
Abstract
The Mexican Social Security Institute registered a significant number of suspected Zika virus (ZIKV) cases during the 2016–2018 outbreak. This study aims to describe the distribution of confirmed ZIKV cases, their correlation with rainfall and temperature, and associated factors with infection or hospitalization, considering pregnancy. A retrospective analysis was performed on 13,259 suspected ZIKV cases. Binary logistic regression was performed to determine potentially associated factors with infection or hospitalization. Correlations between positive cases and environmental factors were analyzed using the Pearson correlation and an autoregressive integrated moving average (ARIMA) test. Female sex and age > 30 were associated with ZIKV infection when excluding pregnant women. In pregnant women, a higher infection rate in the first and second trimesters compared to third trimester was observed. In Veracruz, rainfall correlated with positive cases in 2016 (n = 5; r = 0.9977, p < 0.001) and 2017 (n = 12; r = 0.7467, p = 0.005) correlated with rainfall only in 2017 (r = 0.7975, p = 0.002); this was not significant with the ARIMA analysis. Further research is suggested to elucidate factors involved in the transmission, pathogenicity and epidemiology of this and other vector-borne disease viruse.
Similar content being viewed by others


Introduction
Vector-borne diseases were recognized at the beginning of the last century, but they have gained greater importance in the last decade due to significant outbreaks1. One vector-borne disease that had a great impact in Latin America is the Zika virus disease (ZVD), which is caused by the Orthoflavivirus zikaense species and is transmitted to humans by mosquitoes of the genus Aedes2,3. From the 1960s to the 1980s, local Zika outbreaks occurred in Africa and Asia. Favorable weather and the flow of travelers caused the spread of the virus in India, China, Indonesia, the Philippines, and Thailand3,4, but it was not until 2007 that the first global Zika virus (ZIKV) outbreak occurred in Yap Island, Micronesia5. Later, in 2015, the transmission of ZIKV was confirmed in Latin American countries including Brazil, Colombia, and Mexico6. In 2016, due to multiple outbreaks and aspects such as the association between ZIKV with Guillain-Barre syndrome, microcephaly in newborns7, and the confirmation of sexual, blood transfusion–related, and maternal–fetal transmission of ZIKV8, the World Health Organization declared ZVD to be a global emergency7. ZIKV was initially detected through RNA determination and neutralizing antibodies in the patient’s serum5,9; nonetheless, the gold standard is the reverse transcription and quantitative polymerase chain reaction (RT-qPCR) assay10, performed on blood, saliva, milk, semen, and conjunctival and vaginal secretions11,12.
Many studies have been conducted to elucidate an algorithm that allows for predicting ZIKV outbreaks; however, the intervention of a vector for transmission makes this a complex task13,14,15. Among the most studied variables for ZIKV outbreak prediction, some socio-demographic and environmental conditions have been associated with the vector distribution16,17,18. Moreover, climate change has increased the prevalence of vector-borne diseases, including ZIKV19. Environmental factors such as rainfall and temperature, which contribute to the reproduction of the respective vectors, must be analyzed in the context of every specific population to determine their impact.
Since the 2016 outbreak, ZVD remains under epidemiological surveillance in most countries20,21,22,23. In Mexico, there is an epidemiological surveillance system for ZIKV and other mosquito-transmitted diseases6. The Mexican Social Security Institute (IMSS, its acronym in Spanish) is the largest health system in Mexico, covering more than 50% of the national population24. It offers healthcare and social security services to private sector workers and individual contributors and their dependents; it is financed by the federal government, employer contributions, and employee tax payrolls. Since 2009, the IMSS has established a network of epidemiological surveillance laboratories carrying out the molecular diagnosis of viral diseases including influenza, chikungunya, dengue, Zika and, more recently, COVID-19. The collected information is integrated into the National Epidemiological Surveillances System (SINAVE), which belongs to the General Directorate of Epidemiology.
To the best of our knowledge, the distribution of Zika cases, the potential associated factors with infection and hospitalization in a Mexican population including pregnant women have not been described, even when it is known that pregnancy implies variability and alterations of the immune response25. This work aims to describe the confirmed RT-qPCR ZIKV cases reported by the epidemiological surveillance laboratory network from the IMSS from August 2016 to January 2018, the potential factors associated with infection and hospitalization, and the relationship of ZIKV positive cases with average rainfall scores and temperature. This study thus contributes to the knowledge of ZIKV transmission in Mexico and explores their relationship with factors previously described in the literature.
Methods
Study design and selection criteria
A retrospective study was conducted based on the IMSS ZIKV surveillance data system of four regional molecular diagnostic laboratories authorized by the Institute of Epidemiological Diagnosis and Reference (InDRE), the National Reference Laboratory of the country; they are located in Nuevo Leon, Jalisco, Yucatan, and Mexico City6. Data were analyzed from symptomatic suspected cases of ZIKV whose patient samples were sent for molecular diagnosis by RT-qPCR test from August 2016 to January 2018. The information collected corresponds to those symptomatic patients who came seeking medical attention, including pregnant women, treated in first- and second-level medical units throughout the national territory, who met the operational definition of a suspected case of ZVD. Records with missing data for age, residence state, sampling date, pregnancy status, weeks of pregnancy, sample type, patient type (outpatient or hospitalized), or ZIKV RT-qPCR result, as well as rejected samples that could not be processed due to low quality, were excluded. Samples with negative or positive results were analyzed.
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the Mexican Social Security Institute (Registration No. R-2023-1912-065). Due to the retrospective nature, the Clinical Research Ethics Committee waived the need to obtain informed consent for this study.
Case definitions
The operational definition of a suspected case followed the national guidelines for ZIKV epidemiological surveillance6: Any individual with a rash and at least 2 of the following symptoms: fever, headache, conjunctivitis (non-purulent/hyperemia), arthralgia, myalgia, periarticular edema, pruritus or retroocular pain, as well as an epidemiological association such as a history of residence or travel to an area with local ZIKV transmission two weeks prior to the onset of symptoms and/or a history of unprotected sexual contact in the 2 weeks prior to the onset of symptoms with a person who, in the 8 weeks prior to sexual contact, had a history of residence or traveled to an area with local ZIKV transmission. The operational definition of a suspected case for pregnant women is as previously described without the rash as a constant symptom. All suspected cases must undergo an RT-qPCR diagnostic test within the first 5 days of clinical onset and must be registered in the vector-transmitted diseases database.
RT-qPCR for ZIKV diagnosis
RT-qPCR was performed as previously described26. Briefly, after the sample processing, a 76-bp fragment was amplified using the following primers: Forward 1086–1102, 5’-CCGCTGCCCAACACAAG-3’, Reverse 1162 − 1139, 5’-CCACTAACGTTCTTTTGCAGACAT-3’, probe 1107–1137; and dCAL Fluor Red 610-AGCCTACCTTGACAAGCAGTCAGACACTCAA-BHQ-2, which align with the coding region of the viral E protein gene. Results were visualized and analyzed using 7500 Real-Time PCR System software v.2.3 (Applied Biosystems by Life Technologies).
Variable definitions
The database included independent categorical variables such as sex, age, state of residence, sampling date indicated by months and year, and pregnancy status including trimesters of pregnancy (first trimester < 14 weeks, second trimester 14–27 weeks, third trimester ≥ 28 weeks). The outcome variables (dependent) were PCR result (positive or negative) and patient type according to their status during sampling for qRT-PCR diagnosis, with the categories of hospitalized (patients who met the operational definition of a suspected Zika case and who were admitted to the unit and remained there for more than 24 h), outpatient, and death. All data were obtained from the clinical records. Information about weather conditions (average rainfall in millimeters and environmental temperature in degrees Celsius) was obtained from the Mexican National Meteorological System for each state by month and year27.
Statistical analysis
All the information corresponding to the study variables was recorded in the Microsoft Excel program (Microsoft 365) and analyzed using the IBM SPSS for Windows, Version 26.0 (Armonk, NY: IBM Corp) statistical package in Spanish. Frequencies and percentages were obtained for the categorical variables. The relationship between the independent and outcome variables was analyzed using binary logistic regression models to calculate adjusted odds ratios (AOR) and 95% confidence intervals for each outcome of interest. Continuous variables such as average rainfall and temperature were analyzed using Pearson’s correlation test for the number of cases by state and year. In addition to the correlation test, and given the potential for autocorrelation in time-series data and the complexity of vector-borne disease transmission, a time-series analysis was performed to explore these temporal dependencies and the potencial association between exogenous variables such as average rainfall and temperature and the number of positive cases by month and year. A widely used time series technique suitable for data characterised by autocorrelation, and seasonality - common features of vector-borne disease dynamics - is the autoregressive integrated moving average (ARIMA) test. The parameters of this ARIMA model were (1, 0, 0), which considers a 1 month lag to take into account the mosquito life cycle and the virus incubation times in humans and the vector. Average rainfall and temperature were included in the analysis as exogenous variables. Data analysis was performed using a 95% confidence level and statistical significance of p < 0.05.
Results
Sample characteristics
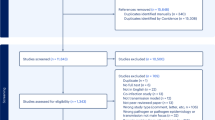
A total of 13,259 suspected ZIKV cases with a RT-qPCR result reported from August 2016 to January 2018 were included, of which 10.7% (n = 1,419) had a positive test for ZVD (Fig. 1). The sample size was sufficiently large for an estimated prevalence of 30.8% ZIKV-positive cases28 at a 95% confidence level.

Zika outbreak in Mexico. Case selection from the IMSS ZVD surveillance database, period August 2016 to January 2018.
Timeline and demographic data
The national distribution of ZIKV suspected cases according to the RT-qPCR results is presented in Table 1 and Supplementary Fig. S1 online. From August 2016 to January 2018, the largest number of ZIKV-positive cases occurred in Veracruz (27.8%), followed by Nuevo León (16.4%) and Yucatan (15.4%). However, the highest positivity rate was observed in Nayarit, at 23.8%. Veracruz reported an 11.4% positivity rate, Nuevo Leon 8.5%, and Yucatan 19.1%.
Most positive cases were reported in 2016 (Supplementary Fig. S2 online). From August to December 2016, out of 7,673 suspected cases, a total of 1,105 (14.4%) were positive for ZVD. Towards the east coast, the states of Veracruz and Quintana Roo had the most positive cases during August. On the Pacific coast, cases began in the state of Michoacan. During this period, the states of Veracruz, Nuevo Leon, and Yucatan had the highest number of positive cases at 321 (29.0%), 219 (19.8%), and 217 (19.6%), respectively.
In 2017, out of 5,429 suspected cases, 313 (5.76%) positive ZIKV cases were reported; fewer than 20 confirmed cases were detected in the first 3 months of the year and, on July, the beginning of the rainy season, the first cases occurred in the states of Nayarit on the Pacific coast and Tamaulipas and Veracruz on the coast of the Gulf of Mexico. During the season, Jalisco, Veracruz, and Tamaulipas had the most cases, with 80 (25.6%), 74 (23.6%), and 43 (13.7%) cases, respectively. In January 2018, only 1 positive case was reported by the epidemiological surveillance laboratory network of the Mexican Social Security Institute.
Percentages were calculated by columns. The positive state rate was calculated as the ratio of positive cases and total cases by state, multiplied by 100. Data collected during the Zika outbreak in Mexico from August 2016 to January 2018. Total, negative, and positive cases confirmed with RT-qPCR assays at the epidemiological surveillance laboratory network of the Mexican Social Security Institute.
In the total sample, the mean age was 30 ± 15 years (median 29, IQR 18), and 68% were women; 36.7% were pregnant with a mean age of 27 ± 6 years. The age distribution shows that most suspected cases occurred in people between 20 and 29 years old (31.8%) (Table 2). Most patients received outpatient treatment (84.2%), and 15.6% were hospitalized. The total case fatality rate was 0.2%, with deaths occurring only in ZIKV-negative RT-qPCR cases (Supplementary Table S1 online). ZIKV was detected in different types of samples, of which 93.3% were serum; the other 6.7% corresponded to urinary sediment, saliva, placental, umbilical cord, and biopsies (Supplementary Table S1 online).
Factors associated with ZIKV infection and hospitalization
Of the 13,259 suspected cases, 1,419 (10.7%) were positive for ZIKV infection. A higher infection rate was observed in women (AOR 2.86, 95% CI 2.44–3.34; p < 0.001) and ages between 20 and 29 years (AOR 1.66, 95% CI 1.21–2.28; p = 0.002). A lower infection rate was observed in children between 0 and 9 years of age (AOR 0.37, 95% CI 0.24–0.58; p < 0.001) (Table 2).
Given the presentation of microcephaly in newborns, there was a special interest in recruiting pregnant women for ZIKV detection. An additional analysis excluding pregnant women was performed for comparative purposes, and the same results were obtained for sex (AOR 1.48, 95% CI 1.24–1.76; p < 0.001). For patients under 30 years of age, a significantly lower association (AOR 0.64, 95% CI 0.45–0.91, p = 0.013) was observed (Supplementary Table S2 online).
Another regression model was performed to determine factors associated with hospitalization. Groups between 20 and 29 years of age and 30 to 39 years had an AOR for hospitalization of 0.39 (95% CI 0.18–0.84, p = 0.015) and 0.41 (95% CI 0.19–0.88; p = 0.022), respectively (Table 3). This analysis was also performed excluding pregnant women (Supplementary Table S3 online), where no significant results were observed for any age group.
Given the higher association observed between infection and female sex, an analysis was performed on the female population. Ages < 10 years had a significantly lower association with infection (AOR 0.56, 95% CI 0.32–1.00; p = 0.046), whereas pregnancy was highly associated with ZIKV infection (AOR 4.11 95% CI 3.52–4.80; p < 0.001) (Table 4).
In pregnant women, a higher infection rate was observed with the first (AOR 1.71, 95% CI 1.35–2.17; p < 0.001) and second trimester of gestation (AOR 2.55, 95% CI 2.08–3.13; p < 0.001) (Table 5). There were no significant differences observed regarding the association of hospitalization with age nor with stage of gestation (Supplementary Table S4).
Environmental factors associated with the ZIKV positivity in Veracruz
During the entire study period (August 2016 to January 2018), positive cases were mainly found in the states of Veracruz, Nuevo Leon, and Yucatan. Correlations between positive cases, average rainfall scores and temperatures were performed only for Veracruz due to its high number of ZIKV-positive cases. In Veracruz, the average rainfall and temperature for the entire period were 158 ± 118 mm and 23.3 ± 2.1 °C, respectively. Also in this state, from August to December 2016 (5 months), a significant correlation was observed between the number of total ZIKV-positive cases and the rainfall scores (r = 0.531, p = 0.027) (Supplementary Fig. S3 online) and the average temperature (23.5 ± 1.87 °C) (0.9739, p = 0.0017) (Supplementary Fig. S4 online). In 2017, from January to December, also in Veracruz, a correlation was observed between hospitalized cases and rainfall scores (r = 0.7975, p = 0.002) (Supplementary Fig. S5 online). These interactions were analyzed with the ARIMA test (1, 0, 0 model) with a 1-month lag and average rainfall and temperature as exogenous variables; there was insufficient evidence to demonstrate an association between environmental factors and the number of positive ZIKV cases (Supplementary Fig. S6 online).
Discussion
This is an exploratory study investigating the association of age, sex, and stage of gestation in pregnant women, in addition to environmental variables, with infection and hospitalization of ZIKV positive-patients during the ZIKV 2016–2018 outbreak. ZIKV outbreaks peaked in 2016 and have declined significantly since 2018. However, as the WHO reported in the epidemiological update from 2019 to 2022, Mexico is on the list of countries with evidence of autochthonous transmission of ZIKV29; in 2024, there were 30 autochthonous confirmed cases of ZVD, as reported by the National Epidemiological Surveillance System of the Ministry of Health30. Furthermore, up to July 21, 2025, there are 2 cases already reported, one taking place in Michoacan and the other in Veracruz31. Therefore, ZIKV continues to be monitored in Mexico32.
The Mexican Social Security Institute (IMSS) is the largest health institution, with a coverage of 51% of the Mexican population33, and it has become a representative institution of the national epidemiology situation. A study carried out with IMSS ZIKV data for a total of 43,725 ZIKV suspected cases dating from January to December 2016 reported that 1,700 (3.8%) were positive for ZIKA28. Compared to our study, we observed a higher positivity (6.0%), which could be due to the period analyzed and the elegibility criteria used.
Factors associated with ZIKV infection and hospitalization
Regarding age, we observed that the group between 20 and 29 years old was significantly associated with ZIKV infection overall, which agrees with previous literature28, except when pregnant women were excluded from the analysis. This could be due to less outdoor exposure and fewer work responsibilities compared with the older groups, as well as the fact that a significant number of pregnant women (n = 3,008) who by sex were already associated with infection, as shown here and elsewhere17, were removed from the analysis.
Regarding sex, our results demonstrate that ZIKV infection was higher in women, even when pregnant women were not considered in the analysis; this agrees with previous reports17,34,35,36. Some of the theories proposed for a higher infection in female sex37,38 is the skin microbiome, which has been shown to predispose women to Aedes mosquito bites37 and other non-vectorial routes38 like the sexual transmission of ZIKV39. Considering an 80% rate of asymptomatic ZIKV cases and since it has been reported that ZIKV RNA can be detected in semen after six months of symptom presentation40, sexually active women are far more likely to get ZIKV than men (90% increase), and this makes direct sexual contact the most probable transmission route since the 2015 outbreak17. Another factor to consider is that in general, there are more women affiliated with the health system compared to men (75% vs. 72% in 2020)41. This is also reflected in the number of women that seek consultation at the IMSS, which in 2020 was 83.2% compared to 81.9% by men41. Furthermore, it has been shown that in Mexico, men consult less than women; in 2016, only 34% of 320 million consults were required by men42.
Even when several studies have reported that there is no difference between pregnant and non-pregnant women regarding their probability to infection neither hospitalization5,43, blood components such as iron have been investigated as potential factors involved in mosquito feeding preferences, and it has been shown that Aedes aegypti feeds more on iron-deficient mice and that iron supplementation reduces dengue virus prevalence and viral load44. Therefore, women with iron deficiency, a common situation in pregnancy, could be more susceptible to the Aedes mosquito bite37.
The present study, observed 25% (n = 3,313) ZIKV positive cases in Mexican pregnant women, which agrees with previous studies28. Our analysis showed an association between infection and the first and second trimesters of pregnancy, which coincides with previous national reports45. These findings highlight the importance of surveillance in this particular population given that ZIKV infection during the first trimester of pregnancy is associated with a higher risk of microcephaly46,47; multiple reports have described their exposure and effects on their fetuses48,49, and the incidence of microcephaly has increased with ZIKV circulation compared with periods when ZIKV was not present47. Therefore, prevention strategies and epidemiological surveillance expansion to pregnant women without symptoms during an epidemic outbreak is suggested, specially during the first two trimesters of pregnancy.
Regarding hospitalization, ZIKV-positive cases had a low rate (11.3%), with zero fatality cases, which is consistent with published literature48,50; in pregnant women, no significant differences in hospitalization by trimester were observed.
Environmental factors and ZIKV infection and hospitalization
ZIKV was introduced in Mexico at the end of 2015. The first cases were observed in areas already endemic to dengue and chikungunya virus since 201451.
The three states with the highest number of ZIKV-positive cases were Veracruz, Nuevo León, and Yucatán, the latter also reported by Grajales-Muñiz et al., (2019)28. A significant correlation was observed between hospitalized positive patients and rainfall scores in 2017 when this was analyzed for Veracruz, the state with most suspected cases.
The abundance of mosquitoes and rainfall has been previously investigated and controversial results have been published where some authors do observe a positive correlation52, whereas others disagree53. Regarding environmental temperatures, it was previously shown that ZIKV spreads efficiently through the host population across a broad range of environmental temperatures, from 17 °C to 37 °C54. This is consistent with our findings where a distribution in climatologically diverse areas, such as Nuevo Leon (dry-warm) and Veracruz (warm-humid) was observed55. Several studies carried out in Ecuador and Vietnam have documented an association between temperature levels and the number of cases and hospitalization; in addition, the relationship of rainfall levels with epidemic outbreaks has been demonstrated in Brazil, Colombia, and Bangladesh15,16,56,57,58. In Mexico, an association between environmental factors and vector-borne diseases has been documented; an increase in environmental temperature, sea surface temperature, precipitation and the “El Niño” phenomenon have been associated with dengue fever59, a disease with a seasonality similar to ZVD, and an increase in cases between the months of July and January60. This is the first exploratory study reporting the number of cases and hospitalizations of the 2016–2018 ZVD outbreak and their relationship with climatic factors in the country.
The influence of climate variability in vector-borne diseases has been evaluated using the index P, which measures the transmission potential of mosquito-borne pathogens. The mathematical model, which includes humidity, temperature, and precipitation variables, showed a high correlation with dengue incidence, chikungunya, and Zika18. Nonetheless, the potential use of mathematical predictor tools based in the epidemiology data of vector-borne diseases is only effective for endemic diseases like dengue because of the high number of cases; for Zika and chikungunya, other factors besides environmental climate conditions must also be considered18.
Low rates of ZIKV in Mexico after the 2016–2018 outbreak
Some theories have been proposed to explain the reason for the low prevalence of ZIKV infections. For instance, a study reporting the vector distribution and transmission risk states that Mexico is one of the countries particularly affected according to their mathematical model. However, their model included habitat suitability and temperature, and underscored that there are very few areas where suitable habitat and optimal temperature conditions overlap for the two main vector species13. Furthermore, competition between vectors is possible—for instance, between Ae. aegypti and Ae. albopictus, it has been reported that vector competition varies among collections and geographic regions, with a lower rate in northeastern Mexico and the highest rate on the Pacific coast61. Cx. quinquefasciatus has been shown to be refractory to ZIKV infection, dissemination, and transmission using adult mosquitoes that were collected in the larva or egg stage from areas where no human confirmed cases were reported in Guadalajara, Jalisco, Mexico62. In addition, the presence of other mosquito species might impact the virus dissemination. It has been shown that at the beginning of the 2015 ZIKV outbreak in Mexico, both Zika and dengue were present in locations with high dengue risk; at the end of the outbreak, Zika was mainly present in areas with low dengue risk14.
Another reason for the low incidence could be that cases are not being officially reported; a research group has investigated the prevalence of ZIKV on serum samples from suspected patients (with symptoms consistent with flavivirus infection) from Yucatan, Mexico, from 2021 to 2022 and a total of 25 cases were positive to ZIKV with an estimated incidence of 2.8 symptomatic cases per 1,000 persons per year63. This emphasized the need for continuous ZIKV surveillance and reporting in Mexico.
Limitations
Among the limitations of this study is the use of a secondary data source; there is a lack of information about the hospital setting and the confirmed cause for hospitalization. In addition, an undercount of cases is possible. During the first year of co-circulation of these arboviruses, there was a generalized underestimation because the diagnostic algorithm consisted of uniplex PCR reactions for each virus and was limited to only 1 reaction per sample; the physician’s clinical suspicion was the only factor defining the laboratory diagnosis64. Furthermore, changes in the internal surveillance policies and diagnostic algorithms ocurred during the study period, which may have impacted the number of reported cases. The generalizability of our findings might be limited due to the combination of specific climatic and environmental conditions for ZIKV during the period of study in Mexico. It is necessary to integrate mosquito genetic, vector, and climatic factors to identify the dynamics of their interaction and temporality. In addition, the process for diagnosis also affects temporality, mainly due to the differences in the times for seeking medical attention and the presentation of the first symptom or the time until sampling. It is also important to consider the low circulation or disappearance of ZIKV in the American continent from 2018 onwards49, which has limited the period of study. Because the database is constructed from passive surveillance, only symptomatic patients who required ZIKV testing were included in this study.
Conclusions
Recently, minimal circulation of ZIKV has been reported in Mexico, with only 30 cases in 2024 and 2 cases up to july 21, 202531. However, the coexistence of three mosquito species of medical importance for vector-borne diseases, Aedes aegypti, Aedes albopictus, and Culex quinquefasciatus, have been reported in urban and semiurban areas65. Therefore, we should not ignore the potential reemergence of ZIKV in the coming years because of the similar seasonality and persistent appearance every 7 or 8 years have been reported for other arboviruses66. Entomological surveillance and appropriate implementation of strategies to control the three species are necessary to avoid the combination of factors such as weather, susceptible population, and vector-borne viruses with infectious potential. Epidemiologic surveillance of ZIKV and exploratory reports like ours must be maintained, emphasizing analysis that includes pregnant women.
Data availability
Data are available as supplementary files.
References
Bueno-Mari, R. & Jimenez-Peydro, R. Global change and human vulnerability to vector-borne diseases. Front. Physiol. 4, 158 (2013).
International Committee on Taxonomy of Viruses: ICTV. (2024). Available from: https://ictv.global/. Last access: June 6, 2024 [.
Kindhauser, M. K., Allen, T., Frank, V., Santhana, R. S. & Dye, C. Zika: the origin and spread of a mosquito-borne virus. Bull. World Health Organ. 94 (9), 675–86 C (2016).
Bogoch, I. I. et al. Potential for Zika virus introduction and transmission in resource-limited countries in Africa and the Asia-Pacific region: a modelling study. Lancet. Infect. Dis. 16 (11), 1237–1245 (2016).
Duffy, M. R. et al. Zika virus outbreak on Yap island, federates States of Micronesia. N. Engl. J. Med. ;360. (2009).
Secretaría de Salud. Lineamientos Estandarizados para la Vigilancia Epidemiológica y Diagnóstico por Laboratorio de Infección por Virus Zika V 3.0 2016 [ (2023). Available from: https://www.gob.mx/cms/uploads/attachment/file/121722/lineamientos_ve_y_lab_virus_zika.pdf last access January 11, (Accessed January 11 2023).
Krauer, F. et al. O. Z. C. W. Zika virus infection as a cause of congenital brain abnormalities and Guillain-Barre syndrome: systematic review. PLoS Med. 14 (1), e1002203 (2017).
Sharma, A. & Lal, S. K. Zika virus: transmission, detection, control, and prevention. Front. Microbiol. 8, 110 (2017).
Calvert, A. E. et al. The specificity of the persistent IgM neutralizing antibody response in Zika virus infections among individuals with prior dengue virus exposure. J. Clin. Microbiol. 59 (8), e0040021 (2021).
Paiva, M. H. S., Guedes, D. R. D., Leal, W. S. & Ayres, C. F. J. Sensitivity of RT-PCR method in samples shown to be positive for Zika virus by RT-qPCR in vector competence studies. Genet. Mol. Biol. 40 (3), 597–599 (2017).
Paz-Bailey, G. et al. Persistence of Zika virus in body Fluids - Final report. N Engl. J. Med. 379 (13), 1234–1243 (2018).
McGibbon, E. et al. Epidemiological characteristics and laboratory findings of Zika virus cases in new York city, January 1, 2016-June 30, 2017. Vector Borne Zoonotic Dis. 18 (7), 382–389 (2018).
Cunze, S., Kochmann, J., Koch, L. K., Genthner, E. & Klimpel, S. Vector distribution and transmission risk of the Zika virus in South and central America. PeerJ 7, e7920 (2019).
Cortes-Escamilla, A., Roche, B., Rodriguez-Lopez, M. H., Lopez Gatell-Ramirez, H. & Alpuche-Aranda, C. M. Spatiotemporal patterns of dengue and Zika incidence during the 2015–2018 outbreak of Zika in Mexico. Salud Publica Mex. 64 (5), sept–oct (2022).
Chien, L. C., Lin, R. T., Liao, Y., Sy, F. S. & Perez, A. Surveillance on the endemic of Zika virus infection by meteorological factors in colombia: a population-based Spatial and Temporal study. BMC Infect. Dis. 18 (1), 180 (2018).
Fuller, T. L. et al. Behavioral, climatic, and environmental risk factors for Zika and Chikungunya virus infections in Rio de janeiro, brazil, 2015-16. PLoS One. 12 (11), e0188002 (2017).
Coelho, F. C. et al. Higher incidence of Zika in adult women than adult men in Rio de Janeiro suggests a significant contribution of sexual transmission from men to women. Int. J. Infect. Dis. 51, 128–132 (2016).
Carreto, C., Gutierrez-Romero, R. & Rodriguez, T. Climate-driven mosquito-borne viral suitability index: measuring risk transmission of dengue, Chikungunya and Zika in Mexico. Int. J. Health Geogr. 21 (1), 15 (2022).
Asad, H. & Carpenter, D. O. Effects of climate change on the spread of Zika virus: a public health threat. Rev. Environ. Health. 33 (1), 31–42 (2018).
Haby, M. M., Pinart, M., Elias, V. & Reveiz, L. Prevalence of asymptomatic Zika virus infection: a systematic review. Bull. World Health Organ. 96 (6), 402–13D (2018).
Fabián, C. M. et al. Cassandra González-Acosta; David Mejía-Zúñiga;;; Moreno-García M. Surveillance for Zika in Mexico: naturally infected mosquitoes in urban and semi-urban areas. Pathogens and Global Health. ;113(7):309 – 14. (2019).
Duong, V., Dussart, P. & Buchy, P. Zika virus in Asia. Int. J. Infect. Dis. 54, 121–128 (2017).
Codrington, J. et al. Zika virus outbreak in suriname, a report based on laboratory surveillance data. PLoS Curr. ;10. (2018).
Gomez-Dantes, O. & Frenk, J. [Chronicle of a century of public health in mexico: from public health to social protection in health]. Salud Publica Mex. 61 (2), 202–211 (2019).
Robinson, D. P. & Klein, S. L. Pregnancy and pregnancy-associated hormones alter immune responses and disease pathogenesis. Horm. Behav. 62 (3), 263–271 (2012).
Lanciotti, R. S. et al. Genetic and serologic properties of Zika virus associated with an epidemic, Yap state, micronesia, 2007. Emerg. Infect. Dis. 14 (8), 1232–1239 (2008).
Servicio Meteorológico Nacional. Comisión Nacional del Agua; Gobierno de México. Resúmenes Mensuales de Temperaturas y Lluvia 2023 [updated December 2023]. (2023). Available from: https://smn.conagua.gob.mx/es/climatologia/temperaturas-y-lluvias/resumenes-mensuales-de-temperaturas-y-lluvias
Grajales-Muniz, C. et al. Zika virus: epidemiological surveillance of the Mexican Institute of social security. PLoS One. 14 (2), e0212114 (2019).
World Health Organization. Zika epidemiology update-February 20222022. Available from: https://www.who.int/publications/m/item/zika-epidemiology-update---february-2022
Dirección General de Epidemiología; Secretaría de Salud. Casos Confirmados Autóctonos de Enfermedad por Virus del Zika por Entidad Federativa. Semana Epidemiológica 50. (2024).
Dirección General de Epidemiología; Secretaría de Salud; Estados Unidos Mexicanos. Boletín Epidemiológico. Sistema Nacional de Vigilancia Epidemiológica, Sistema Único de Información. Vigilancia Epidemiológica, Semana 28. (2025).
Argaez-Sierra, D. G. et al. Entomo-virological surveillance of flavivirus in mosquitoes in Yucatan state, Mexico. Rev. Inst. Med. Trop. Sao Paulo. 66, e56 (2024).
Instituto Nacional de Estadística y Geografía. Demografía y sociedad: Derechohabiencia. (2020). Retrieved from: https://www.inegi.org.mx/temas/derechohabiencia/
Lozier, M. et al. Incidence of Zika virus disease by age and sex- Puerto Rico, November 1, 2015 - October 20, Morbidity and Mortality Weekly Report. (2016).
Jimenez-Corona, M. E. et al. Clinical and epidemiological characterization of Laboratory-Confirmed autochthonous cases of Zika virus disease in Mexico. PLOS Curr. ;15. (2016).
Mungall-Baldwin, C. Women’s participation in the prevention and control of dengue using environmental methods in the global south: a qualitative meta-synthesis. Int. J. Equity Health. 21 (1), 140 (2022).
Gilbert, I. H., Gouck, H. K. & Smith, N. Attractiveness of men and women to Aedes aegypti and relative protection time obtained with Deet. Fla. Entomol. 49 (1), 53–66. https://doi.org/10.2307/3493317 (1966).
Qiu, H. Y. et al. Aerosolized Zika virus infection in Guinea pigs. Emerg. Microbes Infect. 11 (1), 2350–2358 (2022).
da Silva, L. R. C. Zika virus trafficking and interactions in the human male reproductive tract. Pathogens ;7(2). (2018).
Nicastri, E. et al. Persistent detection of Zika virus RNA in semen for six months after symptom onset in a traveller returning from Haiti to italy. Eurosurveillance ;21(32). (2016).
Instituto Nacional de Estadística y Geografía (INEGI). Mujeres y Hombres en México 2021–2022. ; (24). Available from: https://www.inegi.org.mx/contenidos/productos/prod_serv/contenidos/espanol/bvinegi/productos/nueva_estruc/889463907381.pdf (2023).
de Gobierno México; Secretaría de Salud. La prevención entre los hombres: un tema de salud pendiente. (2018).
Zorrilla, C. D., Garcia Garcia, I. & De La Garcia Fragoso, L. Zika virus infection in pregnancy: maternal, fetal, and neonatal considerations. J. Infect. Dis. 216 (suppl_10), S891–S6 (2017).
Zhu, Y. et al. Host serum iron modulates dengue virus acquisition by mosquitoes. Nat. Microbiol. 4 (12), 2405–2415 (2019).
Secretaría de Salud. Casos confirmados por laboratorio de Síndrome Congénito asociado a Zika, México https://www.gob.mx/cms/uploads/attachment/file/652543/Cuadro_SCAZ_CONFIRMADOS_Laboratorio_28junio2021.pdf (2021).
Morris, J., Orioli, I. M. & Benavides-Lara, A. de la Paz Barboza-Arguello M.; Tapia M. A. C.; de Franca G. V. A.; Groisman B.; Holguin J.; Hurtado-Villa P. M.; Ibarra Ramirez M., et al. Prevalence of microcephaly: the Latin American Network of Congenital Malformations 2010–2017. BMJ Paediatr Open. ;5(1):e001235. (2021).
Hernandez-Avila, J. E. et al. Zika virus infection estimates, Mexico. Bull. World Health Organ. 96 (5), 306–313 (2018).
Halani, S. et al. Clinical manifestations and health outcomes associated with Zika virus infections in adults: A systematic review. PLoS Negl. Trop. Dis. 15 (7), e0009516 (2021).
Pielnaa, P. et al. Zika virus-spread, epidemiology, genome, transmission cycle, clinical manifestation, associated challenges, vaccine and antiviral drug development. Virology 543, 34–42 (2020).
Rocha, A. M. O. et al. Palliative care in congenital syndrome of the Zika virus associated with hospitalization and emergency consultation: palliative care and congenital syndrome of Zika. J. Trop. Med. 2018, 1025193 (2018).
Dirección General de Epidemiologia; Secretaría de Salud; Estados Unidos Mexicanos. Anuario de Morbilidad, Distribución de casos nuevos de enfermedad por mes, Población General. 2015 [cited 2022 November 25]. Available from: https://epidemiologia.salud.gob.mx/anuario/html/morbilidad_nacional.html., ( 2022).
Galardo, A. K. R., Zimmerman, R. H., Lounibos, L. P. & Young, L. J. D’almeida Couto A. A. R. Seasonal abundance of anopheline mosquitoes and their association with rainfall and malaria along the Matapí river, amapí, Brazil. Med. Vet. Entomol. 23, 335–349 (2009).
Halai, U. A. et al. Maternal Zika virus disease severity, virus load, prior dengue antibodies, and their relationship to birth outcomes. Clin. Infect. Dis. 65 (6), 877–883 (2017).
Ngonghala, C. N. et al. Effects of changes in temperature on Zika dynamics and control. J. R Soc. Interface. 18 (178), 20210165 (2021).
Instituto Nacional de Estadística y Geografía. Geografía y medio ambiente: Climatología https://www.inegi.org.mx/temas/climatologia/#mapas] (2025).
Dey, S. K. et al. Rahman E. U. Prediction of dengue incidents using hospitalized patients, metrological and socio-economic data in bangladesh: A machine learning approach. PLoS One. 17 (7), e0270933 (2022).
Reina Ortiz, M. et al. Post-earthquake Zika virus surge: disaster and public health threat amid Climatic conduciveness. Sci. Rep. 7 (1), 15408 (2017).
Pham, H. V., Doan, H. T., Phan, T. T. & Minh N. N. Ecological factors associated with dengue fever in a central highlands province, Vietnam. BMC Infect. Dis. 11, 172 (2011).
Colon-Gonzalez, F. J., Lake, I. R. & Bentham, G. Climate variability and dengue fever in warm and humid Mexico. Am. J. Trop. Med. Hyg. 84 (5), 757–763 (2011).
Dirección General de Epidemiología. Secretaría de Salud; Estados Unidos Mexicanos. Informes Semanales para la Vigilancia Epidemiológica de Dengue 2022 [cited 2022 November 25]. Available from: https://www.gob.mx/salud/documentos/informes-semanales-para-la-vigilancia-epidemiologica-de-dengue-2022 (2022).
Garcia-Luna, S. M. et al. Variation in competence for ZIKV transmission by Aedes aegypti and Aedes albopictus in Mexico. PLoS Negl. Trop. Dis. 12 (7), e0006599 (2018).
Elizondo-Quiroga, D. et al. Vector competence of Aedes aegypti and culex quinquefasciatus from the metropolitan area of guadalajara, jalisco, Mexico for Zika virus. Sci. Rep. 9 (1), 16955 (2019).
Earnest, J. T. et al. Evidence of ongoing transmission of Zika virus in mérida, Mexico. Am. J. Trop. Med. Hyg. 110 (4), 724–730 (2024).
Fernandes-Matano, L. et al. Impact of the introduction of Chikungunya and Zika viruses on the incidence of dengue in endemic zones of Mexico. PLoS Negl. Trop. Dis. 15 (12), e0009922 (2021).
Lopez-Solis, A. D. et al. Aedes aegypti, ae. albopictus and culex quinquefasciatus adults found coexisting in urban and semiurban dwellings of Southern Chiapas. Mexico Insects ;14(6). (2023).
Laras, K. et al. Tracking the re-emergence of epidemic Chikungunya virus in Indonesia. Trans. R Soc. Trop. Med. Hyg. 99 (2), 128–141 (2005).
Acknowledgements
We are grateful for the work of the epidemiologists of the Mexican Social Security Institute who were responsible for generating the databases supporting this project.
Author information
Authors and Affiliations
Contributions
M.B.L. and F.G.S. performed the conceptualization. B.L.E.G. and M.B.L. performed investigation. J.E.M.M. provided resources. M.E.C.M., B.T.C. and B.L.E.G. performed data curation. M.E.C.M. and B.L.E.G. performed formal analysis. M.E.C.M., M.B.L. and B.L.E.G. proposed the methodology. M.E.C.M., F.G.S. and B.L.E.G. wrote original draft. M.B.L., B.T.C., A.M.S., K.P.U., J.G.I., C.R.G.B., C.S.T., Y.L.H, H.M.F. and A.M.P. wrote and edited the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Camacho-Moll, M.E., de León, M.B., Muñoz-Medina, J.E. et al. Factors associated with infection and hospitalization of Zika cases during the 2016–2018 outbreak in Mexico. Sci Rep 15, 37585 (2025). https://doi.org/10.1038/s41598-025-16239-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16239-3
