Cases marked as "response but not specified as complete or partial" were reclassified as "partial response." Records categorized as “partial response” and “no response” were grouped as non-pCR. Patients identified as having a complete response were classified as having pCR, and together, pCR and non-pCR patients constitute the NACT group.This reclassification aligned with SEER surgical codes to minimize discrepancies and enhance analytical robustness and consistency.
Statistical analysis
All data were treated as categorical variables. Statistical analysis was performed using SPSS version 22.0. Categorical variables are presented as frequencies and percentages, with associations assessed via chi-square tests.PSM was applied to balance intergroup differences at a 1:1 ratio with a caliper width of 0.01.Kaplan–Meier curves were used to illustrate OS and BCSS, with group differences evaluated using log-rank tests. Cox univariate and multivariate analyses were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for OS and BCSS, with statistical significance set at p < 0.05.
Results
Characteristics of the original patients
From the SEER database, a cohort of 21,299 patients was identified, with 17.83% (3798/21,299) receiving NACT. Compared to the ACT group, the NACT group had a higher proportion of single patients (42.75% vs. 38.79%; P < 0.001), larger tumors (33.59% vs. 7.45% for tumors ≥ 5 cm; P < 0.001), and more advanced disease stage (43.87% vs. 22.77% for Stage III; P < 0.001). To address baseline disparities, 1:1 ratio PSM with a caliper width of 0.01 was applied to balance intergroup differences using covariates including age, race, marital status, grade, AJCC stage, tumor size (T), nodal status (N), surgery type, and radiation receipt. This resulted in well-balanced clinical and pathological characteristics between groups.
Survival analysis of the overall study subjects
Kaplan–Meier curves for study subjects
Before PSM, the mean follow-up time for the 21,299 patients was 126 months. There were 3795 total deaths, with 2749 being breast cancer-specific. The NACT group exhibited significantly poorer OS ( 5-year 82.5% vs. 91.8%; 10-year 69.0% vs. 81.6%, P < 0.001) and BCSS (84.8% vs. 93.9%; 10-year 74.5% vs. 87.0%, P < 0.001) compared to the ACT group. After PSM, the mean follow-up time for 6930 patients was 121 months. There were 1566 deaths, including 1242 breast cancer-specific deaths (79.31%). The NACT group still showed poorer OS (5-year 83.7% vs. 89.6%; 10-year 69.9% vs. 76.7%; P < 0.001) and BCSS (85.9% vs. 91.6%; 10-year 75.3% vs. 81.8%; P < 0.001) compared to the ACT group. (Fig. 2a-d).

Kaplan‒Meier survival curve of Stage II-III HR + /HER2- Breast Cancer:Adjuvant vs. Neoadjuvant Chemotherapy ; Notes:A Before PSM, overall survival; B After PSM, overall survival;C Before PSM, breast cancer-specific survival; D After PSM, breast cancer-specific survival.Abbreviations: NACT: Neoadjuvant Chemotherapy;ACT: Adjuvant Chemotherapy;PSM: Propensity Score Matching.
Cox regression analysis of breast cancer-specific survival and overall survival
In the univariate Cox regression analysis, we examined various clinical and demographic factors impacting OS, including age, race, marital status, tumor grade, clinical stage, tumor size, lymph node status, surgery type,radiation status, and chemotherapy type (Table 1). Patients who underwent NACT exhibited a significantly elevated risk of mortality in comparison to those who received ACT (HR 1.411, 95% CI 1.277–1.559, p < 0.001), To address potential confounding factors identified in the univariate analysis, we conducted a multivariate Cox regression analysis. After adjustment, NACT remained an independent risk factor for OS (HR 1.442, 95% CI 1.304–1.594, p < 0.001). (Table 2).
To further investigate the effects of NACT, we subdivided the NACT group into patients achieving pCR and non-pCR. We then conducted univariate and multivariate Cox proportional hazards analyses to evaluate OS(Table 3) and BCSS(Table 4).The overall pCR rate in the study population was 17.27% (656/3798).Our analysis indicated that patients who achieved pCR after NACT did not show significant survival benefits in terms of OS (P = 0.129) and BCSS (P = 0.435). However, compared to patients receiving adjuvant chemotherapy, the non-pCR group had significantly worse OS (HR 1.580, 95% CI 1.425–1.751, P < 0.001) and BCSS (HR 1.677, 95% CI 1.493–1.883, P < 0.001).
Additionally, higher tumor grade (Grade III and IV), larger tumor size (T3 and T4), and lymph node status (N2/N3) were identified as significant risk factors for both OS and BCSS. Interestingly, while univariate Cox analysis showed significant differences in OS and BCSS across different breast-conserving surgery, these differences were not observed in the multivariate analysis.
Stratified analysis by breast cancer stages
To further investigate the impact of NACT on overall OS and BCSS across different breast cancer stages, we performed a stratified analysis using this study data. Specifically, we examined the survival outcomes of patients with breast cancer stages IIA, IIB,IIIA and IIIB-IIC who received either NACT or ACT. PSM at a 1:1 ratio was employed to ensure comparability between groups. (see Supplementary Table 1.2.3.4).
We constructed Kaplan–Meier survival curves for OS and BCSS for patients in the NACT and ACT groups. After PSM, the analysis of patients with stage IIB, IIIA and IIIB-IIIC breast cancer revealed that both OS and BCSS were consistently lower in the NACT group compared to the ACT group.In patients with stage IIA breast cancer, BCSS were consistently lower in the NACT group compared to those in the ACT group. However, no statistically significant differences were observed in OS between the two groups (p = 0.109). (Fig. 3a-h)).

Kaplan–Meier Survival Curve Stratified by Breast Cancer Stages: Neoadjuvant Chemotherapy vs.Adjuvant Chemotherapy; Notes::3-a stage IIA overall survival;3-b stage IIB overall survival;3-c stage IIIA overall survival;3-d stage IIIB-IIIC breast cancer-specific survival;3-estage IIA breast cancer-specific survival;3-f stage IIB breast cancer-specific survival;3-g stage IIIA breast cancer-specific survival;3-h stage IIIB-IIIC breast cancer-specific survival; Abbreviations: NACT: Neoadjuvant Chemotherapy;ACT: Adjuvant Chemotherapy.
To mitigate potential biases due to tumor burden, particularly in patients with high tumor loads such as T3/T4 and N2/N3 classifications, we conducted a stratified analysis based on tumor size and lymph node staging (T1, T2, T3, T4/N0, N1, N2, N3). Additionally, propensity score matching (PSM) at a 1:1 ratio was employed to ensure comparability between the groups (see Supplementary Table 5.6.7,8,9,10,11,12).
Stratified analyses by primary tumor size (T stage) and nodal status (N stage) revealed consistent and significant survival disadvantages associated with NACT compared to ACT in most subgroups, as detailed in the accompanying forest plots (Fig. 4). For tumor size, patients with T1, T2, and T3 tumors experienced significantly worse OS and BCSS when treated with NACT versus ACT (T1: OS HR 1.945, 95% CI 1.606–2.355, p < 0.001; BCSS HR 2.257, 95% CI 1.798–2.833, p < 0.001; T2: OS HR 1.851, 95% CI 1.625–2.109, p < 0.001; BCSS HR 2.072, 95% CI 1.785–2.404, p < 0.001; T3: OS HR 2.034, 95% CI 1.462–2.829, p < 0.001; BCSS HR 2.162, 95% CI 1.498–3.118, p < 0.001). However, no significant differences in OS (HR 1.535, 95% CI 0.888–2.654, p = 0.125) or BCSS (HR 1.524, 95% CI 0.833–2.789, p = 0.172) were observed for patients with T4 tumors. Similarly, analyses by nodal status demonstrated significantly reduced OS and BCSS with NACT in patients categorized as N0 (OS HR 1.519, 95% CI 1.247–1.851, p < 0.001; BCSS HR 1.820, 95% CI 1.446–2.291, p < 0.001), N1 (OS HR 1.864, 95% CI 1.630–2.132, p < 0.001; BCSS HR 2.143, 95% CI 1.834–2.503, p < 0.001), and N2 (OS HR 2.176, 95% CI 1.666–2.841, p < 0.001; BCSS HR 2.426, 95% CI 1.779–3.310, p < 0.001). While N3 patients also showed significantly worse BCSS with NACT (HR 1.689, 95% CI 1.082–2.636, p = 0.021), the difference in OS for this subgroup did not reach conventional statistical significance (HR 1.431, 95% CI 0.968–2.116, p = 0.073). Importantly, all reported hazard ratios (HRs) were derived from multivariable Cox proportional hazards models applied to propensity score matched (PSM) cohorts. Collectively, these findings indicate a survival detriment associated with NACT compared to ACT, particularly evident in early-stage disease (T1-T3, N0-N2).

Forest Plot of NACT Effects on OS/BCSS by Tumor size and lymph node status (Cox Proportional Hazards Model). Notes:4-a Forest Plot of NACT Effects on OS/BCSS by Tumor size (Cox Proportional Hazards Model) ;4-b: Forest Plot of NACT Effects on OS/BCSS by lymph node status (Cox Proportional Hazards Model) Abbreviations: HR:Hazards Ratio;OS: Overall Survival;BCSS: Breast Cancer-Specific Survival.
Impact of Neoadjuvant Chemotherapy on Breast-Conserving Surgery
To further evaluate the impact of neoadjuvant chemotherapy (NACT) on survival outcomes following breast-conserving surgery (BCS), we conducted a statistical analysis of the study data. Initial analyses revealed an inadequate sample size of T4 patients undergoing BCS after NACT (n = 44), which resulted in an imbalance of covariates between subgroups. This imbalance subsequently affected the validity of propensity score matching (PSM) and the robustness of causal effect estimates.
To address this issue, we implemented several strategies to optimize cohort definition and variable stratification. Specifically, we combined stage III into a single analytical unit that includes IIIA, IIIB, and IIIC sub-stages to enhance the statistical power of this stratification. We further combined T3 tumors (≥ 5 cm) with T4 tumors into a single “T3/T4” group. Additionally, we merged N2 (4–9 positive lymph nodes) with N3 (≥ 10 positive lymph nodes or involvement of supraclavicular/internal mammary lymph nodes) into an “N + ” group. Finally, we conducted additional propensity score matching for patients across different stages (IIA, IIB, and III) (see Supplementary Tables 13, 14, and 15). Kaplan–Meier survival curves were then constructed to compare overall survival (OS) and breast cancer-specific survival (BCSS) among patients undergoing BCS who received either NACT or adjuvant chemotherapy (ACT). This comprehensive approach is intended to ensure a robust analysis of outcomes associated with NACT in the context of BCS.
After further PSM in patients undergoing breast-conserving surgery , Kaplan–Meier survival curves indicated that, in stage III patients, the OS and BCSS were significantly lower in the NACT group compared to the ACT group. In stage IIA/IIB patients, there were no significant differences in OS or BCSS between the NACT and ACT groups.[Fig. 5 (a,b,c,d,e,f)].

Kaplan–Meier Survival Curve Stratified by Breast Cancer Stages: Neoadjuvant Chemotherapy vs.Adjuvant Chemotherapy in Patients Undergoing Breast-Conserving Surgery; Notes::5-a stage IIA overall survival; 5-b stage IIB overall survival;5-c stage III overall survival;5-d stage IIA breast cancer-specific survival; 5-e stage IIB breast cancer-specific survival;5-f stage III breast cancer-specific survival. Abbreviations: NACT: Neoadjuvant Chemotherapy;ACT: Adjuvant Chemotherapy.
To minimize the potential impact of surgical procedures on our findings, we conducted a subgroup analysis stratified by treatment modalities and performed a propensity score-matched study based on surgical categories.(see Supplementary Table 16,17,18,19,20,21).After adjusting for surgical procedures, our analysis revealed that surgical procedures did not significantly impact OS and BCSS in patients with breast cancer, regardless of tumor stage or receipt of neoadjuvant or adjuvant chemotherapy.[Fig. 6 (a,b,c,d,e,f,g,h,i,j,k,l)].

Kaplan–Meier Survival Curves Comparing Breast-Conserving Surgery vs Mastectomy in Breast Cancer Patients Stratified by Breast Cancer Stage and Treated with Adjuvant or Neoadjuvant Chemotherapy. Notes: 6-a stage IIA overall survival in neoadjuvant chemotherapy; 6-b stage IIB overall survival in neoadjuvant chemotherapy; 6-c stage III overall survival in neoadjuvant chemotherapy; 6-d stage IIA breast cancer-specific survival in neoadjuvant chemotherapy; 6-e stage IIB breast cancer-specific survival in neoadjuvant chemotherapy; 6-f stage III breast cancer-specific survival in neoadjuvant chemotherapy; 6-g stage IIA overall survival in adjuvant chemotherapy; 6-h stage IIB overall survival in adjuvant chemotherapy; 6-i stage III overall survival in adjuvant chemotherapy; 6-j stage IIA breast cancer-specific survival in adjuvant chemotherapy; 6-k stage IIB breast cancer-specific survival in adjuvant chemotherapy ; 6-l stage III breast cancer-specific survival in adjuvant chemotherapy. Abbreviations: NACT: Neoadjuvant Chemotherapy;ACT: Adjuvant Chemotherapy.
Discussion
This study offers critical insights by leveraging the SEER database to compare survival outcomes in stage II-III HR + /HER2- breast cancer patients subjected to NACT versus ACT.To minimize selection bias 1:1 PSM was performed for all cohort data prior to statistical analysis. The results revealed that both OS and BCSS were significantly lower in the NACT group compared to the ACT group. Currently, there are no randomized phase III clinical trials to guide the choice between NACT and ACT for HR + /HER2- breast cancer patients; the main evidence comes from the NSABP B-18 trial, NSABP-B27which showed no significant differences in DFS and OS but did not stratify by molecular subtype14,15.In our further multivariate analysis, age ≥ 70 years, Black race, single, grade III/IV tumors, T3 + disease, and N2/N3 nodal involvement as independent risk factors for reduced OS and BCSS. Prompted by these risk profiles and the dual objectives of NACT, we conducted exploratory analyses to elucidate whether achieving NACT’s primary endpoints—tumor downstaging and breast-conserving surgery —mitigates potential survival disparities.
Different stages of breast cancer survival analysis
In our analysis, we observed significant variations in survival outcomes across different stages of breast cancer. For stage IIA patients, while the BCSS was lower than that of patients receiving ACT, there was no significant difference in OS rates. This discrepancy may reflect the inherently better prognosis of stage IIA breast cancer. Conversely, in patients with stage IIB,IIIA and IIIB-IIIC disease, we noted that those receiving NACT had significantly poorer OS and BCSS compared to their ACT counterparts.
To better investigate the role of anatomical staging in NACT, we further analyzed the survival outcomes of NACT compared to ACT by stratifying by T and N stages. Our study showed that NACT significantly reduced OS and BCSS in patients with T1-T3/N0-N2 breast cancer (HRs 1.52–2.43, p < 0.001), challenging traditional views on the survival benefits of NACT. The potential mechanisms behind this include: (1) selection bias (the NACT group may include tumors with more aggressive biological characteristics); (2) delays in local treatment promoting the occurrence of micrometastases; (3) impaired survival in non-pathological complete response (pCR) patients, particularly those with lower tumor burdens; and (4) chemotherapy-induced resistance and the creation of a pro-metastatic microenvironment.An exception was observed in T4 stage patients, where there were no significant differences in OS and BCSS (P > 0.1). In N3 stage patients, BCSS showed a statistically significant difference, while OS did not reach statistical significance, reflecting the value of NACT in local control for advanced disease.
Our findings suggest that for HR + /HER2- breast cancer patients with T1-3/N0-2 disease, neoadjuvant chemotherapy (NACT) should be cautiously selected. Notably, existing studies16 have similarly demonstrated that for patients with earlier anatomical stages of this subtype, the clinical utility of NACT should be rigorously assessed to avoid overtreatment and optimize survival benefits.Therefore, clinical decision-making regarding NACT for HR + /HER2- patients must comprehensively incorporate other high-risk biological indicators such as KI-67 index and multigene assay results.
Role of pathological complete response(pCR)
pCR is often used as a marker of sensitivity to NACT and has been shown to predict long-term outcomes in several neoadjuvant studies17,18. Therefore, it has been used as a surrogate marker for OS, accelerating the approval of certain drugs19. However, its application in HR + /HER2- breast cancer has been questioned. First, HR + /HER2- breast cancers have a lower pCR rate20, and the correlation between pCR and both DFS and OS is weaker compared to HER2-positive and triple-negative breast cancers11,21,22. In our study, the overall pCR rate in the NACT group was 17.27%, which is consistent with most studies. However, achieving pCR did not result in better OS and BCSS, and patients who did not achieve pCR had even poorer survival outcomes. This indicates that these patients may exhibit poor responsiveness to chemotherapy, potentially even inducing chemoresistance, ultimately delaying the timing of surgical intervention.
Breast-conserving surgery in neoadjuvant patients
One of the important goals of NACT is to increase the rate of breast-conserving surgery23,24. Some studies support that NACT can improve breast-conserving surgery rates9,25,26 .However, despite theoretically increasing the chance of breast-conserving surgery by downstaging tumors, these studies did not include long-term survival outcomes for HR + /HER2- population as an endpoint27.
Focusing on survival endpoints, this study found that among patients with stage III disease, OS and BCSS were lower in those receiving NACT compared to those receiving ACT. It is important to emphasize that in clinical practice, physicians tend to prefer NACT for patients with high tumor burden and clinically high-risk features (e.g., elevated multigene scores). This introduces the potential for significant and non-negligible selection bias in the stage III cohort, a bias that likely influences the interpretation of these results. For stage IIA-IIB patients, no statistically significant differences in OS or BCSS were observed between the NACT and ACT groups. Furthermore, consistent with prior studies14,28. our results indicate that the type of surgical intervention (BCS or mastectomy) did not significantly impact OS or BCSS, regardless of tumor stage. Collectively, these findings suggest that for HR + breast cancer patients with higher tumor burden and clinical features indicating elevated risk (particularly when presenting as stage III disease), caution is warranted when considering NACT primarily to increase the BCS rate. The decision requires comprehensive individualized assessment, carefully weighing its potential impact on survival.
Future research directions
Despite the relatively favorable prognosis of HR + /HER2- breast cancer, treatment options remain challenging due to the unique characteristics of this subtype24. Neoadjuvant treatment strategies have diversified, notably with the emergence of neoadjuvant endocrine therapy (NET)5, initially studied in elderly ER + patients unsuitable for chemotherapy or surgery29. Subsequent research has shown that aromatase inhibitors (AIs) are well-tolerated in postmenopausal patients and yield objective response rates and breast-conserving surgery rates comparable to chemotherapy, but with significantly lower toxicity30,31,32. Trials such as IMPACT33 have established AIs as the preferred NET option. For premenopausal patients, ovarian function suppression (OFS) combined with AIs has proven effective34. To optimize stratification strategies for HR + /HER2- breast cancer, genomic analyses are increasingly utilized to identify populations with low benefit from neoadjuvant chemotherapy35,36,37. Advances in genomic research have linked certain gene expressions to endocrine therapy resistance, leading to combinations of targeted agents with NET to overcome this resistance38,39. The SOLAR-1 trial40 has shown significant improvements in progression-free survival with Alpelisib and Fulvestrant in PIK3CA-mutated advanced cases. Furthermore, trials like NeoPalAna41 and PALLET42 have demonstrated that adding CDK4/6 inhibitors to NET enhances the suppression of malignant cell proliferation. However, whether these combinations translate into clinical benefits remains debated, highlighting the need for more large-scale clinical trials to optimize the management of HR + /HER2- breast cancer and confirm these findings.
Limitations of the study
The limitations of this study primarily stem from its retrospective design and reliance on the SEER database. Key clinical and molecular data (such as Ki-67 index, comprehensive genomic analyses, detailed endocrine therapy regimens, specific chemotherapy protocols, and sentinel lymph node biopsy status) are not available in the SEER database. These variables are crucial for assessing tumor biology, treatment efficacy, and heterogeneity within the HR + /HER2- subtype. For instance, the lack of Oncotype DX scores limited our ability to perform genetic risk stratification for patients, potentially masking the identification of subgroups that might benefit less from chemotherapy. Similarly, the absence of Ki-67 data hindered our evaluation of proliferation activity, which is closely related to chemotherapy sensitivity. Additionally, incomplete information regarding adherence to endocrine therapy may confound survival outcomes, as suboptimal treatment could independently lead to worse prognosis. While propensity score matching has balanced observed confounding factors, these unmeasured factors may partially explain the observed survival disadvantage in the NACT group. Future studies integrating multimodal data (genomic, treatment adherence monitoring, and dynamic tumor biomarker assessments) are essential to validate our findings and refine therapeutic decision-making for HR + /HER2- breast cancer."
Conclusion
This study demonstrates that patients with stage II-III HR + /HER2- breast cancer who receive NACT have significantly lower OS and BCSS compared to those receiving ACT, particularly in patients with T1-T3/N0-N2 disease. The survival disadvantage persists even after propensity score matching, and pCR does not improve prognosis. Patients undergoing breast-conserving surgery should also be cautious when selecting NACT (especially stage III patients) to avoid sacrificing survival benefits in pursuit of breast conservation as the primary goal. Future research should focus on optimizing management approaches for HR + /HER2- breast cancer, particularly in the context of emerging therapies such as NET, to improve patient overall survival and quality of life.
Data availability
The datasets analysed during the current study are available in the Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov). SEER*Stat Database: Incidence - SEER Research Data, 17 Registries, November 2023 Submission (2000-2021).
Abbreviations
- NACT:
-
Neoadjuvant chemotherapy
- ACT:
-
Adjuvant chemotherapy
- OS:
-
Overall survival
- BCSS:
-
Breast cancer-specific survival
- HR + /HER2-:
-
Hormone receptor-positive / human epidermal growth factor receptor 2-negative
- PSM:
-
Propensity score matching
- SEER:
-
Surveillance, epidemiology, and end results
- pCR:
-
Pathological complete response
- BSC:
-
Breast-conserving surgery
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- DFS:
-
Disease-free survival
- NSABP:
-
National surgical adjuvant breast and bowel project
- NET:
-
Neoadjuvant endocrine therapy
- AI:
-
Aromatase inhibitors
- ORR:
-
Objective response rate
- RS:
-
Recurrence score
References
Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA: A Cancer J. Clin. 74, 12–49 (2024).
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 Countries. CA Cancer J Clin 71, 209–249 (2021).
Kim, H. J. et al. Efficacy of neoadjuvant endocrine therapy compared with neoadjuvant chemotherapy in pre-menopausal patients with oestrogen receptor-positive and HER2-negative, lymph node-positive breast cancer. Breast Cancer Res. 22, 54 (2020).
Howlader, N. et al., US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst 106 (2014).
Tamirisa, N. & Hunt, K. K. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline. Ann. Surg. Oncol. 29, 1489–1492 (2022).
Schick, P., Goodstein, J., Moor, J., Butler, J. & Senter, K. L. Preoperative chemotherapy followed by mastectomy for locally advanced breast cancer. J. Surg. Oncol. 22, 278–282 (1983).
Fisher, B. et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J. Clin. Oncol. 41, 1795–1808 (2023).
Rastogi, P. et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J. Clin. Oncol. 26, 778–785 (2008).
Killelea, B. K. et al. Neoac for breast cancer increases the rate of breast conservation: Results from the National Cancer database. J. Am. Coll. Surgeons 220, 1063–1069 (2015).
Spring, L. M. et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: A comprehensive meta-analysis. Clin. Cancer Res. 26, 2838–2848 (2020).
von Minckwitz, G. et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 30, 1796–1804 (2012).
Paluch-Shimon, S. et al. ESO-ESMO fifth international consensus guidelines for breast cancer in young women (BCY5). Ann. Oncol. 33, 1097–1118 (2022).
Biganzoli, L. et al. Updated recommendations regarding the management of older patients with breast cancer: a joint paper from the European Society of Breast Cancer Specialists (EUSOMA) and the International Society of Geriatric Oncology (SIOG). Lancet Oncol. 22, e327–e340 (2021).
Bear, H. D. et al. The effect on tumor response of adding sequential preoperative docetaxel to preoperative doxorubicin and cyclophosphamide: preliminary results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 21, 4165–4174 (2003).
Fisher, B. et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-18. J. Clin. Oncol. 15, 2483–2493 (1997).
Zhao, M. et al. Comparing survival outcomes between neoadjuvant and adjuvant chemotherapy within hormone receptor-positive, human epidermal growth factor receptor 2-negative early breast cancer among young women (≤35): a retrospective cohort study based on SEER database and TJMUCH registry. Am. J. Cancer Res. 15, 390–405 (2025).
Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384, 164–172 (2014).
Nekljudova, V. et al. Trial-level prediction of long-term outcome based on pathologic complete response (pCR) after neoadjuvant chemotherapy for early-stage breast cancer (EBC). Contemp. Clin. Trials 71, 194–198 (2018).
Bardia, A. & Baselga, J. Neoadjuvant therapy as a platform for drug development and approval in breast cancer. Clin. Cancer Res. 19, 6360–6370 (2013).
Rouzier, R. et al. Breast cancer molecular subtypes respond differently to preoperative chemotherapy. Clin. Cancer Res. 11, 5678–5685 (2005).
Conforti, F. et al. Evaluation of pathological complete response as surrogate endpoint in neoadjuvant randomised clinical trials of early stage breast cancer: systematic review and meta-analysis. BMJ 375, e66381 (2021).
Cortazar, P. & Geyer, C. J. Pathological complete response in neoadjuvant treatment of breast cancer. Ann. Surg. Oncol. 22, 1441–1446 (2015).
Gradishar, W. J. et al. Breast Cancer, Version 3.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 22, 331–357 (2024).
Spring, L. M., Bar, Y. & Isakoff, S. J. The evolving role of neoadjuvant therapy for operable breast cancer. J Natl Compr Canc Netw 20, 723–734 (2022).
Barbieri, E. et al. Neo-adjuvant chemotherapy in luminal, node positive breast cancer: Characteristics, treatment and oncological outcomes: A single center’s experience. Eur J Breast Health 17, 356–362 (2021).
Fitzal, F. et al. Neoadjuvant chemotherapy increases the rate of breast conservation in lobular-type breast cancer patients. Ann. Surg. Oncol. 19, 519–526 (2012).
Trialists, E. B. C. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 19, 27–39 (2018).
Veronesi, U. et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl. J. Med. 347, 1227–1232 (2002).
Mustacchi, G. et al. Tamoxifen alone versus adjuvant tamoxifen for operable breast cancer of the elderly: long-term results of the phase III randomized controlled multicenter GRETA trial. Ann. Oncol. 14, 414–420 (2003).
Spring, L. M. et al. Neoadjuvant endocrine therapy for estrogen receptor-positive breast cancer: A systematic review and meta-analysis. JAMA Oncol. 2, 1477–1486 (2016).
Palmieri, C. et al. NEOCENT: a randomised feasibility and translational study comparing neoadjuvant endocrine therapy with chemotherapy in ER-rich postmenopausal primary breast cancer. Breast Cancer Res. Treat 148, 581–590 (2014).
Semiglazov, V. F. et al. Phase 2 randomized trial of primary endocrine therapy versus chemotherapy in postmenopausal patients with estrogen receptor-positive breast cancer. Cancer-Am. Cancer Soc. 110, 244–254 (2007).
Smith, I. E. et al. Neoadjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: the Immediate Preoperative Anastrozole, Tamoxifen, or Combined with Tamoxifen (IMPACT) multicenter double-blind randomized trial. J. Clin. Oncol. 23, 5108–5116 (2005).
Masuda, N. et al. Neoadjuvant anastrozole versus tamoxifen in patients receiving goserelin for premenopausal breast cancer (STAGE): a double-blind, randomised phase 3 trial. Lancet Oncol. 13, 345–352 (2012).
Morales, M. S. et al. Selection of neoadjuvant treatment based on the 21-GENE test results in luminal breast cancer. Breast 56, 35–41 (2021).
Pease, A. M., Riba, L. A., Gruner, R. A., Tung, N. M. & James, T. A. Oncotype DX(®) recurrence score as a predictor of response to neoadjuvant chemotherapy. Ann. Surg. Oncol. 26, 366–371 (2019).
Bear, H. D. et al. Using the 21-gene assay from core needle biopsies to choose neoadjuvant therapy for breast cancer: A multicenter trial. J. Surg. Oncol. 115, 917–923 (2017).
Shin, I., Miller, T. & Arteaga, C. L. ErbB receptor signaling and therapeutic resistance to aromatase inhibitors. Clin. Cancer Res. 12, 1008s–1012s (2006).
Schiff, R., Massarweh, S., Shou, J. & Osborne, C. K. Breast cancer endocrine resistance: how growth factor signaling and estrogen receptor coregulators modulate response. Clin. Cancer Res. 9, 447S-454S (2003).
André, F. et al. Alpelisib plus fulvestrant for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: final overall survival results from SOLAR-1. Ann. Oncol. 32, 208–217 (2021).
Ma, C. X. et al. NeoPalAna: Neoadjuvant Palbociclib, a cyclin-dependent kinase 4/6 inhibitor, and anastrozole for clinical stage 2 or 3 estrogen receptor-positive breast cancer. Clin. Cancer Res. 23, 4055–4065 (2017).
Johnston, S. et al. Randomized phase II study evaluating palbociclib in addition to letrozole as neoadjuvant therapy in estrogen receptor-positive early breast cancer: PALLET trial. J. Clin. Oncol. 37, 178–189 (2019).
Acknowledgements
We acknowledge the data support of the SEER program, as well as the Department of Breast Surgery, Guizhou Provincial People’s Hospital.
Funding
This work was supported by the National Natural Science Foundation of China (nos. 81802479, and 82360501).
Author information
Authors and Affiliations
Contributions
Jiaxing Liu and Likuan Tan contributed equally to this work. Jiaxing Liu wrote the manuscript. Likuan Tan collected the literature, created the figures. Yufei Liu and Guanghui Wang conceived the idea and was involved in manuscript conception and drafting. All authors read and approved the final manuscript and contributed to the article.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
We confirmed that the details of any images and recordings can be published.
Ethics approval and informed consent
The SEER database is publicly accessible and does not provide personal identifying information. Therefore, institutional review board approval and informed patient consent were not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, J., Tan, L., Zhang, H. et al. Long-term survival outcomes of neoadjuvant chemotherapy in stage II-III HR+/HER2- breast cancer. Sci Rep 15, 30201 (2025). https://doi.org/10.1038/s41598-025-14012-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-14012-0
