
Abstract
To observe the efficacy and safety of single-access minimally invasive percutaneous nephrolithotomy (MPCNL) combined with flexible cystoscopy and multi-access MPCNL in patients with complex renal stones (CRS). A total of 195 patients with CRS were prospectively randomized into two groups. Ninety-eight in the single-access MPCNL group and 97 cases as control in the multi-access MPCNL group. The stone-free rates (SFRs) at different times were considered as the primary outcome of the study. The secondary end points were operative time, hemoglobin decrease, postoperative hospital stay and operation-related complications. There was no obvious difference between two groups in patients’ demographics and preoperative clinical characteristics (All P > 0.05). Postoperative data showed that mean decrease in hemoglobin level was less in single-access MPCNL group than that in multi-access MPCNL group (P < 0.001). Postoperative hospital stay in single-access MPCNL group was more shorten than that in multi-access MPCNL group (P < 0.001). Moreover, the SFRs of the postoperative 2nd day and 4th week in single-access MPCNL group were both significantly higher than those in multi-access MPCNL group (Both P < 0.05). However, in terms of the rates of low back pain, perirenal hematoma and renal artery embolization, multi-access MPCNL group were all significantly higher than single-access MPCNL group (All P < 0.05). Our study shows that single-access MPCNL and flexible cystoscopy are ideal complementary techniques in the treatment of CRS, satisfying both high SFR and minimized renal injury. This method was safe and reproducible in clinical practice.
Similar content being viewed by others

Introduction
Renal stones are a common disease in urology, often accompanied by various discomfort symptoms, such as low back pain, hematuria, vomiting, nausea, fever, etc. 1. Complex renal stones (CRS) are a challenging type in the classification of renal stones, characterized by high stone burden, distribution in various calices, urinary tract infection (UTI) and renal dysfunction, high surgical risk, or high incidence of complications, including multiple stones, staghorn stones, and isolated renal stones2,3,4. Surgery remains the main treatment for CRS. The traditional surgical method is open nephrolithotomy, which has the disadvantages of large trauma, slow postoperative recovery, and high complications5.
Minimally invasive percutaneous nephrolithotomy (MPCNL) is currently the most widely used and has achieved satisfactory therapeutic effects in CRS. Large T6 et al. reported that single-access MPCNL for CRS was safe and effective for higher stone-free rates (SFRs) and lower complication rates which were similar with standard PCNL. Meanwhile, Balaji S et al.7 considered that multi-access MPCNL was found to be safe, feasible and effective for the management of large burden CRS with respect to stone clearance and morbidity associated with the procedure. It was cost effective and complete stone clearance as a single procedure was higher in comparison to flexible ureteroscopy (FURS) and extracorporeal shock wave lithotripsy (ESWL). Despite the proven advantages of this technique for CRS, it still remains under-utilized for the fear of complications, especially for multi-access MPCNL8. Single-access MPCNL is always difficult to remove all stones due to the angle of the renal calyx for the CRS. To solve these problems, we find in practice that flexible cystoscopy can compensate some limitations of MPCNL. Firstly, flexible cystoscopy can increase the SFRs of MPCNL by searching residual stones or fragments in locations that are inaccessible by MPCNL, such as beside the MPCNL tract insertion. Secondly, flexible cystoscopy can decrease the possibility of establishing the second or third access tracts. Furthermore, stone fragments broken via flexible cystoscopy are also easily washed out through the MPCNL tract. Therefore, the two procedures can well complement each other in lithotripsy.
Higher SFR and lower surgical complications have always been the pursuit of urologists. Different procedures for lithotripsy will inevitably bring different SFR and operative results, so selecting the optimal surgical modality will be a challenge. However, few studies have focused on the comparison between single-access MPCNL combined with flexible cystoscopy and multi-access MPCNL for CRS. Therefore, we conduct this prospective randomized controlled study to investigate whether patients can benefit more from the combination of single-access MPCNL and flexible cystoscopy than multi-access MPCNL.
Patients and methods
Patients
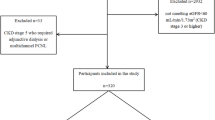
Patients with CRS referred to our institute between October 2021 to March 2024 were considered for this study. Applying strict inclusion criteria, the patients were randomly assigned to the treatment groups using the envelope method. The study included 195 patients, 98 in the single-access MPCNL group and 97 in the multi-access MPCNL group, based on power analysis performed to estimate the sample size (Fig. 1). The participants’ pretreatment evaluation included medical history, physical examination, laboratory investigations (urine analysis, urine culture and/or sensitivity, complete blood count, blood urea nitrogen, serum levels of creatinine, C-reactive protein, and procalcitonin), and radiologic investigations. Patients with a known UTI received antibiotic treatment until infection control was achieved. The protocol for this study has been accepted by the Chinese Clinical Trial Registry (Ethics approval number: ChiCTR2200056402). Meanwhile, The study was approved by the clinical research ethics committee of the Affiliated Jiangning Hospital of Nanjing Medical University (ethics approval number: 202110378). Written informed consent was obtained from all participants. The study followed the principles of the Helsinki Declaration.

Flowchart for cases selection.
Randomization and masking
Parallel randomization was conducted using a stratified approach in our study. Our center enrolled 195 participants, randomized in a 1:1 ratio to either the single-access MPCNL group or the multi-access MPCNL group. Electronic generation of the randomization sequence took place before patient inclusion. Consecutively numbered, sealed envelopes were utilized for random sequence allocation and concealment. After the patients changed their position to prone position and before percutaneous renal puncture, the sealed envelope was opened by a designated nurse, revealing the specific surgical methods. Subsequently, at the conclusion of the procedure, the same individual automatically recorded the operative data.
Perioperative and surgical procedures
All patients underwent a plain preoperative abdominal radiography of the kidneys, ureters, and bladder and unenhanced computed tomography (CT) to assess hydronephrosis and the size, location, and number of the stones. We usually performed preprocedural urine cultures and applied appropriate antibiotic therapy based on the culture-antibiogram test results. The opportunity for operation depended on a downward trend in infection indicators and a negative urine culture. Patients who had negative urine culture took standard peri-operative antibiotic prophylaxis (single shot of cefuroxime 200 mg or levofloxacin 500 mg in cases of allergy) 30 min before intervention. Stone score include stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E). It was found to predict treatment success and the risk of perioperative complications after PCNL9. All procedures were performed by the same urologist in the study. The selection of the surgical method for the enrolled patients was random, excluding any artificial subjective factors.
Multi-access MPCNL
Under genel anesthesia, the patient was placed in a lithotomy position. A 6Fr ureteral catheter (Boston Scientific, USA) was inserted into the ureteropelvic junction of the target ureter. The patient was then turned to a prone position and the percutaneous tract was punctured under ultrasonographic guidance with an 18-gauge coaxial needle (Cook Medical, USA). Chief surgeon planed the number of percutaneous renal accesses before surgery and establish upper access firstly to facilitate intraoperative operations. The percutaneous tract was serially dilated using fascial dilators (Cook Medical, USA) of up to 20 Fr. Then a nephroscope (8.5/11 Fr, Suode medical, Hangzhou, China) was inserted into the collecting system to fragment stones within the field of view by a 550 μm holmium laser fiber with the settings of 40–60 W ((1.6-2) J * (25–30) HZ) based on the hardness of stones. Smaller stone fragments were washed out through the sheath by retrograde irrigation. We always used ultrasound to monitor the clearance of stones in real-time during surgery. The second or third access tracts (18 Fr) would be established to achieve maximum SFR. A 6 Fr double-J stent (Bard, USA) was inserted into the ureter using a loach guidewire (Bard, USA) and nephrostomy tubes (14 Fr) was placed.
Single-access MPCNL combined with flexible cystoscopy
The method of establishing percutaneous renal accesses was similar to that of multi-access MPCNL group, but we will choose a renal calyx that can maximize the clearance of stones. Then the disposable electronic flexible cystoscopy (PC515, Pusen medical, Zhuhai, China) was operated to search and fragment residual stones in the inaccessible locations of nephroscope (mainly beside the PCNL tract insertion) (Fig. 2). At the conclusion of procedure, ultrasound were taken to assess stone clearance. Similarly, a 6 Fr double-J stent and a 14 Fr nephrostomy tube were placed separately. The KUB results of one patient, who has multiple stones, were shown in Fig. 3. During the surgery, a flexible cystoscopy was used to search for residual stones, ultimately achieving complete removal of the stones.

Diagram for single-access MPCNL combined with flexible cystoscopy.

KUB during the perioperative period (A preoperative; B postoperative).
Postoperative follow-up
All patients were checked including complete blood count, routine urinalysis, serum creatinine, procalcitonin and KUB at the postoperative 2nd day and 4th week. If stone composition was pure uric acid or cystine that could not be showed in KUB films, an ultra-low-dose CT examination would be taken to evaluate the residual stones. The stone-free status was defined as no radiological evidence of stone or the presence of ≤ 2 mm asymptomatic fragments in the urinary system10,11. The primary study outcome was the SFRs at the 2nd day postoperatively. The secondary endpoints were SFRs at the 4th week postoperatively, operative time, hemoglobin decrease, postoperative hospital stay and operation-related complications. Postoperative complications were graded according to the modified Clavien classification system as applied to PCNL12,13. If the patient had no residual stones and evidence of bleeding or infection, nephrostomy tube would be removed at the postoperative 3rd day and double-J stent was removed at the postoperative 4th week. Patients with residual stones underwent auxiliary procedures four weeks or more after surgery. These included external physical vibration lithecbole (EPVL), ESWL, or position therapy14,15.
Statistical analysis
IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables are presented as means ± standard deviations. The groups were compared for patient demographics, follow-up, and surgical outcomes using independent samples t-test; The Shapiro-Wilk test was used to test the normality of the initial data. A chi-squared test compared the groups for other pre- and postoperative clinical characteristics. A P-value < 0.05 was considered statistically significant. The STONE score can vary from a minimum of 3 to a maximum of 12. A score of 3–5 denotes the ‘low complex stone’, a score of 6–8 denotes ‘moderate complex stone’, and a score of 9–12 reveals ‘the high complex stone’9.
Results
Demographics and preoperative clinical characteristics
The 195 patients in this study were randomly assigned to the single-access MPCNL (n = 98) or the multi-access MPCNL (n = 97) group. The groups were similar in the patients’ demographics and preoperative clinical characteristics (Table 1). The mean STONE score was 8.9 in single-access MPCNL group and 8.7 in multi-access MPCNL group, and no significant difference was found (P = 0.148). In addition, there was no substantial difference between the two groups in mean age at diagnosis, body mass index, sex ratio, history of hypertension and diabetes, STONE score, degree of hydronephrosis, urine culture, distribution of stones and histories of upper urinary stone operation (all P > 0.05).
Postoperative clinical characteristics
Differences in postoperative clinical outcomes between two groups were shown in Table 2. Mean operative time between two groups was similar (P > 0.05). Mean decrease in hemoglobin level was less in single-access MPCNL group than that in multi-access MPCNL group (7.3 vs. 13.4 g/L, P < 0.001). Meanwhile, postoperative hospital stay in single-access MPCNL group was shorter than that in multi-access MPCNL group (4.2 vs. 5.1 days, P < 0.001). Moreover, the SFRs of the postoperative 2nd day and 4th week in single-access MPCNL group were both significantly higher than those in multi-access MPCNL group (88.8% vs. 74.2%, P = 0.009; 94.9% vs. 85.6%, P = 0.028, respectively). Postoperative complications were classified using the modified Clavien system, including fever (≥ 38.5℃), low back pain, perirenal hematoma, renal artery embolization and urosepsis. In terms of the rates of low back pain, perirenal hematoma and renal artery embolization, multi-access MPCNL group were all significantly higher than single-access MPCNL group (18.5 vs. 7.1%, P = 0.017; 13.4 vs. 4.1%, P = 0.021; 4.1 vs. 0.0%, P = 0.042; respectively). No case needed blood transfusion in single-access MPCNL group and one case needed blood transfusion in multi-access MPCNL group. No significant difference was found between two groups in stone compositions (P > 0.05).
Discussion
Currently, various minimally invasive treatment strategies have succeeded in the treatment of renal stones16,17. For the CRS, there is still a need to develop a surgical procedure satisfying both high SFR and minimized renal injury. In the past decade, more and more researches were focusing on multi-access MPCNL for the treatment of CRS5,18,19. Although the surgical method can increase the SFR, it may invisibly increase the occurrence of complications such as renal parenchymal damage and bleeding. However, compared with multi-access MPCNL, single-access MPCNL often requires more operative duration and postoperative ancillary treatments20,21. Furthermore, single-access MPCNL commonly has more blind areas in renal collecting system. So we consider to develop a new hybrid technique, combining single-access MPCNL with flexible cystoscopy, to avoid the shortcomings of multi-access MPCNL and further improve therapeutic outcomes of CRS.
Improving the SFR and reducing the recurrence rate of CRS has always been a key and difficult point in treatment22,23. Given the high risk of stone recurrence, it is imperative to implement effective preventive and therapeutic measures for those identified at high risk24,25. A one-year follow-up analysis pinpointed the treatment regimen, BMI, and STONE score as significant independent risk factors for the recurrence of renal stones26. However, no substantial difference between the two groups in our study was observed in demographics and preoperative clinical characteristics. Then treatment regimen became the key to solving problems. In response to these challenges, our study explored the efficacy of combining MPCNL with flexible cystoscopy for a more comprehensive management of CRS, especially those located in hard-to-reach areas. The introduction of flexible cystoscopy offers a precise method for locating and addressing stones in areas of the renal that are traditionally difficult to reach. Thus, our outcomes showed that the initial and total SFRs in single-access MPCNL group were both significantly higher than those in multi-access MPCNL group (88.8% vs. 74.2%, P = 0.009; 94.9% vs. 85.6%, P = 0.028, respectively).
Flexible cystoscopy in the hybrid technique can increase intraoperative visual fields to search residual stones and decrease the possibility of establishing multiple percutaneous tracts. Complications in PCNL were directly proportional to the number of percutaneous tracts used for the stone clearance. In a meta-analysis, the complications of multi-access MPCNL varied from 5 to 44% overall7. Gorbachinsky I et al. showed that multi-access PCNL was associated with a significant reduction in the function of the targeted kidney compared to a single access approach27. Another study reported that single-access PCNL provides excellent outcomes in the treatment of CRS, including high SFRs and minimal morbidity6. These coincides with our research findings. Our data also showed that multi-access MPCNL group were all significantly higher than single-access MPCNL group (18.5 vs. 7.1%, P = 0.017; 13.4 vs. 4.1%, P = 0.021; 4.1 vs. 0.0%, P = 0.042; respectively) in terms of the rates of low back pain, perirenal hematoma and renal artery embolization.
In addition, for CRS, our study showed that single-access MPCNL was inefficient and safe with the assistance of flexible cystoscopy. Mean decrease in hemoglobin level was less in single-access MPCNL group than that in multi-access MPCNL group (7.3 vs. 13.4 g/L, P < 0.001). And postoperative hospital stay in single-access MPCNL group was more shorten than that in multi-access MPCNL group (4.2 vs. 5.1 days, P < 0.001). As was approved by before, this was related to the number of percutaneous tracts established in MPCNL. The mean operative time reached 96.7 min in single-access MPCNL group and was similar between two groups (P > 0.05).
Finally, there are also some limitations in our study. Firstly, the follow-up is short and may have affected the outcome. Furthermore, the study is based on single center with a small sample size and there may be certain sampling errors. Therefore, large-scale multicenter prospective studies are still needed to further prove the above conclusions. We believe that the ideal procedure will be formulated through a long period of clinical application and observation.
Conclusions
Our study shows that single-access MPCNL and flexible cystoscopy are ideal complementary techniques in the treatment of CRS, satisfying both high SFR and minimized renal injury. This method was safe and reproducible in clinical practice. However, large-scale multicenter prospective studies are still needed to further prove the above conclusions.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to the nature of this research participants of this study did not agree for their data to be shared publicly, so supporting data is not available, but are available from the corresponding author on reasonable request.
References
Perri, D. et al. A proposed mathematical model to help preoperative planning between RIRS and miniperc for renal stones between 10 and 20 mm using holmium:yag laser (Cyber Ho): the stone management according to size-hardness (SMASH) score. Urolithiasis 52 (1), 58. https://doi.org/10.1007/s00240-024-01536-9 (2024).
Perri, D. et al. Risk of bleeding after retrograde intrarenal surgery vs miniaturised percutaneous nephrolithotomy for 10–20 mm renal stones: a not so different safety profile. BJU Int. 19 https://doi.org/10.1111/bju.16585 (2024 Nov).
Singh, A. G. et al. Role of flexible uretero-renoscopy in management of renal calculi in anomalous kidneys: single-center experience. World J. Urol. 35 (2), 319–324. https://doi.org/10.1007/s00345-016-1881-8 (2017).
Zhu, H. et al. Multiple-tract percutaneous nephrolithotomy as a day surgery for the treatment of complex renal stones: an initial experience. World J. Urol. 39 (3), 921–927. https://doi.org/10.1007/s00345-020-03260-6 (2021).
Liang, T. et al. Multi-tract percutaneous nephrolithotomy combined with EMS lithotripsy for bilateral complex renal stones: our experience. BMC Urol. 17 (1), 15. https://doi.org/10.1186/s12894-017-0205-7 (2017).
Large, T. et al. A Multi-institutional review of Single-access percutaneous nephrolithotomy for complex Staghorn stones. Eur. Urol. Focus. 7 (5), 1170–1175. https://doi.org/10.1016/j.euf.2020.11.005 (2021).
Balaji, S. et al. Contemporary role of multi-tract percutaneous nephrolithotomy in the treatment of complex renal calculi. Asian J. Urol. 7 (2), 102–109. https://doi.org/10.1016/j.ajur.2019.12.012 (2020).
Ganpule, A. P., Mishra, S. & Desai, M. R. Multiperc versus single perc with flexible instrumentation for staghorn calculi. J Endourol. ;23(10):1675-8. (2009). https://doi.org/10.1089/end.2009.1535. PMID: 19715481.
Okhunov, Z. et al. S.T.O.N.E. Nephrolithometry: novel surgical classification system for kidney calculi. Urology 81 (6), 1154–1159. https://doi.org/10.1016/j.urology.2012.10.083 (2013).
Ghani, K. R. & Wolf, J. S. Jr What is the stone-free rate following flexible ureteroscopy for kidney stones? Nat. Rev. Urol. 12 (5), 281–288. https://doi.org/10.1038/nrurol.2015.74 (2015).
Dauw, C. A. et al. Contemporary practice patterns of flexible ureteroscopy for treating renal stones: results of a worldwide survey. J. Endourol. 29 (11), 1221–1230. https://doi.org/10.1089/end.2015.0260 (2015).
Singh, A. K. et al. Using the modified clavien grading system to classify complications of percutaneous nephrolithotomy. Curr. Urol. 11 (2), 79–84. https://doi.org/10.1159/000447198 (2018).
Labate, G. et al. The percutaneous nephrolithotomy global study: classification of complications. J. Endourol. 25 (8), 1275–1280. https://doi.org/10.1089/end.2011.0067 (2011).
Tao, R. Z. et al. External physical vibration Lithecbole facilitating the expulsion of upper ureteric stones 1.0–2.0 cm after extracorporeal shock wave lithotripsy: a prospective randomized trial. Urolithiasis 48 (1), 71–77. https://doi.org/10.1007/s00240-018-1100-8 (2020).
Yang, J. et al. Efficacy analysis of self-help position therapy after holmium laser lithotripsy via flexible ureteroscopy. BMC Urol. 18 (1), 33. https://doi.org/10.1186/s12894-018-0348-1 (2018).
Zeng, G. et al. Super-mini percutaneous nephrolithotomy (SMP): a new concept in technique and instrumentation. BJU Int. 117 (4), 655–661. https://doi.org/10.1111/bju.13242 (2016).
Desai, J. et al. A novel technique of ultra-mini-percutaneous nephrolithotomy: introduction and an initial experience for treatment of upper urinary calculi less than 2 cm. Biomed. Res. Int. 2013, 490793. https://doi.org/10.1155/2013/490793 (2013).
Liatsikos, E. N. et al. Multiple tracts through a single incision for Staghorn calculous treatment in a single session. Eur. Urol. 48 (5), 832–837. https://doi.org/10.1016/j.eururo.2005.08.009 (2005).
Liu, C. et al. The optimal minimally invasive percutaneous nephrolithotomy strategy for the treatment of Staghorn stones in a solitary kidney. Urolithiasis 44 (2), 149–154. https://doi.org/10.1007/s00240-015-0803-3 (2016).
Li, X. et al. Chinese minimally invasive percutaneous nephrolithotomy: the Guangzhou experience. J. Endourol. 23 (10), 1693–1697. https://doi.org/10.1089/end.2009.1537 (2009).
Hamamoto, S. et al. Endoscopic combined intrarenal surgery for large calculi: simultaneous use of flexible ureteroscopy and mini-percutaneous nephrolithotomy overcomes the disadvantageous of percutaneous nephrolithotomy monotherapy. J. Endourol. 28 (1), 28–33. https://doi.org/10.1089/end.2013.0361 (2014).
Widyokirono, D. R. et al. Endoscopic combined intrarenal surgery vs percutaneous nephrolithotomy for large and complex renal stone: A systematic review and Meta-Analysis. J. Endourol. 36 (7), 865–876. https://doi.org/10.1089/end.2021.0761 (2022).
Rashid, A. O., Amin, S. H., Al Kadum, M. A., Mohammed, S. K. & Buchholz, N. Mini-Percutaneous nephrolithotomy for complex Staghorn stones in children. Urol. Int. 102 (3), 356–359. https://doi.org/10.1159/000499491 (2019).
Fan, B. Y., Gu, L., Chand, H., Liu, W. J. & Yuan, J. B. Mini-percutaneous nephrolithotomy for pediatric complex renal calculus disease: one-stage or two-stage? Int. Urol. Nephrol. 51 (2), 201–206. https://doi.org/10.1007/s11255-018-2054-z (2019). Epub 2018 Dec 12.
Kavoussi, N. L. et al. Feasibility of stone recurrence risk stratification using the recurrence of kidney stone (ROKS) nomogram. Urolithiasis 51 (1), 73. https://doi.org/10.1007/s00240-023-01446-2 (2023).
Laurenius, A. et al. Incidence of Kidney Stones After Metabolic and Bariatric Surgery-Data from the Scandinavian Obesity Surgery Registry. Obes. Surg. ;33(5):1564–1570. doi: https://doi.org/10.1007/s11695-023-06561-y. (2023).
Gorbachinsky, I. et al. Evaluation of renal function after percutaneous Nephrolithotomy-Does the number of percutaneous access tracts matter?? J. Urol. 196 (1), 131–136. https://doi.org/10.1016/j.juro.2016.01.121 (2016).
Acknowledgements
We thank Dr. Rong-zhen Tao and Prof. Qing-lai Tang for technical assistance and manuscript preparation. This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
QL Tang and RZ Tao: Project development. JD Guo and DJ Wang: Data Collection. JY Ji, YY Tu and XZ Zhou: Data analysis and Manuscript writing. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tang, Ql., Ji, Jb., Tu, Yy. et al. Single-access mini-PCNL with flexible cystoscopy vs. multi-access mini-PCNL for complex renal stones in prospective study. Sci Rep 15, 30523 (2025). https://doi.org/10.1038/s41598-025-15887-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-15887-9
