
Abstract
Spinal nerve sheath tumors are slow-growing neoplasms that arise from Schwann cell lineage and encompass schwannomas, neurofibromas, hybrid nerve sheath tumors, and malignant peripheral nerve sheath tumors. These lesions most commonly present as intradural extramedullary (IDEM) tumors, although extradural and dumbbell-shaped variants are also observed. Due to their typically benign behavior, gross total resection (GTR) remains the standard of care. However, there is a paucity of literature comparing the impact of open versus minimally invasive surgery (MIS) on postoperative extended length of stay (LOS). Prolonged hospitalization can increase healthcare costs, patient morbidity, and resource utilization. This study aims to compare the impact of MIS and open surgical approaches on extended LOS in patients undergoing resection of spinal nerve sheath tumors. Patients diagnosed with spinal nerve sheath tumors between 2004 and 2017 were identified from the National Cancer Database (NCDB) using ICD-O code 8680, 9560, 9490, 9540, and 9561. The cohort was stratified into four racial groups: White, Black, Hispanic, and Asian. Univariate analyses were performed to compare demographic, disease characteristics, and clinical outcomes. Additionally, a multivariate linear regression model was constructed to identify factors associated with extended length of stay, adjusting for sex, race, surgical modality (MIS, open, robotics), use of robotic surgery, facility type, insurance status, distance from facility to patient, comorbidities, age category, tumor behavior, and tumor size. Extended length of stay was defined as hospitalization exceeding the 75th percentile of the entire study population’s length of stay. A total of 5,968 patients with spinal nerve sheath tumors were identified: 202 (3.4%) underwent MIS and 5,766 (96.6%) underwent open surgery. After 1:1 propensity score matching, 404 patients were equally distributed between the two groups. Prior to matching, MIS was more frequently used in the South Atlantic and East North Central regions compared to open surgery (29.3% vs. 21.4%; 20.1% vs. 16.1%; p = 0.008). Postoperative LOS was significantly shorter in the MIS group both before (4.4 ± 3.1 vs. 5.3 ± 3.5 days; p < 0.001) and after matching (4.4 ± 3.0 vs. 5.4 ± 3.5 days; p < 0.001). Patients treated with MIS were also less likely to experience an extended LOS both before (21.5% vs. 32.1%; p = 0.002) and after matching (21.5% vs. 35.4%; p = 0.002). On multivariable analysis, geriatric age (OR: 1.28; 95% CI: 1.12–1.46; p < 0.001), comorbidity burden (1 comorbidity: OR: 1.47; 95% CI: 1.25–1.72; ≥2: OR: 2.15; 95% CI: 1.72–2.68; p < 0.001), larger tumor size (OR: 1.02; 95% CI: 1.01–1.02; p < 0.001), and invasive behavior (OR: 1.41; 95% CI: 1.10–1.80; p = 0.007) were associated with increased odds of extended LOS. Male sex (OR: 0.83; 95% CI: 0.74–0.93; p = 0.001) and MIS approach (OR: 0.55; 95% CI: 0.36–0.80; p = 0.003) were associated with reduced odds. Robotic assistance did not significantly impact extended LOS (OR: 1.38; 95% CI: 0.61–3.01; p = 0.429). Gradient Boosting had the highest predictive performance among machine learning models (AUC: 0.594), followed by AdaBoost and logistic regression. SHAP analysis identified surgical approach, comorbidity score, tumor size, and behavior as the most influential features on extended LOS. MIS was associated with significantly lower odds of extended length of stay compared to open surgery for spinal nerve sheath tumor resection. Robotic assistance did not confer a significant additional benefit. These findings suggest that MIS may improve postoperative recovery and resource utilization in appropriately selected patients. Further prospective studies are needed to validate these results and clarify the role of MIS and robotic approaches in spinal tumor surgery.
Similar content being viewed by others
Introduction
Spinal nerve sheath tumors are neoplasms thought to originate from Schwann progenitor cells consisting of schwannomas, neurofibroma, hybrid nerve sheath tumor, paraganglioma, malignant melanotic schwannoma and malignant peripheral nerve sheath tumors and represent approximately one fourth of all primary spinal tumors1,2. Typically presenting as intradural extramedullary (IDEM) lesions, they also demonstrate extradural or dumbbell-shaped extensions2,3,4. Although their indolent growth is often associated with low tumor-associated mortality, symptomatic lesions can cause significant morbidity through local mass effect, nerve root compression, and spinal cord displacement, manifesting as radiculopathy, myelopathy, motor weakness, sensory deficits, or urinary dysfunction5,6.
Gross total resection (GTR) with neurological preservation remains the standard of care, offering excellent long-term outcomes and low recurrence rates2,7,8. However, aggressive resection carries a nontrivial risk of postoperative neurological deficits due to proximity to critical structures such as the vertebral artery and adhesive attachment to the spinal cord. In recent years, minimally invasive spine (MIS) surgery has emerged as a promising alternative, aiming to reduce iatrogenic injury, minimize perioperative complications, and accelerate postoperative recovery9. For spinal nerve sheath tumors, treatment paradigms should prioritize functional preservation and quality of life relative to the degree of interaction of the surrounding critical structures. Extended hospital length of stay (LOS) following surgery not only increases the risk of hospital-acquired complications (HACs) but also drives up healthcare costs and patient burden10,11. While MIS techniques have demonstrated shorter LOS and expedited return to function in degenerative spinal and oncological spinal procedures, their specific impact on LOS following spinal nerve sheath tumor resection remains poorly characterized12,13,14,15.
In our study, we evaluate the association between surgical approach (MIS vs. open) and postoperative LOS among patients undergoing resection of spinal nerve sheath tumors, using the National Cancer Database (NCDB). We hypothesize that MIS resection is associated with significantly shorter LOS compared to open surgery in patients treated for spinal nerve sheath tumors. Furthermore, we seek to identify additional predictors of extended LOS, including demographic factors, comorbidity burden, tumor characteristics, and the role of robotic-assisted techniques, with the aim of informing surgical decision-making and optimizing resource utilization in the management of spinal nerve sheath tumors.
Methods
Cohort selection
The National Cancer Database (NCDB) is one of the largest cancer registries in the United States and contains almost 34 million cases from over 1500 hospitals. The data is collected from selected health registries accredited by the American College of Surgeons’ Commission on Cancer (Commission on Cancer | ACS). The NCDB sponsored by the American College of Surgeons (ACS) and the American Cancer Society (ACS) gathers data from qualified facilities across the United States, which enables robust multi-center retrospective research.
For this study, the NCDB was queried for patients diagnosed and treated for spinal nerve sheath tumors between January 1, 2004, and December 31, 2017. Cases were identified using the ICD-O-3 histology code 8680, 9560, 9490, 9540, and 9561. Patients were categorized based on surgical approach variable as either minimally invasive surgery (MIS) or open surgery. The study was conducted in compliance with the Health Insurance Portability and Accountability Act (HIPAA) and adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. Institutional Review Board (IRB) review determined the study to be exempt from full review, and informed consent was waived due to the use of de-identified data.
Patient demographics and disease and treatment characteristics
Our study included patient demographics such as age at diagnosis, sex (male and female), race (classified as White, Black, Hispanic, and Asian), and insurance status (Private, Medicaid, Medicare, Other Government, and Not Insured). Location was stratified into urban, metro and rural based on degree of urbanization, adjacency to metro areas and population size recommended by the United States Department of Agriculture Economic Research Service16. Median income (High Income, Higher-Middle Income, Lower-Middle Income, Low Income) and no high school diploma (Highly Educated, Moderately Educated, Minimally Educated, Poorly Educated) quartiles were noted. The CROWFLY distance was calculated based on the zip codes of patients and facilities. The Charlson-Deyo Comorbidity Classification (CDCC) score was calculated for each patient using the CDCC Mapping Table, categorized as 0, 1, or 2 +17. Facility type and facility locations were identified. Behavior was categorized into invasive and non-invasive and tumor size was measured in millimeters (mm) and defined as the diameter of the tumor. All cases of spinal nerve sheath tumors were identified. Patients were then categorized according to treatment modality: MIS and open surgical resection.
Primary and secondary outcome variables
The primary outcomes of interest was extended LOS (binary classification), defined as the values greater than the 75th percentile of the distribution for the overall cohort. Secondary outcomes included days from diagnosis to surgical start. Baseline patient characteristics, including demographics, comorbidities, and tumor details, were analyzed to evaluate factors influencing these outcomes.
Statistical analysis
We performed univariate comparisons between open and MIS groups. Categorical variables were presented as frequencies and percentages and analyzed using Chi-square tests or Fisher’s exact tests, while continuous variables were summarized by mean and standard deviation and analyzed using independent samples t-tests for parametric data or Mann-Whitney U tests for nonparametric data. Formal tests of normality were not performed due to the large sample size and heterogeneous nature of the NCDB dataset. Instead, we applied non-parametric methods and modeling approaches that do not assume normality, including categorical thresholds for extended LOS and tree-based machine learning algorithms. We performed univariate comparisons between the MIS and open approaches. Categorical variables were presented as frequencies and percentages and analyzed using while continuous variables were summarized by mean and standard deviation and analyzed using independent samples t-tests for parametric data or Mann-Whitney U tests for nonparametric data. K-Nearest Neighbor (KNN) propensity score matching was performed at a 1:1 ratio between surgery types based on CCDC score, sex and age for descriptive comparisons between surgical approach groups, but not for multivariable regression or machine learning models, in order to preserve sample size and allow for flexible modeling of covariate effects. To explore the association between patient variables and the outcomes of interest, a multivariable logistic regression model was constructed to identify independent predictors of extended LOS, including sex, age category, tumor size, CDCC score, tumor behavior, application of robotics, and surgical approach (MIS vs. open). All variables were entered simultaneously into the model. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to quantify the independent associations of these variables with early outcomes. Forest plots were generated to visualize the ORs and highlight significant associations (p < 0.05). All statistical analyses were conducted using R Studio and Python, adhering to STROBE reporting guidelines for observational studies. The model included age category (Adult vs. Geriatric), sex, race, robotic approach (Robotics vs. No Robotic MIS), surgical approach (open vs. MIS), comorbidity score, tumor size and behavior as variables, with hazard ratios (HRs), 95% confidence intervals (CIs), and p-values reported for each.
Machine learning models were employed to predict the extended length of stay (LOS). The dataset was split into training and testing sets at an 80/20 ratio. To address class imbalance of the outcome variable, we applied the Synthetic Minority Over-sampling Technique (SMOTE) to the training set to generate synthetic samples for the minority class by creating new instances between existing data points. SMOTE was applied exclusively within the full unmatched cohort, was not used to balance treatment groups (MIS vs. open), and no synthetic data were included in testing or evaluation. After data preprocessing, we implemented eight primary machine-learning-based that were employed to predict the extended LOS: the Random Survival Forest model, Logistic Regression model, Extra Trees model, KNN model, Naive Bayes model, Decision Tree model, AdaBoost model and Gradient Boosting Survival model. Stratified 5-fold cross-validation was applied within the training set to maintain balanced outcome distribution. Model performance was assessed using Receiver Operating Characteristic (ROC) curves, with the Area Under the Curve (AUC) calculated to measure predictive accuracy. The 95% Confidence Intervals (CIs) were calculated using repeated 10-fold cross-validation. One-way analysis of variance (ANOVA) was conducted across AUC distributions to statistically compare model performance, and a Post hoc Tukey’s Honest Significant Difference (HSD) testing was then used to identify significant pairwise differences in performance between individual models. SHapley Additive exPlanations (SHAP) were applied to the best-performing model, as determined by the highest AUC, to interpret the influence of each feature on predictions of extended LOS. Variables that encompass patients’ baseline health status, socioeconomic access, tumor biology, and system-level variables all of which could potentially influence LOS were incorporated into the ML analyses, including age, sex, race, CDCC scores, tumor behavior, tumor size, surgical approach, robotic application and radiation therapy use. The machine learning analysis was conducted as an exploratory adjunct to conventional regression, designed to assess variable importance and non-linear relationships influencing extended LOS. These models were not intended to serve as clinical prediction tools but rather to complement traditional analysis and generate hypotheses for future research.
Results
Patient demographics and disease characteristics
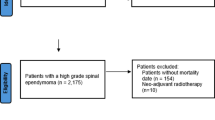
A total of 5968 patients with spinal nerve sheath tumors were included in the study, with 5,766 (96.6%) undergoing open surgery and 202 (3.4%) undergoing MIS surgery (Fig. 1). After 1:1 KNN matching, the final cohort consisted of 404 patients, equally distributed between the open and MIS groups (Table 1).
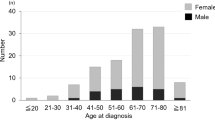
The open surgery group had a lower mean age than the MIS group before matching, though this difference was not statistically significant. After matching, the mean age continued to be well distributed between the two treatment groups. Sex distribution was similar between groups without a significant difference, with male patients being slightly more predominant (53.2% vs. 52.0%). White patients were the most prevalent racial group before matching (84.3%), followed by Black (8.0%), Asian (6.0%), and Hispanic (1.7%). However, after matching, racial distribution remained similar across groups without significant difference. The distance from home to the surgical facility was comparable both before and after matching between the MIS and open groups (108.9 ± 72.8 vs. 111.8 ± 73.8 miles, p = 0.717). Insurance status was similar between groups before and after matching. Private insurance was the most common (61.0%), followed by Medicare (24.2%) and Medicaid (9.1%). Education level, residential location and median income quartiles were similarly distributed between groups before and after matching. Facility location differed significantly before matching (p = 0.008), with MIS procedures more frequently performed in the South Atlantic (District of Columbia, Delaware, Florida, Georgia, Maryland, North Carolina, South Carolina, Virginia, West Virginia) (29.3%) and East North Central (Illinois, Indiana, Michigan, Ohio, Wisconsin) (20.1%) regions, while open surgery was more evenly distributed. After matching, regional differences were no longer significant. Facility type was comparable between groups before and after matching. The majority of patients underwent treatment at academic/research centers (52.3%) or comprehensive community cancer programs (31.0%). This distribution remained unchanged after matching. CDCC scores were well balanced between groups before and after matching. Before matching, tumor size was not significantly different. After matching, tumor sizes trended towards being larger in the MIS group (21.6 ± 12.4 mm vs. 18.3 ± 10.6 mm, p = 0.059), approaching statistical significance. Tumor behavior was primarily non-invasive in both groups before and after matching and remained non-significant. Overall, following propensity score matching, there were no significant differences between MIS and open cohorts in demographic or clinical characteristics, including age, sex, race, insurance status, distance to facility, facility type, facility location, residential location, income quartile, education level, CDCC score, tumor behavior, or tumor size (all p > 0.05), indicating successful covariate balance.
Among patients treated with a minimally invasive surgical approach, we compared those who underwent robotic-assisted MIS versus those who underwent non-robotic MIS (Supplementary Table 1). The mean age was similar between groups (54.4 ± 17.7 years for robotic vs. 54.9 ± 5.9 years for non-robotic MIS, p = 0.860). Both sex and racial distribution were comparable without statistical significance.
Interestingly, patients in the robotic group lived significantly closer to their treatment facility compared to the non-robotic group (173.5 ± 190 miles vs. 286.9 ± 299.3 miles, p = 0.027). Insurance status did not differ significantly between groups, with private insurance being the most common type (48.8% robotic vs. 63.2% non-robotic). Education level and income quartile were similarly distributed across groups (p = 0.093 and p = 0.971, respectively). Residential location did not significantly differ, with the majority of patients in both groups residing in metropolitan areas (93.0% robotic vs. 84.7% non-robotic).
Facility location and type demonstrated variation. Patients undergoing robotic MIS were more likely to be treated at comprehensive community cancer programs (62.5%) compared to the non-robotic group (25.0%), whereas non-robotic MIS was more common in academic/research centers (59.1% vs. 25.0%, p < 0.001). Facility location trended toward significance (p = 0.078), with robotic cases more frequently performed in the Pacific and South Atlantic regions.
Charlson-Deyo comorbidity scores and tumor characteristics including size and behavior were similar between groups. Most patients had a CDCC score of 0 (86.0% robotic vs. 81.1% non-robotic), and tumors were largely non-invasive (95.3% vs. 94.3%). Mean tumor size was slightly larger in the robotic group (33.5 ± 23 mm vs. 27.9 ± 17.9 mm), though this difference did not reach statistical significance.
Clinical outcomes
Significant differences in postoperative clinical outcomes were observed between the open and MIS groups before and after matching (Table 2). The mean number of days from diagnosis to surgery was comparable between groups before matching and remained similar after matching. Postoperative LOS was significantly shorter in the MIS group before matching (4.4 ± 3.1 days vs. 5.3 ± 3.5 days, p < 0.001). After matching, the MIS group continued to demonstrate a significantly shorter LOS (4.4 ± 3.0 days vs. 5.4 ± 3.5 days, p < 0.001). Patients who experienced an extended hospital stay were more prevalent in the open surgery group both before and after matching relative to normal stays. Before matching, 32.1% of open surgery patients had an extended stay compared to 21.5% of MIS patients (p = 0.002). After matching, the proportion of extended stays remained significantly higher in the open group compared to normal stays (35.4% vs. 21.5%, p = 0.002).
The clinical outcomes were similarly compared between the robotic and non-robotics MIS cohorts (Supplementary Table 2). No significant differences were observed in time from diagnosis to surgical start (22.4 ± 8.3 vs. 30.4 ± 49.3 days, p = 0.337), postoperative LOS (4.2 ± 2.8 vs. 4.5 ± 3.2 days, p = 0.646), or the proportion of patients experiencing extended length of stay (26.8% vs. 20.1%, p = 0.354).
Risk factors for extended length of stay
The multivariate logistic regression analysis showed several significant factors influencing risk of extended length of stay in patients undergoing surgical resection of spinal nerve sheath tumors. Male patients had significantly lower odds of an extended length of stay compared to female patients (OR = 0.83, 95% CI: 0.74–0.93, p = 0.001). Age also played a significant role, with geriatric patients exhibiting higher odds of an extended hospital stay compared to adult patients (OR = 1.28, 95% CI: 1.12–1.46, p < 0.001) (Fig. 2).
Tumor size was positively correlated with an increased likelihood of extended hospitalization, with each unit increase in size slightly raising the odds (OR = 1.02, 95% CI: 1.01–1.02, p < 0.001). The CDCC score was a strong predictor, with patients having a score of 1 showing increased odds of extended hospitalization (OR = 1.47, 95% CI: 1.25–1.72, p < 0.001) compared to those with a CDCC score of 0, while those with a CDCC score of 2 or more had even higher odds (OR = 2.15, 95% CI: 1.72–2.68, p < 0.001).
Tumor behavior also influenced hospital stay, as patients with non-invasive tumors had significantly lower odds of an extended length of stay compared to those with invasive tumors (OR = 0.71, 95% CI: 0.56–0.91, p = 0.007). Surgical approach was another key determinant, with patients undergoing minimally invasive surgery having significantly lower odds of prolonged hospitalization compared to those who underwent open surgery (OR = 1.83, 95% CI: 1.24–2.78, p = 0.003). However, the use of robotic-assisted techniques did not significantly affect the odds of an extended length of stay compared to non-robotic-assisted MIS techniques (OR = 1.38, 95% CI: 0.61–3.01, p = 0.429).
Machine-learning-based models
All machine learning models demonstrated modest predictive performance, with AUCs ranging from 0.594 to 0.71, which exceed random chance. The Receiver Operating Characteristic (ROC) curves for different machine learning models show that the Gradient Boosting model achieved the highest performance (AUC: 0.594, 95% CIs: 0.584–0.604), indicating higher accuracy in distinguishing between extended LOS outcomes compared to other models. This is followed closely by the Ada Boost model (AUC: 0.592, 95% CIs: 0.582–0.602), and the Logistic Regression (AUC: 0.590, 95% CIs: 0.576–0.604). A one-way ANOVA confirmed significant differences across model AUCs (F = 946.95, p < 0.001). Subsequent Tukey HSD testing showed that the Gradient Boosting model significantly outperformed Extra Trees, KNN, Decision Tree, and Random Forest models. These results support the superior performance of Gradient Boosting for predicting extended length of stay (Fig. 3A and B).
The SHAP analysis from the Random Survival Forest model identified several key factors associated with risk of extended length of stay in patients undergoing spinal tumor resections (Fig. 3C and D). MIS without robotic assistance significantly elevated extended LOS risk. The surgical approach (MIS vs. open), tumor size, sex, CDCC score, and behavior of the tumor were all linked to a significantly lower risk of extended LOS. The impact of sex and race was not distinct per the visualization of the SHAP analysis. Patients with female sex, younger age, and lower tumor burden are associated with reduced risk of extended length of stay, as evidenced by negative SHAP values. Patients with fewer comorbidities and less aggressive tumor behavior similarly demonstrated improved outcomes for extended length of stay (Fig. 3C). The feature importance analysis further supports these findings, with the surgical approach contributing the highest importance to the model’s predictions, followed by MIS with robotics, sex, and tumor size (Fig. 3D).
Discussion
There is limited literature available on the optimal surgical modality (open versus minimally invasive) for the treatment of spinal nerve sheath tumors. We thus used a large-population national database to explore the impact of surgical approach on postoperative outcomes, with a particular focus on LOS. One important note is that fewer than 5% of patients in our cohort underwent the MIS approach for spinal nerve sheath tumor resection, likely reflecting appropriate selection criteria. As such, MIS may be best reserved for specific cases that are not intradural, not within the spinal canal, and not closely associated with critical neurovascular structures. Yet further institutional examination is necessary to further expand on such findings. Our study demonstrated that patients undergoing open surgery experienced a longer LOS than patients undergoing MIS, a finding that was preserved after using propensity score matching to balance the demographic characteristics of both treatment groups. Open surgery was similarly associated with extended LOS, defined by a cutoff at the 75th percentile of LOS (days) of the entire study population. Multivariable and machine learning analyses revealed additional variables associated with extended LOS including old age, larger tumor size, tumor invasiveness, and higher comorbidity scores. Use of robotic assistance in surgery, however, did not have a definitive impact on LOS in our study. Our study overall contributes several new insights in terms of key predictive factors of LOS for patients undergoing spinal nerve sheath tumor resection, while also validating findings from prior spinal oncology literature.
Our main finding regarding the superiority of MIS for reducing length-of-stay builds on insights found in related literature. Helal et al.’s meta-analysis of 7 studies covering 302 intradural extramedullary spinal cord tumor patients with a primary pathology of schwannoma and meningioma found that MIS was generally associated with shorter hospital stays. The authors attributed their finding of a quicker recovery time to shorter operative times, lower amounts of operative blood loss, and lower overall operative complication rates associated with MIS, despite maintaining a GTR rate of 92–100%18. Fontes et al. also found reduced complication rates and shorter ICU stays associated with MIS in their analysis of 35 intradural extramedullary tumor patients (primarily meningioma and schwannoma), in addition to reduced hospital costs19. Our study validates this finding to be accurate for spinal nerve sheath tumors specifically as well. But beyond establishing the relevance of surgical approach, our analysis further emphasizes the use of MIS as an important determinant of shorter length of stay in our study over factors relating to tumor burden and patient frailty. While these findings suggest potential benefits of MIS for intradural tumors, it is important to note that such cases must be carefully selected, as the limited exposure inherent to MIS can constrain microsurgical dissection from the spinal cord and nerve roots, particularly in tumors that are adherent or centrally located.
Before KNN matching, geographic variation in MIS use was observed in our analysis with a higher percentage of patients treated with MIS approaches being in the South Atlantic and East North Central regions. Addressing this potential regional disparity through expanding MIS capabilities to other regions and establishing standardized treatment protocols and optimal selection criteria for spinal nerve sheath tumors could be key to improving extended hospital LOS outcomes. Furthermore, such findings may reflect regional differences in institutional practice patterns, access to MIS-trained surgeons, or insurance reimbursement policies. Investigation using datasets with more granular economic and provider-level information is needed to clarify the underlying factors driving these disparities.
Our study also reinforces the impact of tumor burden, represented by factors like invasiveness and size, on hospital length-of-stay. Past literature suggests that these tumor characteristics overall correspond to higher rates of intraoperative blood loss and postoperative complications, which in turn lead to an extended recovery process for patients. Bhimani et al.’s analysis of National Surgical Quality Improvement Program (NSQIP) data for patients with IDEM tumors showed that patients with more invasive tumors, per the definition defined in the respective database, tended to experience more postoperative complications like the need for transfusions or infections20. Zong et al.’s analysis of 37 thoracic spinal schwannoma patients found increased intraoperative blood loss and longer hospital length of stay associated with larger tumors21. Furthermore, higher tumor burden may also fundamentally pose challenges associated with higher rates of residual tumor after surgery. Park et al.’s analysis of 102 benign spinal schwannomas supports this notion of gross total resection being harder to achieve for certain tumors based on larger size, dumbbell and foraminal presence and cervical and sacral locations22. Spinal nerve sheath tumor patients in the MIS cohort in our study (after KNN matching) tended to have larger tumors than those of patients in the open cohort, a finding that approached statistical significance. Intriguingly, patients in the MIS cohort still experienced a lower LOS than patients in the open surgery cohort despite this discrepancy in tumor size. This may suggest that electing the minimally invasive approach may be able to improve postoperative recovery time and complications even for patients with greater tumor burden. However, further insight into the complexity of the cases treated with each approach is necessary to explore and confirm such findings.
Beyond tumor burden, several clinical characteristics of patients including age and comorbidity score also influenced length of stay. This insight aligns well with past literature on the relationship between preoperative functional status and postoperative recovery for patients with intradural tumors. Bhimani’s aforementioned NSQIP study of IDEM tumor patients claimed that patients who were older or who were assigned higher ASA (American Society of Anesthesiologists) classifications were more likely to experience longer LOS and postoperative complications20. Elsamadicy et al.’s study of intradural tumors using the National Inpatient Sample (NIS) database similarly reported that patients with more comorbidities had higher odds of experiencing perioperative complications and extended LOS23. The clear impact of patient comorbidities on LOS suggests several modifiable risk factors that can be addressed preoperatively through increased care coordination for spinal nerve sheath tumor patients.
Regarding the impact of robotic assistance, minimal evidence exists in the literature regarding postoperative outcomes for spinal oncology patients undergoing robotic surgery. Several studies such as a preliminary case series by Menta et al. have suggested the relative safety of robot-assisted surgery for resecting spinal metastases. The authors especially noted a potential advantage in improving accuracy of pedicle screw placement24. Additionally, a study by Barzilai et al. demonstrated that robotic-assisted surgery using the Da Vinci system was effective in achieving GTR of 11 paraspinal nerve sheath tumors located in the thoracic, retroperitoneal, and presacral regions, while preserving neurological function and yielding favorable perioperative outcomes25. The safety and efficacy of robotic-assisted techniques in the resection of nerve sheath tumors have also been further supported in the literature26,27,28. Notably, Barzilai et al. also incorporated intraoperative ultrasound probes and nerve stimulators, paralleling the approach described by Garzon-Muvdi et al., and underscoring ongoing technological advancements and growing optimism surrounding the use of robotic-assisted systems in the surgical management of spinal tumors25,27. While several studies have also concluded benefits of robotic surgery for spinal fusions, our initial findings did not show a definitive benefit to robotic assistance in terms of length of stay. Yet, due to the limitations of the database, we were unable to discern the type of robot employed and its intended application for treatment (soft tissue dissection vs. hardware placement). Further research on the utility of robotic assistance for spinal nerve sheath tumor resection (and spinal oncology at-large) is certainly warranted.
Although the machine learning models demonstrated only modest predictive accuracy, they provided additional context for understanding variable influence beyond the scope of traditional regression. SHAP values in particular offered intuitive insights into feature importance, reinforcing the role of clinical factors such as comorbid burden, tumor size, and surgical approach in predicting LOS. While ML did not replace regression analyses, it served a valuable hypothesis-generating function and highlighted potential areas for further investigation in larger, prospective datasets.
Limitations
There are several limitations to this study. Firstly, as a retrospective database study, we cannot make any definitive claims of causality for the significant associations found between key variables. The NCDB data also lacks certain clinical and demographic patient-specific information that would have been worth incorporating into our analyses. For example, potential predictor variables like exact tumor location, presenting symptoms (e.g. bowel or bladder dysfunction), and perioperative laboratory values were not available in the database. NCDB also does not have several outcome variables of interest such as presence of postoperative complications, discharge disposition, or 30-day readmission/reoperation. Another limitation of the ML analysis is the suboptimal predictive accuracy of all models. The restricted variable set available in NCDB likely lacks sufficient granularity to capture key predictors of extended LOS. Additionally, the imbalance in outcome classes and small MIS samples may have further hindered performance. Given these limitations, the machine learning analysis should be interpreted as an exploratory or hypothesis-generating effort rather than a definitive predictive tool. Furthermore, the NCDB does not specify how the robot was utilized, whether for dissection with the Da Vinci system or spinal instrumentation with the Globus Excelcius system, limiting our ability to interpret its true role in outcomes. Given that only 3.4% of patients underwent MIS, this reflects highly selective use likely based on tumor location, case complexity, and surgeon preference. While observable confounders were adjusted for using propensity score matching and multivariable models, unmeasured variables such as exact anatomical location, intradural involvement, and surgeon-level factors were not available in the NCDB and may have influenced both treatment selection and outcomes. In particular, the inability to distinguish between intradural and extradural tumors is a major limitation, as this classification is critical to surgical planning and complexity. Without this level of granularity, it remains unclear whether the observed differences in length of stay are attributable to the surgical approach itself or to inherent differences in tumor location and complexity. As such, the observed association between MIS and reduced LOS may be subject to residual confounding, and these findings should be interpreted as exploratory, warranting confirmation in prospective studies with more granular clinical data. In connection, the NCDB lacks several critical clinical and outcome variables that likely influence length of stay, including tumor anatomical location (foraminal vs. intradural), presenting symptoms (radiculopathy, bowel/bladder dysfunction), postoperative complications, 30-day readmission or reoperation, discharge disposition, and postoperative functional status. The absence of these variables limits our ability to control for important confounders and interpret functional recovery, underscoring the need for more granular prospective datasets. Despite these limitations, our study is the first to provide insights into the impact of surgical approach on patient recovery and resource utilization (via a proxy of length of stay) for spinal nerve sheath tumor patients.
Conclusion
MIS for spinal nerve sheath tumor resection was associated with significantly lower odds of extended length of stay compared to open surgery. Although only a small proportion of patients underwent MIS, the findings support its use in appropriately selected cases. Robotic assistance did not confer additional benefit in this context. Given the lack of granular tumor and surgical detail in the NCDB, these results should be interpreted as exploratory. Further prospective studies are needed to validate these findings and better define the role of MIS and robotics in spinal tumor surgery.
Funding declaration
There was no funding.

Flowchart of the Cohort Selection and Representation of Treatment Distribution.

Multivariable logistic regression model showing adjusted odds ratios (ORs) and 95% confidence intervals for predictors of extended length of stay. All variables listed were included simultaneously in a single model. Statistically significant predictors (p < 0.05).

Predictive Modeling of Extended Length of Stay in Spinal Nerve Sheath Tumor Surgery. (A) ROC curves for each machine learning model based on predictions made on test sets during stratified 5-fold cross-validation. (B) Boxplots showing the distribution of ROC-AUC scores across validation folds for each model, reflecting variability and model stability. (C) SHAP summary plot illustrating the direction and magnitude of feature contributions to extended LOS prediction, with higher SHAP values indicating stronger influence on model output. (D) Bar plot showing mean SHAP feature importance scores from the best-performing (Gradient Boosting model) identifying the most influential predictors for extended LOS.
Data availability
The data used in this study are available from the National Cancer Database (https://www.facs.org/quality-programs/cancer/ncdb ).
References
McCormick, P. C. & Stein, B. M. Intramedullary tumors in adults. Neurosurg. Clin. N Am. 1 (3), 609–630 (1990).
Wen, P. Y. & Packer, R. J. The 2021 WHO classification of tumors of the central nervous system: clinical implications. Neuro Oncol. 23 (8), 1215–1217 (2021).
Jinnai, T. & Koyama, T. Clinical characteristics of spinal nerve sheath tumors: analysis of 149 cases. Neurosurgery 56 (3), 510–515 (2005). discussion 510–515.
Singh, A. et al. Long-Term functional outcomes following surgical treatment of spinal schwannomas: A Population-Based cohort study. Cancers (Basel). 16 (3). https://doi.org/10.3390/cancers16030519 (2024).
Moini, J., Avgeropoulos, N. G. & Samsam, M. Schwannoma. In: Epidemiology of Brain and Spinal Tumors. 179–196 (Elsevier, 2021).
Desai, K. I. The surgical management of symptomatic benign peripheral nerve sheath tumors of the neck and extremities: an experience of 442 cases. Neurosurgery 81 (4), 568–580 (2017).
Halvorsen, C. M. et al. The long-term outcome after resection of intraspinal nerve sheath tumors: report of 131 consecutive cases. Neurosurgery 77 (4), 585–592 (2015). discussion 592–593.
Alvarez-Crespo, D. J. et al. Clinical characteristics and surgical outcomes of 2542 patients with spinal schwannomas: A systematic review and Meta-Analysis. World Neurosurg. 182, 165–183e1 (2024).
Argiti, K. et al. Minimally invasive tubular removal of spinal Schwannoma and neurofibroma - a case series of 49 patients and review of the literature. Neurosurg. Rev. 47 (1), 418 (2024).
Kumar, N. et al. Factors influencing extended hospital stay in patients undergoing metastatic spine tumour surgery and its impact on survival. J Clin. Neurosci. 27 https://doi.org/10.1016/j.jocn.2018.06.041 (2018).
Arora, A. et al. Predictive models to assess risk of extended length of stay in adults with spinal deformity and lumbar degenerative pathology: development and internal validation. Spine J. 23 (3), 457–466 (2023).
Adogwa, O., Parker, S. L., Bydon, A., Cheng, J. & McGirt, M. J. Comparative effectiveness of minimally invasive versus open transforaminal lumbar interbody fusion: 2-year assessment of narcotic use, return to work, disability, and quality of life. J. Spinal Disord Tech. 24 (8), 479–484 (2011).
Parker, S. L., Lerner, J. & McGirt, M. J. Effect of minimally invasive technique on return to work and narcotic use following transforaminal lumbar inter-body fusion: a review. Prof. Case Manag. 17 (5), 229–235 (2012).
Banczerowski, P. et al. Minimally invasive spine surgery: systematic review. Neurosurg. Rev. 38 (1), 11–26 (2015).
Zuckerman, S. L. et al. When less is more: the indications for MIS techniques and separation surgery in metastatic spine disease. Spine (Phila Pa. 1976). 41 (Suppl 20), S246–S253 (2016).
Sanders, A. & Cromartie, J. Rural-Urban Continuum Codes. (accessed 7 November 2024). https://www.ers.usda.gov/data-products/rural-urban-continuum-codes
Concept Charlson Comorbidity Index. (accessed 7 November 2024). http://mchp-appserv.cpe.umanitoba.ca/viewConcept.php?conceptID=1098
Helal, A., Yolcu, Y. U., Kamath, A., Wahood, W. & Bydon, M. Minimally invasive versus open surgery for patients undergoing intradural extramedullary spinal cord tumor resection: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 214 (107176), 107176 (2022).
Fontes, R. B. V., Wewel, J. T. & OʼToole, J. E. Perioperative cost analysis of minimally invasive vs open resection of intradural extramedullary spinal cord tumors. Neurosurgery 78 (4), 531–539 (2016).
Bhimani, A. D. et al. Surgical complications in intradural extramedullary spinal cord tumors - an ACS-NSQIP analysis of spinal cord level and malignancy. World Neurosurg. 117, e290–e299 (2018).
Zong, S., Zeng, G., Xiong, C. & Wei, B. Treatment results in the differential surgery of intradural extramedullary Schwannoma of 110 cases. PLoS One. 8 (5), e63867 (2013).
Park, B. J. et al. Spinal nerve sheath tumors: factors associated with postoperative residual and recurrent tumors: A single-center experience. World Neurosurg. 167, e1062–e1071 (2022).
Elsamadicy, A. A. et al. Cost and health care resource utilization differences after spine surgery for bony spine versus primary intradural spine tumors. World Neurosurg. 151, e286–e298 (2021).
Menta, A. K. et al. Robotic assisted surgery for the treatment of spinal metastases: A case series. Clin. Neurol. Neurosurg. 243 (108393), 108393 (2024).
Barzilai, O. et al. Robotic resection of spinal and paraspinal tumors. Oper. Neurosurg. (Hagerstown). 28 (5), 608–616 (2025).
Rapoport, B. I. et al. Robotic resection of a nerve sheath tumor via a retroperitoneal approach. Oper. Neurosurg. (Hagerstown). 20 (2), E85–E90 (2021).
Garzon-Muvdi, T., Belzberg, A., Allaf, M. E. & Wolinsky, J. P. Intraoperative nerve monitoring in robotic-assisted resection of presacral ganglioneuroma: operative technique. Oper. Neurosurg. (Hagerstown). 16 (1), 103–110 (2019).
Finley, D., Sherman, J. H., Avila, E. & Bilsky, M. Thorascopic resection of an apical paraspinal Schwannoma using the Da Vinci surgical system. J. Neurol. Surg. Cent. Eur. Neurosurg. 75 (1), 58–63 (2014).
Author information
Authors and Affiliations
Contributions
A.K.G. and D.L. conceptualized and supervised the study. A.K.G., T.K., and X.Y. performed data acquisition, preprocessing, and statistical analysis. S.B. and L.T. contributed to methodology design and result interpretation. Y.X. and R.C. supported clinical validation and critically reviewed the manuscript. T.A. and J.K. assisted with literature review and drafting of the discussion. A.K.A. contributed to manuscript editing and visualization of key results. N.T. provided neurosurgical expertise and oversight throughout the study. A.K.G. wrote the initial manuscript draft. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Khalilullah, T., Ghaith, A.K., Yang, X. et al. Extended length of stay in open versus minimally invasive surgery with robotic-assisted sub-analysis for spinal nerve sheath tumor resection: a nationwide analysis. Sci Rep 15, 30309 (2025). https://doi.org/10.1038/s41598-025-15121-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-15121-6
