
Abstract
Pain-related discussions on social media provide valuable insights into how people naturally express and communicate their pain experiences. However, the network structure of these discussions remains poorly understood. This study analyzed 57,000 Reddit comments from the GoEmotions dataset (2005–2019) using natural language processing and network analysis techniques grounded in discrete mathematical principles. The constructed network, comprising 5,630 nodes and 86,972 edges, revealed complex patterns of pain-related language use. The network exhibited a sparse overall density (0.0055) but a high clustering coefficient (0.7700), indicating the presence of distinct thematic communities. At the center of the network was the term pain, which showed the highest degree centrality (0.821429), reflecting its semantic anchoring function in pain discourse. Other terms, such as headache, served as context-sensitive bridge nodes that connected different semantic subdomains. In contrast, terms like burning, despite moderate centrality values, were found to co-occur predominantly with metaphorical or decorative expressions rather than emotion- or symptom-related descriptors. Community detection revealed 12 distinct clusters, with the largest containing 1,021 nodes, capturing diverse aspects of pain communication. Stability analysis demonstrated that core pain-related terms maintained consistent centrality, while peripheral or metaphorical terms showed greater variability. These findings offer novel insights into the semantic structure of pain discourse and suggest that network analysis of social media discussions can inform improved clinical communication and symptom assessment.
Similar content being viewed by others


Introduction
Various methods have been used to study emotion. Research based primarily on data obtained from surveys and controlled experimental environments has been common, employing techniques where participants evaluate stimuli, such as photographs of facial expressions or music, to explore emotional dimensions and experiences1,2. However, these methods have limitations in terms of ecological validity, that is, the extent to which the findings reflect natural language use and emotional expression in real-life contexts. Studies based on natural text expressions found on social media or online forums, which are part of daily communication, remain limited3,4.
Unlike other emotions, pain is not only a biological or psychological phenomenon but also a communicative act deeply embedded in social and intersubjective contexts. The Social Communication Model of Pain posits that linguistic expression plays a critical role in shaping how pain is perceived, evaluated, and responded to by others5. Phenomenological approaches further emphasize that pain is lived and expressed within a “lifeworld,” where metaphor and imagination help constitute its meaning beyond numerical intensity6,7. These perspectives suggest that the study of pain-related language can illuminate the social construction of suffering and the dynamics of its recognition.
This study analyzed the network structure of discussions related to pain on online platforms using Natural Language Processing (NLP) techniques. Unlike other emotions, pain is a complex experience that encompasses both psychological and physiological effects, positioning it uniquely in emotional research8,9. The GoEmotions dataset enabled the construction of a pain-related terms network, with topological analysis revealing how pain discussions unfolded10. This approach offers a novel perspective for understanding the experience of pain through natural language expressions, independent of self-reports or survey-based methods11.
Results
Network structure and central nodes
This section provides a global overview of the pain-related lexical network, focusing on its structural scale, density, and community structure derived from 123,840 word co-occurrence relations. The resulting network comprises 5630 nodes and 86,972 edges, where each node represents a word and each edge denotes co-occurrence4,8,9. Terms such as burning, headache, discomfort, and ache exhibit prominent connectivity, suggesting frequent semantic associations.
Figure 1 illustrates a core–periphery structure: larger central nodes reflect higher centrality and discourse influence, while peripheral nodes reveal the stratified nature of pain-related language11,12.

Network visualization of pain-related terms. Co-occurrence network of 5,630 unique terms and 86,972 edges. Nodes represent individual terms; edges represent co-occurrence within a five-word sliding window. Node size scaled by centrality values. All nodes displayed in uniform color.
Although sparse in overall density (0.005500), the network displays high local connectivity. The average degree is 30.900000, indicating that each term connects to roughly 31 others13. The network diameter is 5, suggesting even distant terms are linked via short paths, supporting efficient semantic flow14.
The clustering coefficient of 0.770000 confirms that words form tightly connected local subgroups15. Louvain community detection identified 12 distinct communities16, with the largest including 1,021 nodes and others containing 911, 842, 520, and 495. These findings indicate a globally cohesive structure with semantically distinct subgroups reflecting thematic and contextual variation.
Structural roles of pain-related terms
This section focuses on identifying the lexical roles and relative centrality of individual symptom-related terms within the network. Figure 2 shows centrality metrics for key pain-related terms and their co-occurrence patterns. The analysis revealed a structured subgraph of 309 nodes and 363 edges11,12, capturing the complexity of symptom language on social media, including both frequent and unique word pairings.

Centrality measures for key pain-related terms in the network. Red nodes: primary pain-related keywords (pain, headache, burning, discomfort, ache). Blue nodes: secondary terms connected via co-occurrence. Node size proportional to degree centrality. Edge length inversely related to co-occurrence strength; shorter edges represent stronger associations.
The term pain consistently scored highest across all three centrality metrics—degree (0.821429), betweenness (0.930134), and eigenvector centrality (0.695893)—indicating its dominant role in organizing and connecting discourse elements across the lexical network13,15,17. In contrast, terms such as headache (0.107000, 0.109000, 0.055000), burning (0.182000, 0.166000, 0.110000), and discomfort (0.049000, 0.052000, 0.024000) displayed substantially lower scores, pointing to a pronounced structural hierarchy.
Notably, contextual analysis using the GoEmotions corpus showed that burning co-occurred almost exclusively with metaphorical or aesthetic descriptors (e.g., glass, carving), rather than with emotion- or symptom-oriented terms, suggesting a more figurative usage pattern.
Beyond individual terms, we examined centrality patterns across broader categories of pain—neuropathic, somatic, visceral, and psychosomatic—using a lexicon-based classification. Of the 21 predefined terms, only 6 (28.6%) were found in the co-occurrence network. Among them, psychosomatic terms such as depression and anxiety exhibited the highest eigenvector centralities (≈ 0.710000), indicating central placement in semantically influential regions. In contrast, clinically salient neuropathic terms like burning and shooting had lower connectivity and minimal network influence (e.g., burning ≈ 0.000000000000013). Somatic and visceral descriptors were largely absent, with only pressure marginally represented.
These findings reveal an asymmetry in how different pain modalities are linguistically expressed: while affective and cognitive terms dominate the discourse structure, physiologically grounded vocabulary remains peripheral or omitted. Full metrics by category are provided in Supplementary Table S1.
Statistical profiling of centrality in the pain network
This section presents a statistical characterization of centrality patterns among symptom-related terms, with the aim of evaluating structural hierarchy and connectivity within the lexical network. The pain-focused network exhibits a sparse but semantically ordered structure, with a density of 0.005500. The average degree is 30.900000, indicating that each node is connected to approximately 31 other terms on average. The network diameter is 5, meaning that even the most distant nodes are linked via relatively short paths, enabling efficient semantic propagation13,14.
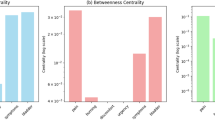
Centrality analysis identified pain as a pronounced hub node, with markedly higher values than all other terms in degree centrality (0.821429), betweenness centrality (0.930134), and eigenvector centrality (0.695893)13,15,17. These values indicate an integrative function across the network. Figure 3 presents a logarithmic histogram of these three centrality measures, highlighting the dominant position of pain in contrast to terms such as headache (0.107000, 0.109000, 0.055000), burning (0.182000, 0.166000, 0.110000), and discomfort (0.049000, 0.052000, 0.024000); ache also displayed similarly low scores (not shown in the figure).

Logarithmic histogram of centrality measures for key pain-related terms. (a) Degree centrality. (b) Betweenness centrality. (c) Eigenvector centrality. Terms: pain, headache, burning, discomfort, ache. X-axis: node labels. Y-axis: centrality values (log scale). Each bar represents a node.
Figure 3a shows degree centrality, which reflects the number of direct lexical connections maintained by a node. Pain exhibits the highest value, indicating its role in anchoring extensive semantic associations within the network. In contrast, headache and burning maintain fewer but still moderate links, while discomfort and ache are sparsely connected, reflecting their marginal connectivity.
Figure 3b highlights betweenness centrality, which measures how often a node lies on the shortest paths between other nodes—indicating its function as a bridge across semantic subgroups. Here again, pain dominates, suggesting that it facilitates cross-cluster discourse integration. Burning and headache display lower but nontrivial betweenness values, implying partial bridging roles. Meanwhile, discomfort and ache are nearly absent from these connective pathways, underscoring their peripheral status.
Figure 3c quantifies eigenvector centrality, which evaluates a node’s influence based on its proximity to other highly connected terms. The figure shows that pain holds a privileged position within the semantic core, exerting influence through its connections with other central terms. Burning ranks second in this metric, although it remains substantially lower than pain. In contrast, headache, discomfort, and ache display lower and more stable eigenvector centrality scores, indicating that they are situated in more context-specific and structurally marginal positions.
Together, these visualizations reinforce a clear structural hierarchy: while pain anchors the network’s core, other symptom terms form secondary or peripheral nodes, playing more specialized roles within constrained lexical contexts.
Each centrality metric offers a unique interpretive lens: degree centrality reflects the number of direct connections, betweenness centrality captures the term’s bridging role between semantic clusters, and eigenvector centrality quantifies influence within densely connected regions. These distinctions illuminate the functional heterogeneity of symptom vocabulary. While pain anchors the structure by linking diverse terms and domains, other expressions such as headache and burning occupy more context-dependent and localized roles.
Community structure in pain discourse
This section presents an analysis of how symptom-related terms cluster into semantically coherent communities, building on the centrality results described above. Based on Louvain modularity analysis, we examine whether structurally prominent terms like pain anchor broader thematic clusters, and how other expressions organize into distinct experiential or symbolic subdomains.
As shown in Fig. 4, the network is divided into multiple color-coded communities. The largest, labeled Community 2, contains 225 nodes and functions as a central hub of general pain discourse. Its average degree centrality is 0.007100, betweenness centrality is 0.004500, and eigenvector centrality is 0.046400. These values suggest that this community not only exhibits dense internal connectivity but also acts as a semantic bridge across other subgroups. With an average edge weight of 5.906200, terms in this cluster tend to co-occur frequently, reinforcing their mutual contextual associations.

Detected Communities in the Pain-Related Network Using the Louvain Method. Community structure of the pain-related lexical network, based on Louvain modularity detection. Each color denotes a distinct community. Community 0 (light blue): cluster around headache, including both literal symptom terms (e.g., sinus, minor) and metaphorical expressions (e.g., border, legacy). Community 1(Red): centered on discomfort, including relational and evaluative terms (e.g., who, would, deserved). Community 2 (yellow): largest cluster (225 nodes), centered on the term pain, representing general pain discourse. Community 3 (purple): cluster anchored by burning, combining somatic (e.g., legs, bloated) and symbolic terms (e.g., regret, church). Node size corresponds to degree centrality. Edge length inversely proportional to co-occurrence frequency.
The presence of additional, smaller communities reflects the thematic diversification of pain-related expressions. For example, Community 0, with 44 nodes and an average degree centrality of 0.008900, likely represents a moderately connected but distinct conceptual subgroup. Community 3, consisting of 14 nodes, stands out for its relatively high betweenness centrality of 0.009000, implying a mediating role despite its small size.
Close examination of the semantic profiles of specific communities reveals how pain-related terms are framed across experiential, emotional, and symbolic dimensions. One community, colored red and centered around the term discomfort, includes primarily relational and evaluative expressions such as who, would, and deserved. This linguistic configuration suggests that discomfort is often articulated in interpersonal or normative contexts, rather than through direct sensory description. Another cluster, shown in light blue and structured around headache, contains both symptomatic terms like sinus and minor, and systemic or metaphorical ones like border, legacy, and outsource. This distribution highlights the dual semantic role of headache, functioning both as a literal symptom and as a metaphor for social or cognitive burdens.
A third notable cluster, represented in purple and organized around burning, integrates terms with somatic references—such as bloated, legs, and skinny—alongside words associated with emotion, society, or spirituality, including regret, church, and world. This blend illustrates the polysemous character of burning, which serves as both a physiological descriptor and a symbolic or emotional expression in discourse.
Taken together, these findings indicate that social media users construct pain not only as a physical sensation but also as an emotionally charged and morally situated experience. The network structure shows that linguistic representations of pain diverge across bodily, emotional, and social registers, yet often reconnect through central terms that bridge these domains. This pattern of differentiation and reintegration underscores the complexity of symptom discourse in online contexts.
Structural centrality of pain compared to emotion-related terms
This section presents a comparative analysis between pain and emotion-related terms, building on the preceding findings that established pain’s structural dominance and thematic centrality in the symptom discourse network. To determine whether this prominence reflects general emotional salience or a unique structural role, we examine centrality metrics of pain relative to two core emotion terms: fear and nervousness.
Table 1 summarizes the results of this comparison. Across all three centrality metrics—degree, betweenness, and eigenvector centrality—pain exhibited markedly higher values. For example, its degree centrality (0.821429) was more than six times greater than the highest value in the fear group (0.0937), and substantially higher than the top score in the nervousness group (0.1297). A similar pattern was observed in betweenness centrality (0.930134 for pain versus ≤ 0.2025) and eigenvector centrality (0.695893 for pain versus ≤ 0.3426).
Permutation tests (n = 10,000) confirmed that pain’s centrality scores were significantly greater than those observed in either emotion-related group (p < 0.0001 for all metrics). These results indicate that pain functions not merely as a frequent or emotionally salient term, but rather as a structurally dominant hub within the symptom discourse network. Its high connectivity and bridging role distinguish it from typical emotion terms, which tend to cluster within narrower affective contexts. This supports the interpretation of pain as a central organizing term that integrates diverse semantic domains.
Stability analysis of centrality measures
This section presents an evaluation of the stability of key symptom-related terms using centrality metrics and their standard deviations, building on the previous structural analysis. Figure 5 provides a comparative visualization of centrality values and their variability for five key terms—pain, headache, burning, discomfort, and ache—across three centrality measures. Each panel in the figure corresponds to a specific metric: Fig. 5a shows degree centrality, Fig. 5b shows betweenness centrality, and Fig. 5c displays eigenvector centrality. Points represent mean centrality scores, while vertical error bars indicate standard deviations calculated from bootstrap resampling.

Instability of centrality measures for key pain-related terms. Centrality values and standard deviations for five pain-related terms (pain, headache, burning, discomfort, ache). (a) Degree centrality. (b) Betweenness centrality. (c) Eigenvector centrality. X-axis: node labels. Y-axis: centrality values. Error bars: standard deviations.
In Fig. 5a, pain shows the highest degree centrality with a moderate standard deviation, indicating that it consistently forms a dense set of direct lexical connections across samples. Burning and headache follow with lower scores and slightly higher variability. Discomfort and ache show both low centrality and limited variation, suggesting marginal connectivity and functional specificity in the network.
Figure 5b highlights pain’s role as a semantic bridge, with a betweenness centrality of 0.930134 and substantial variability, reflecting its dynamic positioning across contextual subgroups. Headache displays a standard deviation of 0.161610—greater than other non-central nodes—indicating its context-dependent bridging function. In contrast, discomfort and ache appear rarely along shortest paths between clusters, affirming their peripheral discursive role.
Figure 5c quantifies influence within densely connected regions. Pain again dominates, with burning positioned second in influence but showing a greater variance. Headache, discomfort, and ache all exhibit lower and more stable eigenvector centralities, reinforcing their limited integration into the semantic core of the network.
To further assess the robustness of these findings, 95% confidence intervals (CIs) for degree centrality were calculated using bootstrap standard deviations. Pain had the widest CI (0.193–1.450), underscoring both its dominant and context-sensitive role. Headache showed a CI of 0.020–0.195, while burning ranged from 0.034 to 0.329. Both discomfort and ache maintained lower and narrower ranges, each under 0.090, suggesting stable but structurally marginal positions.
To determine whether centrality variability differs by semantic category, we compared the standard deviations of degree centrality across three lexical groups: pain-related, metaphorical, and emotional terms. Statistical tests revealed that pain-related terms exhibited significantly higher variability than metaphorical terms (Welch’s t = 4.11, p = 0.0052; permutation p = 0.0034), whereas no significant difference was observed between pain-related and emotional terms (p > 0.77). These results suggest that variability is not randomly distributed but reflects functional distinctions within the discourse structure.
Taken together, the centrality stability profiles clarify the structural resilience and contextual adaptability of symptom-related terms. Pain consistently occupies a central yet flexible role, while headache and burning function within narrower, more variable contexts. In contrast, discomfort and ache remain stable but peripheral, contributing minimally to the broader organization of symptom-related language. These findings highlight the importance of incorporating stability metrics into network-based discourse analysis.
Discussion
This study reveals a pronounced structural hierarchy in pain-related discourse, with pain functioning as a semantic anchor that organizes symptom expressions across diverse communicative contexts3,5,18. This centrality extends beyond frequency, reflecting pain's role as a linguistic attractor that binds disparate sensory, emotional, and cognitive descriptors into coherent symptom narratives3,10. The network’s sparse overall density (0.0055) is counterbalanced by a high clustering coefficient (0.7700), indicating tightly knit local groupings. Moreover, the network exhibits a short diameter of 5—that is, even the most distant terms are connected by five or fewer co-occurrence steps—demonstrating efficient semantic linkage across the lexical structure19,20.
Within this framework, pain consistently dominates all centrality measures, while terms like headache, burning, and discomfort occupy more peripheral or context-specific positions21,22. This asymmetric configuration suggests that symptom discourse is not evenly distributed but shaped by key organizing principles20. The observed hierarchy also reflects the phenomenological reality that pain serves as both a descriptive label and an interpretive framework through which bodily experiences are conceptualized5. Unlike other sensory or emotional terms that cluster within narrower affective subdomains, pain demonstrates remarkable semantic breadth, linking physiological states to psychological and social meanings3,5,10.
This structural organization holds critical implications for how individuals conceptualize and communicate suffering, positioning pain not merely as a symptom descriptor but as a foundational organizing concept in health-related language3,5,10.
While centrality metrics provide valuable insight into lexical prominence, they alone cannot capture the full functional complexity of symptom-related vocabulary21,22. The term burning, for instance, displays moderate centrality in the network, yet closer examination reveals a disconnect between its structural presence and its clinical function23,24. Co-occurrence analysis within the GoEmotions corpus shows that burning frequently appears in metaphorical or decorative contexts—such as burning glass or burning wood—rather than in pain-related or emotional narratives23,24,25.
In contrast to its clinical role as a hallmark descriptor for neuropathic pain, burning in digital discourse fails to maintain semantic proximity to other pain terms, highlighting a fundamental divergence between medical language and everyday usage26,27. Similarly, headache exhibits high variability across centrality metrics, suggesting that its discursive role shifts depending on context—sometimes used literally, other times metaphorically or emotionally27,28. This functional plasticity implies that such terms operate as context-sensitive bridges within the discourse, adapting their meaning based on narrative framing29,30.
These observations underscore the need for contextual validation in network-based health communication studies24,29. Metrics alone cannot account for the pragmatic dimensions of lexical meaning. Instead, terms must be evaluated within the discursive ecosystems they inhabit, where semantic roles are negotiated dynamically rather than statically defined30,31.
The pragmatic divergence observed above, particularly in the case of burning, exposes deeper structural issues in the clinical use of diagnostic vocabulary31,32. In the context of interstitial cystitis/bladder pain syndrome, burning sensation is a central diagnostic criterion embedded in standardized questionnaires33,34,35. Yet our analysis shows that burning is rarely used in pain-related contexts on social media platforms. This suggests that younger, digitally native populations may not associate their lived sensory experiences with the terminology employed in formal diagnostic instruments—raising the risk of underreporting, misrecognition, or diagnostic delay31,36.
This gap is not isolated. In cardiovascular medicine, chest discomfort is widely used to characterize myocardial infarction, yet the term discomfort in online discourse frequently appears in psychological or environmental frames rather than somatic symptom contexts37,38. Similarly, tingling—a key term in describing neuropathic symptoms such as diabetic neuropathy or postherpetic neuralgia—is often employed in metaphorical expressions to denote emotional states39,40.
These patterns reflect a broader generational and linguistic shift that challenges the assumptions embedded in patient-reported outcomes and symptom checklists41,42. As clinical vocabularies fail to align with the language patients use organically, the risk of miscommunication increases43,44. Bridging this semantic gap will require systematic updates to diagnostic tools, guided by empirical discourse analysis, to ensure that clinical instruments remain intelligible, resonant, and effective in contemporary health communication45,46.
The variability observed in centrality measures should not be dismissed as methodological noise but rather interpreted as a structural indicator of functional diversity within symptom discourse47. This variability reflects the adaptive capacity of lexical items to operate across multiple narrative contexts, revealing fundamental differences in how terms function within the semantic ecosystem48,49. Terms with high centrality coupled with moderate instability, such as pain, demonstrate remarkable functional plasticity—maintaining structural dominance while adapting to diverse communicative situations3. This flexibility enables pain to serve as a versatile organizing principle across physiological, emotional, and social registers, explaining both its consistent prominence and contextual adaptability5,6.
In contrast, terms like discomfort and ache exhibit low centrality with minimal variability, suggesting constrained semantic functions and stable but peripheral roles. Their consistent positioning reflects specialized usage patterns that resist contextual adaptation, indicating narrow functional niches within pain discourse13,21. The statistical comparison across semantic categories further illuminates this pattern: pain-related terms showed significantly higher variability than metaphorical expressions (Welch’s t = 4.11, p = 0.0052), while showing no significant difference from emotional terms, suggesting that core symptom descriptors share the contextual flexibility characteristic of affective language50.
These findings reveal a fundamental principle of lexical organization in health discourse: the coexistence of “fluid centers” and "fixed peripheries." While central terms like pain maintain their structural importance through adaptive flexibility, peripheral terms preserve their positions through functional specificity17,20. This hierarchical arrangement reflects how symptom vocabulary balances semantic stability with communicative versatility, enabling both precise description and flexible meaning negotiation51.
Understanding the structural hierarchy and functional variability of symptom vocabulary offers significant implications for clinical communication and practice. Building on the structural insights outlined above, pain can be strategically leveraged as a central lexical anchor in diagnostic contexts, providing clinicians with a valuable entry point for eliciting more comprehensive symptom narratives5,7. The identification of stable peripheral terms versus variable bridging concepts provides a framework for interpreting patient language patterns, potentially improving triage efficiency and educational interventions by focusing on the lexical nodes through which patients naturally structure their experiences29,46.
The divergence between clinical terminology and everyday language usage, particularly evident in terms like burning, suggests the need for bridging models that can translate between professional medical discourse and patient-generated descriptions. Such translation frameworks could enhance patient-provider communication by recognizing how symptom descriptors function differently across contexts, enabling more accurate interpretation of patient reports and more effective health education strategies31,36.
However, several limitations constrain the immediate clinical applicability of these findings. In particular, social media users represent a self-selected and demographically skewed population—typically younger, digitally fluent, and culturally specific—limiting the generalizability of these findings to more diverse clinical populations. The reliance on social media data may not fully capture the linguistic patterns present in direct clinical encounters, and the temporal stability of these network structures requires validation across different time periods and demographic populations9,24. Moreover, while our quantitative network analysis provides structural insights into pain-related discourse, it should be interpreted alongside qualitative and ethnographic approaches that capture the lived experiences, cultural narratives, and interpersonal dynamics that shape how pain is communicated and understood52,53. Future research should integrate electronic medical records with patient-reported outcome measures to validate the clinical relevance of social media-derived language patterns11,12. Although our analyses confirmed the robustness of key network properties, we acknowledge that formal comparisons with graph-randomized or degree-preserving null models were not performed. Incorporating such null model frameworks would allow more rigorous inference of structural significance for metrics like clustering and modularity, and represents an important direction for future methodological work.
From a methodological perspective, this discrete mathematical approach to symptom language analysis provides a quantitative foundation for advancing personalized patient communication strategies in clinical practice54,55. The development of hybrid analytical frameworks that bridge social media linguistics with clinical communication represents a promising direction56. Such approaches could potentially transform network-derived centrality metrics into predictive indicators for patient communication preferences, symptom progression patterns, and treatment adherence, ultimately advancing personalized approaches to clinical dialogue and care delivery.
Methods
Ethics statement
This study analyzed publicly available data from the GoEmotions dataset, which contained anonymized Reddit comments. According to the platform’s terms of service, Reddit users consent to their public posts being viewed and analyzed. No additional ethical approval was required as this study used only publicly available, anonymized data and did not involve any direct human participant interaction. All data handling complied with Reddit’s terms of service and data-usage policies.
Data collection and preprocessing
An analysis was conducted on 57,000 Reddit comments from the GoEmotions dataset (2005–2019), which provides emotion-labeled social media texts4,8,9. Given the growing body of evidence suggesting that emotionally annotated language corpora can validly reflect underlying psychological constructs—including affective states, somatic perception, and interoceptive awareness3,5,18,37, this dataset offers a suitable foundation for analyzing spontaneously expressed pain-related discourse. Recent studies further support the use of word embeddings and emotion-tagged corpora to infer nuanced emotional and bodily experiences from naturalistic text3,57. The dataset was pre-processed using a multistage approach. Initial cleaning involved the removal of toxic or offensive content through a combination of automated filtering (using predefined word lists) and manual annotation. To ensure the reliability of toxicity identification, a random subset of comments was independently reviewed by two annotators, yielding substantial inter-rater agreement (Cohen’s κ = 0.85). In addition, only comments originating from subreddits with more than 10,000 posts were included to ensure data quality and adequate contextual richness.
Text preprocessing was performed using a custom-built NLP pipeline in Python 3.8. This included tokenization via the Penn Treebank tokenizer from the NLTK toolkit, followed by stop word removal and the elimination of special characters25,27. To improve terminological consistency, medical terms were standardized using a modified version of the Unified Medical Language System (UMLS) metathesaurus31,36. The accuracy of this standardization process was verified through manual inspection of a randomly sampled subset of 1,000 comments, achieving approximately 95% concordance between the output and clinical reference forms.
Pain-related comment identification and validation
To isolate pain-related discourse from the GoEmotions dataset, we applied a keyword-based filtering strategy. The pain-related keyword list was developed iteratively by two practicing physicians through interactive sessions with a large language model ChatGPT (OpenAI, San Francisco, CA, USA), with the goal of maximizing clinical relevance and semantic coverage. The final list was reviewed and refined under the supervision of an English language specialist (K.O.) to ensure terminological precision and consistency with biomedical discourse norms.
The resulting lexicon included over 90 pain-related terms encompassing urogenital, musculoskeletal, neuropathic, inflammatory, and psychosomatic categories. These terms were matched using case-insensitive substring search following tokenization. The full list used for filtering comprises:
genital pain, urinary pain, sexual dysfunction, dyspareunia, pain during sexual intercourse, pelvic pain, vaginal pain, erectile pain, testicular pain, bladder pain, reproductive organ pain, prostate pain, menstrual pain, intercourse pain, painful urination, genital discomfort, sexual pain, abdominal pain, headache, migraine, back pain, neck pain, shoulder pain, joint pain, muscle pain, chronic pain, acute pain, leg pain, foot pain, hand pain, stomach ache, toothache, sinus pain, chest pain, rib pain, arthritis pain, cramping, burning, throbbing, ache, soreness, discomfort, numbness, stiffness, tenderness, inflammation, spasm, nerve pain, perineal pain, bowel symptoms, urinary symptoms, bladder distension, dysuria, suprapubic pain, urethral burning, hesitancy, incontinence, frequency, urgency, sleep disturbance, fatigue, insomnia, depression, anxiety, hopelessness, sadness, loneliness, guilt, stress, apathy, worthlessness, isolation, lethargy, mood swings, irritability, withdrawal, appetite loss, emptiness, despair, suicidal thoughts, restlessness, helplessness, disability, posture issues, mobility limitations, lifestyle impact, backache, sciatica, bleeding, bloating, malnutrition, dehydration, anemia, weight loss, fever, bloody stools, diarrhea, mucus, complications, steroid therapy, immunosuppression, strictures.
Although the GoEmotions dataset was originally designed for emotion classification, its inclusion of naturalistic, emotionally annotated text makes it well-suited for identifying spontaneously expressed pain-related content in everyday language.
To assess the reliability of the filtering process, a random sample of 1,000 extracted comments was independently reviewed by N.O. and M.O. The two annotators demonstrated a high level of agreement in identifying pain-related content, confirming the consistency and thematic relevance of the filtered corpus.
Keyword identification and network analysis
Co-occurrence was defined using a five-word sliding window, in which any two terms appearing within the same five-word span were considered co-occurring. This method captures short-range contextual associations while maintaining semantic proximity and has been widely used in lexical network studies. This allowed lexical associations and patterns to emerge naturally from within the filtered subset. By analyzing co-occurrences among 123,840 potential word relationships, central terms such as pain, headache, discomfort, and burning surfaced as prominent nodes within the network.
This data-driven approach enabled the identification of emergent linguistic structures and thematic clusters without relying on externally imposed categories, offering an unbiased view of how pain is framed and communicated in social media.
Network analysis was implemented using NetworkX 2.5, employing a sliding window approach of size 5 (optimized through a sensitivity analysis of sizes 3–7). Co-occurrence weights were calculated using frequency-adjusted normalization to account for baseline term prevalence, with statistical significance assessed using Bonferroni-corrected Spearman’s correlation coefficients (p < 0.05).
Advanced statistical analysis
Network analysis employed three centrality measures to characterize the term relationships: degree centrality to measure term connectivity, betweenness centrality to identify bridge terms between symptom clusters, and eigenvector centrality to assess node influence within the network. The community structure was detected using the Louvain method with a resolution parameter of 1.0, optimized through modularity maximization (Q > 0.3)30,31. These metrics provide complementary perspectives on the network structure of pain-related studies.
Validation and quality control
Network stability was validated using both internal and external approaches. Internal validation employed bootstrap analysis (1000 iterations) with 80/20 data splits, maintaining edge weight distribution stability (coefficient of variation < 15%) and cross-validation with fivefold partitioning stratified by year32. For external validation, network findings were cross-referenced with established clinical literature through a systematic review of pain comorbidity studies (2000–2023)33.
Visualization and data representation
Network visualization was implemented using a modified force-directed layout algorithm in Python, with node sizes scaled logarithmically by term frequency. Edge weights were represented by a continuous color gradient from light grey (weak correlation) to black (strong correlation, r ≥ 0.7)34. Term categories were distinguished by color: pain terms in red, associated symptoms in blue, and psychological terms in green, with node opacity reflecting term specificity scores. All visualizations were optimized for colorblind accessibility according to established guidelines. No comparisons with graph-randomized or null networks were performed in this study; however, network stability was assessed through bootstrap, perturbation, and permutation-based validation strategies.
Quality assurance and reproducibility
Text processing quality was verified through a manual review of a stratified random sample (10% of the corpus) by two independent reviewers, achieving high inter-rater reliability (Cohen’s κ = 0.88 for term classification)35. Network stability was further evaluated through perturbation analysis, where up to 20% of the edges were randomly removed to assess changes in the community structure31,36.
Comparative centrality analysis and permutation testing
To evaluate the statistical significance and variability of key node centrality, we focused on the term pain and its comparison with emotion-related terms such as fear and nervousness. Separate co-occurrence networks were constructed for each emotional category using identical preprocessing and windowing parameters. Centrality measures (degree, betweenness, and eigenvector) were extracted from each network.
For each metric, we computed the maximum and mean values for the emotion-related networks and compared them with those of pain. To assess statistical significance, permutation tests (n = 10,000) were conducted using the combined centrality distribution from emotion-related terms as the null distribution. Pain exhibited significantly higher centrality in all metrics (p < 0.0001).
In addition, to estimate the variability of pain and other key nodes (e.g., headache, burning), we performed a bootstrap analysis (1,000 iterations). In each iteration, 80% of the corpus was resampled with replacement, and degree centrality was recalculated using the same network parameters. The resulting 95% confidence intervals (mean ± 1.96 × SD) provided estimates of centrality stability across corpus subsets. This analysis complements the network-wide validation and clarifies how robustly specific terms maintain their structural prominence.
Statistical analysis
Network characteristics were analyzed using the centrality analysis framework implemented in Network X 2.5. This included the extraction and normalization of 11 key pain descriptors, which were analyzed for co-occurrence patterns using a five-word window. The analysis revealed 363 significant relationships among 309 unique terms, with co-occurrence strength normalized by the total term frequencies to prevent bias in high-frequency terms.
Network analysis employed three centrality measures (degree, betweenness, and eigenvector centrality) to identify the key hub terms and bridge concepts. Community detection was performed using the Louvain method (resolution parameter: 1.0), with significance established through bootstrap analysis (1000 iterations) and Bonferroni correction. The final integration stage included the cross-validation of centrality measures and sensitivity analyses for parameter stability. The results were visualized using matplotlib and seaborn libraries, with node sizes reflecting centrality values, and edge weights representing co-occurrence strength.
Data availability
Publicly available datasets were analyzed in this study. This data can be found at: https://github.com/hplisiecki/emotion_topology."
Code availability
The code used in this study is available at: https://github.com/Okuinobuo/PainAnalysisNLP/
References
Bradley, M. M. & Lang, P. J. Affective norms for English words (ANEW): instruction manual and affective ratings. Technical report C-2. Univ. Florida, Gainesville (2010).
Ekman, P., Davidson, R. J. & Friesen, W. V. The Duchenne smile: Emotional expression and brain physiology. II. J. Pers. Soc. Psychol. 58, 342–353 (1990).
Jackson, J. C. et al. From text to thought: How analyzing language can advance psychological science. Perspect. Psychol. Sci. 17, 805–826 (2022).
Saffar, A. H., Mann, T. K. & Ofoghi, B. Textual emotion detection in health: Advances and applications. J. Biomed. Inform. 137, 104258 (2023).
Craig, K. D. Toward the social communication model of pain. In Social and Interpersonal Dynamics in Pain (eds Vervoort, T. et al.) 23–41 (Springer, 2018).
Geniusas, S. The Phenomenology of Pain (Ohio University Press, 2020).
Miglio, N. & Stanier, J. Beyond pain scales: A critical phenomenology of the expression of pain. Front. Pain Res. 3, 895443 (2022).
Barrett, L. F., Quigley, K. S. & Hamilton, P. An active inference theory of allostasis and interoception in depression. Philos. Trans. R. Soc. B Biol. Sci. 371, 20160011 (2016).
Kabir, M. K., Islam, M., Kabir, A. N. B., Haque, A. & Rhaman, M. K. Detection of depression severity using Bengali social media posts on mental health: Study using natural language processing techniques. JMIR Form Res. 6, e36118 (2022).
Demszky, D., Movshovitz-Attias, D., Ko, J., Cowen, A., Nemade, G. & Ravi, S. GoEmotions: a dataset of fine-grained emotions. Preprint at https://arxiv.org/abs/2005.00547 (2020).
Heintzelman, N. H. et al. Longitudinal analysis of pain in patients with metastatic prostate cancer using natural language processing of medical record text. J. Am. Med. Inform. Assoc. 20, 898–905 (2013).
Bacco, L. et al. Natural language processing in low back pain and spine diseases: A systematic review. Front. Surg. 9, 957085 (2022).
Cardoso, F. M. et al. Effect of network topology and node centrality on trading. Sci. Rep. 10, 11113 (2020).
Liu, M., Zou, X., Chen, J. & Ma, S. Comparative analysis of social support in online health communities using a word co-occurrence network analysis approach. Entropy 24, 174 (2022).
Newman, M. E. J. Networks: An Introduction (Oxford University Press, 2010). https://doi.org/10.1093/acprof:oso/9780199206650.001.0001.
Blondel, V. D., Guillaume, J. L., Lambiotte, R. & Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. 2008, P10008 (2008).
Cavallaro, L., De Meo, P., Fiumara, G. & Liotta, A. On the sensitivity of centrality metrics. PLoS ONE 19, e0299255 (2024).
Bunzli, S. et al. How do people communicate about knee osteoarthritis? A discourse analysis. Pain Med. 22, 1127–1148 (2021).
Fernández-de-las-Peñas, C. et al. Understanding sensitization, cognitive and neuropathic associated mechanisms behind post-COVID pain: A network analysis. Diagnostics 12, 1538 (2022).
Barabási, A.-L. Network Science (Cambridge University Press, 2016).
Oldham, S. et al. Consistency and differences between centrality measures across distinct classes of networks. PLoS ONE 14, e0220061 (2019).
Yadav, A. A comparative analysis of centrality measures in complex networks. Autom. Remote Control 85, 685–695 (2024).
Li, Z. et al. Temporal grading index of functional network topology predicts pain perception of patients with chronic back pain. Front. Neurol. 13, 899254 (2022).
Wu, S. et al. Deep learning in clinical natural language processing: A methodical review. J. Am. Med. Inform. Assoc. 27, 457–470 (2020).
Denecke, K. & Reichenpfader, D. Sentiment analysis of clinical narratives: A scoping review. J. Biomed. Inform. 140, 104336 (2023).
Bouhassira, D. et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 114, 29–36 (2005).
Zhang, Y., Zhang, Y., Qi, P., Manning, C. D. & Langlotz, C. P. Biomedical and clinical English model packages for the Stanza Python NLP library. J. Am. Med. Inform. Assoc. 28, 1892–1899 (2021).
Cheung, T. et al. Network analysis of depressive symptoms in Hong Kong residents during the COVID-19 pandemic. Transl. Psychiatry. 11, 460 (2021).
Jones, P. J., Ma, R. & McNally, R. Bridge centrality: A network approach to understanding comorbidity. Multivar. Behav. Res. 56, 353–367 (2019).
Zamani Esfahlani, F. et al. Modularity maximization as a flexible and generic framework for brain network exploratory analysis. Neuroimage 244, 118607 (2021).
Xu, D. et al. Unified Medical Language System resources improve sieve-based generation and Bidirectional Encoder Representations from Transformers (BERT)-based ranking for concept normalization. J. Am. Med. Inform. Assoc. 27, 1510–1519 (2020).
Neal, Z. P. How strong is strong? The challenge of interpreting network edge weights. PLoS ONE 19, e0311614 (2024).
Doiron, R. C., Nickel, J. C. & Siemens, D. R. Diagnosis and management of interstitial cystitis/bladder pain syndrome: CUA guideline. Can. Urol. Assoc. J. 19, 92–102 (2025).
Yu, W.-R., Jiang, Y.-H., Jhang, J.-F. & Kuo, H.-C. Bladder pain syndrome associated with interstitial cystitis: Recent research and treatment options. Curr. Bladder Dysfunct. Rep. 18, 389–400 (2023).
Clemens, J. Q., Erickson, D. R. & Varela, N. P. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J. Urol. 208, 34–42 (2022).
Zheng, L. et al. A review of auditing techniques for the Unified Medical Language System. J. Am. Med. Inform. Assoc. 27, 1625–1638 (2020).
Altstidl, J. et al. Absence of chest discomfort in type 1 NSTEMI patients: Predictors and impact on outcome. Clin. Res. Cardiol. 114, 1234–1245 (2025).
Kumar, A. et al. Chest pain symptoms during myocardial infarction in patients with and without diabetes: A systematic review and meta-analysis. Heart 109, 1516–1524 (2023).
Baba, M., Kuroha, M., Wasaki, Y. & Ohwada, S. Effects of mirogabalin on tingling or pins & needles in a phase 3 study of diabetic peripheral neuropathy. J. Jpn. Soc. Pain Clin. 27, 287–295 (2020).
Wu, S., Wahle, J. P. & Mohammad, S. The Language of Interoception: Examining Embodiment and Emotion Through a Corpus of Body Part Mentions. arXiv:2505.16189 (2025).
Borbjerg, M. K. et al. Understanding the impact of diabetic peripheral neuropathy and neuropathic pain on quality of life and mental health in 6,960 people with diabetes. Diabetes Care 48, 588–595 (2025).
Tofthagen, C., Visovsky, C., Dominic, S. & McMillan, S. Neuropathic symptoms, physical and emotional well-being, and quality of life at the end of life. Support. Care Cancer 27, 3357–3364 (2019).
Hu, Y., Keloth, V. K., Raja, K., Chen, Y. & Xu, H. Towards precise PICO extraction from abstracts of randomized controlled trials using a section-specific learning approach. Bioinformatics 39, btad542 (2023).
Engels, G. et al. Clinical pain and functional network topology in Parkinson’s disease: A resting-state fMRI study. J. Neural Transm. 125, 1449–1459 (2018).
Brusco, M. J., Steinley, D. & Watts, A. L. On maximization of the modularity index in network psychometrics. Behav. Res. Methods. 55, 3549–3565 (2023).
Hoffman, M., Steinley, D., Gates, K. M., Prinstein, M. J. & Brusco, M. J. Detecting clusters/communities in social networks. Multivar. Behav. Res. 53, 57–73 (2018).
Filosi, M., Visintainer, R., Riccadonna, S., Jurman, G. & Furlanello, C. Stability indicators in network reconstruction. PLoS ONE 9, e89815 (2014).
Mokhtari, F., Akhlaghi, M. I., Simpson, S. L., Wu, G. & Laurienti, P. J. Sliding window correlation analysis: Modulating window shape for dynamic brain connectivity in resting state. Neuroimage 189, 655–666 (2019).
Shakil, S., Lee, C. H. & Keilholz, S. D. Evaluation of sliding window correlation performance for characterizing dynamic functional connectivity and brain states. Neuroimage 133, 111–128 (2016).
Daly, C. H. et al. Empirical evaluation of SUCRA-based treatment ranks in network meta-analysis: Quantifying robustness using Cohen’s kappa. BMJ Open 9, e024625 (2019).
Wongpakaran, N., Wongpakaran, T., Wedding, D. & Gwet, K. L. A comparison of Cohen’s Kappa and Gwet’s AC1 when calculating inter-rater reliability coefficients: A study conducted with personality disorder samples. BMC Med. Res. Methodol. 13, 61 (2013).
Kleinman, A. The Illness Narratives: Suffering, Healing, and the Human Condition. (Basic Books, 1988).
Good, B. J. Medicine, Rationality, and Experience: An Anthropological Perspective (Cambridge University Press, 1994).
Okui, N. Laser treatment for urinary incontinence in elite female athletes analyzed using a discrete mathematics approach. Sci. Rep. 15, 15450 (2025).
Okui, N. Innovative decision making tools using discrete mathematics for stress urinary incontinence treatment. Sci. Rep. 14, 9900 (2024).
Turner, R. J., Hagoort, K., Meijer, R. J., Coenen, F. & Scheepers, F. E. Bayesian network analysis of antidepressant treatment trajectories. Sci. Rep. 13, 8428 (2023).
Plisiecki, H. & Sobieszek, A. Emotion topology: extracting fundamental components of emotions from text using word embeddings. Front. Psychol. 15, 1401084 (2024).
Acknowledgements
We thank Karen Okui for English language editing and proofreading of the manuscript. We are also grateful to Dr. Machiko Okui for her support in the identification and refinement of pain-related lexical terms. This paper is dedicated to the memory of my late high school friend, mathematician Yasushi Kondoh. Our shared passion for mathematics during those formative years has remained a lasting source of inspiration, ultimately leading to the writing of this work more than four decades later.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
N.O. and S.H. contributed equally to all aspects of this research including: conceptualization, data curation, formal analysis, investigation, writing the manuscript, reviewing and editing. Both authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Generative AI and AI-assisted technologies in the writing process
We used Python libraries with machine learning capabilities for statistical analysis and network visualization. However, no generative AI or AI-assisted technologies were used in the writing or editing of the manuscript text.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Okui, N., Horie, S. Natural language processing reveals network structure of pain communication in social media using discrete mathematical analysis. Sci Rep 15, 29219 (2025). https://doi.org/10.1038/s41598-025-14680-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-14680-y
